
Ciprofloxacin-Loaded Inhalable Formulations against Lower Respiratory Tract Infections: Challenges, Recent Advances, and Future Perspectives

Abstract

1. Introduction
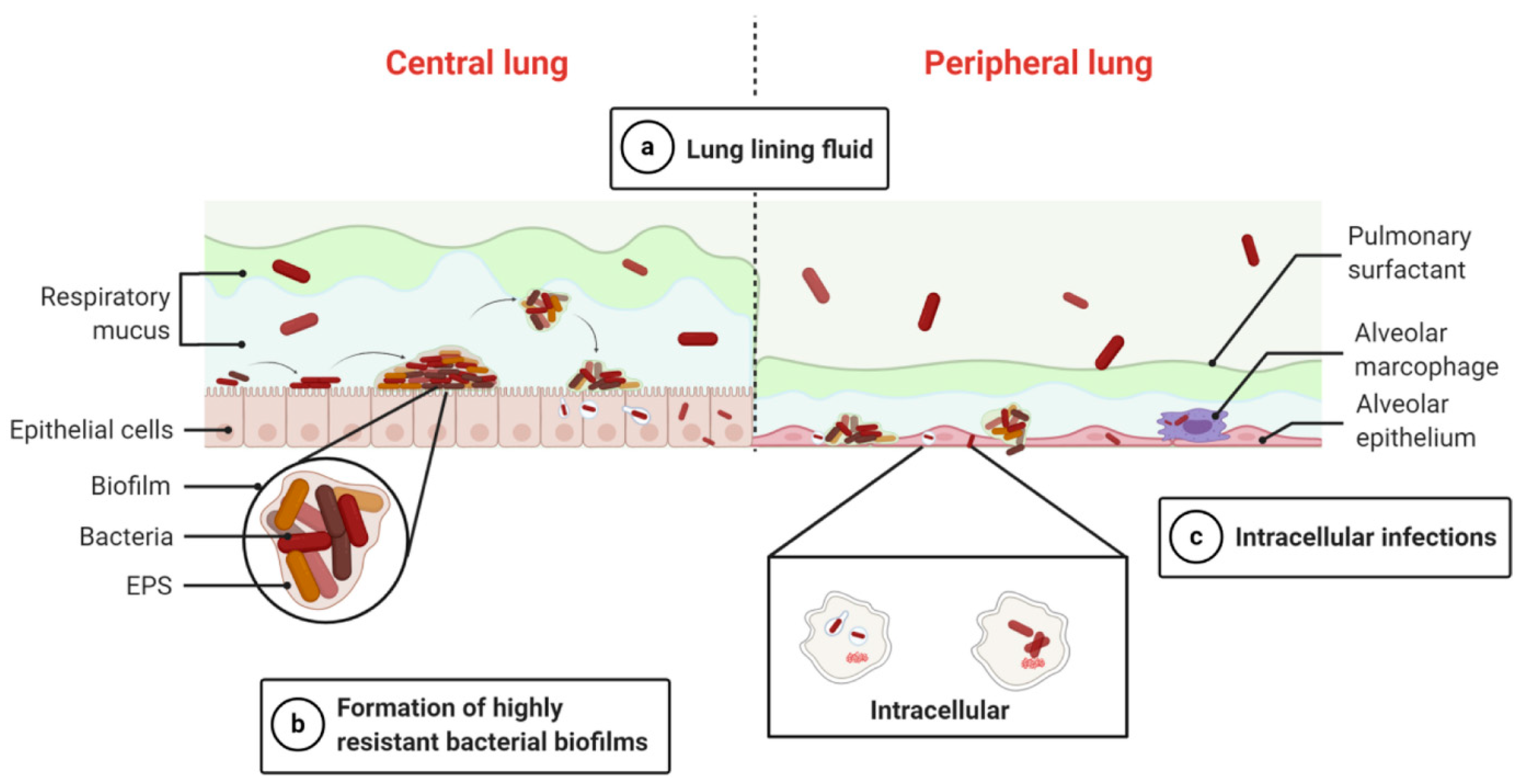
1.1. Biological Barriers for Effective Inhalation Antimicrobials Delivery
1.1.1. Lung Lining Fluid
1.1.2. Bacterial Biofilms
1.1.3. Intracellular Infections
2. CFX DPI: Pharmacokinetics, Pharmacodynamics, and Metabolism
3. Inhalation Devices and CFX Inhalable Formulations: Merits and Demerits in LRTIs
3.1. Inhalation Devices
3.1.1. Nebulizers
3.1.2. Metered-Dose Inhaler (MDI)
3.1.3. Dry Powder Inhaler (DPI)
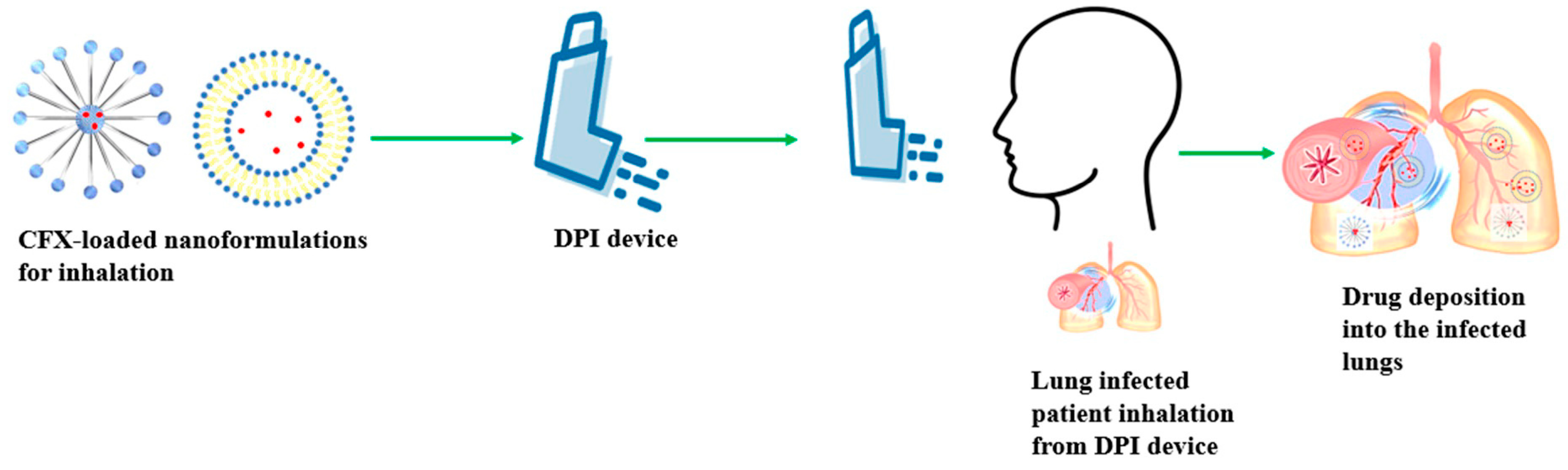
3.2. CFX Inhalable Formulations
3.2.1. Liposomes
3.2.2. Micelles
3.2.3. Nanosuspensions
3.2.4. Chitosan Loaded Nanoparticles
3.2.5. Solid Lipid Nanoparticles
3.2.6. Metal-Containing Nanoparticles
3.3. Commercialized Formulations of Inhaled CFX
3.4. Potential Biomarkers for Identifying CFX Resistance in LRTIs
3.5. CFX Inhalable Formulations for LRTIs Management in Preclinical Settings
3.6. CFX Inhalable Formulations for LRTI Management in Clinical Settings
4. Challenges and Recent Advances
5. Safety, Tolerability, and Regulatory Concerns
6. Future Perspectives
7. Expert Opinion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sabuj, M.Z.R.; Dargaville, T.R.; Nissen, L.; Islam, N. Inhaled ciprofloxacin-loaded poly(2-ethyl-2-oxazoline) nanoparticles from dry powder inhaler formulation for the potential treatment of lower respiratory tract infections. PLoS ONE 2021, 16, e0261720. [Google Scholar] [CrossRef] [PubMed]
- Panthi, V.K.; Fairfull-Smith, K.E.; Islam, N. Antibiotic loaded inhalable liposomal nanoparticles against lower respiratory tract infections: Challenges, recent advances, and future perspectives. J. Drug Deliv. Sci. Technol. 2024, 94, 105517. [Google Scholar] [CrossRef]
- Bensman, T.J.; Wang, J.; Jayne, J.; Fukushima, L.; Rao, A.P.; D’Argenio, D.Z.; Beringer, P.M. Pharmacokinetic-Pharmacodynamic Target Attainment Analyses to Determine Optimal Dosing of Ceftazidime-Avibactam for the Treatment of Acute Pulmonary Exacerbations in Patients with Cystic Fibrosis. Antimicrob. Agents Chemother. 2017, 61, e00988-17. [Google Scholar] [CrossRef]
- Kumbhar, P.; Kaur, J.; De Rubis, G.; Paudel, K.R.; Prasher, P.; Patel, V.K.; Corrie, L.; Chellappan, D.K.; Gupta, G.; Singh, S.K.; et al. Inhalation drug delivery in combating pulmonary infections: Advances and challenges. J. Drug Deliv. Sci. Technol. 2023, 89, 105022. [Google Scholar] [CrossRef]
- García Clemente, M.; Olveira, C.; Girón, R.; Máiz, L.; Sibila, O.; Golpe, R.; Menéndez, R.; Rodríguez, J.; Barreiro, E.; Rodríguez Hermosa, J.L.; et al. Impact of Chronic Bronchial Infection by Staphylococcus aureus on Bronchiectasis. J. Clin. Med. 2022, 11, 3960. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Guo, K.; Zhang, L.; Guo, Y.; Feng, Y.; Cvijić, S.; Cun, D.; Yang, M. In Vitro and In Vivo Evaluation of Inhalable Ciprofloxacin Sustained Release Formulations. Pharmaceutics 2023, 15, 2287. [Google Scholar] [CrossRef] [PubMed]
- VanDevanter, D.R.; Heltshe, S.L.; Hilliard, J.B.; Konstan, M.W. Pseudomonas aeruginosa antimicrobial susceptibility test (AST) results and pulmonary exacerbation treatment responses in cystic fibrosis. J. Cyst. Fibros. 2021, 20, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Cipolla, D.; Chan, H.K. Inhaled antibiotics to treat lung infection. Pharm. Pat. Anal. 2013, 2, 647–663. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.H.; Brown, G.H.; Peterson, M.L.; Rotschafer, J.C. Application of fluoroquinolone pharmacodynamics. J. Antimicrob. Chemother. 2000, 46, 669–683. [Google Scholar] [CrossRef]
- Weers, J. Inhaled antimicrobial therapy—Barriers to effective treatment. Adv. Drug Deliv. Rev. 2015, 85, 24–43. [Google Scholar] [CrossRef]
- Fink, M.P.; Snydman, D.R.; Niederman, M.S.; Leeper, K.V., Jr.; Johnson, R.H.; Heard, S.O.; Wunderink, R.G.; Caldwell, J.W.; Schentag, J.J.; Siami, G.A.; et al. Treatment of severe pneumonia in hospitalized patients: Results of a multicenter, randomized, double-blind trial comparing intravenous ciprofloxacin with imipenem-cilastatin. The Severe Pneumonia Study Group. Antimicrob. Agents Chemother. 1994, 38, 547–557. [Google Scholar] [CrossRef]
- Peloquin, C.A.; Cumbo, T.J.; Nix, D.E.; Sands, M.F.; Schentag, J.J. Evaluation of intravenous ciprofloxacin in patients with nosocomial lower respiratory tract infections. Impact of plasma concentrations, organism, minimum inhibitory concentration, and clinical condition on bacterial eradication. Arch. Intern. Med. 1989, 149, 2269–2273. [Google Scholar] [CrossRef]
- McShane, P.J.; Weers, J.G.; Tarara, T.E.; Haynes, A.; Durbha, P.; Miller, D.P.; Mundry, T.; Operschall, E.; Elborn, J.S. Ciprofloxacin Dry Powder for Inhalation (ciprofloxacin DPI): Technical design and features of an efficient drug–device combination. Pulm. Pharmacol. Ther. 2018, 50, 72–79. [Google Scholar] [CrossRef]
- De Soyza, A.; Aksamit, T. Ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Expert Opin. Orphan Drugs 2016, 4, 875–884. [Google Scholar] [CrossRef]
- Cipolla, D.; Gonda, I.; Chan, H.-K. Liposomal formulations for inhalation. Ther. Deliv. 2013, 4, 1047–1072. [Google Scholar] [CrossRef]
- Choi, J.M.; Park, K.; Lee, B.; Jeong, D.; Dindulkar, S.D.; Choi, Y.; Cho, E.; Park, S.; Yu, J.H.; Jung, S. Solubility and bioavailability enhancement of ciprofloxacin by induced oval-shaped mono-6-deoxy-6-aminoethylamino-β-cyclodextrin. Carbohydr. Polym. 2017, 163, 118–128. [Google Scholar] [CrossRef]
- Stass, H.; Badorrek, P.; Hohlfeld, J.; Krug, N.; Nagelschmitz, J.; Welte, T. Safety and Pharmacokinetics of Multiple-Dose Ciprofloxacin Dry Powder for Inhalation in Patients with Moderate or Severe COPD. Eur. Respir. J. 2011, 38, 3011. [Google Scholar]
- Stass, H.; Weimann, B.; Nagelschmitz, J.; Rolinck-Werninghaus, C.; Staab, D. Tolerability and pharmacokinetic properties of ciprofloxacin dry powder for inhalation in patients with cystic fibrosis: A phase I, randomized, dose-escalation study. Clin. Ther. 2013, 35, 1571–1581. [Google Scholar] [CrossRef]
- Stass, H.; Delesen, H.; Nagelschmitz, J.; Staab, D. Safety and pharmacokinetics of ciprofloxacin dry powder for inhalation in cystic fibrosis: A phase I, randomized, single-dose, dose-escalation study. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Stass, H.; Nagelschmitz, J.; Willmann, S.; Delesen, H.; Gupta, A.; Baumann, S. Inhalation of a dry powder ciprofloxacin formulation in healthy subjects: A phase I study. Clin. Drug Investig. 2013, 33, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Shariati, A.; Arshadi, M.; Khosrojerdi, M.A.; Abedinzadeh, M.; Ganjalishahi, M.; Maleki, A.; Heidary, M.; Khoshnood, S. The resistance mechanisms of bacteria against ciprofloxacin and new approaches for enhancing the efficacy of this antibiotic. Front. Public Health 2022, 10, 1025633. [Google Scholar] [CrossRef]
- Yayehrad, A.T.; Wondie, G.B.; Marew, T. Different Nanotechnology Approaches for Ciprofloxacin Delivery Against Multidrug-Resistant Microbes. Infect. Drug Resist. 2022, 15, 413–426. [Google Scholar] [CrossRef]
- Wilson, R.; Welte, T.; Polverino, E.; De Soyza, A.; Greville, H.; O’Donnell, A.; Alder, J.; Reimnitz, P.; Hampel, B. Ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis: A phase II randomised study. Eur. Respir. J. 2013, 41, 1107–1115. [Google Scholar] [CrossRef]
- Chorepsima, S.; Kechagias, K.S.; Kalimeris, G.; Triarides, N.A.; Falagas, M.E. Spotlight on inhaled ciprofloxacin and its potential in the treatment of non-cystic fibrosis bronchiectasis. Drug Des. Dev. Ther. 2018, 12, 4059–4066. [Google Scholar] [CrossRef]
- Huang, Z.; Kłodzińska, S.N.; Wan, F.; Nielsen, H.M. Nanoparticle-mediated pulmonary drug delivery: State of the art towards efficient treatment of recalcitrant respiratory tract bacterial infections. Drug Deliv. Transl. Res. 2021, 11, 1634–1654. [Google Scholar] [CrossRef]
- Poschet, J.; Perkett, E.; Deretic, V. Hyperacidification in cystic fibrosis: Links with lung disease and new prospects for treatment. Trends Mol. Med. 2002, 8, 512–519. [Google Scholar] [CrossRef]
- Tate, S.; MacGregor, G.; Davis, M.; Innes, J.; Greening, A. Airways in cystic fibrosis are acidified: Detection by exhaled breath condensate. Thorax 2002, 57, 926. [Google Scholar] [CrossRef]
- Celli, J.P.; Turner, B.S.; Afdhal, N.H.; Ewoldt, R.H.; McKinley, G.H.; Bansil, R.; Erramilli, S. Rheology of gastric mucin exhibits a pH-dependent sol−gel transition. Biomacromolecules 2007, 8, 1580–1586. [Google Scholar] [CrossRef]
- Li, M.; Yao, M.; Wang, W.; Wan, P.; Chu, X.; Zheng, Y.; Yang, K.; Zhang, Y. Nitrogen-containing bisphosphonate-loaded micro-arc oxidation coating for biodegradable magnesium alloy pellets inhibits osteosarcoma through targeting of the mevalonate pathway. Acta Biomater. 2021, 121, 682–694. [Google Scholar] [CrossRef]
- Panthi, V.K.; Dua, K.; Singh, S.K.; Gupta, G.; Hansbro, P.M.; Paudel, K.R. Nanoformulations-Based Metronomic Chemotherapy: Mechanism, Challenges, Recent Advances, and Future Perspectives. Pharmaceutics 2023, 15, 1192. [Google Scholar] [CrossRef]
- Parra, E.; Pérez-Gil, J. Composition, structure and mechanical properties define performance of pulmonary surfactant membranes and films. Chem. Phys. Lipids 2015, 185, 153–175. [Google Scholar] [CrossRef] [PubMed]
- García-Díaz, M.; Birch, D.; Wan, F.; Nielsen, H.M. The role of mucus as an invisible cloak to transepithelial drug delivery by nanoparticles. Adv. Drug Deliv. Rev. 2018, 124, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Wan, F.; Nylander, T.; Foged, C.; Yang, M.; Baldursdottir, S.G.; Nielsen, H.M. Qualitative and quantitative analysis of the biophysical interaction of inhaled nanoparticles with pulmonary surfactant by using quartz crystal microbalance with dissipation monitoring. J. Colloid. Interface Sci. 2019, 545, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Flemming, H.C.; Wingender, J. The biofilm matrix. Nat. Rev. Microbiol. 2010, 8, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Ciofu, O.; Tolker-Nielsen, T.; Jensen, P.; Wang, H.; Høiby, N. Antimicrobial resistance, respiratory tract infections and role of biofilms in lung infections in cystic fibrosis patients. Adv. Drug Deliv. Rev. 2015, 85, 7–23. [Google Scholar] [CrossRef]
- Panthi, V.K.; Jha, S.K.; Chaubey, R.; Pangeni, R. Formulation and development of Serratiopeptidase enteric coated tablets and analytical method validation by UV Spectroscopy. Int. J. Anal. Chem. 2021, 2021, 9749474. [Google Scholar] [CrossRef] [PubMed]
- Panthi, V.K.; Fairfull-Smith, K.E.; Islam, N. Liposomal drug delivery strategies to eradicate bacterial biofilms: Challenges, recent advances, and future perspectives. Int. J. Pharm. 2024, 655, 124046. [Google Scholar] [CrossRef] [PubMed]
- Kamaruzzaman, N.F.; Kendall, S.; Good, L. Targeting the hard to reach: Challenges and novel strategies in the treatment of intracellular bacterial infections. Br. J. Pharmacol. 2017, 174, 2225–2236. [Google Scholar] [CrossRef] [PubMed]
- Panthi, V.K.; Jha, S.K.; Pangeni, R.; Paudel, K.R.; Wang, R. Formulation and Development of Adapalene Topical Nanohydrogel Using Different Surfactants and Cosurfactants for Antiacne Activity: In Vitro and Ex Vivo Evaluation. J. Nanomater. 2022, 2022, 19. [Google Scholar] [CrossRef]
- Watson, R.O.; Manzanillo, P.S.; Cox, J.S. Extracellular M. tuberculosis DNA targets bacteria for autophagy by activating the host DNA-sensing pathway. Cell 2012, 150, 803–815. [Google Scholar] [CrossRef]
- Abed, N.; Couvreur, P. Nanocarriers for antibiotics: A promising solution to treat intracellular bacterial infections. Int. J. Antimicrob. Agents 2014, 43, 485–496. [Google Scholar] [CrossRef]
- Ladavière, C.; Gref, R. Toward an optimized treatment of intracellular bacterial infections: Input of nanoparticulate drug delivery systems. Nanomedicine 2015, 10, 3033–3055. [Google Scholar] [CrossRef]
- Tokimatsu, I.; Hiramatsu, K.; Morimoto, T.; Imai, H.; Suzaki, Y.; Stass, H.; Okumura, K.; Kadota, J. Safety, tolerability and pharmacokinetics of a single dose of ciprofloxacin dry powder for inhalation in Japanese patients with mild to moderate chronic obstructive pulmonary disease: A randomized controlled trial. In B46. Inhaled and Systemic Anti-Inflammatory Therapy in Copd; American Thoracic Society: San Diego, CA, USA, 2011; p. A3105. [Google Scholar]
- Liao, X.; Li, B.; Zou, R.; Dai, Y.; Xie, S.; Yuan, B. Biodegradation of antibiotic ciprofloxacin: Pathways, influential factors, and bacterial community structure. Environ. Sci. Pollut. Res. 2016, 23, 7911–7918. [Google Scholar] [CrossRef]
- Stass, H.; Nagelschmitz, J.; Kappeler, D.; Weimann, B. Lung deposition of Ciprofloxacin Dry Powder for Inhalation in healthy subjects and patients suffering from chronic obstructive pulmonary disease or non-cystic fibrosis bronchiectasis. In A43. Chronic Obstructive Pulmonary Disease Treatment: Novel Agents and Safety Studies; American Thoracic Society: San Diego, CA, USA, 2013; p. A1507. [Google Scholar]
- Schwarz, C. Colobreathe® for the treatment of cystic fibrosis-associated pulmonary infections. Pulm. Ther. 2015, 1, 19–30. [Google Scholar] [CrossRef]
- Pleasants, R.A.; Hess, D.R. Aerosol Delivery Devices for Obstructive Lung Diseases. Respir. Care 2018, 63, 708–733. [Google Scholar] [CrossRef]
- Mishra, B.; Singh, J. Novel drug delivery systems and significance in respiratory diseases. In Targeting Chronic Inflammatory Lung Diseases Using Advanced Drug Delivery Systems; Academic Press: Cambridge, MA, USA, 2020; pp. 57–95. [Google Scholar] [CrossRef]
- Hess, D.R. Aerosol delivery devices in the treatment of asthma. Respir. Care 2008, 53, 699–723; discussion 723–725. [Google Scholar]
- Liu, C.; Lin, L.; Huang, Z.; Wu, Q.; Jiang, J.; Lv, L.; Yu, X.; Quan, G.; Li, G.; Wu, C. Novel Inhalable Ciprofloxacin Dry Powders for Bronchiectasis Therapy: Mannitol-Silk Fibroin Binary Microparticles with High-Payload and Improved Aerosolized Properties. AAPS PharmSciTech 2019, 20, 85. [Google Scholar] [CrossRef]
- Guo, Y.; Bera, H.; Shi, C.; Zhang, L.; Cun, D.; Yang, M. Pharmaceutical strategies to extend pulmonary exposure of inhaled medicines. Acta Pharm. Sin. B 2021, 11, 2565–2584. [Google Scholar] [CrossRef]
- Panthi, V.K.; Imran, M.; Chaudhary, A.; Paudel, K.R.; Mohammed, Y. The significance of quercetin-loaded advanced nanoformulations for the management of diabetic wounds. Nanomedicine 2023, 18, 391–411. [Google Scholar] [CrossRef]
- Cipolla, D.; Wu, H.; Eastman, S.; Redelmeier, T.; Gonda, I.; Chan, H.K. Development and characterization of an in vitro release assay for liposomal ciprofloxacin for inhalation. J. Pharm. Sci. 2014, 103, 314–327. [Google Scholar] [CrossRef]
- Ong, H.X.; Benaouda, F.; Traini, D.; Cipolla, D.; Gonda, I.; Bebawy, M.; Forbes, B.; Young, P.M. In vitro and ex vivo methods predict the enhanced lung residence time of liposomal ciprofloxacin formulations for nebulisation. Eur. J. Pharm. Biopharm. 2014, 86, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.X.; Traini, D.; Cipolla, D.; Gonda, I.; Bebawy, M.; Agus, H.; Young, P.M. Liposomal nanoparticles control the uptake of ciprofloxacin across respiratory epithelia. Pharm. Res. 2012, 29, 3335–3346. [Google Scholar] [CrossRef]
- Chono, S.; Tanino, T.; Seki, T.; Morimoto, K. Efficient drug targeting to rat alveolar macrophages by pulmonary administration of ciprofloxacin incorporated into mannosylated liposomes for treatment of respiratory intracellular parasitic infections. J. Control Release 2008, 127, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Shi, J.; Dai, Q.; Yin, X.; Zhang, X.; Zheng, A. In-vitro and in-vivo evaluation of ciprofloxacin liposomes for pulmonary administration. Drug Dev. Ind. Pharm. 2015, 41, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wong, C.Y.J.; Gholizadeh, H.; Aluigi, A.; Tiboni, M.; Casettari, L.; Young, P.; Traini, D.; Li, M.; Cheng, S.; et al. Microfluidics assembly of inhalable liposomal ciprofloxacin characterised by an innovative in vitro pulmonary model. Int. J. Pharm. 2023, 635, 122667. [Google Scholar] [CrossRef] [PubMed]
- Haworth, C.; Wanner, A.; Froehlich, J.; O’Neal, T.; Davis, A.; Gonda, I.; O’Donnell, A. Inhaled liposomal ciprofloxacin in patients with bronchiectasis and chronic Pseudomonas aeruginosa infection: Results from two parallel phase III trials (ORBIT-3 and-4). In B14. Clinical Trials Across Pulmonary Disease; American Thoracic Society: San Diego, CA, USA, 2017; p. A7604. [Google Scholar]
- Maselli, D.J.; Keyt, H.; Restrepo, M.I. Inhaled Antibiotic Therapy in Chronic Respiratory Diseases. Int. J. Mol. Sci. 2017, 18, 1062. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, K.; Togami, K.; Yamamoto, E.; Wang, S.; Morimoto, K.; Itagaki, S.; Chono, S. Sustained distribution of aerosolized PEGylated liposomes in epithelial lining fluids on alveolar surfaces. Drug Deliv. Transl. Res. 2016, 6, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Ngan, C.L.; Asmawi, A.A. Lipid-based pulmonary delivery system: A review and future considerations of formulation strategies and limitations. Drug Deliv. Transl. Res. 2018, 8, 1527–1544. [Google Scholar] [CrossRef] [PubMed]
- Panthi, V.K.; Bashyal, S.; Paudel, K.R. Docetaxel-loaded nanoformulations delivery for breast cancer management: Challenges, recent advances, and future perspectives. J. Drug Deliv. Sci. Technol. 2024, 92, 105314. [Google Scholar] [CrossRef]
- Chen, M.; Xie, S.; Wei, J.; Song, X.; Ding, Z.; Li, X. Antibacterial Micelles with Vancomycin-Mediated Targeting and pH/Lipase-Triggered Release of Antibiotics. ACS Appl. Mater. Interfaces 2018, 10, 36814–36823. [Google Scholar] [CrossRef]
- Stancheva, R.; Paunova-Krasteva, T.; Topouzova-Hristova, T.; Stoitsova, S.; Petrov, P.; Haladjova, E. Ciprofloxacin-Loaded Mixed Polymeric Micelles as Antibiofilm Agents. Pharmaceutics 2023, 15, 1147. [Google Scholar] [CrossRef] [PubMed]
- Milović, N.M.; Wang, J.; Lewis, K.; Klibanov, A.M. Immobilized N-alkylated polyethylenimine avidly kills bacteria by rupturing cell membranes with no resistance developed. Biotechnol. Bioeng. 2005, 90, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ren, Y.; Li, Y.; Su, L.; Zhang, Y.; Huang, F.; Liu, J.; Liu, J.; van Kooten, T.G.; An, Y.; et al. Nanocarriers with conjugated antimicrobials to eradicate pathogenic biofilms evaluated in murine in vivo and human ex vivo infection models. Acta Biomater. 2018, 79, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Leng, M.; Hu, S.; Lu, A.; Cai, M.; Luo, X. The anti-bacterial poly (caprolactone)-poly (quaternary ammonium salt) as drug delivery carriers. Appl. Microbiol. Biotechnol. 2016, 100, 3049–3059. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, K.B.; Northeved, H.; Kumar, P.E.; Permin, A.; Gjetting, T.; Andresen, T.L.; Larsen, S.; Wegener, K.M.; Lykkesfeldt, J.; Jantzen, K.; et al. In vivo toxicity of cationic micelles and liposomes. Nanomedicine 2015, 11, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Farhangi, M.; Mahboubi, A.; Kobarfard, F.; Vatanara, A.; Mortazavi, S.A. Optimization of a dry powder inhaler of ciprofloxacin-loaded polymeric nanomicelles by spray drying process. Pharm. Dev. Technol. 2019, 24, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Chiang, P.C.; Alsup, J.W.; Lai, Y.; Hu, Y.; Heyde, B.R.; Tung, D. Evaluation of Aerosol Delivery of Nanosuspension for Pre-clinical Pulmonary Drug Delivery. Nanoscale Res. Lett. 2009, 4, 254–261. [Google Scholar] [CrossRef]
- Liu, Y.; Ma, Y.; Xue, L.; Guan, W.; Wang, Y. Pulmonary multidrug codelivery of curcumin nanosuspensions and ciprofloxacin with N-acetylcysteine for lung infection therapy. J. Drug Deliv. Sci. Technol. 2023, 84, 104474. [Google Scholar] [CrossRef]
- Ingle, A.P.; Shende, S.; Pandit, R.; Paralikar, P.; Tikar, S.; Kon, K.; Rai, M. Chapter 15—Nanotechnological applications for the control of pulmonary infections. In The Microbiology of Respiratory System Infections; Kon, K., Rai, M., Eds.; Academic Press: Cambridge, MA, USA, 2016; Volume 1, pp. 223–235. [Google Scholar]
- Manimekalai, P.; Manavalan, R. Selection of excipients for the formulation of Ceftriaxone sodium loaded chitosan nanoparticle through drug-excipient compatibility testing. Int. J. PharmTech Res. 2015, 8, 5–10. [Google Scholar]
- Rasul, R.M.; Tamilarasi Muniandy, M.; Zakaria, Z.; Shah, K.; Chee, C.F.; Dabbagh, A.; Rahman, N.A.; Wong, T.W. A review on chitosan and its development as pulmonary particulate anti-infective and anti-cancer drug carriers. Carbohydr. Polym. 2020, 250, 116800. [Google Scholar] [CrossRef]
- Egorov, A.R.; Kurasova, M.N.; Khubiev, O.; Bogdanov, N.A.; Tskhovrebov, A.G.; Kirichuk, A.A.; Khrustalev, V.N.; Rubanik, V.V.; Rubanik, V.V.; Kritchenkov, A.S. Ciprofloxacin chitosan conjugate: Combined antibacterial effect and low toxicity. Mendeleev Commun. 2022, 32, 774–776. [Google Scholar] [CrossRef]
- Egorov, A.R.; Kirichuk, A.A.; Rubanik, V.V.; Rubanik, V.V.; Tskhovrebov, A.G.; Kritchenkov, A.S. Chitosan and Its Derivatives: Preparation and Antibacterial Properties. Materials 2023, 16, 6076. [Google Scholar] [CrossRef] [PubMed]
- Amani, A.; York, P.; Chrystyn, H.; Clark, B.J. Evaluation of a nanoemulsion-based formulation for respiratory delivery of budesonide by nebulizers. AAPS PharmSciTech 2010, 11, 1147–1151. [Google Scholar] [CrossRef]
- Shah, K.; Chan, L.W.; Wong, T.W. Critical physicochemical and biological attributes of nanoemulsions for pulmonary delivery of rifampicin by nebulization technique in tuberculosis treatment. Drug Deliv. 2017, 24, 1631–1647. [Google Scholar] [CrossRef]
- Pangeni, R.; Choi, J.U.; Panthi, V.K.; Byun, Y.; Park, J.W. Enhanced oral absorption of pemetrexed by ion-pairing complex formation with deoxycholic acid derivative and multiple nanoemulsion formulations: Preparation, characterization, and in vivo oral bioavailability and anticancer effect. Int. J. Nanomed. 2018, 13, 3329–3351. [Google Scholar] [CrossRef] [PubMed]
- Kucukoglu, V.; Uzuner, H.; Kenar, H.; Karadenizli, A. In vitro antibacterial activity of ciprofloxacin loaded chitosan microparticles and their effects on human lung epithelial cells. Int. J. Pharm. 2019, 569, 118578. [Google Scholar] [CrossRef]
- Sobhani, Z.; Mohammadi Samani, S.; Montaseri, H.; Khezri, E. Nanoparticles of Chitosan Loaded Ciprofloxacin: Fabrication and Antimicrobial Activity. Adv. Pharm. Bull. 2017, 7, 427–432. [Google Scholar] [CrossRef]
- Marei, N.; Elwahy, A.H.M.; Salah, T.A.; El Sherif, Y.; El-Samie, E.A. Enhanced antibacterial activity of Egyptian local insects’ chitosan-based nanoparticles loaded with ciprofloxacin-HCl. Int. J. Biol. Macromol. 2019, 126, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Alhajj, N.; Zakaria, Z.; Naharudin, I.; Ahsan, F.; Li, W.; Wong, T.W. Critical physicochemical attributes of chitosan nanoparticles admixed lactose-PEG 3000 microparticles in pulmonary inhalation. Asian J. Pharm. Sci. 2020, 15, 374–384. [Google Scholar] [CrossRef]
- Egorov, A.R.; Kurliuk, A.V.; Rubanik, V.V.; Kirichuk, A.A.; Khubiev, O.; Golubev, R.; Lobanov, N.N.; Tskhovrebov, A.G.; Kritchenkov, A.S. Chitosan-Based Ciprofloxacin Extended Release Systems: Combined Synthetic and Pharmacological (In Vitro and In Vivo) Studies. Molecules 2022, 27, 8865. [Google Scholar] [CrossRef]
- Shazly, G.A. Ciprofloxacin Controlled-Solid Lipid Nanoparticles: Characterization, In Vitro Release, and Antibacterial Activity Assessment. BioMed Res. Int. 2017, 2017, 2120734. [Google Scholar] [CrossRef] [PubMed]
- Torge, A.; Wagner, S.; Chaves, P.S.; Oliveira, E.G.; Guterres, S.S.; Pohlmann, A.R.; Titz, A.; Schneider, M.; Beck, R.C.R. Ciprofloxacin-loaded lipid-core nanocapsules as mucus penetrating drug delivery system intended for the treatment of bacterial infections in cystic fibrosis. Int. J. Pharm. 2017, 527, 92–102. [Google Scholar] [CrossRef]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Solid lipid nanoparticles and nanostructured lipid carriers as novel drug delivery systems: Applications, advantages and disadvantages. Res. Pharm. Sci. 2018, 13, 288–303. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Meng, J.; Cao, L.; Li, Y.; Deng, P.; Pan, P.; Hu, C.; Yang, H. Synthesis and investigations of ciprofloxacin loaded engineered selenium lipid nanocarriers for effective drug delivery system for preventing lung infections of interstitial lung disease. J. Photochem. Photobiol. B Biol. 2019, 197, 111510. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Vena, A.; Russo, A.; Peghin, M. Inhaled Liposomal Antimicrobial Delivery in Lung Infections. Drugs 2020, 80, 1309–1318. [Google Scholar] [CrossRef] [PubMed]
- Serisier, D.J.; Bilton, D.; De Soyza, A.; Thompson, P.J.; Kolbe, J.; Greville, H.W.; Cipolla, D.; Bruinenberg, P.; Gonda, I.; ORBIT-2 Investigators. Inhaled, dual release liposomal ciprofloxacin in non-cystic fibrosis bronchiectasis (ORBIT-2): A randomised, double-blind, placebo-controlled trial. Thorax 2013, 68, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Rubin, B.K. Aerosolized antibiotics for non-cystic fibrosis bronchiectasis. J. Aerosol Med. Pulm. Drug Deliv. 2008, 21, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Smith, M.P.; McHugh, B.J.; Doherty, C.; Govan, J.R.; Hill, A.T. Short- and long-term antibiotic treatment reduces airway and systemic inflammation in non-cystic fibrosis bronchiectasis. Am. J. Respir. Crit. Care Med. 2012, 186, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Haworth, C.S.; Bilton, D.; Chalmers, J.D.; Davis, A.M.; Froehlich, J.; Gonda, I.; Thompson, B.; Wanner, A.; O’Donnell, A.E. Inhaled liposomal ciprofloxacin in patients with non-cystic fibrosis bronchiectasis and chronic lung infection with Pseudomonas aeruginosa (ORBIT-3 and ORBIT-4): Two phase 3, randomised controlled trials. Lancet Respir. Med. 2019, 7, 213–226. [Google Scholar] [CrossRef]
- Ciuca, I.M.; Marian, P.; Monica, M. Biomarkers in Cystic Fibrosis Lung Disease—A Review. Rom. J. Anaesth. Intensive Care 2020, 27, 34–36. [Google Scholar] [CrossRef]
- Su, Y.B.; Tang, X.K.; Zhu, L.P.; Yang, K.X.; Pan, L.; Li, H.; Chen, Z.G. Enhanced Biosynthesis of Fatty Acids Contributes to Ciprofloxacin Resistance in Pseudomonas aeruginosa. Front. Microbiol. 2022, 13, 845173. [Google Scholar] [CrossRef]
- Yu, S.; Wang, S.; Zou, P.; Chai, G.; Lin, Y.W.; Velkov, T.; Li, J.; Pan, W.; Zhou, Q.T. Inhalable liposomal powder formulations for co-delivery of synergistic ciprofloxacin and colistin against multi-drug resistant gram-negative lung infections. Int. J. Pharm. 2020, 575, 118915. [Google Scholar] [CrossRef]
- Chai, G.; Park, H.; Yu, S.; Zhou, F.; Li, J.; Xu, Q.; Zhou, Q.T. Evaluation of co-delivery of colistin and ciprofloxacin in liposomes using an in vitro human lung epithelial cell model. Int. J. Pharm. 2019, 569, 118616. [Google Scholar] [CrossRef]
- Almurshedi, A.S.; Aljunaidel, H.A.; Alquadeib, B.; Aldosari, B.N.; Alfagih, I.M.; Almarshidy, S.S.; Eltahir, E.K.D.; Mohamoud, A.Z. Development of Inhalable Nanostructured Lipid Carriers for Ciprofloxacin for Noncystic Fibrosis Bronchiectasis Treatment. Int. J. Nanomed. 2021, 16, 2405–2417. [Google Scholar] [CrossRef]
- Al-Obaidi, H.; Kalgudi, R.; Zariwala, M.G. Fabrication of inhaled hybrid silver/ciprofloxacin nanoparticles with synergetic effect against Pseudomonas aeruginosa. Eur. J. Pharm. Biopharm. 2018, 128, 27–35. [Google Scholar] [CrossRef]
- Tran, T.-T.; Vidaillac, C.; Lee, V.Y.F.; Chandrasekaran, R.; Lim, A.; Low, T.; Tan, G.; Abisheganaden, J.; Koh, M.; Teo, J.; et al. Inhalable Ciprofloxacin-Nanoplex (CIP-Np) combined with mannitol as a novel bronchiectasis therapeutic. Eur. Respir. J. 2017, 50, PA4120. [Google Scholar] [CrossRef]
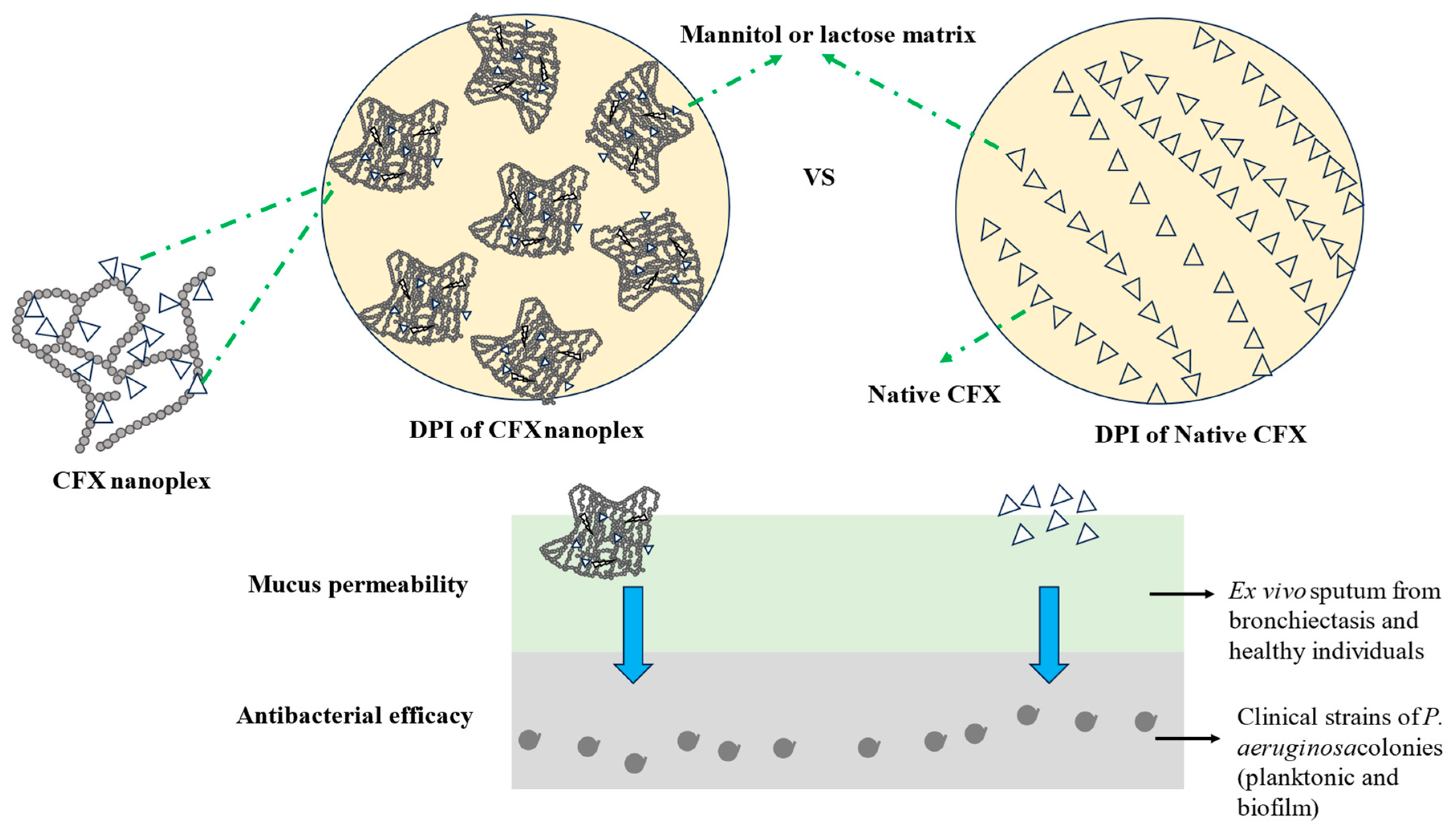
- Tran, T.T.; Vidaillac, C.; Yu, H.; Yong, V.F.L.; Roizman, D.; Chandrasekaran, R.; Lim, A.Y.H.; Low, T.B.; Tan, G.L.; Abisheganaden, J.A.; et al. A new therapeutic avenue for bronchiectasis: Dry powder inhaler of ciprofloxacin nanoplex exhibits superior ex vivo mucus permeability and antibacterial efficacy to its native ciprofloxacin counterpart. Int. J. Pharm. 2018, 547, 368–376. [Google Scholar] [CrossRef]
- Gunday Tureli, N.; Torge, A.; Juntke, J.; Schwarz, B.C.; Schneider-Daum, N.; Tureli, A.E.; Lehr, C.M.; Schneider, M. Ciprofloxacin-loaded PLGA nanoparticles against cystic fibrosis P. aeruginosa lung infections. Eur. J. Pharm. Biopharm. 2017, 117, 363–371. [Google Scholar] [CrossRef]
- Hamblin, K.A.; Armstrong, S.J.; Barnes, K.B.; Davies, C.; Laws, T.; Blanchard, J.D.; Harding, S.V.; Atkins, H.S. Inhaled Liposomal Ciprofloxacin Protects against a Lethal Infection in a Murine Model of Pneumonic Plague. Front. Microbiol. 2017, 8, 91. [Google Scholar] [CrossRef] [PubMed]
- Tewes, F.; Lamy, B.; Laroche, J.; Lamarche, I.; Marchand, S. PK-PD Evaluation of Inhaled Microparticles loaded with Ciprofloxacin-Copper complex in a Rat Model of Chronic Pseudomonas aeruginosa Lung Infection. Int. J. Pharm. X 2023, 5, 100178. [Google Scholar] [CrossRef] [PubMed]
- Tewes, F.; Brillault, J.; Lamy, B.; O’Connell, P.; Olivier, J.-C.; Couet, W.; Healy, A.M. Ciprofloxacin-Loaded Inorganic–Organic Composite Microparticles To Treat Bacterial Lung Infection. Mol. Pharm. 2016, 13, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Chang, R.Y.K.; Britton, W.J.; Morales, S.; Kutter, E.; Li, J.; Chan, H.K. Inhalable combination powder formulations of phage and ciprofloxacin for P. aeruginosa respiratory infections. Eur. J. Pharm. Biopharm. 2019, 142, 543–552. [Google Scholar] [CrossRef]
- Arauzo, B.; Lobera, M.P.; Monzon, A.; Santamaria, J. Dry powder formulation for pulmonary infections: Ciprofloxacin loaded in chitosan sub-micron particles generated by electrospray. Carbohydr. Polym. 2021, 273, 118543. [Google Scholar] [CrossRef] [PubMed]
- Karimi, K.; Pallagi, E.; Szabo-Revesz, P.; Csoka, I.; Ambrus, R. Development of a microparticle-based dry powder inhalation formulation of ciprofloxacin hydrochloride applying the quality by design approach. Drug Des. Devel Ther. 2016, 10, 3331–3343. [Google Scholar] [CrossRef]
- Xu, Z.; Bera, H.; Wang, H.; Wang, J.; Cun, D.; Feng, Y.; Yang, M. Inhalable ciprofloxacin/polymyxin B dry powders in respiratory infection therapy. Acta Mater. Medica 2023, 2, 142–156. [Google Scholar] [CrossRef]
- Wang, J.; Stegger, M.; Moodley, A.; Yang, M. Drug Combination of Ciprofloxacin and Polymyxin B for the Treatment of Multidrug-Resistant Acinetobacter baumannii Infections: A Drug Pair Limiting the Development of Resistance. Pharmaceutics 2023, 15, 720. [Google Scholar] [CrossRef] [PubMed]
- Chono, S.; Tanino, T.; Seki, T.; Morimoto, K. Efficient drug delivery to alveolar macrophages and lung epithelial lining fluid following pulmonary administration of liposomal ciprofloxacin in rats with pneumonia and estimation of its antibacterial effects. Drug Dev. Ind. Pharm. 2008, 34, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Shetty, N.; Ahn, P.; Park, H.; Bhujbal, S.; Zemlyanov, D.; Cavallaro, A.; Mangal, S.; Li, J.; Zhou, Q.T. Improved Physical Stability and Aerosolization of Inhalable Amorphous Ciprofloxacin Powder Formulations by Incorporating Synergistic Colistin. Mol. Pharm. 2018, 15, 4004–4020. [Google Scholar] [CrossRef]
- Akdag Cayli, Y.; Sahin, S.; Buttini, F.; Balducci, A.G.; Montanari, S.; Vural, I.; Oner, L. Dry powders for the inhalation of ciprofloxacin or levofloxacin combined with a mucolytic agent for cystic fibrosis patients. Drug Dev. Ind. Pharm. 2017, 43, 1378–1389. [Google Scholar] [CrossRef]
- Alhajj, N.; O’Reilly, N.J.; Cathcart, H. Development and characterization of a spray-dried inhalable ciprofloxacin-quercetin co-amorphous system. Int. J. Pharm. 2022, 618, 121657. [Google Scholar] [CrossRef]
- Dorkin, H.L.; Staab, D.; Operschall, E.; Alder, J.; Criollo, M. Ciprofloxacin DPI: A randomised, placebo-controlled, phase IIb efficacy and safety study on cystic fibrosis. BMJ Open Respir. Res. 2015, 2, e000100. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Cipolla, D.; Thompson, B.; Davis, A.M.; O’Donnell, A.; Tino, G.; Gonda, I.; Haworth, C.; Froehlich, J. Changes in respiratory symptoms during 48-week treatment with ARD-3150 (inhaled liposomal ciprofloxacin) in bronchiectasis: Results from the ORBIT-3 and -4 studies. Eur. Respir. J. 2020, 56, 2000110. [Google Scholar] [CrossRef]
- Soyza, A.D.; Aksamit, T.; Bandel, T.-J.; Criollo, M.; Elborn, J.S.; Operschall, E.; Polverino, E.; Roth, K.; Winthrop, K.L.; Wilson, R. RESPIRE 1: A phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur. Respir. J. 2018, 51, 1702052. [Google Scholar] [CrossRef]
- Aksamit, T.; Soyza, A.D.; Bandel, T.-J.; Criollo, M.; Elborn, J.S.; Operschall, E.; Polverino, E.; Roth, K.; Winthrop, K.L.; Wilson, R. RESPIRE 2: A phase III placebo-controlled randomised trial of ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis. Eur. Respir. J. 2018, 51, 1702053. [Google Scholar] [CrossRef]
- Bilton, D.; Henig, N.; Morrissey, B.; Gotfried, M. Addition of inhaled tobramycin to ciprofloxacin for acute exacerbations of Pseudomonas aeruginosa infection in adult bronchiectasis. Chest 2006, 130, 1503–1510. [Google Scholar] [CrossRef]
- Bilton, D.; Serisier, D.J.; Soyza, A.T.D.; Wolfe, R.; Bruinenberg, P. Multicenter, randomized, double-blind, placebo-controlled study (ORBIT 1) to evaluate the efficacy, safety, and tolerability of once daily ciprofloxacin for inhalation in the management of pseudomonas aeruginosa infections in patients with non-cystic fibrosis bronchiectasis. Eur. Respir. J. 2011, 38, 1925. [Google Scholar]
- Ho, D.-K.; Nichols, B.L.B.; Edgar, K.J.; Murgia, X.; Loretz, B.; Lehr, C.-M. Challenges and strategies in drug delivery systems for treatment of pulmonary infections. Eur. J. Pharm. Biopharm. 2019, 144, 110–124. [Google Scholar] [CrossRef]
- Wauthoz, N.; Amighi, K. Formulation strategies for pulmonary delivery of poorly soluble drugs. In Pulmonary Drug Delivery; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 87–122. [Google Scholar]
- Fröhlich, E.; Mercuri, A.; Wu, S.; Salar-Behzadi, S. Measurements of deposition, lung surface area and lung fluid for simulation of inhaled compounds. Front. Pharmacol. 2016, 7, 181. [Google Scholar] [CrossRef]
- Hastedt, J.E.; Bäckman, P.; Clark, A.R.; Doub, W.; Hickey, A.; Hochhaus, G.; Kuehl, P.J.; Lehr, C.-M.; Mauser, P.; McConville, J. Scope and Relevance of a Pulmonary Biopharmaceutical Classification System. In Proceedings of the AAPS/FDA/USP Workshop, Baltimore, MD, USA, 16–17 March 2015; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Tolker-Nielsen, T. Pseudomonas aeruginosa biofilm infections: From molecular biofilm biology to new treatment possibilities. Apmis 2014, 122, 1–51. [Google Scholar] [CrossRef] [PubMed]
- Mesallati, H.; Tajber, L. Polymer/amorphous salt solid dispersions of ciprofloxacin. Pharm. Res. 2017, 34, 2425–2439. [Google Scholar] [CrossRef] [PubMed]
- Shetty, N.; Zeng, L.; Mangal, S.; Nie, H.; Rowles, M.R.; Guo, R.; Han, Y.; Park, J.H.; Zhou, Q. Effects of moisture-induced crystallization on the aerosol performance of spray dried amorphous ciprofloxacin powder formulations. Pharm. Res. 2018, 35, 7. [Google Scholar] [CrossRef] [PubMed]
- Dhanani, J.; Fraser, J.F.; Chan, H.K.; Rello, J.; Cohen, J.; Roberts, J.A. Fundamentals of aerosol therapy in critical care. Crit. Care 2016, 20, 269. [Google Scholar] [CrossRef] [PubMed]
- Antonela Antoniu, S. Inhaled ciprofloxacin for chronic airways infections caused by Pseudomonas aeruginosa. Expert Rev. Anti-Infect. Ther. 2012, 10, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Alhajj, N.; O’Reilly, N.J.; Cathcart, H. Developing ciprofloxacin dry powder for inhalation: A story of challenges and rational design in the treatment of cystic fibrosis lung infection. Int. J. Pharm. 2022, 613, 121388. [Google Scholar] [CrossRef]
- Lin, Y.; Quan, D.; Chang, R.Y.K.; Chow, M.Y.T.; Wang, Y.; Li, M.; Morales, S.; Britton, W.J.; Kutter, E.; Li, J.; et al. Synergistic activity of phage PEV20-ciprofloxacin combination powder formulation-A proof-of-principle study in a P. aeruginosa lung infection model. Eur. J. Pharm. Biopharm. 2021, 158, 166–171. [Google Scholar] [CrossRef]
- Lin, L.; Zhou, Y.; Quan, G.; Pan, X.; Wu, C. The rough inhalable ciprofloxacin hydrochloride microparticles based on silk fibroin for non-cystic fibrosis bronchiectasis therapy with good biocompatibility. Int. J. Pharm. 2021, 607, 120974. [Google Scholar] [CrossRef] [PubMed]
- Stass, H.; Nagelschmitz, J.; Kappeler, D.; Sommerer, K.; Kietzig, C.; Weimann, B. Ciprofloxacin dry powder for inhalation in patients with non-cystic fibrosis bronchiectasis or chronic obstructive pulmonary disease, and in healthy volunteers. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhang, A.; Yao, X. Meta-analysis of efficacy and safety of inhaled ciprofloxacin in non-cystic fibrosis bronchiectasis patients. Intern. Med. J. 2021, 51, 1505–1512. [Google Scholar] [CrossRef]
- Amaro, R.; Panagiotarakou, M.; Alcaraz, V.; Torres, A. The efficacy of inhaled antibiotics in non-cystic fibrosis bronchiectasis. Expert Rev. Respir. Med. 2018, 12, 683–691. [Google Scholar] [CrossRef]
- Miller, D.P.; Tan, T.; Nakamura, J.; Malcolmson, R.J.; Tarara, T.E.; Weers, J.G. Physical characterization of tobramycin inhalation powder: II. State diagram of an amorphous engineered particle formulation. Mol. Pharm. 2017, 14, 1950–1960. [Google Scholar] [CrossRef]
- Justo, J.A.; Danziger, L.H.; Gotfried, M.H. Efficacy of inhaled ciprofloxacin in the management of non-cystic fibrosis bronchiectasis. Ther. Adv. Respir. Dis. 2013, 7, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Plaunt, A.J.; Nguyen, T.L.; Corboz, M.R.; Malinin, V.S.; Cipolla, D.C. Strategies to Overcome Biological Barriers Associated with Pulmonary Drug Delivery. Pharmaceutics 2022, 14, 302. [Google Scholar] [CrossRef] [PubMed]
- Akkerman-Nijland, A.M.; Akkerman, O.W.; Grasmeijer, F.; Hagedoorn, P.; Frijlink, H.W.; Rottier, B.L.; Koppelman, G.H.; Touw, D.J. The pharmacokinetics of antibiotics in cystic fibrosis. Expert Opin. Drug Metab. Toxicol. 2021, 17, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Pangeni, R.; Panthi, V.K.; Yoon, I.S.; Park, J.W. Preparation, Characterization, and In Vivo Evaluation of an Oral Multiple Nanoemulsive System for Co-Delivery of Pemetrexed and Quercetin. Pharmaceutics 2018, 10, 158. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Incorporated | Formulation Type | Bacterial Strain | Major Findings | Ref. |
|---|---|---|---|---|
| CFX and colistin | Liposomal powder | P. aeruginosa | Remarkable antibacterial effectiveness | [97] |
| CFX and colistin | Liposomal powder | P. aeruginosa | Enhanced drug retention on the lung epithelial surfaces | [98] |
| CFX | Nanostructured lipid carriers | Significant amelioration in the FPF and higher FPD | [99] | |
| CFX | Silver nanoparticles | P. aeruginosa | Highly efficacious against impeding growth and biofilm formation | [100] |
| CFX | Dry powder | P. aeruginosa | Markedly higher antibacterial effect | [101] |
| CFX | Dry powder | Considerably higher mucus permeation and greater antibacterial effectiveness | [102] | |
| CFX | PLGA nanoparticles | P. aeruginosa | Improved effectiveness and noticeable reduction in mucus turbidity | [103] |
| CFX | Liposome | Yersinia pestis (Murine model of Pneumonic plaque) | Notable enhancement in survival Reduced bacterial load in the lungs and spleens | [104] |
| CFX | Liposome | Effectively regulated drug release | [58] | |
| CFX | Dry powder | Demonstrated superior performance in terms of aerosolization and increased drug content | [50] | |
| CFX-Cu2+ | Microparticles | P. aeruginosa (Rat model) | Significant reduction of lung burden of bacteria | [105] |
| CFX | Microparticles | P. aeruginosa S. aureus | Sustained drug levels in the lungs to obtain therapeutic effects | [106] |
| CFX | Spray-dried powder | Rat model | Exhibited rapid drug release rate and higher in vivo lung exposure | [6] |
| CFX | Nanoparticles | FPF enhanced proportionally with higher drug loading Proposed PEtOx is a potential carrier for LRTIs | [1] | |
| CFX and phage | Dry powder | P. aeruginosa | Demonstrated excellent synergistic antimicrobial killing efficacy and preserved bactericidal synergy | [107] |
| CFX | Sub-micron particles | P. aeruginosa and S. aureus | Revealed effective antimicrobial action Particles were biocompatible with A549 | [108] |
| CFX | Microparticle-based dry powder | Ameliorated aerosol performance | [109] | |
| CFX and PMB | Dry powder | P. aeruginosa | Maintained their ability to combat bacterial strain Good stability in solid-state form and suitable aerodynamic properties | [110] |
| CFX and PMB | Dry powder | A. baumannii | Efficaciously inhibited the emergence of resistance | [111] |
| CFX and curcumin | Nanosuspension-based dry powder | P. aeruginosa and S. aureus | Effective antibacterial effects and excellent release properties | [72] |
| CFX | Liposome | Rat model (Lipopolysaccharide-induced pneumonia) | CFX concentration in both AMs and lung ELF followed significantly higher time-courses compared to free CFX CFX concentration in plasma is lower than AMs and ELF | [112] |
| CFX and colistin | Dry powder | Elevated physical stability and aerosolization of amorphous inhalable CFX | [113] | |
| CFX with acetylcysteine and dornase alfa | Dry powder | Improved dissolution rates than untreated CFX | [114] | |
| CFX and quercetin | Spray-dried particles | Improved stability and better aerosol performance | [115] |
| Inhalable Formulation Type | Study Type | Disease Category | Major Findings | Ref. |
|---|---|---|---|---|
| Dry powder | Phase II, randomized double-blind, multicenter | Bronchiectasis | Well tolerated and remarkable reduction in total bacterial load | [23] |
| Dry powder | Phase I, single-dose, randomized, placebo-controlled | Chronic pulmonary infections | Well-tolerated with no detrimental implications on lung function evidenced clinically | [20] |
| Dry powder | Phase I, randomized, single-dose, dose-escalation | Cystic fibrosis | Well-tolerated and no instances of mortality | [19] |
| Dry powder | Phase I, randomized, dose-escalation | Cystic fibrosis | No serious detrimental effects, no notable changes in lung function measurements, and quickly absorbed | [18] |
| Dry powder | Phase I, randomized, single-blind design | Moderate to severe COPD | No occurrences of serious or severe detrimental effects, well-tolerated Elevated drug levels achieved in sputum | [17] |
| Liposome | Two phase III, randomized | Bronchiectasis and chronic lung infection | Significantly higher median duration than placebo group | [94] |
| Liposome | Phase II, randomized, double-blind, and placebo-controlled | Bronchiectasis | Decline in P. aeruginosa burden by day 28 and better tolerated | [91] |
| Dry powder | Placebo-controlled, randomized, phase IIb | Cystic fibrosis | No remarkable variations in primary efficacy endpoint but significant reduction in FEV1 reduction than placebo Positive impacts on sputum bacterial burden and well-being | [116] |
| Liposome | Two phase III, randomized | Bronchiectasis | Significant improvements in respiratory symptoms | [117] |
| Dry powder | Phase III, double-blind, placebo-controlled | Bronchiectasis | Remarkably extended the duration until the initial exacerbation than placebo Diminished the incidence of exacerbations | [118] |
| Dry powder | Phase III, placebo-controlled, randomized trial | Bronchiectasis | Revealed tendencies toward extending the duration before the initial exacerbation, diminished repetition of exacerbations, and well-tolerated | [119] |
| Solution (Tobramycin + CFX) | Double-blind, randomized, active comparator, parallel design | Bronchiectasis | Demonstrated greater microbiological response (against P. aeruginosa) | [120] |
| Dry powder | Multicenter, randomized, double-blind, placebo-controlled | Bronchiectasis | Well-tolerated and considerable mean reductions from baseline in P. aeruginosa CFUs at 28 days | [121] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panthi, V.K.; Fairfull-Smith, K.E.; Islam, N. Ciprofloxacin-Loaded Inhalable Formulations against Lower Respiratory Tract Infections: Challenges, Recent Advances, and Future Perspectives. Pharmaceutics 2024, 16, 648. https://doi.org/10.3390/pharmaceutics16050648
Panthi VK, Fairfull-Smith KE, Islam N. Ciprofloxacin-Loaded Inhalable Formulations against Lower Respiratory Tract Infections: Challenges, Recent Advances, and Future Perspectives. Pharmaceutics. 2024; 16(5):648. https://doi.org/10.3390/pharmaceutics16050648
Chicago/Turabian StylePanthi, Vijay Kumar, Kathryn E. Fairfull-Smith, and Nazrul Islam. 2024. "Ciprofloxacin-Loaded Inhalable Formulations against Lower Respiratory Tract Infections: Challenges, Recent Advances, and Future Perspectives" Pharmaceutics 16, no. 5: 648. https://doi.org/10.3390/pharmaceutics16050648
APA StylePanthi, V. K., Fairfull-Smith, K. E., & Islam, N. (2024). Ciprofloxacin-Loaded Inhalable Formulations against Lower Respiratory Tract Infections: Challenges, Recent Advances, and Future Perspectives. Pharmaceutics, 16(5), 648. https://doi.org/10.3390/pharmaceutics16050648