
Medication Lubricants for Oral Delivery of Drugs: Oral Processing Reduces Thickness, Changes Characteristics, and Improves Dissolution Profile

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Experimental Design
2.3. Sample Preparation
2.4. Oral Processing Effect
2.5. Drug release and Dissolution
2.6. Viscosity Measurements
2.7. Texture Features Measurements
3. Results
3.1. Dissolution Experiment
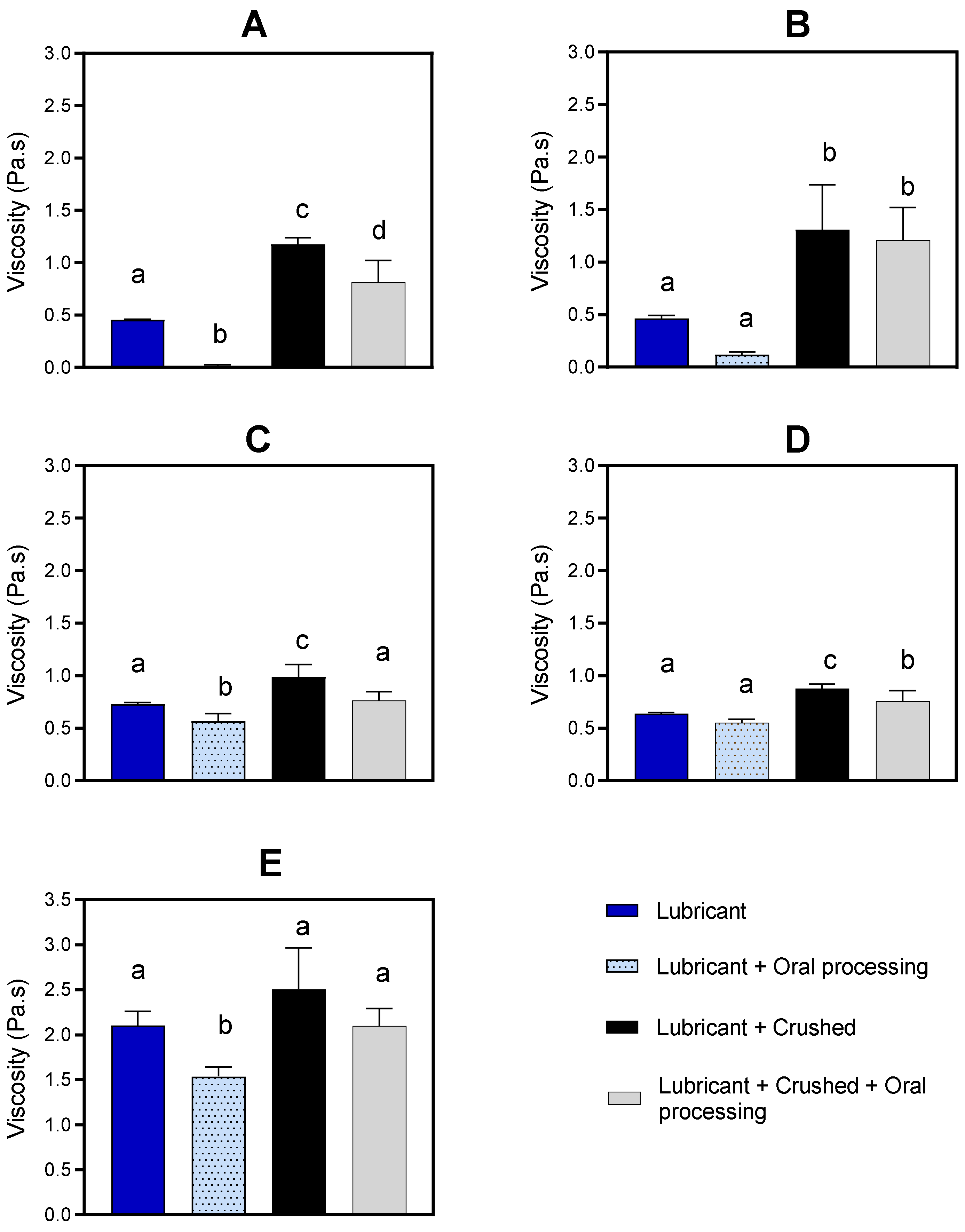
3.2. Viscosity Measurements
3.3. Texture Features Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buhmann, C.; Bihler, M.; Emich, K.; Hidding, U.; Pötter-Nerger, M.; Gerloff, C.; Niessen, A.; Flügel, T.; Koseki, J.-C.; Nienstedt, J.C.; et al. Pill Swallowing in Parkinson’s Disease: A Prospective Study Based on Flexible Endoscopic Evaluation of Swallowing. Park. Relat. D 2019, 62, 51–56. [Google Scholar] [CrossRef]
- Cicala, G.; Barbieri, M.A.; Spina, E.; De Leon, J. A Comprehensive Review of Swallowing Difficulties and Dysphagia Associated with Antipsychotics in Adults. Expert. Rev. Clin. Pharmacol. 2019, 12, 219–234. [Google Scholar] [CrossRef]
- Miles, A.; McLellan, N.; Machan, R.; Vokes, D.; Hunting, A.; McFarlane, M.; Holmes, J.; Lynn, K. Dysphagia and Laryngeal Pathology in Post-Surgical Cardiothoracic Patients. J. Crit. Care 2018, 45, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Leonard, R.J.; White, C.; Mckenzie, S.; Belafsky, P.C. Effects of Bolus Rheology on Aspiration in Patients with Dysphagia. J. Acad. Nutr. Diet. 2014, 114, 590–594. [Google Scholar] [CrossRef]
- Sopade, P.; Halley, P.; Cichero, J.; Ward, L. Rheological Characterisation of Food Thickeners Marketed in Australia in Various Media for the Management of Dysphagia. I: Water and Cordial. J. Food Eng. 2007, 79, 69–82. [Google Scholar] [CrossRef]
- Zargaraan, A.; Rastmanesh, R.; Fadavi, G.; Zayeri, F.; Mohammadifar, M.A. Rheological Aspects of Dysphagia-Oriented Food Products: A Mini Review. Food Sci. Hum. Wellness 2013, 2, 173–178. [Google Scholar] [CrossRef]
- Sestili, M.; Logrippo, S.; Cespi, M.; Bonacucina, G.; Ferrara, L.; Busco, S.; Grappasonni, I.; Palmieri, G.F.; Ganzetti, R.; Blasi, P. Potentially Inappropriate Prescribing of Oral Solid Medications in Elderly Dysphagic Patients. Pharmaceutics 2018, 10, 280. [Google Scholar] [CrossRef] [PubMed]
- Drumond, N.; Stegemann, S. Better Medicines for Older Patients: Considerations between Patient Characteristics and Solid Oral Dosage Form Designs to Improve Swallowing Experience. Pharmaceutics 2020, 13, 32. [Google Scholar] [CrossRef] [PubMed]
- Forough, A.S.; Lau, E.T.; Steadman, K.J.; Cichero, J.A.; Kyle, G.J.; Santos, J.M.S.; Nissen, L.M. A Spoonful of Sugar Helps the Medicine Go Down? A Review of Strategies for Making Pills Easier to Swallow. Patient Prefer. Adherence 2018, 12, 1337–1346. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Ghaffur, A.; Bains, J.; Hamdy, S. Acceptability of Oral Solid Medicines in Older Adults with and without Dysphagia: A Nested Pilot Validation Questionnaire Based Observational Study. Int. J. Pharm. 2016, 512, 374–381. [Google Scholar] [CrossRef]
- Lau, E.T.; Steadman, K.J.; Cichero, J.A.; Nissen, L.M. Dosage Form Modification and Oral Drug Delivery in Older People. Adv. Drug Deliv. Rev. 2018, 135, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Haw, C.; Stubbs, J. Administration of Medicines in Food and Drink: A Study of Older Inpatients with Severe Mental Illness. Int. Psychogeriatr. 2010, 22, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Mc Gillicuddy, A.; Crean, A.M.; Sahm, L.J. Older Adults with Difficulty Swallowing Oral Medicines: A Systematic Review of the Literature. Eur. J. Clin. Pharmacol. 2016, 72, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Malouh, M.A.; Cichero, J.A.; Manrique, Y.J.; Crino, L.; Lau, E.T.L.; Nissen, L.M.; Steadman, K.J. Are Medication Swallowing Lubricants Suitable for Use in Dysphagia? Consistency, Viscosity, Texture, and Application of the International Dysphagia Diet Standardization Initiative (IDDSI) Framework. Pharmaceutics 2020, 12, 924. [Google Scholar] [CrossRef] [PubMed]
- Manrique, Y.J.; Sparkes, A.M.; Cichero, J.A.; Stokes, J.R.; Nissen, L.M.; Steadman, K.J. Oral Medication Delivery in Impaired Swallowing: Thickening Liquid Medications for Safe Swallowing Alters Dissolution Characteristics. Drug Dev. Ind. Pharm. 2016, 42, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Manrique-Torres, Y.J.; Lee, D.J.; Islam, F.; Nissen, L.M.; Cichero, J.A.; Stokes, J.R.; Steadman, K.J. Crushed Tablets: Does the Administration of Food Vehicles and Thickened Fluids to Aid Medication Swallowing Alter Drug Release? J. Pharm. Pharm. Sci. 2014, 17, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Dressman, J.B.; Amidon, G.L.; Reppas, C.; Shah, V.P. Dissolution Testing as a Prognostic Tool for Oral Drug Absorption: Immediate Release Dosage Forms. Pharm. Res. 1998, 15, 11–22. [Google Scholar] [CrossRef]
- Martir, J.; Flanagan, T.; Mann, J.; Fotaki, N. Impact of Food and Drink Administration Vehicles on Paediatric Formulation Performance Part 2: Dissolution of Montelukast Sodium and Mesalazine Formulations. AAPS PharmSciTech 2020, 21, 287. [Google Scholar] [CrossRef]
- Ruiz-Picazo, A.; Colón-Useche, S.; Gonzalez-Alvarez, M.; Gonzalez-Alvarez, I.; Bermejo, M.; Langguth, P. Effect of Thickener on Disintegration, Dissolution and Permeability of Common Drug Products for Elderly Patients. Eur. J. Pharm. Biopharm. 2020, 153, 168–176. [Google Scholar] [CrossRef]
- Onuki, Y.; Sugiura, D.; Kumada, S.; Kobayashi, R.; Nakamura, T.; Kogawa, T.; Sakai, H.; Okada, K. The Molded Tablet, a Disintegrant-Free Orally Disintegrating Tablet, Resists Thickening Solution-Reduced Drug Dissolution. J. Drug Deliv. Sci. Technol. 2022, 69, 103179. [Google Scholar] [CrossRef]
- Radhakrishnan, C. Oral Medication Dose Form Alteration: Patient Factors and the Effect of Adding Thickened Fluids. Ph.D. Thesis, The University of Queensland, Brisbane, Australia, 2016. [Google Scholar]
- Torres, Y.J.M. Understanding the Mechanism of Drug Delivery from Thickened Fluids to Aid Swallowing of Medications. Ph.D. Thesis, The University of Queensland, Brisbane, Australia, 2015. [Google Scholar]
- Chen, F.; Dirven, S.; Xu, W.; Bronlund, J.; Li, X.; Pullan, A. Review of the Swallowing System and Process for a Biologically Mimicking Swallowing Robot. Mechatronics 2012, 22, 556–567. [Google Scholar] [CrossRef]
- Sharma, M.; Pico, J.; Martinez, M.M.; Duizer, L. The Dynamics of Starch Hydrolysis and Thickness Perception During Oral Processing. Int. Food Res. J. 2020, 134, 109275. [Google Scholar] [CrossRef] [PubMed]
- Ferry, A.; Hort, J.; Mitchell, J.; Lagarrigue, S.; Pamies, B. Effect of Amylase Activity on Starch Paste Viscosity and Its Implications for Flavor Perception. J. Texture Stud. 2004, 35, 511–524. [Google Scholar] [CrossRef]
- Vilardell, N.; Rofes, L.; Arreola, V.; Speyer, R.; Clavé, P. A Comparative Study between Modified Starch and Xanthan Gum Thickeners in Post-Stroke Oropharyngeal Dysphagia. Dysphagia 2016, 31, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Hanson, B.; O’leary, M.T.; Smith, C.H. The Effect of Saliva on the Viscosity of Thickened Drinks. Dysphagia 2012, 27, 10–19. [Google Scholar] [CrossRef]
- Peyron, M.-A.; Gierczynski, I.; Hartmann, C.; Loret, C.; Dardevet, D.; Martin, N.; Woda, A. Role of Physical Bolus Properties as Sensory Inputs in the Trigger of Swallowing. PLoS ONE 2011, 6, e21167. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.S.; Park, D.; Oh, Y.; Lee, S.T.; Kang, J.Y. The Effects of Bolus Volume and Texture on Pharyngeal Pressure Events Using High-Resolution Manometry and Its Comparison with Videofluoroscopic Swallowing Study. J. Neurogastroenterol. Motil. 2016, 22, 231–239. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chen, J. Food Oral Processing—A Review. Food Hydrocoll. 2009, 23, 1–25. [Google Scholar] [CrossRef]
- Stading, M.; Waqas, M.Q.; Holmberg, F.; Wiklund, J.; Kotze, R.; Ekberg, O. A Device That Models Human Swallowing. Dysphagia 2019, 34, 615–626. [Google Scholar] [CrossRef]
- Kalantzi, L.; Reppas, C.; Dressman, J.; Amidon, G.; Junginger, H.; Midha, K.; Shah, V.; Stavchansky, S.; Barends, D.M. Biowaiver Monographs for Immediate Release Solid Oral Dosage Forms: Acetaminophen (Paracetamol). J. Pharm. Sci. 2006, 95, 4–14. [Google Scholar] [CrossRef]
- Bernal, V.; Erto, A.; Giraldo, L.; Moreno-Piraján, J.C. Effect of Solution Ph on the Adsorption of Paracetamol on Chemically Modified Activated Carbons. Molecules 2017, 22, 1032. [Google Scholar] [CrossRef]
- Nissen, L.M.; Haywood, A.; Steadman, K.J. Solid Medication Dosage Form Modification at the Bedside and in the Pharmacy of Queensland Hospitals. J. Pharm. Pract. Res. 2009, 39, 129–134. [Google Scholar] [CrossRef]
- Marquis, J.; Schneider, M.-P.; Payot, V.; Cordonier, A.-C.; Bugnon, O.; Hersberger, K.E.; Arnet, I. Swallowing Difficulties with Oral Drugs among Polypharmacy Patients Attending Community Pharmacies. Int. J. Clin. Pharm. 2013, 35, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Mandel, A.L.; des Gachons, C.P.; Plank, K.L.; Alarcon, S.; Breslin, P.A.S. Individual Differences in Amy1 Gene Copy Number, Salivary A-Amylase Levels, and the Perception of Oral Starch. PLoS ONE 2010, 5, e13352. [Google Scholar] [CrossRef]
- British Pharmacopoeia Commission. Appendix XII Recommendations on Dissolution Testing. In The British Pharmacopoeia 2018; The Stationary Office: London, UK, 2018. [Google Scholar]
- United States Pharmacopoeia. The United States Pharmacopeia and National Formulary USP 34–NF 29; The United States Pharmacopoeial Convention: Rockville, MD, USA, 2011. [Google Scholar]
- The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). Guidance for industry: Validation of Analytical Procedures: Text and Methodology. 1996. Available online: https://www.ich.org/page/quality-guidelines (accessed on 16 November 2023).
- Su, M.; Zheng, G.; Chen, Y.; Xie, H.; Han, W.; Yang, Q.; Sun, J.; Lv, Z.; Chen, J. Clinical Applications of IDDSI Framework for Texture Recommendation for Dysphagia Patients. J. Texture Stud. 2018, 49, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Hadde, E.K.; Cichero, J.A.; Nicholson, T.M. Viscosity of Thickened Fluids That Relate to the Australian National Standards. Int. J. Speech-Lang. Pathol. 2016, 18, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Szabó, P.; Kállai-Szabó, B.; Kállai-Szabó, N.; Sebe, I.; Zelkó, R. Preparation of Hydroxypropyl Cellulose Microfibers by High-Speed Rotary Spinning and Prediction of the Fiber-Forming Properties of Hydroxypropyl Cellulose Gels by Texture Analysis. Cellulose 2014, 21, 4419–4427. [Google Scholar] [CrossRef]
- Food and Drug Administration. Guidance for industry: Dissolution testing of Immediate Release Solid Oral Dosage Forms. Rockville, MD: US Department of Health and Human Services, FDA, Center for Drug Evaluation and Research. 1997. Available online: https://www.fda.gov/media/70936/download (accessed on 16 November 2023).
- Chen, J.; Stokes, J.R. Rheology and Tribology: Two Distinctive Regimes of Food Texture Sensation. Food Sci. Technol. 2012, 25, 4–12. [Google Scholar] [CrossRef]
- Van Eck, A.; Stieger, M. Oral Processing Behavior, Sensory Perception and Intake of Composite Foods. Food Sci. Technol. 2020, 106, 219–231. [Google Scholar] [CrossRef]
- Janssen, A.M.; Terpstra, M.E.; De Wijk, R.A.; Prinz, J.F. Relations between Rheological Properties, Saliva-Induced Structure Breakdown and Sensory Texture Attributes of Custards. J. Texture Stud. 2007, 38, 42–69. [Google Scholar] [CrossRef]
- Dirven, S.; Xu, W.; Cheng, L.K. Sinusoidal Peristaltic Waves in Soft Actuator for Mimicry of Esophageal Swallowing. IEEE ASME Trans. Mechatron. 2015, 20, 1331–1337. [Google Scholar] [CrossRef]
- Dirven, S.; Xu, W.; Cheng, L.K.; Allen, J. Biomimetic Investigation of Intrabolus Pressure Signatures by a Peristaltic Swallowing Robot. IEEE T. Instrum. Meas. 2015, 64, 967–974. [Google Scholar] [CrossRef]
- Lavoisier, A.; Shreeram, S.; Jedwab, M.; Ramaioli, M. Effect of the Rheological Properties of the Liquid Carrier on the in Vitro Swallowing of Solid Oral Dosage Forms. J. Texture Stud. 2021, 52, 623–637. [Google Scholar] [CrossRef]
- Saitoh, E.; Shibata, S.; Matsuo, K.; Baba, M.; Fujii, W.; Palmer, J.B. Chewing and Food Consistency: Effects on Bolus Transport and Swallow Initiation. Dysphagia 2007, 22, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Guo, Y.; Li, R.; Ma, A.; Zhang, H. Rheological Characterization of Polysaccharide Thickeners Oriented for Dysphagia Management: Carboxymethylated Curdlan, Konjac Glucomannan and Their Mixtures Compared to Xanthan Gum. Food Hydrocoll. 2020, 110, 106198. [Google Scholar] [CrossRef]
- Himashree, P.; Sengar, A.S.; Sunil, C. Food Thickening Agents: Sources, Chemistry, Properties and Applications—A Review. Int. J. Gastron. Food Sci. 2022, 27, 100468. [Google Scholar] [CrossRef]
- Salah, R.B.; Besbes, S.; Chaari, K.; Rhouma, A.; Attia, H.; Deroanne, C.; Blecker, C. Rheological and Physical Properties of Date Juice Palm by-Product (Phoenix dactylifera L.) and Commercial Xanthan Gums. J. Texture Stud. 2010, 41, 125–138. [Google Scholar] [CrossRef]
- Houjaij, N.; Dufresne, T.; Lachance, N.; Ramaswamy, H. Textural Characterization of Pureed Cakes Prepared for the Therapeutic Treatment of Dysphagic Patients. Int. J. Food Prop. 2009, 12, 45–54. [Google Scholar] [CrossRef]
- Steele, C.M.; Alsanei, W.A.; Ayanikalath, S.; Barbon, C.E.A.; Chen, J.; Cichero, J.A.Y.; Coutts, K.; Dantas, R.O.; Duivestein, J.; Giosa, L.; et al. The Influence of Food Texture and Liquid Consistency Modification on Swallowing Physiology and Function: A Systematic Review. Dysphagia 2015, 30, 2–26. [Google Scholar] [CrossRef]
- Momosaki, R.; Abo, M.; Kobayashi, K. Swallowing Analysis for Semisolid Food Texture in Poststroke Dysphagic Patients. J. Stroke Cerebrovasc. Dis. 2013, 22, 267–270. [Google Scholar] [CrossRef]
- Sungsinchai, S.; Niamnuy, C.; Wattanapan, P.; Charoenchaitrakool, M.; Devahastin, S. Texture Modification Technologies and Their Opportunities for the Production of Dysphagia Foods: A Review. Compr. Rev. Food Sci. Food Saf. 2019, 18, 1898–1912. [Google Scholar] [CrossRef]
- Vallons, K.J.; Helmens, H.J.; Oudhuis, A. Effect of Human Saliva on the Consistency of Thickened Drinks for Individuals with Dysphagia. Int. J. Lang Comm. Dis. 2015, 50, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Rofes, L.; Arreola, V.; Mukherjee, R.; Swanson, J.; Clavé, P. The Effects of a Xanthan Gum-Based Thickener on the Swallowing Function of Patients with Dysphagia. Aliment. Pharmacol. Ther. 2014, 39, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Vallons, K.J.; Oudhuis, L.A.; Helmens, H.J.; Kistemaker, C. The Effect of Oral Processing on the Viscosity of Thickened Drinks for Patients with Dysphagia. Ann. Rehabil. Med. 2015, 39, 772. [Google Scholar] [CrossRef] [PubMed]
- Chojin, Y.; Kato, T.; Rikihisa, M.; Omori, M.; Noguchi, S.; Akata, K.; Ogoshi, T.; Yatera, K.; Mukae, H. Evaluation of the mann assessment of swallowing ability in elderly patients with pneumonia. Aging Dis. 2017, 8, 420. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Akagi, J. Decreased Tongue Pressure Is Associated with Sarcopenia and Sarcopenic Dysphagia in the Elderly. Dysphagia 2015, 30, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Marcott, S.; Dewan, K.; Kwan, M.; Baik, F.; Lee, Y.-J.; Sirjani, D. Where Dysphagia Begins: Polypharmacy and Xerostomia. Fed. Pract. 2020, 37, 234. [Google Scholar]



{kind=link}
{kind=link}
| Name | Manufacturer | Flavour | Composition | IDDSI Classification | Yield Stress (Pa) |
|---|---|---|---|---|---|
| MediSpend | Fagron, Rotterdam, The Netherlands | lemon | Purified water, modified food starch, natural lemon flavour, sodium citrate, citric acid, sucralose, sodium benzoate. | 2—mildly thick | 2.47 |
| Severo | IMS Medical, Grootebroek, The Netherlands | anise | purified water, cellulose gum, flavour (anise), citric acid, potassium sorbate, aspartame, acesulfame K. | 2—mildly thick | - |
| Gloup Low Sugar | Rushwood, Raamsdonksveer, The Netherlands | raspberry | Water, xylitol, carrageenan, maltodextrin, potassium sorbate, citric acid, colour, aroma. | 3—moderately thick | 12.50 |
| Gloup Original | Rushwood, Raamsdonksveer, The Netherlands | strawberry/ banana | Water, carrageenan, maltodextrin, potassium sorbate, sucrose, calcium chloride, citric acid, colour, aroma. | 3—moderately thick | 9.76 |
| Gloup Forte | Rushwood, Raamsdonksveer, The Netherlands | vanilla | Water, dried glucose syrup, sucrose, carrageenan, maltodextrin, potassium sorbate, citric acid, (natural) aroma | 4—extremely thick | 38.13 |
| Loss of Crushed Paracetamol (%) | ||
|---|---|---|
| Lubricant | without Oral Processing | with Oral Processing |
| MediSpend | 1.20 ± 022 | 1.78 ± 0.37 |
| Severo | 1.47 ± 0.29 | 1.42 ± 0.21 |
| Gloup Low Sugar | 1.88 ± 0.43 | 2.65 ± 0.55 |
| Gloup Original | 1.82 ± 0.98 | 2.64 ± 0.92 |
| Gloup Forte | 4.61 ± 0.97 | 3.24 ± 0.78 |
| No lubricant (Control) | 0.46 ± 0.12 | |
| Paracetamol Dissolved at 30 Min (%) | ||||
|---|---|---|---|---|
| Crushed | Whole | |||
| without Oral Processing | with Oral Processing | without Oral Processing | with Oral Processing | |
| Tablets with: | ||||
| MediSpend | 91.0 ± 0.8 | 88.6 ± 3.3 | 88.8 ± 0.3 | 81.6 ± 3.1 |
| Severo | 84.6 ± 4.8 | 82.6 ± 2.5 | 85.2 ± 2.3 | 87.0 ± 3.0 |
| Gloup Low Sugar | 63.8 ± 7.4 *** | 80.2 ± 2.5 | 85.8 ± 3.2 | 83.0 ± 10.8 |
| Gloup Original | 49.2 ± 7.9 *** | 79.4 ± 5.7 | 71.0 ± 7.8 | 81.4 ± 12.8 |
| Gloup Forte | 30.6 ± 3.8 *** | 42.8 ± 2.3 * | 54.0 ± 17.7 * | 95.2 ± 7.1 |
| No lubricant (control) | 95.8 ± 1.3 | 91.0 ± 3.1 | ||
| Medication Lubricant | Crush Tablet | Treatment | Texture Characteristic | ||||
|---|---|---|---|---|---|---|---|
| Hardness (g) | Adhesiveness (mJ) | Cohesiveness | Gumminess (g) | Springiness (mm) | |||
| MediSpend | N | Control | 3.33 ± 0.36 a | 0.07 ± 0.04 a | 0.85 ± 0.01 a | 3.17 ± 0.14 b | 19.37 ± 0.22 a |
| N | Oral processing | 2.26 ± 0.20 ab | 0.24 ± 0.18 a | 0.47 ± 0.21 a | 1.01 ± 0.30 a | 15.41 ± 1.56 a | |
| Y | Control | 2.00 ± 0.47 b | 0.06 ± 0.01 a | 0.44 ± 0.12 a | 2.00 ± 0.47 a | 11.60 ± 2.00 a | |
| Y | Oral processing | 1.96 ± 0.13 b | 0.03 ± 0.01 a | 0.55 ± 0.13 a | 1.00 ± 0.28 a | 16.24 ± 1.63 a | |
| Severo | N | Control | 3.33 ± 0.14 a | 0.08 ± 0.02 a | 0.59 ± 0.13 a | 2.00 ± 0.50 a | 19.65 ± 0.04 a |
| N | Oral processing | 1.87 ± 0.36 b | 0.02 ± 0.01 a | 0.59 ± 0.09 a | 2.59 ± 0.33 a | 17.66 ± 0.94 a | |
| Y | Control | 1.83 ± 0.14 b | 0.02 ± 0.01 a | 0.69 ± 0.07 a | 1.37 ± 0.15 a | 13.97 ± 2.60 a | |
| Y | Oral processing | 1.88 ± 0.15 b | 0.05 ± 0.02 a | 0.56 ± 0.07 a | 1.04 ± 0.20 a | 18.86 ± 0.92 a | |
| Gloup Low Sugar | N | Control | 4.83 ± 0.68 a | 0.12 ± 0.04 a | 0.75 ± 0.09 a | 3.67 ± 0.73 a | 16.79 ± 0.29 a |
| N | Oral processing | 5.16 ± 0.64 a | 0.15 ± 0.04 a | 0.72 ± 0.05 a | 3.77 ± 0.61 a | 18.74 ± 0.44 a | |
| Y | Control | 3.33 ± 0.36 a | 0.07 ± 0.03 a | 0.80 ± 0.09 a | 2.47 ± 0.40 a | 12.05 ± 1.48 a | |
| Y | Oral processing | 4.77 ± 0.59 a | 0.10 ± 0.02 a | 0.78 ± 0.05 a | 3.56 ± 0.53 a | 18.44 ± 1.52 a | |
| Gloup Original | N | Control | 4.33 ± 0.27 ab | 0.08 ± 0.02 a | 0.93 ± 0.03 a | 4.03 ± 0.40 a | 19.70 ± 0.06 a |
| N | Oral processing | 4.43 ± 0.19 a | 0.10 ± 0.00 a | 0.75 ± 0.01 a | 3.26 ± 0.11 ab | 16.94 ± 0.52 ab | |
| Y | Control | 2.58 ± 0.60 b | 0.09 ± 0.03 a | 0.82 ± 0.04 a | 2.60 ± 0.39 b | 13.13 ± 2.69 b | |
| Y | Oral processing | 4.82 ± 0.22 a | 0.10 ± 0.02 a | 0.74 ± 0.04 a | 3.03 ± 0.32 ab | 18.26 ± 0.32 a | |
| Gloup Forte | N | Control | 9.17 ± 0.14 a | 0.33 ± 0.01 a | 0.83 ± 0.01 a | 7.60 ± 0.19 a | 19.62 ± 0.06 a |
| N | Oral processing | 9.16 ± 0.25 a | 0.26 ± 0.02 a | 0.80 ± 0.01 a | 7.27 ± 0.22 a | 17.32 ± 0.49 ab | |
| Y | Control | 4.50 ± 0.24 b | 0.20 ± 0.05 a | 0.83 ± 0.04 a | 3.87 ± 0.31 b | 12.20 ± 2.31 b | |
| Y | Oral processing | 9.37 ± 0.39 a | 0.29 ± 0.02 a | 0.81 ± 0.01 a | 7.27 ± 0.14 a | 18.09 ± 0.14 a | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malouh, M.A.; Cichero, J.A.Y.; Sun, Y.; Lau, E.T.L.; Nissen, L.M.; Steadman, K.J. Medication Lubricants for Oral Delivery of Drugs: Oral Processing Reduces Thickness, Changes Characteristics, and Improves Dissolution Profile. Pharmaceutics 2024, 16, 417. https://doi.org/10.3390/pharmaceutics16030417
Malouh MA, Cichero JAY, Sun Y, Lau ETL, Nissen LM, Steadman KJ. Medication Lubricants for Oral Delivery of Drugs: Oral Processing Reduces Thickness, Changes Characteristics, and Improves Dissolution Profile. Pharmaceutics. 2024; 16(3):417. https://doi.org/10.3390/pharmaceutics16030417
Chicago/Turabian StyleMalouh, Marwa A., Julie A. Y. Cichero, Yu Sun, Esther T. L. Lau, Lisa M. Nissen, and Kathryn J. Steadman. 2024. "Medication Lubricants for Oral Delivery of Drugs: Oral Processing Reduces Thickness, Changes Characteristics, and Improves Dissolution Profile" Pharmaceutics 16, no. 3: 417. https://doi.org/10.3390/pharmaceutics16030417
APA StyleMalouh, M. A., Cichero, J. A. Y., Sun, Y., Lau, E. T. L., Nissen, L. M., & Steadman, K. J. (2024). Medication Lubricants for Oral Delivery of Drugs: Oral Processing Reduces Thickness, Changes Characteristics, and Improves Dissolution Profile. Pharmaceutics, 16(3), 417. https://doi.org/10.3390/pharmaceutics16030417