1. Introduction
Ibuprofen (IBU), a propionic acid derivative (
Figure 1), is a classical Biopharmaceutical Classification System (BCS) class II nonsteroidal anti-inflammatory drug (NSAID) that is mostly administered orally to relieve acute pain and inflammation. Its effect, like other NSAIDs, is based on its ability to inhibit the production of prostaglandins by reducing the activity of cyclooxygenase enzymes (COX-1 and COX-2) [
1]. IBU is extremely poorly soluble in aqueous media [
2] as its solubility is 0.021 mg·mL
−1 [
3]. Therefore, the rate of dissolution from the solid dosage forms that are currently available is limited. The required dosage for a therapeutic effect in an adult is approximately 20–30 mg, whereas the provided dose is more than 10 times this amount [
4] because of its poor bioavailability and first-pass metabolism. In addition to being economically inefficient, this significantly increases the occurrence of side effects caused by IBU [
5], e.g., stomachache, indigestion, or gastrointestinal bleeding and kidney injury [
6]. To overcome this issue, alternative administration routes have been investigated for the delivery of IBU, including ocular [
7], nasal [
8], inhalation [
9,
10], and transdermal routes [
11]. The use of these routes offers the opportunity to reduce the amount of active substances by bypassing the first-pass mechanism and exerting their effect locally.
Although IBU is not primarily used for cystic fibrosis (CF) therapy, it is the only NSAID approved for chronic use in CF, which is an autosomal recessive inheritance. Among the symptoms, in addition to inflammation and infection, the production of excessive viscous mucus can be observed. This mucus overproduction arises from the dysregulated transport of ions and water through the epithelial cells [
6]. Consequently, the impaired epithelial function leads to inadequate oxygenation of the lungs. Since inflammation is a characteristic of the lung disease of CF and contributes to lung destruction, anti-inflammatory therapy may be helpful in slowing disease progression [
5]. Treatment of the disease is especially important in the early stages [
12,
13,
14], because in the case of CF patients, abnormal mucus production usually begins immediately after birth [
15], which later leads to infection and inflammation, which in the end causes death. Several clinical trials document the benefits and relative safety of long-term use of high-dose IBU in CF patients [
16,
17,
18]. We therefore declare that IBU may be useful in the treatment of CF, but the challenge lies in the fact that, in addition to having very poor water solubility, due to the mentioned side effects, it is necessary to introduce IBU through an alternative administration route, which is evident in the case of CF: the lung. With local therapy, pulmonary drug delivery can greatly improve drug absorption due to the unique physiological characteristics of the lung, such as a large alveolar surface area [
19], extensive vascularization, and thin alveolar epithelium. However, since there is just 5.6 mL/kg extravascular lung water in normal lungs [
20] to keep the tissues moist, it is advisable to increase the solubility of poorly water-soluble active ingredients such as IBU in order to achieve the desired absorption. It is noteworthy to mention that patients with cystic fibrosis (CF) exhibit significantly higher lung water content [
21,
22], which can be attributed to several factors such as edema and infections. Utilizing cyclodextrins (CDs), the aforementioned issues can be resolved.
CDs are truncated cone-shaped cyclic oligosaccharide compounds which are formed by six (αCD), seven (βCD), or eight (γCD)
D-glucopyranose units, bound via α-1,4- glycosidic linkages (
Figure 2a). The inner cavities of CDs are formed by the hydrophobic carbon backbones of glucopyranose monomers, making the interior hydrophobic (
Figure 2b) [
23]. Due to this structural feature, the use of CDs is mostly focused on their use as solubilizers for molecules that are poorly soluble in water [
24,
25,
26,
27]. In addition to absorbing poorly water-soluble compounds, CDs can also modify the physicochemical characteristics of these molecules; for example, they can increase stability [
24,
25,
26,
27,
28] and permeability [
28,
29]. The spread of CDs in the food industry and the pharmaceutical industry is made possible by the fact that they are edible and not toxic [
30] for human use. With the application of CDs, the listed positive benefits provide the opportunity to increase IBU’s solubility in aqueous media and, consequently, its bioavailability while utilizing less of the active ingredient. In addition to the water solubility of the active ingredient, there are other factors that strongly influence the effectiveness of dry powder inhalers (DPIs), mainly aerodynamic particle size, particle shape, texture, and density [
31]. For the use of CDs in the lungs, more and more research is appearing in the literature on the use of cyclodextrin-based metal-organic frameworks (CD-MOFs) [
32,
33,
34,
35,
36] as they have excellent aerodynamic properties.
γCD-MOFs have been studied more than any other type of CDs thanks to their largest specific surface area (approximately 1220 m
2/g [
37]), richest pore channels (spherical pore diameter is about 0.4–1.7 nm [
37]), structural symmetry, and stability. For γCD-MOFs, six γCD organic ligand molecules are bridged by alkali metal salt (mostly potassium ions (K
+)) through coordination bonds to form a repeating unit (γ-CD)
6, which is bridged by K
+ and extended along the a, b, and c crystallographic axes in a specific manner [
38], forming a new topological structure (
Figure 2c). Because of their uniform nanoporous structure, CD-MOFs demonstrated greater aerosolization performance when compared to commercial inhalation carriers [
39]. The biocompatibility of CD-MOF in pulmonary administration has also been proven. Yong et al. demonstrated that CD-MOFs can be directly used as a DPI without any other excipients [
33]. According to their research, the aerosolization of the carriers depended primarily on the particle size and not on the flowability, so the added excipient did not promote the deep deposition of the sample in the lungs. Another study on pulmonary applicability of CD-MOFs reported that curcumin was loaded into CD-MOFs and compared with micronized curcumin (Cur-CD-MOF) [
32]. The results showed that the Cur-CD-MOF, in addition to exhibiting excellent aerodynamic performance, showed a much faster drug release rate than that of micronized curcumin, while CD-MOFs could dramatically improve the solubility of various hydrophobic active pharmaceutical ingredients (APIs). Even if a lot of studies on the pulmonary application of CD-MOFs have been published, the quantity of these studies is still quite low. Nonetheless, they appear extremely promising, and an increasing amount of research is required to explore and comprehend the topic more thoroughly.
Vapor diffusion is the most widely used method for synthesizing CD-MOFs; however, this process can take 3–5 days or weeks, requires the use of a large amount of organic solvent and provides low product yield [
40]. Furthermore, in several cases, the active ingredient was loaded in a separate step [
41,
42,
43], which means a multi-step process. Consequently, the development of alternative protocols for CD-MOF production was deemed essential, with proposed advantages including enhanced product yield, reduced preparation time, and minimized amount of organic solvent. Alternative production techniques already exist in the literature [
38], such as microwave-, ultrasound-, or modulator-assisted synthesis. The use of modulators further complicated the production, as they were often inseparable from the final product [
44]. In addition, the previously mentioned techniques require a subsequent drying process. Despite the freeze-drying method occasionally mentioned in literature as a final step of synthesis [
42,
45,
46,
47], there has been limited comprehensive investigation into its suitability for complex preparation from solutions, even though analogous experiments have been carried out using the spray-drying method [
36,
48]. In comparison to the traditional vapor diffusion method, spray-drying presents a promising alternative for production, offering advantages such as higher product yield, reduced synthesis time, and tunable particle properties, all achieved in a single step without the need for a subsequent drying process. However, the technique has certain limitations; for instance, its application is not advantageous for heat-sensitive, highly viscous, or highly foaming materials. The alternative freeze-drying technique can provide a solution to the problem. In comparison to spray-drying, freeze-drying is a more time-consuming, complex, and expensive process. However, it retains the advantages associated with spray-drying over the traditional vapor diffusion method. Moreover, freeze-drying can address specific challenges that arise during spray drying and provides an opportunity to assist in the production of a stable product. Taking these factors into consideration, we strongly believe that developing a freeze-drying production process for CD-MOFs could represent a valuable strategy.
Quality by Design (QbD) is a comprehensive methodology in pharmaceutical development that prioritizes systematic, scientific, risk-based, and proactive approaches [
49,
50]. It emphasizes establishing predefined quality objectives, thorough understanding of product and process, and stringent process control. QbD integrates quality risk management into every stage of formulation, focusing on ensuring consistent product quality. The QbD strategy, outlined in the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) quality guidelines, including Q8 (Pharmaceutical Development [
51]), Q9 (Quality Risk Management [
52], Q10 (Pharmaceutical Quality System [
53]), and Q11 (Development and Manufacture of Drug Substances [
54]) aligns with the standards and expectations of both national and international regulatory bodies. In the QbD approach, the first step involves determining the Quality Profile of the Target Product (QTPP) [
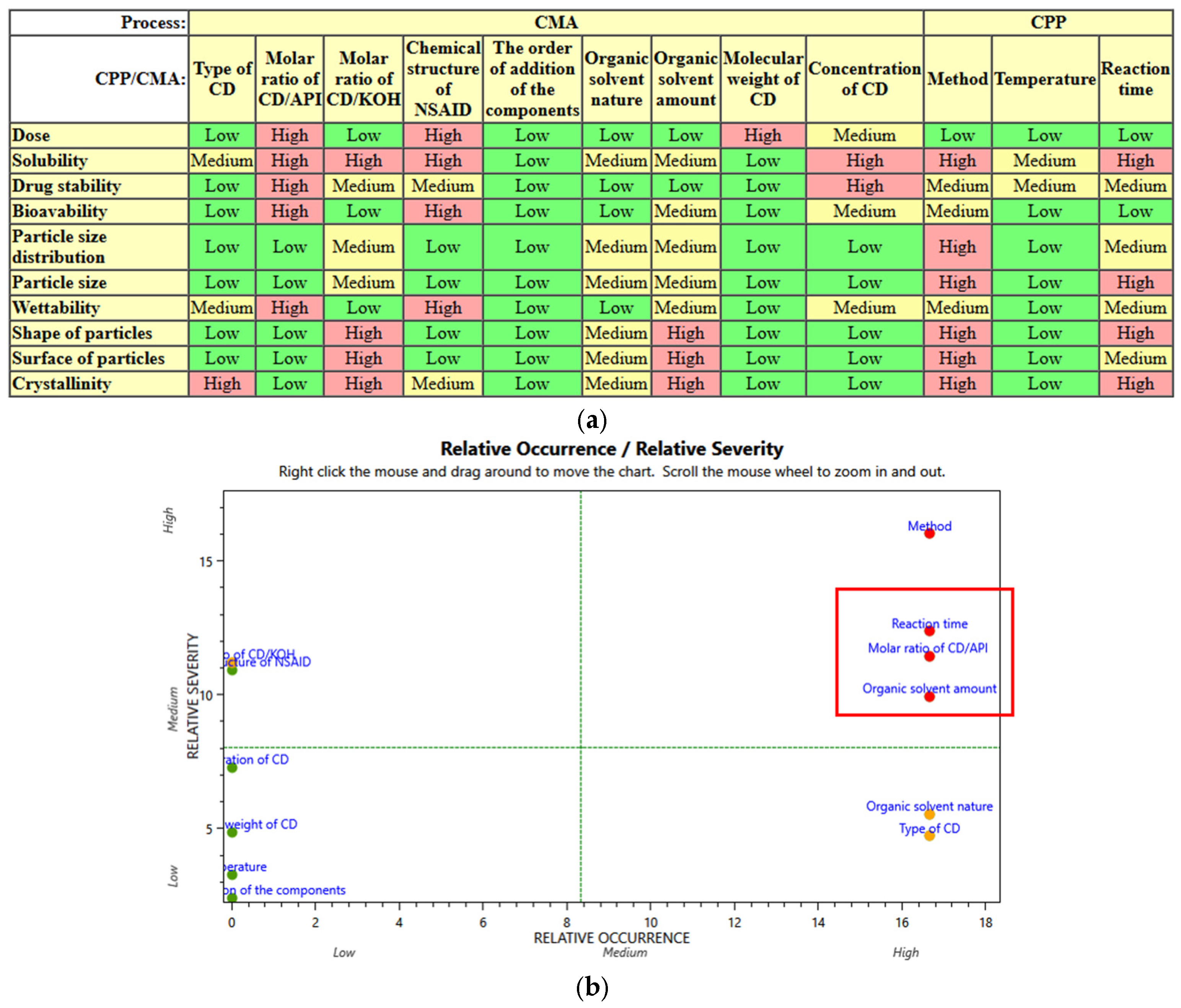
55], which outlines the essential characteristics crucial for its therapeutic application. After determining the QTPP, it is necessary to define Critical Quality Attributes (CQAs), which encompass the physical, chemical, and microbiological properties directly impacting the safety and efficacy of the product. Following CQAs establishment, it is necessary to identify Critical Material Attributes (CMAs) and Critical Process Parameters (CPPs). CMAs express which Material Properties (MAs) are critical relating to CQAs, while CPPs outline the process parameters that significantly influence the production process. Risk Assessment (RA) plays a key role in this process by evaluating the severity and likelihood of occurrence of identified risks. This assessment guides the prioritization of critical parameters influencing CQAs. Once the critical parameters are identified, factorial experimental designs, such as the 3
3 Box–Behnken experimental design, are employed [
56,
57]. These designs allow for the systematic exploration of multiple factors and their interactions, facilitating the optimization of the production process.
In this study, γCD-MOF composed of γCD and K+ ions were utilized to form an inclusion complex with the model drug IBU. The Box–Behnken factorial design has been applied based on a QbD approach to produce new formulations. Although the use of QbD is becoming more and more widespread in drug research, we did not find any publication that applied it in the field of CD-MOFs. The preparation process for the approach was freeze-drying. First analyses were conducted to evaluate morphology, particle size, and crystallinity, ensuring the suitability of the particles for targeted lung delivery. Next, investigations focused on the thermostability of IBU and its interaction with γCD-MOF. To evaluate the practical application of the prepared samples, in vitro pulmonary deposition studies were carried out utilizing the Andersen Cascade Impactor. In vitro release assays were also carried out to measure the encapsulated drug’s release profile. These investigations shed light on the potential of γ-CD-MOF complexes as promising carriers for pulmonary drug delivery systems, underscoring the significance of the QbD approach in the field of pharmaceutical sciences.
4. Conclusions
In this research, instead of using the commonly used vapor diffusion method, γCD-MOFs were created by freeze-drying, which has not been published yet in the literature. We were the first to implement the QbD method in the production of inhalable γCD-MOFs. By defining the CMAs and CPPs, with the help of the RA, we successfully fulfilled our expectations for the QTPP, which means, we successfully produced preparations that could potentially be used in the treatment of CF. Based on QbD, we identified three critical factors, namely the molar ratio of the IBU to the γCD, incubation time, and the percentage of the organic solvent. Morphology, particle size, particle size distribution, and crystallinity could be tuned by changing the factors. The molar ratio of γCD and IBU had an effect on the particle size, as increasing the IBU concentration significantly decreased the particle size. Our assumption about this appearance was that the pores in the cubic crystals can provide additional space outside of the γCD cavity for IBU molecules to wedge in, which do not necessarily affect the morphology, but can inhibit crystal growth. This made it possible to increase the IBU content in the γCD-MOFs, as the higher IBU content created a more favorable size for pulmonary intake. In the in vitro aerodynamic study, the most favorable results were observed in samples with a 1:2 molar ratio of γCD to IBU when the initial solution contained 10% organic solvent. The MMAD[μm] and FPF[%] values of the sample incubated for 48 h were 4.15 ± 0.57 and 47.18 ± 4.18, respectively, while the values of the immediately frozen sample were 5.06 ± 0.21 and 38.10 ± 5.06. We demonstrated that, in terms of deposition efficiency, particle size is a key factor. From the aforementioned samples, nearly the entire quantity of IBU dissolved within the first 5 min during the in vitro dissolution tests; therefore, we achieved a rapid dissolution of the active ingredient for the effective treatment of CF. The effectiveness was further enhanced by the fact that the solubility of IBU was drastically increased due to the complexation. In order to prove that an inclusion complex was indeed formed, we supplemented our XRPD, DSC, and FT-IR structural analysis methods with NMR spectroscopy, which adequately supported our assumptions. Our formulations could be suggested for further investigations, while γCD-MOFs are expected to be promising carriers for IBU delivery by pulmonary route.

 ,
, 


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}