
Topical Delivery of Atraric Acid Derived from Stereocaulon japonicum with Enhanced Skin Permeation and Hair Regrowth Activity for Androgenic Alopecia

 , , , , , ,
, , , , , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Animals
2.3. Preparation of AA from Stereocaulon japonicum
2.4. Solubility of AA in Various Solvents
2.5. Preparation of AA–TFs
2.6. In Vitro Permeability of AA–TF across an Artificial Membrane
2.7. In Vitro Infiltration and Deposition of AA in Full-Thickness Human Skin
2.8. In Vitro Cell Proliferation Assay
2.9. In Vitro Scratch-Wound Recovery Assay
2.10. Efficacy of In Vivo Hair Regrowth
2.11. Western Blot Assay
2.12. Statistical Analysis
3. Results
3.1. Solubility of AA
3.2. Design and Analysis of Artificial Membrane Permeability of AA–TF
3.3. In Vitro Infiltration and Deposition of AA in Full-Thickness Human Skin
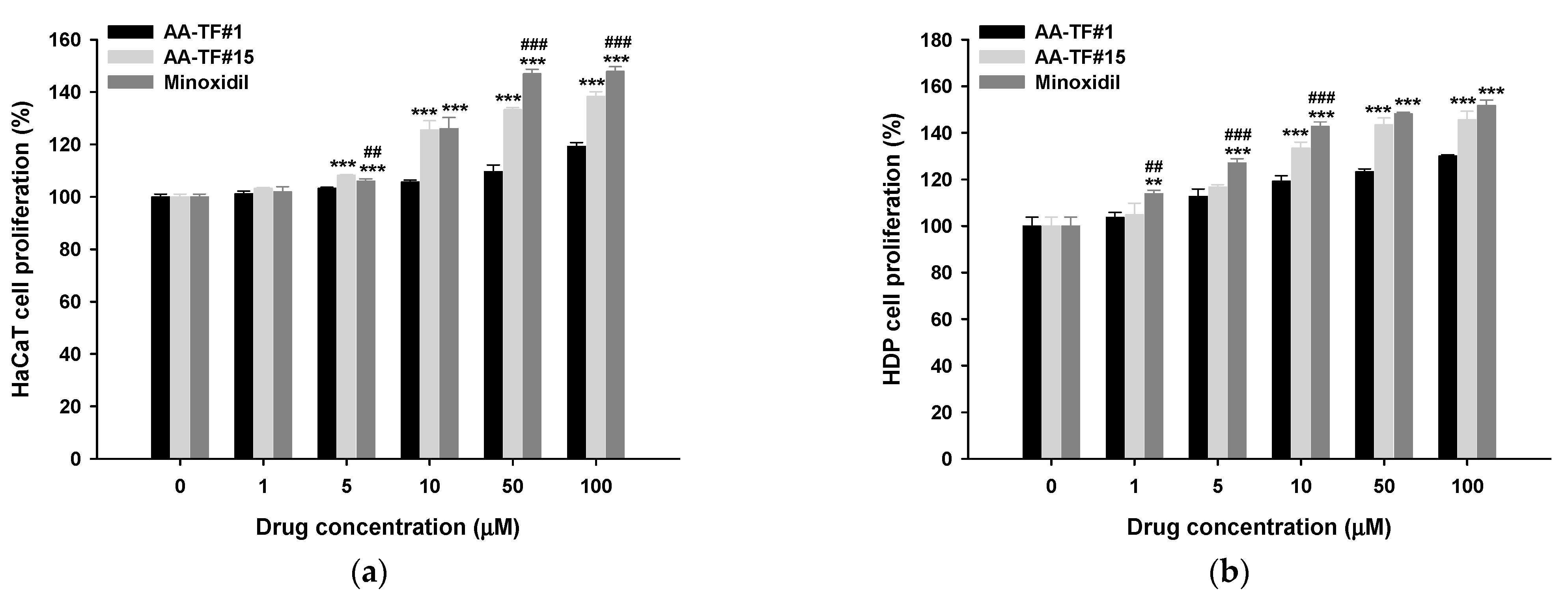
3.4. Cell Proliferation Assay
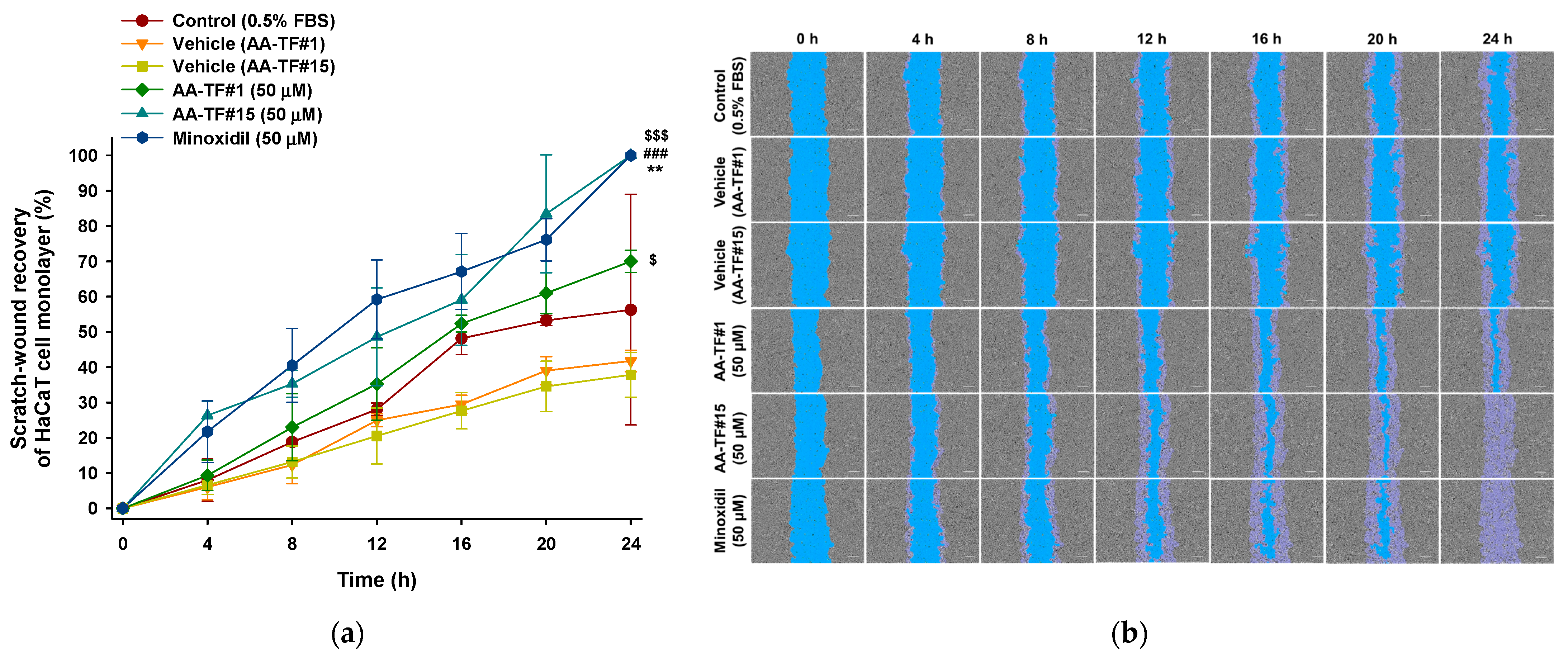
3.5. In Vitro Scratch-Wound Recovery Assay
3.6. In Vivo Hair Regrowth Study
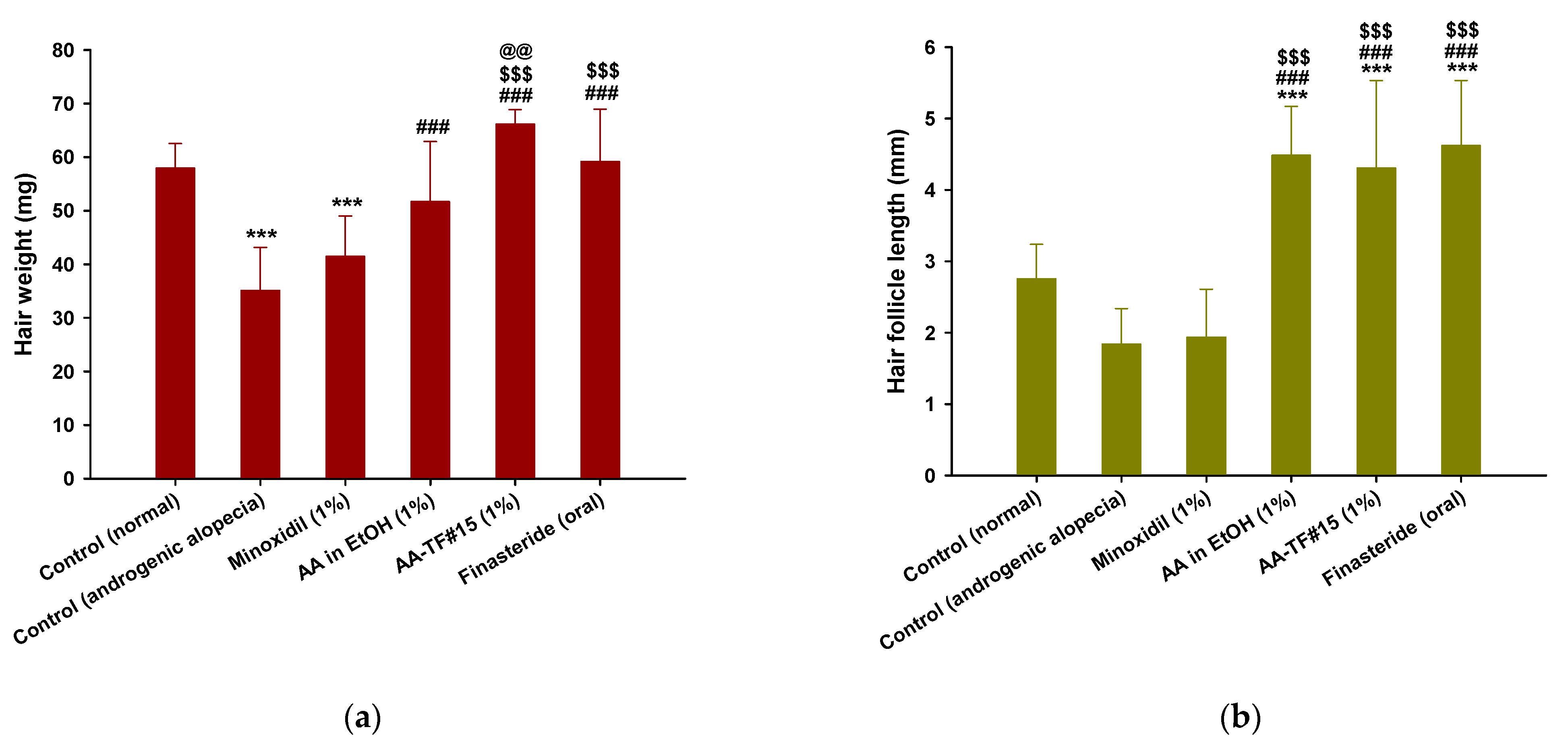
3.7. Hair Weight and Histological Evaluation
3.8. Effects of AA–TF on Activation of the Wnt/β-Catenin Pathway in Androgenic Mice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jain, R.; Monthakantirat, O.; Tengamnuay, P.; De-Eknamkul, W. Identification of a new plant extract for androgenic alopecia treatment using a non-radioactive human hair dermal papilla cell-based assay. BMC Complement. Altern. Med. 2016, 16, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Semwal, D.; Kotiyal, R.; Chauhan, A.; Mishra, A.; Adhikari, L.; Semalty, A.; Semalty, M. Alopecia and the herbal drugs, An overview of the current status. Adv. Biomed. Pharm. 2015, 2, 246–254. [Google Scholar] [CrossRef]
- Seo, M.J.; Song, S.H.; Kim, S.; Jang, W.J.; Jeong, C.H.; Lee, S. Characteristics of Korean patients with methamphetamine use disorder based on the quantitative analysis of methamphetamine and amphetamine in hair. Arch. Pharm. Res. 2020, 43, 798–807. [Google Scholar] [CrossRef]
- Seo, M.J.; Song, S.H.; Kim, S.; Jang, W.J.; Jeong, C.H.; Lee, S. Mass spectrometry-based metabolomics in hair from current and former patients with methamphetamine use disorder. Arch. Pharm. Res. 2021, 44, 890–901. [Google Scholar] [CrossRef]
- Grymowicz, M.; Rudnicka, E.; Podfigurna, A.; Napierala, P.; Smolarczyk, R.; Smolarczyk, K.; Meczekalski, B. Hormonal Effects on Hair Follicles. Int. J. Mol. Sci. 2020, 21, 5342. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J.A.; Sinclair, R.; Harrap, S.B. Androgenetic alopecia: Pathogenesis and potential for therapy. Expert Rev. Mol. Med. 2002, 4, 1–11. [Google Scholar] [CrossRef]
- Papaioannou, M.; Söderholm, A.A.; Hong, W.; Dai, Y.; Roediger, J.; Roell, D.; Thiele, M.; Nyrönen, T.H.; Baniahmad, A. Computational and functional analysis of the androgen receptor antagonist atraric acid and its derivatives. Anticancer Agents Med. Chem. 2013, 13, 801–810. [Google Scholar] [CrossRef]
- Choudhry, R.; Hodgins, M.B.; Van der Kwast, T.H.; Brinkmann, A.O.; Boersma, W.J. Localization of androgen receptors in human skin by immunohistochemistry: Implications for the hormonal regulation of hair growth, sebaceous glands and sweat glands. J. Endocrinol. 1992, 133, 467–475. [Google Scholar] [CrossRef]
- Yang, Y.C.; Fu, H.C.; Wu, C.Y.; Wei, K.T.; Huang, K.E.; Kang, H.Y. Androgen receptor accelerates premature senescence of human dermal papilla cells in association with DNA damage. PLoS ONE 2013, 8, 79434–79443. [Google Scholar] [CrossRef]
- Truong, V.L.; Bak, M.J.; Lee, C.; Jun, M.; Jeong, W.S. Hair Regenerative Mechanisms of Red Ginseng Oil and Its Major Components in the Testosterone-Induced Delay of Anagen Entry in C57BL/6 Mice. Molecules 2017, 22, 1505. [Google Scholar] [CrossRef]
- Katzer, T.; Leite Junior, A.; Beck, R.; da Silva, C. Physiopathology and current treatments of androgenetic alopecia: Going beyond androgens and anti-androgens. Dermatol. Ther. 2019, 32, 13059–13068. [Google Scholar] [CrossRef] [PubMed]
- Saceda-Corralo, D.; Pindado-Ortega, C.; Moreno-Arrones, Ó.M.; Fernández-González, P.; Rodrigues-Barata, A.R.; Jaén-Olasolo, P.; Vañó-Galván, S. Health-related quality of life in patients with frontal fibrosing alopecia. JAMA Dermatol. 2018, 154, 479–480. [Google Scholar] [CrossRef] [PubMed]
- Kerure, A.S.; Patwardhan, N. Complications in hair transplantation. J. Cutan.Aesthc. Surg. 2018, 11, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Ro In, B.; Kim, W.J.; Kang, J. Therapeutic effects of a new long-acting growth factor cocktail (Cellcurex™) injected using a microneedle on the scalp in patients with androgenetic alopecia: A split study. Glob. Dermatol. 2021, 7, 1–4. [Google Scholar]
- Choi, N.; Shin, S.; Song, S.U.; Sung, J.H. Minoxidil Promotes Hair Growth through Stimulation of Growth Factor Release from Adipose-Derived Stem Cells. Int. J. Mol. Sci. 2018, 19, 691. [Google Scholar] [CrossRef]
- Libecco, J.F.; Bergfeld, W.F. Finasteride in the treatment of alopecia. Expert Opin. Pharmacother. 2004, 5, 933–940. [Google Scholar] [CrossRef]
- Suchonwanit, P.; Thammarucha, S.; Leerunyakul, K. Minoxidil and its use in hair disorders: A review. Drug Des. Devel. Ther. 2019, 13, 2777–2786. [Google Scholar] [CrossRef]
- BinJadeed, H.; Almudimeegh, A.M.; Alomran, S.A.; Alshathry, A.H. A case of contact allergic dermatitis to topical minoxidil. Cureus 2021, 13, 12510–12513. [Google Scholar] [CrossRef]
- Zhou, Z.; Song, S.; Gao, Z.; Wu, J.; Ma, J.; Cui, Y. The efficacy and safety of dutasteride compared with finasteride in treating men with androgenetic alopecia: A systematic review and meta-analysis. Clin. Interv. Aging 2019, 14, 399–406. [Google Scholar] [CrossRef]
- Swerdloff, R.S.; Dudley, R.E.; Page, S.T.; Wang, C.; Salameh, W.A. Dihydrotestosterone: Biochemistry, Physiology, and Clinical Implications of Elevated Blood Levels. Endocr. Rev. 2017, 38, 220–254. [Google Scholar] [CrossRef]
- Hirshburg, J.M.; Kelsey, P.A.; Therrien, C.A.; Gavino, A.C.; Reichenberg, J.S. Adverse Effects and Safety of 5-alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. J. Clin. Aesthet. Dermatol. 2016, 9, 56–62. [Google Scholar] [PubMed]
- Seale, L.R.; Eglini, A.N.; McMichael, A.J. Side Effects Related to 5 α-Reductase Inhibitor Treatment of Hair Loss in Women: A Review. J. Drugs Dermatol. 2016, 15, 414–419. [Google Scholar]
- Mun, S.K.; Kang, K.Y.; Jang, H.Y.; Hwang, Y.H.; Hong, S.G.; Kim, S.J.; Cho, H.W.; Chang, D.J.; Hur, J.S.; Yee, S.T. Atraric Acid Exhibits Anti-Inflammatory Effect in Lipopolysaccharide-Stimulated RAW264.7 Cells and Mouse Models. Int. J. Mol, Sci. 2020, 21, 7070. [Google Scholar] [CrossRef]
- Khantham, C.; Linsaenkart, P.; Chaitep, T.; Jantrawut, P.; Chittasupho, C.; Rachtanapun, P.; Jantanasakulwong, K.; Phimolsiripol, Y.; Sommano, S.R.; Prom, U.T.C.; et al. Antioxidation, Anti-Inflammation, and Regulation of SRD5A Gene Expression of Oryza sativa cv. Bue Bang 3 CMU Husk and Bran Extracts as Androgenetic Alopecia Molecular Treatment Substances. Plants 2022, 11, 330. [Google Scholar] [CrossRef] [PubMed]
- Ehsani, M.; Bartsch, S.; Rasa, S.M.M.; Dittmann, J.; Pungsrinont, T.; Neubert, L.; Huettner, S.S.; Kotolloshi, R.; Schindler, K.; Ahmad, A.; et al. The natural compound atraric acid suppresses androgen-regulated neo-angiogenesis of castration-resistant prostate cancer through angiopoietin 2. Oncogene 2022, 41, 3263–3277. [Google Scholar] [CrossRef] [PubMed]
- Ruksiriwanich, W.; Khantham, C.; Muangsanguan, A.; Chittasupho, C.; Rachtanapun, P.; Jantanasakulwong, K.; Phimolsiripol, Y.; Sommano, S.R.; Sringarm, K.; Ferrer, E.; et al. Phytochemical Constitution, Anti-Inflammation, Anti-Androgen, and Hair Growth-Promoting Potential of Shallot (Allium ascalonicum L.) Extract. Plants 2022, 11, 1499. [Google Scholar] [CrossRef]
- Zhu, H.L.; Gao, Y.H.; Yang, J.Q.; Li, J.B.; Gao, J. Serenoa repens extracts promote hair regeneration and repair of hair loss mouse models by activating TGF-β and mitochondrial signaling pathway. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 4000–4008. [Google Scholar]
- Tehler, U.; Fagerberg, J.H.; Svensson, R.; Larhed, M.; Artursson, P.; Bergström, C.A.S. Optimizing Solubility and Permeability of a Biopharmaceutics Classification System (BCS) Class 4 Antibiotic Drug Using Lipophilic Fragments Disturbing the Crystal Lattice. J. Med. Chem. 2013, 56, 2690–2694. [Google Scholar] [CrossRef]
- Wertz, P.W. Roles of Lipids in the Permeability Barriers of Skin and Oral Mucosa. Int. J. Mol. Sci. 2021, 22, 5229. [Google Scholar] [CrossRef]
- Benson, H.A.E.; Grice, J.E.; Mohammed, Y.; Namjoshi, S.; Roberts, M.S. Topical and Transdermal Drug Delivery: From Simple Potions to Smart Technologies. Curr. Drug Deliv. 2019, 16, 444–460. [Google Scholar] [CrossRef]
- Huanbutta, K.; Sittikijyothin, W.; Sangnim, T. Development of topical natural based film forming system loaded propolis from stingless bees for wound healing application. J. Pharm. Investig. 2020, 50, 625–634. [Google Scholar] [CrossRef]
- Hasan, N.; Cao, J.; Lee, J.; Kim, H.; Yoo, J.-W. Development of clindamycin-loaded alginate/pectin/hyaluronic acid composite hydrogel film for the treatment of MRSA-infected wounds. J. Pharm. Investig. 2021, 51, 597–610. [Google Scholar] [CrossRef]
- Shah, B. Microemulsion as a promising carrier for nose to brain delivery: Journey since last decade. J. Pharm. Investig. 2021, 51, 611–634. [Google Scholar] [CrossRef]
- Garg, T.; Rath, G.; Goyal, A.K. Comprehensive review on additives of topical dosage forms for drug delivery. Drug Deliv. 2015, 22, 969–987. [Google Scholar] [CrossRef] [PubMed]
- Kathe, K.; Kathpalia, H. Film forming systems for topical and transdermal drug delivery. Asian J. Pharm. Sci. 2017, 12, 487–497. [Google Scholar] [CrossRef]
- Cilurzo, F.; Casiraghi, A.; Selmin, F.; Minghetti, P. Supersaturation as a tool for skin penetration enhancement. Curr. Pharm. Des. 2015, 21, 2733–2744. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Imran, M.; Mohammed, Y. Topical Semisolid Products—Understanding the Impact of Metamorphosis on Skin Penetration and Physicochemical Properties. Pharmaceutics 2022, 14, 2487. [Google Scholar] [CrossRef]
- Horita, D.; Todo, H.; Sugibayashi, K. Effect of ethanol pretreatment on skin permeation of drugs. Biol. Pharm. Bull. 2012, 35, 1343–1348. [Google Scholar] [CrossRef]
- Moghadam, S.H.; Saliaj, E.; Wettig, S.D.; Dong, C.; Ivanova, M.V.; Huzil, J.T.; Foldvari, M. Effect of Chemical Permeation Enhancers on Stratum Corneum Barrier Lipid Organizational Structure and Interferon Alpha Permeability. Mol. Pharm. 2013, 10, 2248–2260. [Google Scholar] [CrossRef]
- Kim, K.T.; Kim, J.S.; Kim, M.-H.; Park, J.-H.; Lee, J.-Y.; Lee, W.; Min, K.K.; Song, M.G.; Choi, C.-Y.; Kim, W.-S. Effect of Enhancers on in vitro and in vivo Skin Permeation and Deposition of S-Methyl-L-Methionine. Biomol. Ther. 2017, 25, 434–440. [Google Scholar] [CrossRef]
- Osborne, D.W.; Musakhanian, J. Skin Penetration and Permeation Properties of Transcutol®—Neat or Diluted Mixtures. AAPS PharmSciTech 2018, 19, 3512–3533. [Google Scholar] [CrossRef] [PubMed]
- Amatya, R.; Kim, D.; Min, K.A.; Shin, M.C. Iron oxide nanoparticles-loaded hydrogels for effective topical photothermal treatment of skin cancer. J. Pharm. Investig. 2022, 52, 775–785. [Google Scholar] [CrossRef]
- Gupta, R.; Badhe, Y.; Rai, B.; Mitragotri, S. Molecular mechanism of the skin permeation enhancing effect of ethanol: A molecular dynamics study. RSC Adv. 2020, 10, 12234–12248. [Google Scholar] [CrossRef]
- Karakatsani, M.; Dedhiya, M.; Plakogiannis, F.M. The effect of permeation enhancers on the viscosity and the release profile of transdermal hydroxypropyl methylcellulose gel formulations containing diltiazem HCl. Drug Dev. Ind. Pharm. 2010, 36, 1195–1206. [Google Scholar] [CrossRef]
- Subedi, L.; Pandey, P.; Shim, J.H.; Kim, K.T.; Cho, S.S.; Koo, K.T.; Kim, B.J.; Park, J.W. Preparation of topical bimatoprost with enhanced skin infiltration and in vivo hair regrowth efficacy in androgenic alopecia. Drug Deliv. 2022, 29, 328–341. [Google Scholar] [CrossRef] [PubMed]
- Clausen, M.-L.; Slotved, H.-C.; Krogfelt, K.A.; Agner, T. Tape stripping technique for stratum corneum protein analysis. Sci. Rep. 2016, 6, 19918. [Google Scholar] [CrossRef]
- Subedi, L.; Song, S.-Y.; Jha, S.K.; Lee, S.-H.; Pangeni, R.; Koo, K.-T.; Kim, B.J.; Cho, S.-S.; Park, J.W. Preparation of Topical Itraconazole with Enhanced Skin/Nail Permeability and In Vivo Antifungal Efficacy against Superficial Mycosis. Pharmaceutics 2021, 13, 622. [Google Scholar] [CrossRef] [PubMed]
- Lachenmeier, D.W. Safety evaluation of topical applications of ethanol on the skin and inside the oral cavity. J. Occup. Med. Toxicol. 2008, 3, 26–41. [Google Scholar] [CrossRef]
- Kim, Y.; Lim, K.M. Skin barrier dysfunction and filaggrin. Arch. Pharm. Res. 2021, 44, 36–48. [Google Scholar] [CrossRef]
- Yu, Y.Q.; Yang, X.; Wu, X.F.; Fan, Y.B. Enhancing Permeation of Drug Molecules Across the Skin via Delivery in Nanocarriers: Novel Strategies for Effective Transdermal Applications. Front. Bioeng. Biotechnol. 2021, 9, 646554–646570. [Google Scholar] [CrossRef]
- Souto, E.B.; Fangueiro, J.F.; Fernandes, A.R.; Cano, A.; Sanchez-Lopez, E.; Garcia, M.L.; Severino, P.; Paganelli, M.O.; Chaud, M.V.; Silva, A.M. Physicochemical and biopharmaceutical aspects influencing skin permeation and role of SLN and NLC for skin drug delivery. Heliyon 2022, 8, 8938–8953. [Google Scholar] [CrossRef] [PubMed]
- Ossowicz, P.; Klebeko, J.; Janus, E.; Nowak, A.; Duchnik, W.; Kucharski, Ł.; Klimowicz, A. The effect of alcohols as vehicles on the percutaneous absorption and skin retention of ibuprofen modified with l-valine alkyl esters. RSC Adv. 2020, 10, 41727–41740. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Durrani, M.J.; Reddy, I.K.; Khan, M.A. Effect of permeation enhancers on the release of ketoprofen through transdermal drug delivery systems. Pharmazie 1996, 51, 741–744. [Google Scholar]
- Suh, H.; Jun, H.W. Effectiveness and mode of action of isopropyl myristate as a permeation enhancer for naproxen through shed snake skin. J. Pharm. Pharmacol. 1996, 48, 812–816. [Google Scholar] [CrossRef] [PubMed]
- Carrer, V.; Alonso, C.; Pont, M.; Zanuy, M.; Córdoba, M.; Espinosa, S.; Barba, C.; Oliver, M.A.; Martí, M.; Coderch, L. Effect of propylene glycol on the skin penetration of drugs. Arch. Dermatol. Res. 2020, 312, 337–352. [Google Scholar] [CrossRef]
- Haq, A.; Dorrani, M.; Goodyear, B.; Joshi, V.; Michniak-Kohn, B. Membrane properties for permeability testing: Skin versus synthetic membranes. Int. J. Pharm. 2018, 539, 58–64. [Google Scholar] [CrossRef]
- Tan, G.; Xu, P.; Lawson, L.B.; He, J.; Freytag, L.C.; Clements, J.D.; John, V.T. Hydration effects on skin microstructure as probed by high-resolution cryo-scanning electron microscopy and mechanistic implications to enhanced transcutaneous delivery of biomacromolecules. J. Pharm. Sci. 2010, 99, 730–740. [Google Scholar] [CrossRef]
- Taghiabadi, E.; Nilforoushzadeh, M.A.; Aghdami, N. Maintaining Hair Inductivity in Human Dermal Papilla Cells: A Review of Effective Methods. Skin Pharmacol. Physiol. 2020, 33, 280–292. [Google Scholar] [CrossRef]
- Herce, H.D.; Garcia, A.E.; Cardoso, M.C. Fundamental Molecular Mechanism for the Cellular Uptake of Guanidinium-Rich Molecules. J. Am. Chem. Soc. 2014, 136, 17459–17467. [Google Scholar] [CrossRef]
- Yang, C.; Lim, W.; Bazer, F.W.; Song, G. Oleic acid stimulation of motility of human extravillous trophoblast cells is mediated by stearoyl-CoA desaturase-1 activity. Mol. Hum. Reprod. 2017, 23, 755–770. [Google Scholar] [CrossRef]
- Piraccini, B.M.; Alessandrini, A. Androgenetic alopecia. G. Ital. Dermatol. Venereol. 2014, 149, 15–24. [Google Scholar] [PubMed]
- Kische, H.; Arnold, A.; Gross, S.; Wallaschofski, H.; Völzke, H.; Nauck, M.; Haring, R. Sex Hormones and Hair Loss in Men From the General Population of Northeastern Germany. JAMA Dermatol. 2017, 153, 935–937. [Google Scholar] [CrossRef] [PubMed]
- Steiner, J.F. Clinical pharmacokinetics and pharmacodynamics of finasteride. Clin. Pharmacokinet. 1996, 30, 16–27. [Google Scholar] [CrossRef]
- Lundahl, A.; Hedeland, M.; Bondesson, U.; Knutson, L.; Lennernäs, H. The effect of St. John’s wort on the pharmacokinetics, metabolism and biliary excretion of finasteride and its metabolites in healthy men. Eur. J. Pharm. Sci. 2009, 36, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Bejaoui, M.; Villareal, M.O.; Isoda, H. β-catenin-mediated hair growth induction effect of 3,4,5-tri-O-caffeoylquinic acid. Aging 2019, 11, 4216–4237. [Google Scholar] [CrossRef] [PubMed]
- Burger, P.E.; Gupta, R.; Xiong, X.; Ontiveros, C.S.; Salm, S.N.; Moscatelli, D.; Wilson, E.L. High aldehyde dehydrogenase activity: A novel functional marker of murine prostate stem/progenitor cells. Stem Cells 2009, 27, 2220–2228. [Google Scholar] [CrossRef]
- Everts, H.B. Endogenous retinoids in the hair follicle and sebaceous gland. Biochim.Biophys. Acta. 2012, 1821, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.; Guerrero-Juarez, C.F.; Plikus, M.V. Hair Follicle Signaling Networks: A Dermal Papilla–Centric Approach. J. Investig. Dermatol. 2013, 133, 2306–2308. [Google Scholar] [CrossRef]
- Tomita, H.; Tanaka, K.; Tanaka, T.; Hara, A. Aldehyde dehydrogenase 1A1 in stem cells and cancer. Oncotarget. 2016, 7, 11018–11032. [Google Scholar] [CrossRef]
- Cojoc, M.; Peitzsch, C.; Kurth, I.; Trautmann, F.; Kunz-Schughart, L.A.; Telegeev, G.D.; Stakhovsky, E.A.; Walker, J.R.; Simin, K.; Lyle, S.; et al. Aldehyde Dehydrogenase Is Regulated by β-Catenin/TCF and Promotes Radioresistance in Prostate Cancer Progenitor Cells. Cancer Res. 2015, 75, 1482–1494. [Google Scholar] [CrossRef]
- Ryu, Y.C.; Kim, Y.-R.; Park, J.; Choi, S.; Ryu, W.-J.; Kim, G.-U.; Kim, E.; Hwang, Y.; Kim, H.; Lee, S.-H. Pyruvate Kinase M2 Promotes Hair Regeneration by Connecting Metabolic and Wnt//β-Catenin Signaling. Pharmaceutics 2022, 14, 2774. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulations (%, w/w) | AA | Propylene Glycol | Transcutol P | Isopropyl Myristate | Polyethylene Glycol 400 | Oleic Acid | Ethanol | Water |
|---|---|---|---|---|---|---|---|---|
| AA–TF#1 | 1 | 49.5 | 49.5 | |||||
| AA–TF#2 | 1 | 9.9 | 44.6 | 44.5 | ||||
| AA–TF#3 | 1 | 9.9 | 44.6 | 44.5 | ||||
| AA–TF#4 | 1 | 9.9 | 44.6 | 44.5 | ||||
| AA–TF#5 | 1 | 9.9 | 44.6 | 44.5 | ||||
| AA–TF#6 | 1 | 9.9 | 44.6 | 44.5 | ||||
| AA–TF#7 | 1 | 8.3 | 8.3 | 41.2 | 41.2 | |||
| AA–TF#8 | 1 | 15.2 | 7.6 | 38.1 | 38.1 | |||
| AA–TF#9 | 1 | 26.4 | 6.6 | 33.0 | 33.0 | |||
| AA–TF#10 | 1 | 29.7 | 0.5 | 49.5 | 19.3 | |||
| AA–TF#11 | 1 | 29.7 | 1 | 49.5 | 18.8 | |||
| AA–TF#12 | 1 | 29.7 | 1.5 | 49.5 | 18.3 | |||
| AA–TF#13 | 1 | 29.7 | 2 | 49.5 | 17.8 | |||
| AA–TF#14 | 1 | 5 | 39.5 | 54.5 | ||||
| AA–TF#15 | 1 | 9.9 | 39.5 | 49.6 | ||||
| AA–TF#16 | 1 | 19.8 | 39.5 | 39.7 | ||||
| AA–TF#17 | 1 | 5 | 49.5 | 44.5 | ||||
| AA–TF#18 | 1 | 9.9 | 49.5 | 39.6 | ||||
| AA–TF#19 | 1 | 19.8 | 49.5 | 29.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pulat, S.; Subedi, L.; Pandey, P.; Bhosle, S.R.; Hur, J.-S.; Shim, J.-H.; Cho, S.-S.; Kim, K.-T.; Ha, H.-H.; Kim, H.; et al. Topical Delivery of Atraric Acid Derived from Stereocaulon japonicum with Enhanced Skin Permeation and Hair Regrowth Activity for Androgenic Alopecia. Pharmaceutics 2023, 15, 340. https://doi.org/10.3390/pharmaceutics15020340
Pulat S, Subedi L, Pandey P, Bhosle SR, Hur J-S, Shim J-H, Cho S-S, Kim K-T, Ha H-H, Kim H, et al. Topical Delivery of Atraric Acid Derived from Stereocaulon japonicum with Enhanced Skin Permeation and Hair Regrowth Activity for Androgenic Alopecia. Pharmaceutics. 2023; 15(2):340. https://doi.org/10.3390/pharmaceutics15020340
Chicago/Turabian StylePulat, Sultan, Laxman Subedi, Prashant Pandey, Suresh R. Bhosle, Jae-Seoun Hur, Jung-Hyun Shim, Seung-Sik Cho, Ki-Taek Kim, Hyung-Ho Ha, Hangun Kim, and et al. 2023. "Topical Delivery of Atraric Acid Derived from Stereocaulon japonicum with Enhanced Skin Permeation and Hair Regrowth Activity for Androgenic Alopecia" Pharmaceutics 15, no. 2: 340. https://doi.org/10.3390/pharmaceutics15020340
APA StylePulat, S., Subedi, L., Pandey, P., Bhosle, S. R., Hur, J.-S., Shim, J.-H., Cho, S.-S., Kim, K.-T., Ha, H.-H., Kim, H., & Park, J. W. (2023). Topical Delivery of Atraric Acid Derived from Stereocaulon japonicum with Enhanced Skin Permeation and Hair Regrowth Activity for Androgenic Alopecia. Pharmaceutics, 15(2), 340. https://doi.org/10.3390/pharmaceutics15020340