

What Are the Key Anatomical Features for the Success of Nose-to-Brain Delivery? A Study of Powder Deposition in 3D-Printed Nasal Casts
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Nasal Cast
2.1.1. Choice of the Patients
2.1.2. Creation of 3D-Printed Nasal Casts from the CT Scans
2.2. Methods
2.2.1. Design of Experiments
2.2.2. Deposition Tests
2.3. Cast Classification
2.3.1. Geometrical Characterisation of the Anatomies
2.3.2. Correlation between Anatomy and Deposition
2.3.3. Anatomy Clustering
3. Results and Discussion
3.1. Individual Optimisation of the Delivery in the Olfactory Region
3.2. Classification by Anatomical Trait
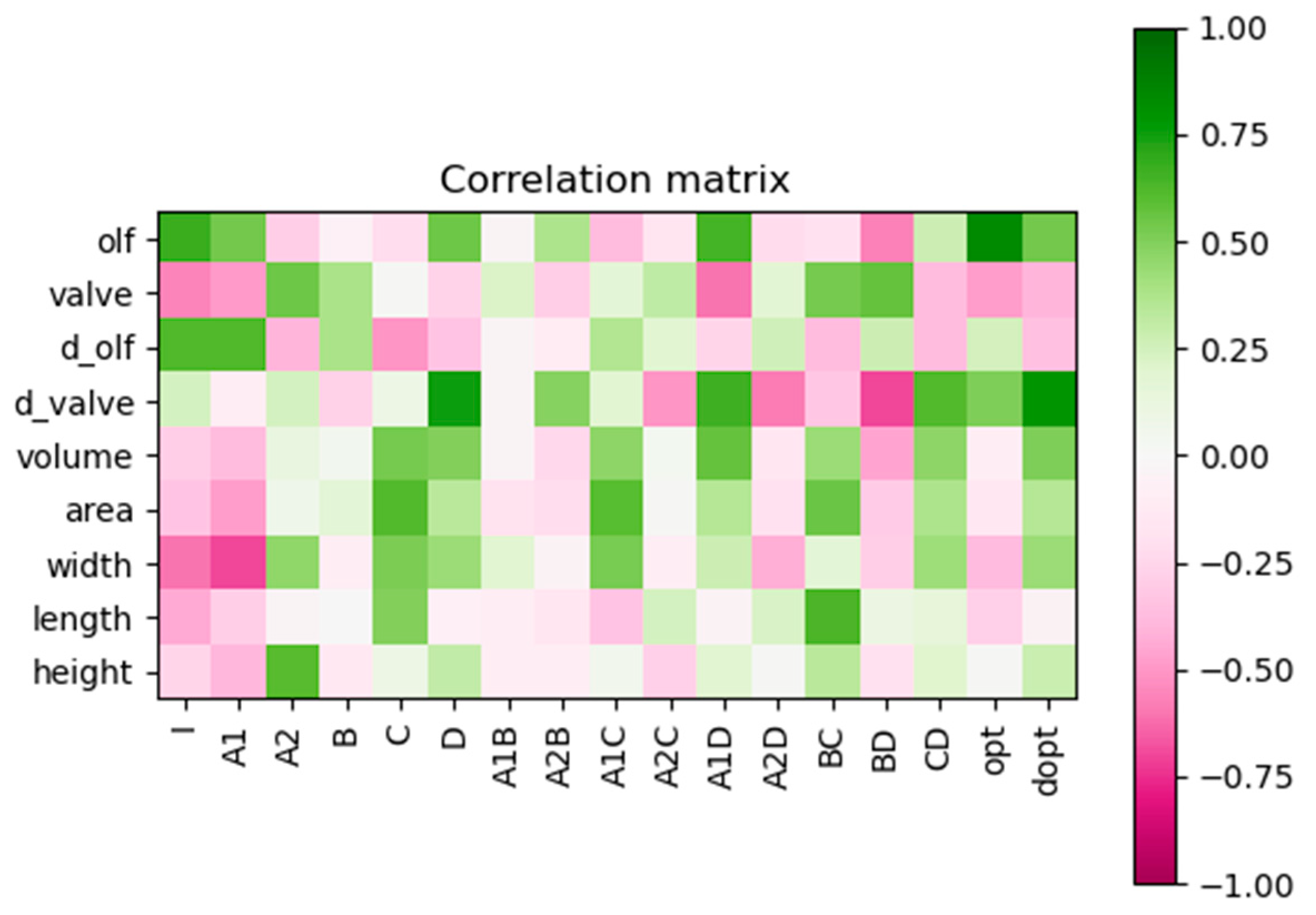
3.3. Correlation between the Anatomy and the Predictive Deposition Model
3.4. Deposition Efficiency Prediction
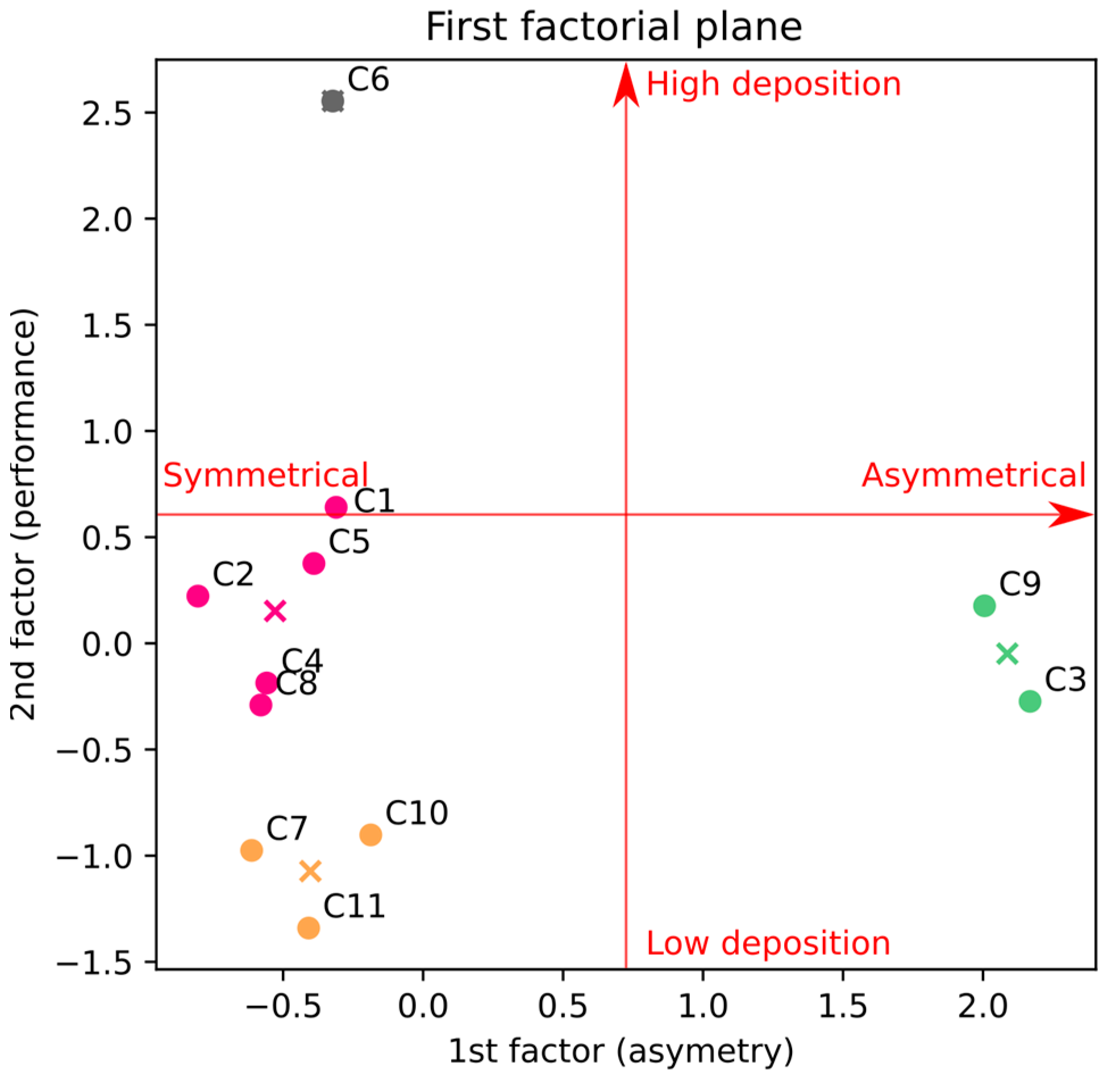
3.5. Exploratory Factor Analysis and Clustering
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| DLS | Dynamic light scattering |
| DoE | Design of Experiments |
| EMA | European Medicines Agency |
| ENT | Ear–Nose–Throat |
| N2B | Nose-to-brain |
| NSD | Nasal septal deviation |
| SNES | Simulated nasal electrolyte solution |
| UDS | Unidose System |
References
- Aschenbrenner, D.S. New Nasal Spray for Migraine Headaches. AJN Am. J. Nurs. 2023, 123, 16. [Google Scholar] [CrossRef]
- Johnson, B.; Freitag, F.G. New Approaches to Shifting the Migraine Treatment Paradigm. Front. Pain Res. 2022, 3, 873179. [Google Scholar] [CrossRef]
- Naguy, A.; Alayadhi, N.; Pridmore, S.; Alhazeem, H.; Alamiri, B. 2023 FDA-approved psychotropic medications. Asian J. Psychiatr. 2023, 87, 103684. [Google Scholar] [CrossRef] [PubMed]
- AL-Tabbaa, M.M.; Bdiwi, E.; Endress, K.; Altarras, K. The Significant Impact of Narcan Reversals on Overdose Mortality in Peoria County, IL. Cureus 2022, 14, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Illum, L. Transport of drugs from the nasal cavity to the central nervous system. Eur. J. Pharm. Sci. 2000, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.L.; Wang, L.H.; Yang, T.; Sun, J.Y.; Mao, L.L.; Yang, M.F.; Yuan, H.; Colvin, R.A.; Yang, X.Y. Lymphatic drainage system of the brain: A novel target for intervention of neurological diseases. Prog. Neurobiol. 2018, 163, 118–143. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.; Saraf, S. Nose-to-brain drug delivery approach: A key to easily accessing the brain for the treatment of Alzheimer’s disease. Neural Regen. Res. 2018, 13, 2102. [Google Scholar] [CrossRef]
- Giunchedi, P.; Gavini, E. Nose-to-Brain Delivery. Pharmaceutics 2020, 12, 138. [Google Scholar] [CrossRef]
- Illum, L. Nasal drug delivery: New developments and strategies. Drug Discov. Today 2002, 7, 1184–1189. [Google Scholar] [CrossRef]
- Martin, V.; Hoekman, J.; Aurora, S.K.; Shrewsbury, S.B. Nasal delivery of acute medications for migraine: The upper versus lower nasal space. J. Clin. Med. 2021, 10, 2468. [Google Scholar] [CrossRef]
- Naclerio, R.M.; Pinto, J.; Assanasen, P.; Baroody, F.M. Observations on the ability of the nose to warm and humidify inspired air. Rhinology 2007, 45, 102–111. [Google Scholar] [PubMed]
- Deruyver, L.; Rigaut, C.; Lambert, P.; Haut, B.; Goole, J. The importance of pre-formulation studies and of 3D-printed nasal casts in the success of a pharmaceutical product intended for nose-to-brain delivery. Adv. Drug Deliv. Rev. 2021, 175, 113826. [Google Scholar] [CrossRef]
- Sawarkar, S.; Suman, J. Nasal Drug Delivery System: Regulatory Perspective. In Nasal Drug Delivery; Springer International Publishing: Cham, Switzerland, 2023; pp. 393–416. [Google Scholar]
- EMA. Doc Ref.: EMEA/CHMP/QWP/49313/2005 Corr: Committee for Medicinal Products for Human Use (CHMP) Guide-Line on the Pharmaceutical Quality of Inhalation and Nasal Products Draft Agreed by Quality Working Party Agreed by Quality Working Party. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-pharmaceutical-quality-inhalation-nasal-products_en.pdf (accessed on 2 October 2023).
- Chow, M.Y.T.; Tai, W.; Chang, R.Y.K.; Chan, H.K.; Kwok, P.C.L. In vitro-in vivo correlation of cascade impactor data for orally inhaled pharmaceutical aerosols. Adv. Drug Deliv. Rev. 2021, 177, 113952. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.; Boussel, L.; Taconnet, F.; Serfaty, J.M.; Alsaid, H.; Attia, C.; Huet, L.; Douek, P. In vitro non-rigid life-size model of aortic arch aneurysm for endovascular prosthesis assessment. Eur. J. Cardio-Thorac. Surg. 2008, 33, 53–57. [Google Scholar] [CrossRef]
- Borup, D.D.; Engel, L.E.; Elkins, C.J.; Eaton, J.K. Transport and dispersion of particle-Laden streaks in a standardized human nasal geometry. Exp. Fluids 2020, 61, 43. [Google Scholar] [CrossRef]
- Keustermans, W.; Huysmans, T.; Schmelzer, B.; Sijbers, J.; Dirckx, J.J.J. The effect of nasal shape on the thermal conditioning of inhaled air: Using clinical tomographic data to build a large-scale statistical shape model. Comput. Biol. Med. 2020, 117, 103600. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.W.; Del Signore, A.G.; Raithatha, R.; Senior, B.A. Nasal airway obstruction: Prevalence and anatomic contributors. Ear, Nose Throat J. 2018, 97, 173–176. [Google Scholar] [CrossRef]
- Mladina, R.; Čujić, E.; Šubarić, M.; Vuković, K. Nasal septal deformities in ear, nose, and throat patients. An international study. Am. J. Otolaryngol.-Head Neck Med. Surg. 2008, 29, 75–82. [Google Scholar] [CrossRef]
- Sánchez Trocino, B.; De la Fuente Hernández, J.; Díaz Acevedo, J.A.; Vilar Pineda, G. Alterations and Pathologies Prevalence in Panoramic Radiographs in Patients Attending the University Dental Clinic. Int. J. Odontostomatol. 2013, 7, 47–52. [Google Scholar] [CrossRef]
- Öberg, D.; Åkerlund, A.; Johansson, L.; Bende, M. Prevalence of nasal septal perforation: The Skövde population-based study. Rhinology 2003, 41, 72–75. [Google Scholar]
- Pereira, C.; Santamaría, A.; Langdon, C.; López-Chacón, M.; Hernández-Rodríguez, J.; Alobid, I. Nasoseptal Perforation: From Etiology to Treatment. Curr. Allergy Asthma Rep. 2018, 18, 5. [Google Scholar] [CrossRef]
- Ertekin, T.; Deermenci, M.; Nisari, M.; Unur, E.; Cokun, A. Age-related changes of nasal cavity and conchae volumes and volume fractions in children: A stereological study. Folia Morphol. 2016, 75, 38–47. [Google Scholar] [CrossRef]
- Gao, M.; Shen, X.; Mao, S. Factors influencing drug deposition in the nasal cavity upon delivery via nasal sprays. J. Pharm. Investig. 2020, 50, 251–259. [Google Scholar] [CrossRef]
- Calmet, H.; Inthavong, K.; Eguzkitza, B.; Lehmkuhl, O.; Houzeaux, G.; Vázquez, M. Nasal sprayed particle deposition in a human nasal cavity under different inhalation conditions. PLoS ONE 2019, 14, e0221330. [Google Scholar] [CrossRef] [PubMed]
- Tong, X.; Dong, J.; Shang, Y.; Inthavong, K.; Tu, J. Effects of nasal drug delivery device and its orientation on sprayed particle deposition in a realistic human nasal cavity. Comput. Biol. Med. 2016, 77, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Moraga-Espinoza, D.; Warnken, Z.; Moore, A.; Williams, R.O.; Smyth, H.D.C.C. A modified USP induction port to characterize nasal spray plume geometry and predict turbinate deposition under flow. Int. J. Pharm. 2018, 548, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-S.; Oh, K.T.; Choi, H.-G.; Lim, S.-J. Liposomal Formulations for Nose-to-Brain Delivery: Recent Advances and Future Perspectives. Pharmaceutics 2019, 11, 540. [Google Scholar] [CrossRef]
- Illum, L. Is nose-to-brain transport of drugs in man a reality? J. Pharm. Pharmacol. 2010, 56, 3–17. [Google Scholar] [CrossRef]
- Hussein, N.R.; Omer, H.K.; Elhissi, A.M.A.; Ahmed, W. Advances in nasal drug delivery systems. In Advances in Medical and Surgical Engineering; Ahmed, W., Phoenix, D.A., Jackson, M.J., Charalambous, C.P., Eds.; Academic Press: Cambridge, MA, USA; Elsevier: Amsterdam, The Netherlands, 2020; pp. 279–311. ISBN 9780128197127. [Google Scholar]
- Moinuddin, S.; Hasan Razvi, S.; Fazil, M.; Mustaneer Akmal, M.; Syed Moinuddin, C.; Shanawaz Uddin, M.; Shahidulla, S. Nasal drug delivery system: A innovative approach. Pharma Innov. J. 2019, 8, 169–177. [Google Scholar]
- Tiozzo Fasiolo, L.; Manniello, M.D.; Tratta, E.; Buttini, F.; Rossi, A.; Sonvico, F.; Bortolotti, F.; Russo, P.; Colombo, G. Opportunity and challenges of nasal powders: Drug formulation and delivery. Eur. J. Pharm. Sci. 2018, 113, 2–17. [Google Scholar] [CrossRef]
- Liu, Y.; Johnson, M.R.; Matida, E.A.; Kherani, S.; Marsan, J. Creation of a standardized geometry of the human nasal cavity. J. Appl. Physiol. 2009, 106, 784–795. [Google Scholar] [CrossRef] [PubMed]
- Rigaut, C.; Deruyver, L.; Goole, J.; Haut, B.; Lambert, P. Instillation of a Dry Powder in Nasal Casts: Parameters Influencing the Olfactory Deposition with Uni- and Bi-Directional Devices. Front. Med. Technol. 2022, 4, 924501. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, D.C. Design and Analysis of Experiments, 10th ed.; Wiley: Hoboken, NJ, USA, 2019; ISBN 978-1-119-49244-3. [Google Scholar]
- Deruyver, L.; Rigaut, C.; Gomez-Perez, A.; Lambert, P.; Haut, B.; Goole, J. In vitro Evaluation of Paliperidone Palmitate Loaded Cubosomes Effective for Nasal-to-Brain Delivery. Int. J. Nanomed. 2023, 18, 1085–1106. [Google Scholar] [CrossRef] [PubMed]
- Scherließ, R. Nasal formulations for drug administration and characterization of nasal preparations in drug delivery. Ther. Deliv. 2020, 11, 183–191. [Google Scholar] [CrossRef]
- Yarragudi, S.B.; Kumar, H.; Jain, R.; Tawhai, M.; Rizwan, S. Olfactory Targeting of Microparticles through Inhalation and Bi-directional Airflow: Effect of Particle Size and Nasal Anatomy. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Hyatt, R.E. Expiratory flow limitation. J. Appl. Physiol. 1983, 55, 1–7. [Google Scholar] [CrossRef]
- Meloun, M.; Militký, J. Correlation. In Statistical Data Analysis; Elsevier: Amsterdam, The Netherlands, 2011; pp. 631–666. [Google Scholar]
- Abdullah, B.; Singh, S. Surgical interventions for inferior turbinate hypertrophy: A comprehensive review of current techniques and technologies. Int. J. Environ. Res. Public Health 2021, 18, 3441. [Google Scholar] [CrossRef]
- Ciprandi, G.; Tosca, M.A. Turbinate Hypertrophy, Allergic Rhinitis, and Otitis Media. Curr. Allergy Asthma Rep. 2021, 21, 44. [Google Scholar] [CrossRef]
- Frank, D.O.; Kimbell, J.S.; Pawar, S.; Rhee, J.S. Effects of anatomy and particle size on nasal sprays and nebulizers. Otolaryngol.-Head Neck Surg. 2012, 146, 313–319. [Google Scholar] [CrossRef]
- Hosseini, S.; Wei, X.; Wilkins, J.V.; Fergusson, C.P.; Mohammadi, R.; Vorona, G.; Golshahi, L. In Vitro Measurement of Regional Nasal Drug Delivery with Flonase,® Flonase® Sensimist,TM and MAD NasalTM in Anatomically Correct Nasal Airway Replicas of Pediatric and Adult Human Subjects. J. Aerosol Med. Pulm. Drug Deliv. 2019, 32, 374–385. [Google Scholar] [CrossRef]
- Trows, S.; Scherließ, R. Carrier-based dry powder formulation for nasal delivery of vaccines utilizing BSA as model drug. Powder Technol. 2016, 292, 223–231. [Google Scholar] [CrossRef]
- Kolanjiyil, A.V.; Alfaifi, A.; Aladwani, G.; Golshahi, L.; Longest, W. Importance of Spray–Wall Interaction and Post-Deposition Liquid Motion in the Transport and Delivery of Pharmaceutical Nasal Sprays. Pharmaceutics 2022, 14, 956. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anatomy | Sex (M/F) * | Age (Years) | Cast |
|---|---|---|---|
| Standard | - | - | C1 |
| Normal | F | - | C2 |
| Normal | F | 92 | C3 |
| Normal | M | 56 | C4 |
| Septum perforation | F | - | C5 |
| Paediatric | F | 7 | C6 |
| Paediatric | F | 11 | C7 |
| Septum deviation | M | 44 | C8 |
| Septum deviation | M | 21 | C9 |
| Turbinate hypertrophy | F | 23 | C10 |
| Turbinate hypertrophy | F | 79 | C11 |
| Factors | Level (1) | Level (2) | Level (3) |
|---|---|---|---|
| A: Device | UDS | TriVair | Miat |
| B: Angle | Centre | Direct | - |
| C: Inspiratory flow (L/min) | 0 | 15 | 30 |
| D: Side | Left | Right | - |
| Device | Dv50 (μm) | Span | Ejection Velocity (m/s) | Plume Angle (°) |
|---|---|---|---|---|
| UDS | 25.21 ± 1.45 | 1.76 ± 0.03 | 49.20 ± 5.97 | 16.83 ± 2.42 |
| TriVair | 69.79 ± 12.20 | 1.89 ± 0.27 | 5.93 ± 0.14 | 3.93 ± 0.29 |
| MIAT | 38.24 ± 8.84 | 1.82 ± 0.37 | 7.49 ± 4.02 | 3.1 ± 0.5 |
| Cast | Total Area of the Olfactory Region (mm2) | Total Area of the Nasal Valve (mm2) | Relative Difference between Left and Right Olfactory Areas (%) | Relative Difference between Left and Right Valve Areas (%) | Overall Volume of the Cavity (mm3) | Overall Area of the Cavity (mm2) | Width (mm) | Length (mm) | Height (mm) |
|---|---|---|---|---|---|---|---|---|---|
| C1 | 1334 | 84 | - | - | 17,226 | 10,220 | 15 | 125 | 48 |
| C2 | 2200 | 213 | 7.76 | 33.96 | 56,637 | 26,331 | 49 | 108 | 69 |
| C3 | 2274 | 123 | 3.88 | 45.41 | 57,949 | 27,395 | 50 | 104 | 67 |
| C4 | 1082 | 226 | 9.44 | 4.31 | 84,385 | 31,109 | 55 | 114 | 40 |
| C5 | 2200 | 213 | 7.76 | 33.96 | 56,637 | 26,331 | 49 | 108 | 69 |
| C6 | 2158 | 98 | 43.63 | 18.73 | 19,063 | 16,854 | 32 | 94 | 36 |
| C7 | 685 | 140 | 14.89 | 11.17 | 69,317 | 27,015 | 46 | 106 | 69 |
| C8 | 1938 | 203 | 10.86 | 16.06 | 81,948 | 42,188 | 44 | 121 | 63 |
| C9 | 3367 | 104 | 10.85 | 42.29 | 118,140 | 39,080 | 55 | 114 | 56 |
| C10 | 1024 | 192 | 2.56 | 22.82 | 71,002 | 32,523 | 54 | 121 | 58 |
| C11 | 723 | 149 | 8.62 | 21.56 | 38,852 | 27,378 | 55 | 107 | 44 |
| Cast | Mean Olfactory Deposition (%) | Maximal Olfactory Deposition (%) | Optimal Parameters to Reach the Olfactory Region | Maximal Deposition Predicted with Each Device (%) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Side | Device | Angle | Inspiratory Flow (L/min) | UDS | TriVair | MIAT | |||
| C1 | 19 | 35 | - | UDS | Centre | 0 | 33 | 13 | 11 |
| C2 | 16 | 40 | No influence | UDS | Direct aim | 0 | 36 | 7 | 21 |
| C3 | 12 | 43 | Right | UDS | Centre | 60 | 48 | 41 | 29 |
| C4 | 7 | 29 | Left | UDS | Direct aim | 60 | 22 | 8 | 5 |
| C5 | 17 | 48 | Right | UDS | Direct aim | 0 | 34 | 18 | 25 |
| C6 | 29 | 59 | No influence | UDS | no influence | No influence | 47 | 24 | 20 |
| C7 | 4 | 12 | No influence | MIAT | Centre | 0 | 9 | 6 | 11 |
| C8 | 11 | 35 | No influence | TriVair | Direct aim | 60 | 25 | 31 | 16 |
| C9 | 12 | 43 | Left | UDS | Direct aim | 60 | 42 | 18 | 21 |
| C10 | 3 | 12 | Right | UDS | no influence | 60 | 17 | 15 | 12 |
| C11 | 3 | 15 | Left | TriVair | Direct aim | 60 | 2 | 12 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigaut, C.; Deruyver, L.; Niesen, M.; Vander Ghinst, M.; Goole, J.; Lambert, P.; Haut, B. What Are the Key Anatomical Features for the Success of Nose-to-Brain Delivery? A Study of Powder Deposition in 3D-Printed Nasal Casts. Pharmaceutics 2023, 15, 2661. https://doi.org/10.3390/pharmaceutics15122661
Rigaut C, Deruyver L, Niesen M, Vander Ghinst M, Goole J, Lambert P, Haut B. What Are the Key Anatomical Features for the Success of Nose-to-Brain Delivery? A Study of Powder Deposition in 3D-Printed Nasal Casts. Pharmaceutics. 2023; 15(12):2661. https://doi.org/10.3390/pharmaceutics15122661
Chicago/Turabian StyleRigaut, Clément, Laura Deruyver, Maxime Niesen, Marc Vander Ghinst, Jonathan Goole, Pierre Lambert, and Benoit Haut. 2023. "What Are the Key Anatomical Features for the Success of Nose-to-Brain Delivery? A Study of Powder Deposition in 3D-Printed Nasal Casts" Pharmaceutics 15, no. 12: 2661. https://doi.org/10.3390/pharmaceutics15122661
APA StyleRigaut, C., Deruyver, L., Niesen, M., Vander Ghinst, M., Goole, J., Lambert, P., & Haut, B. (2023). What Are the Key Anatomical Features for the Success of Nose-to-Brain Delivery? A Study of Powder Deposition in 3D-Printed Nasal Casts. Pharmaceutics, 15(12), 2661. https://doi.org/10.3390/pharmaceutics15122661