
Physiologically Based Biopharmaceutics Modeling of Food Effect for Basmisanil: A Retrospective Case Study of the Utility for Formulation Bridging

Abstract
1. Introduction
2. Materials and Methods
2.1. API and Formulation Properties
2.2. Clinical Pharmacokinetic Data of Basmisanil
2.3. Construction of the Baseline GastroPlus™ Model
2.4. Food Effect Modeling Approach
2.5. Parameter Sensitivity Analysis
3. Results
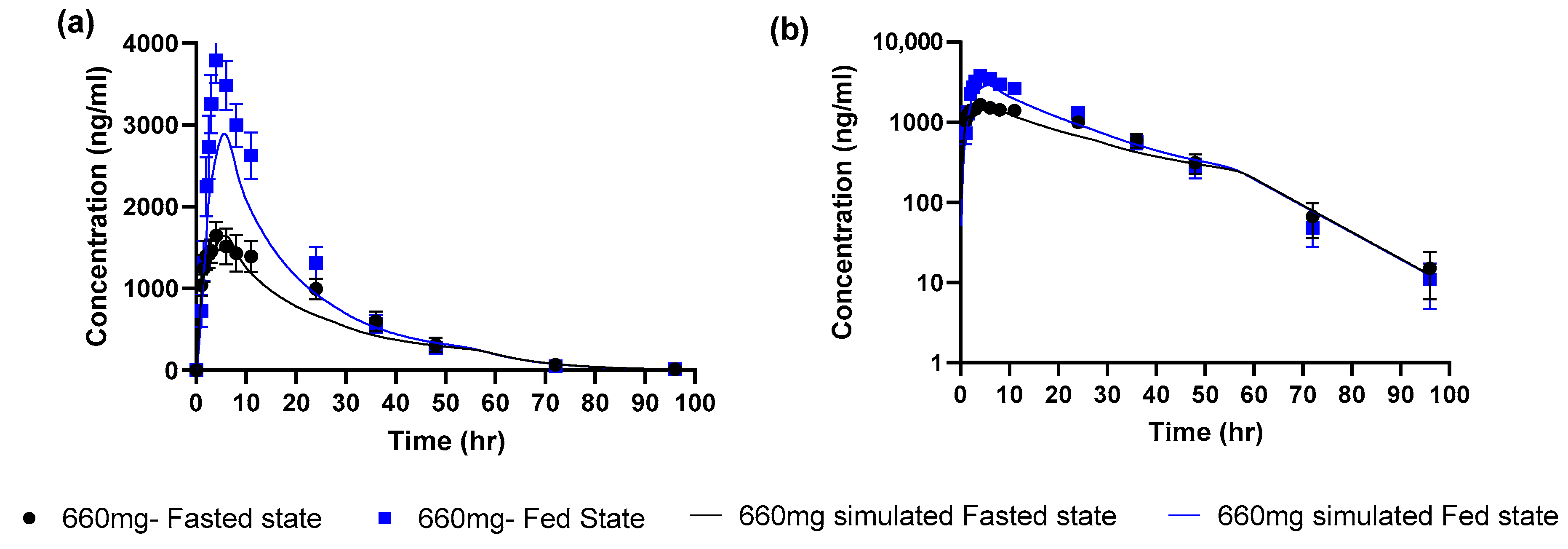
3.1. Simulations for Uncoated Tablet Formulation at a Dose of 660 mg
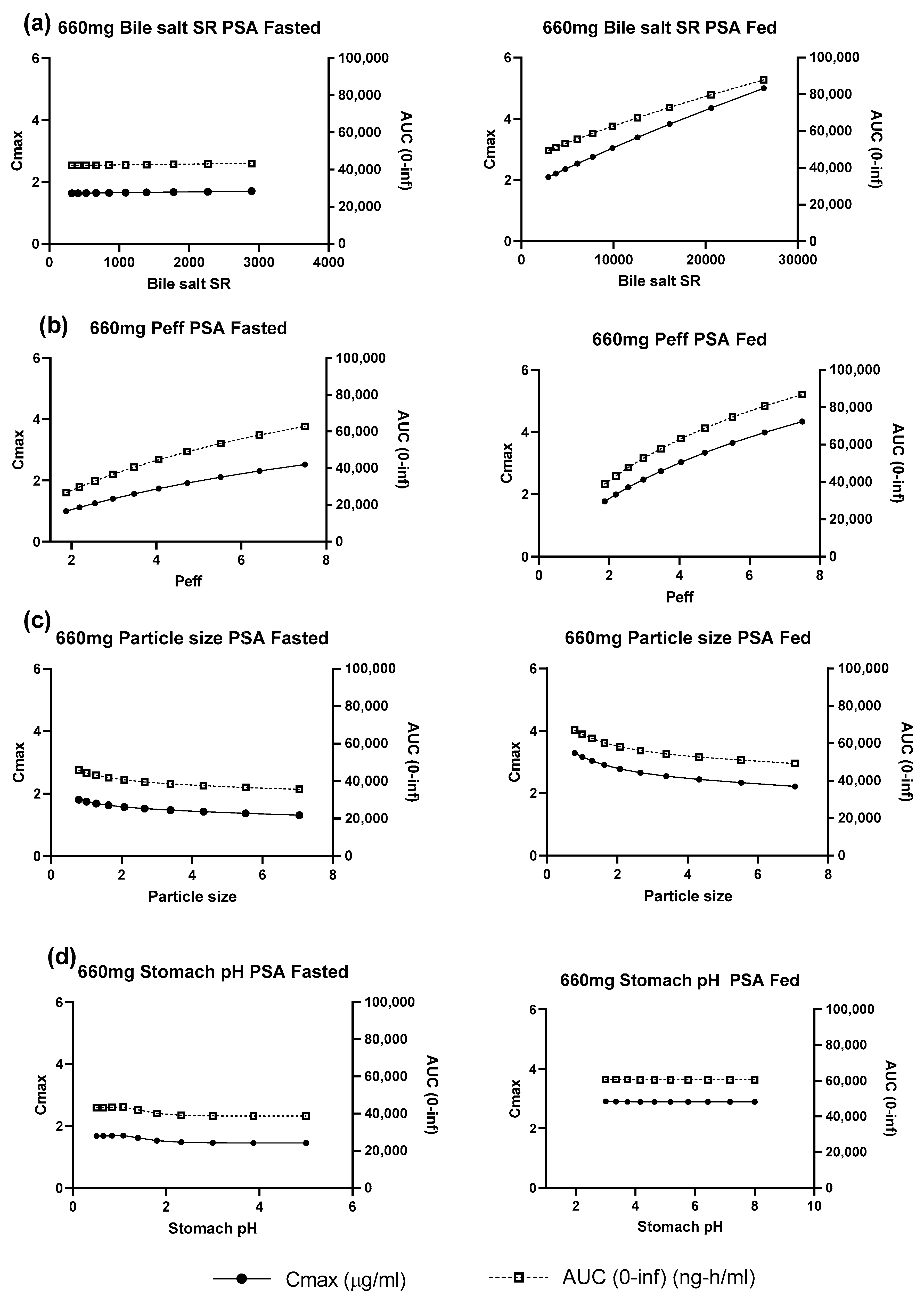
3.2. Model Parameter Sensitivity Analysis at a Dose of 660 mg
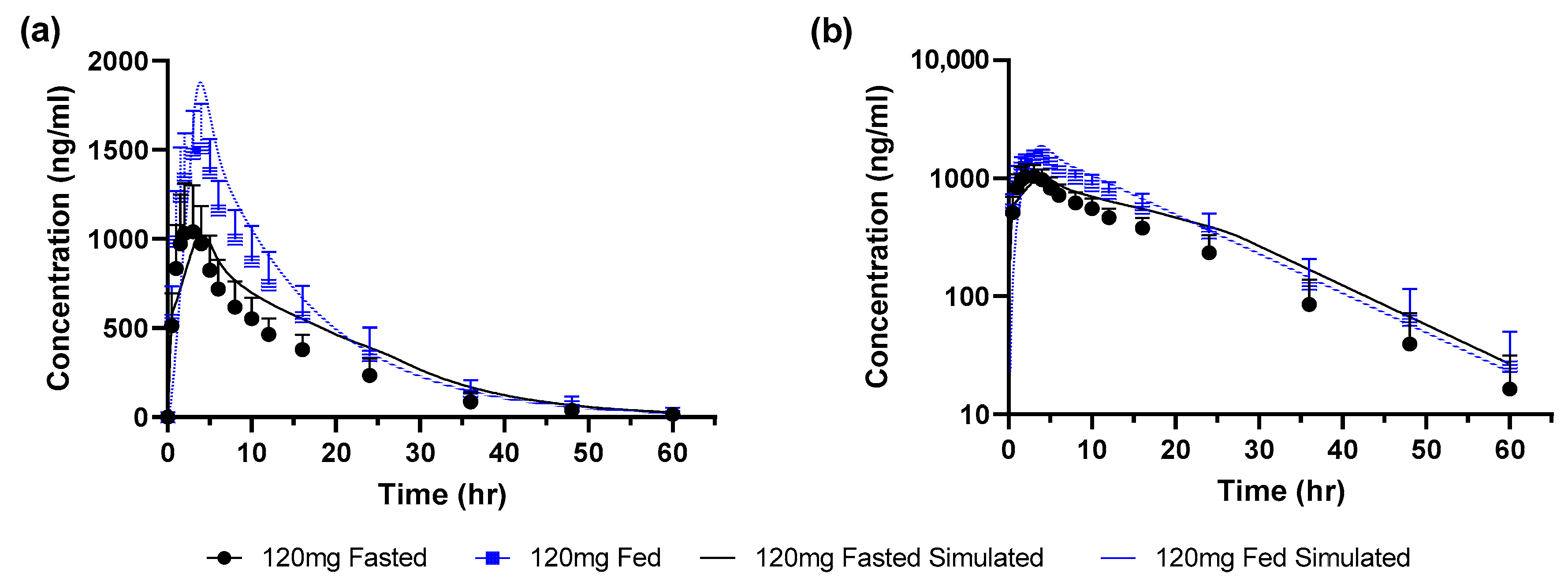
3.3. GastroPlus™ Model Simulations for Granules at a Dose of 120 mg
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jones, H.; Parrott, N.; Ohlenbusch, G.; Lavé, T. Predicting Pharmacokinetic Food Effects Using Biorelevant Solubility Media and Physiologically Based Modelling. Clin. Pharmacokinet. 2006, 45, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Riedmaier, A.; DeMent, K.; Huckle, J.; Bransford, P.; Stillhart, C.; Lloyd, R.; Alluri, R.; Basu, S.; Chen, Y.; Dhamankar, V.; et al. Use of Physiologically Based Pharmacokinetic (PBPK) Modeling for Predicting Drug-Food Interactions: An Industry Perspective. AAPS J. 2020, 22, 123. [Google Scholar] [CrossRef] [PubMed]
- Pepin, X.J.H.; Huckle, J.E.; Alluri, R.V.; Basu, S.; Dodd, S.; Parrott, N.; Emami Riedmaier, A. Understanding Mechanisms of Food Effect and Developing Reliable PBPK Models Using a Middle-out Approach. AAPS J. 2021, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.; Kesisoglou, F.; Pepin, X.J.H.; Parrott, N.; Emami Riedmaier, A. Use of Physiologically Based Pharmacokinetic Modeling for Predicting Drug–Food Interactions: Recommendations for Improving Predictive Performance of Low Confidence Food Effect Models. AAPS J. 2021, 23, 85. [Google Scholar] [CrossRef] [PubMed]
- Tistaert, C.; Heimbach, T.; Xia, B.; Parrott, N.; Samant, T.S.; Kesisoglou, F. Food Effect Projections via Physiologically Based Pharmacokinetic Modeling: Predictive Case Studies. J. Pharm. Sci. 2019, 108, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Koziolek, M.; Alcaro, S.; Augustijns, P.; Basit, A.W.; Grimm, M.; Hens, B.; Hoad, C.L.; Jedamzik, P.; Madla, C.M.; Maliepaard, M.; et al. The mechanisms of pharmacokinetic food-drug interactions—A perspective from the UNGAP group. Eur. J. Pharm. Sci. 2019, 134, 31–59. [Google Scholar] [CrossRef] [PubMed]
- Emami Riedmaier, A. Predicting Food Effects: Are We There Yet? AAPS J. 2022, 24, 25. [Google Scholar] [CrossRef] [PubMed]
- Pepin, X.J.H.; Parrott, N.; Dressman, J.; Delvadia, P.; Mitra, A.; Zhang, X.; Babiskin, A.; Kolhatkar, V.; Suarez-Sharp, S. Current State and Future Expectations of Translational Modeling Strategies to Support Drug Product Development, Manufacturing Changes and Controls: A Workshop Summary Report. J. Pharm. Sci. 2021, 110, 555–566. [Google Scholar] [CrossRef] [PubMed]
- Stillhart, C.; Parrott, N.J.; Lindenberg, M.; Chalus, P.; Bentley, D.; Szepes, A. Characterising Drug Release from Immediate-Release Formulations of a Poorly Soluble Compound, Basmisanil, Through Absorption Modelling and Dissolution Testing. AAPS J. 2017, 19, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Parrott, N.; Lave, T. Applications of Physiologically Based Absorption Models in Drug Discovery and Development. Mol. Pharm. 2008, 5, 760–775. [Google Scholar] [CrossRef] [PubMed]
- Parrott, N.; Lukacova, V.; Fraczkiewicz, G.; Bolger, M. Predicting Pharmacokinetics Of Drugs Using Physiologically Based Modeling—Application To Food Effects. AAPS J. 2009, 11, 45. [Google Scholar] [CrossRef]
- Porter, C.J.H.; Trevaskis, N.L.; Charman, W.N. Lipids and lipid-based formulations: Optimizing the oral delivery of lipophilic drugs. Nat. Rev. Drug Discov. 2007, 6, 231. [Google Scholar] [CrossRef]
- Mithani, S.D.; Bakatselou, V.; TenHoor, C.N.; Dressman, J.B. Estimation of the Increase in solubility of Drugs as a Function of Bile Salt Concentration. Pharm. Res. 1996, 13, 163–167. [Google Scholar] [CrossRef]
- Parrott, N.; Stillhart, C.; Lindenberg, M.; Wagner, B.; Kowalski, K.; Guerini, E.; Djebli, N.; Meneses-Lorente, G. Physiologically Based Absorption Modelling to Explore the Impact of Food and Gastric pH Changes on the Pharmacokinetics of Entrectinib. AAPS J. 2020, 22, 78. [Google Scholar] [CrossRef]
- Mota, F.L.; Carneiro, A.P.; Queimada, A.J.; Pinho, S.P.; Macedo, E.A. Temperature and solvent effects in the solubility of some pharmaceutical compounds: Measurements and modeling. Eur. J. Pharm. Sci. 2009, 37, 499–507. [Google Scholar] [CrossRef]
- Dressman, J.B.; Vertzoni, M.; Goumas, K.; Reppas, C. Estimating drug solubility in the gastrointestinal tract. Adv. Drug Deliv. Rev. 2007, 59, 591–602. [Google Scholar] [CrossRef]
- Pathak, S.M.; Ruff, A.; Kostewicz, E.S.; Patel, N.; Turner, D.B.; Jamei, M. Model-Based Analysis of Biopharmaceutic Experiments To Improve Mechanistic Oral Absorption Modeling: An Integrated in Vitro in Vivo Extrapolation Perspective Using Ketoconazole as a Model Drug. Mol. Pharm. 2017, 14, 4305–4320. [Google Scholar] [CrossRef]
- Jantratid, E.; Janssen, N.; Reppas, C.; Dressman, J.B. Dissolution Media Simulating Conditions in the Proximal Human Gastrointestinal Tract: An Update. Pharm. Res. 2008, 25, 1663. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter * | Value |
|---|---|
| Molecular weight | 445.5 g/mol |
| pKa | 2.07 (base) |
| logD (pH 7.4) | 1.86 |
| Melting point | 148.3 °C |
| Blood/plasma concentration ratio Fraction of drug unbound in plasma | 0.59 5.6% |
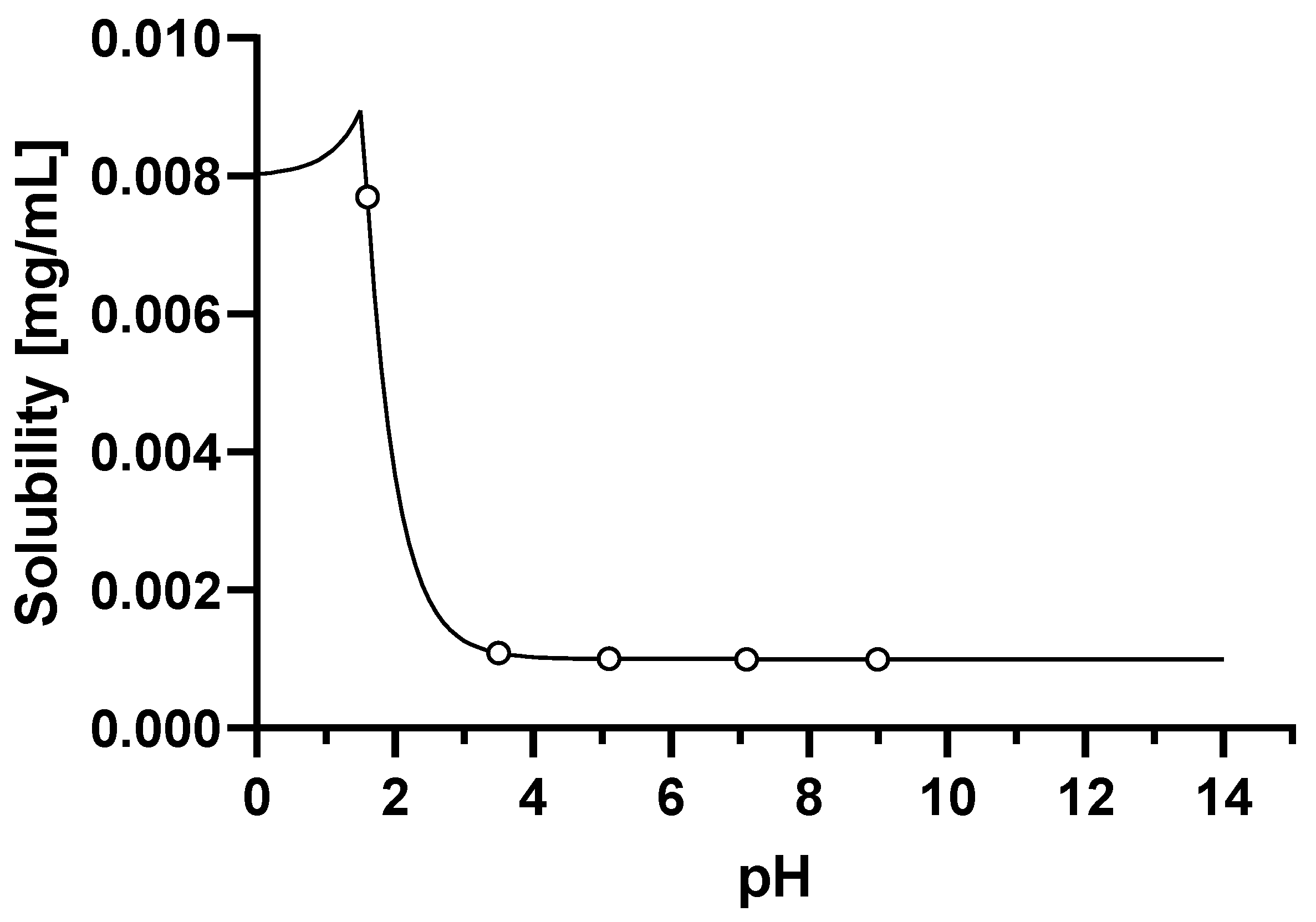
| Solubility at 25 °C | |
| Aqueous buffer pH 1–9 Solubility at 37 °C | 0.001 mg/mL |
| SGF pH 1.6 | 0.008 mg/mL |
| FaSSIF pH 6.5 | 0.010 mg/mL |
| FeSSIF pH 5 | 0.032 mg/mL |
| Particle size distribution | |
| D10 | 1.4 μm |
| D50 | 4.7 μm |
| D90 | 10.1 μm |
| Effective human jejunal permeability | 3.75 × 10−4 cm/s |
| Disposition model parameters | |
| k12 | 1.294 1/h |
| k21 | 0.979 1/h |
| k10 | 0.245 1/h |
| Vc/kg | 0.235 L/kg |
| V2/kg | 0.311 L/kg |
| CL/kg | 0.058 L/h/kg |
| CL2/kg | 0.304 L/h/kg |
| Elimination half-life | 7.0 h |
| Fasted State | Fed State | |||||
|---|---|---|---|---|---|---|
| Parameters | Observed | Simulated | Simulated/Observed | Observed | Simulated | Simulated/Observed |
| Cmax (ng/mL) | 1649 | 1648 | 0.999 | 3787 | 2892 | 0.764 |
| AUCinf (ng.h/mL) | 51,400 | 42,600 | 0.829 | 76,900 | 60,500 | 0.786 |
| Tmax (h) | 4 | 5.74 | 1.435 | 4 | 5.64 | 1.410 |
| Parameters | Fasted State | Fed State | ||||
|---|---|---|---|---|---|---|
| Parameter Range Explored (Baseline) | Cmax (ng/mL) | AUC(0-inf) (ng.h.mL) | Parameter Range Explored (Baseline) | Cmax (ng/mL) | AUC(0-inf) (ng.h.mL) | |
| Peff | 1.87–7.5 (3.75) | 60.4–153 | 62.6–148 | 1.87–7.5 (3.75) | 61.5–150 | 64.3–143 |
| Particle size (D50) | 0.78–7.05 (2.35) | 109–79.5 | 108–83.5 | 0.78–7.05 (2.35) | 113.7–76.7 | 111–81.3 |
| Bile salt Solubiliza-tion Ratio | 323–2897.1 (965.7) | 98.9–103 | 99.5–102 | 2917–26,300 (8753.6) | 72.4–173 | 81.6–145 |
| Stomach pH | 0.5–5 (1.3) | 102–88.1 | 101–90.8 | 4–6 (4.9) | 100–99.9 | 99.9–99.9 |
| Fasted State | Fed State | |||||
|---|---|---|---|---|---|---|
| Parameters | Observed | Simulated | Simulated/Observed | Observed | Simulated | Simulated/Observed |
| Cmax (ng/mL) | 1043 | 1006 | 0.96 | 1513 | 1877 | 1.2 |
| AUCinf (ng.h/mL) | 16,010 | 20,760 | 1.3 | 24,050 | 26,090 | 1.1 |
| Tmax (h) | 3 | 4.26 | 1.4 | 4 | 3.94 | 0.99 |
| Formulation | Simulated | Observed * | Ratio of Simulated/Observed Food Effect | |||
|---|---|---|---|---|---|---|
| Cmax | AUC | Cmax | AUC | Cmax | AUC | |
| 660 mg uncoated tablets | 1.75 | 1.42 | 2.31 | 1.52 | 0.76 | 0.93 |
| 120 mg granules | 1.86 | 1.25 | 1.38 | 1.5 | 1.35 | 0.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belubbi, T.; Bassani, D.; Stillhart, C.; Parrott, N. Physiologically Based Biopharmaceutics Modeling of Food Effect for Basmisanil: A Retrospective Case Study of the Utility for Formulation Bridging. Pharmaceutics 2023, 15, 191. https://doi.org/10.3390/pharmaceutics15010191
Belubbi T, Bassani D, Stillhart C, Parrott N. Physiologically Based Biopharmaceutics Modeling of Food Effect for Basmisanil: A Retrospective Case Study of the Utility for Formulation Bridging. Pharmaceutics. 2023; 15(1):191. https://doi.org/10.3390/pharmaceutics15010191
Chicago/Turabian StyleBelubbi, Tejashree, Davide Bassani, Cordula Stillhart, and Neil Parrott. 2023. "Physiologically Based Biopharmaceutics Modeling of Food Effect for Basmisanil: A Retrospective Case Study of the Utility for Formulation Bridging" Pharmaceutics 15, no. 1: 191. https://doi.org/10.3390/pharmaceutics15010191
APA StyleBelubbi, T., Bassani, D., Stillhart, C., & Parrott, N. (2023). Physiologically Based Biopharmaceutics Modeling of Food Effect for Basmisanil: A Retrospective Case Study of the Utility for Formulation Bridging. Pharmaceutics, 15(1), 191. https://doi.org/10.3390/pharmaceutics15010191