
Efficacy and Safety of Daptomycin versus Vancomycin for Bacteremia Caused by Methicillin-Resistant Staphylococcus aureus with Vancomycin Minimum Inhibitory Concentration > 1 µg/mL: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection Criteria
2.2. Data Extraction and Subgroup Categories
2.3. Statistical Analysis
3. Results
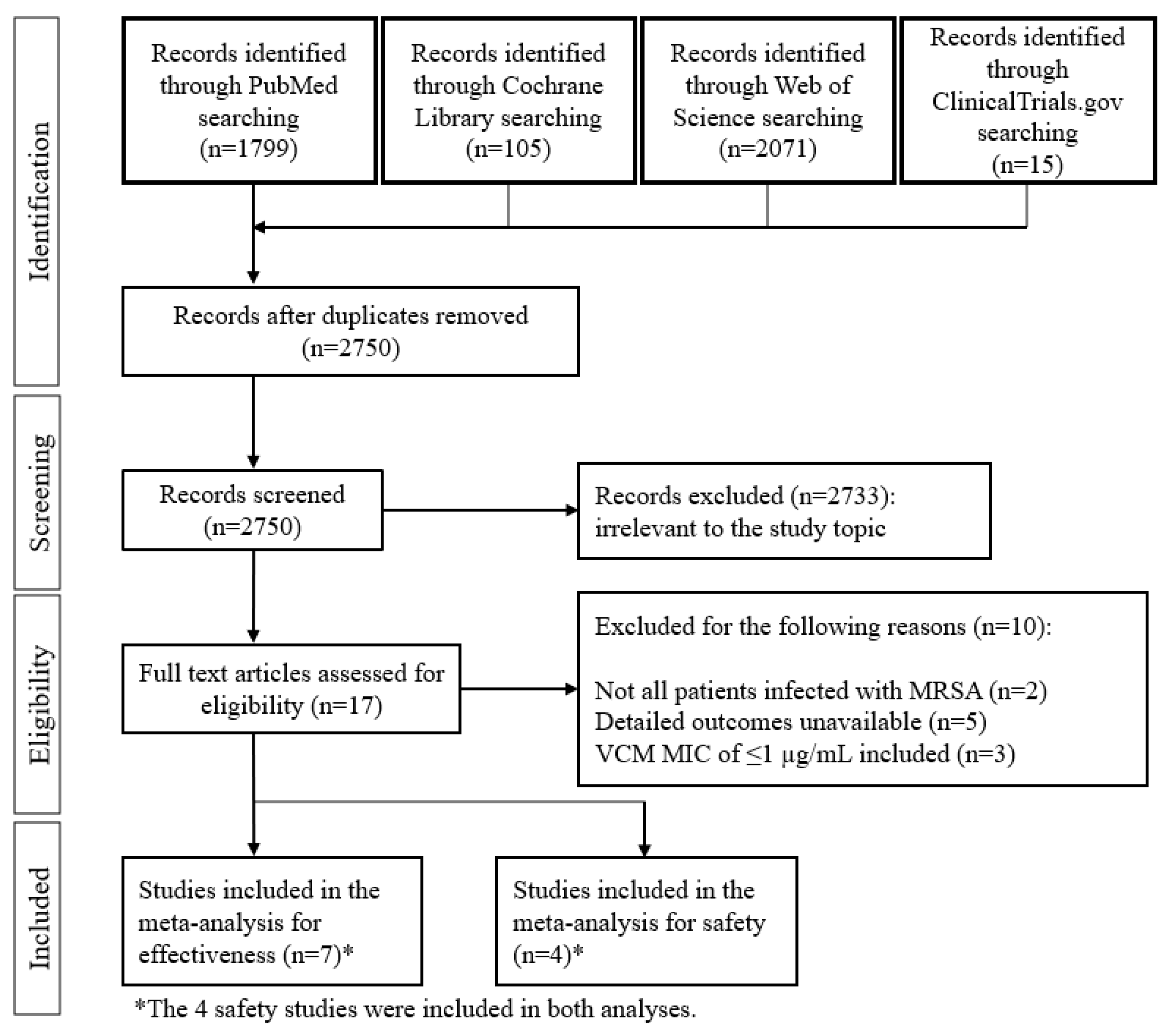
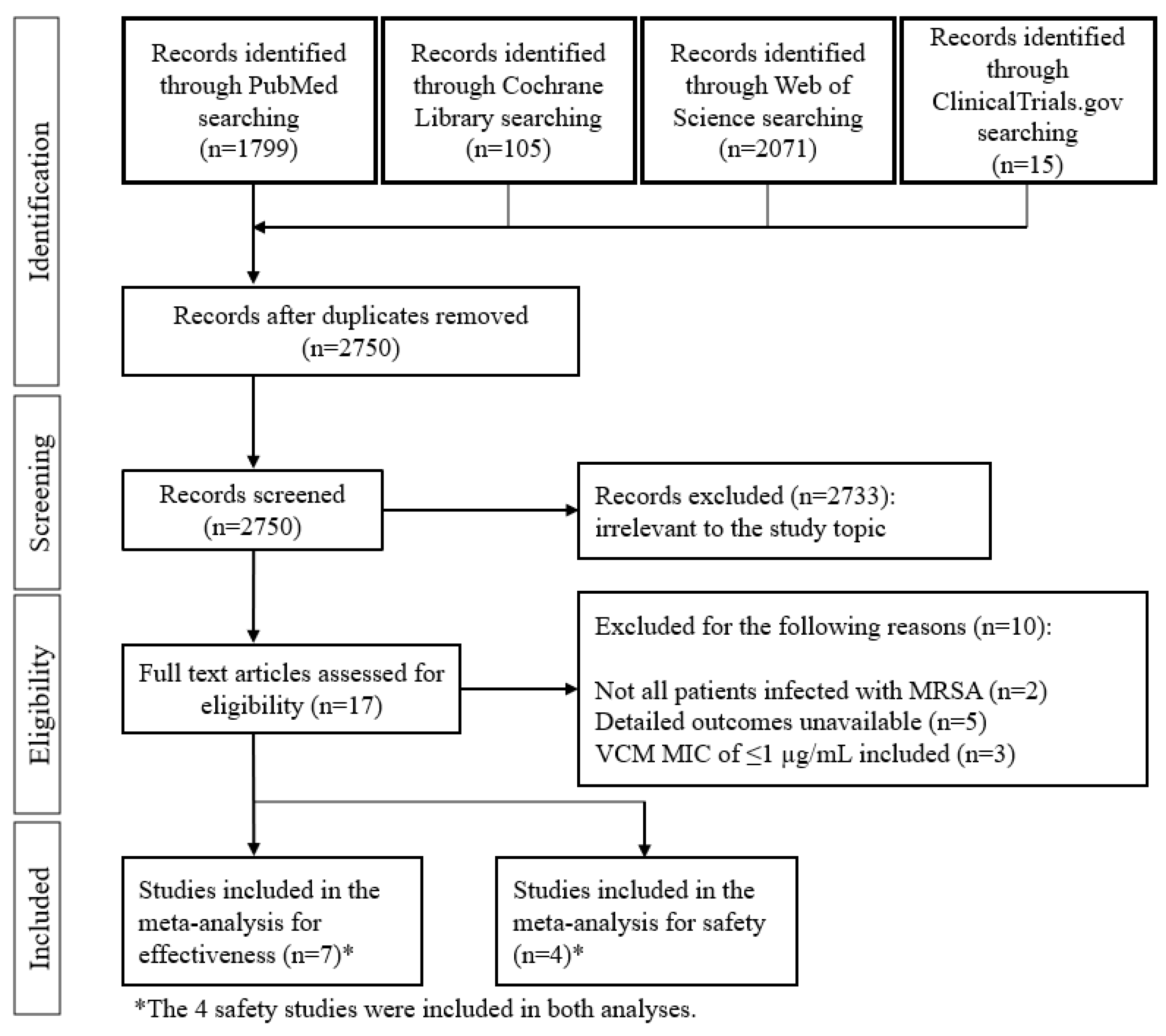
3.1. Search Results
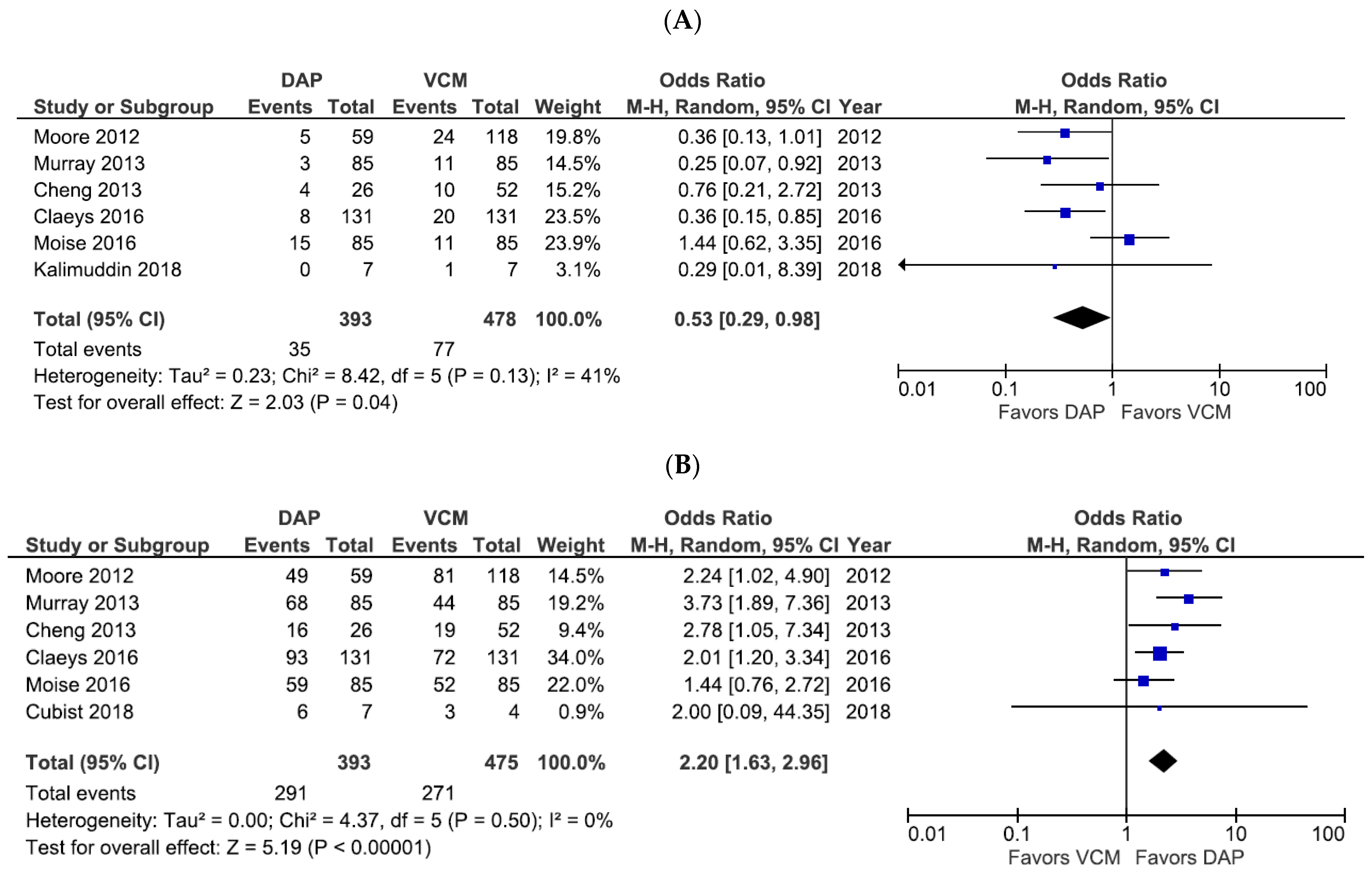
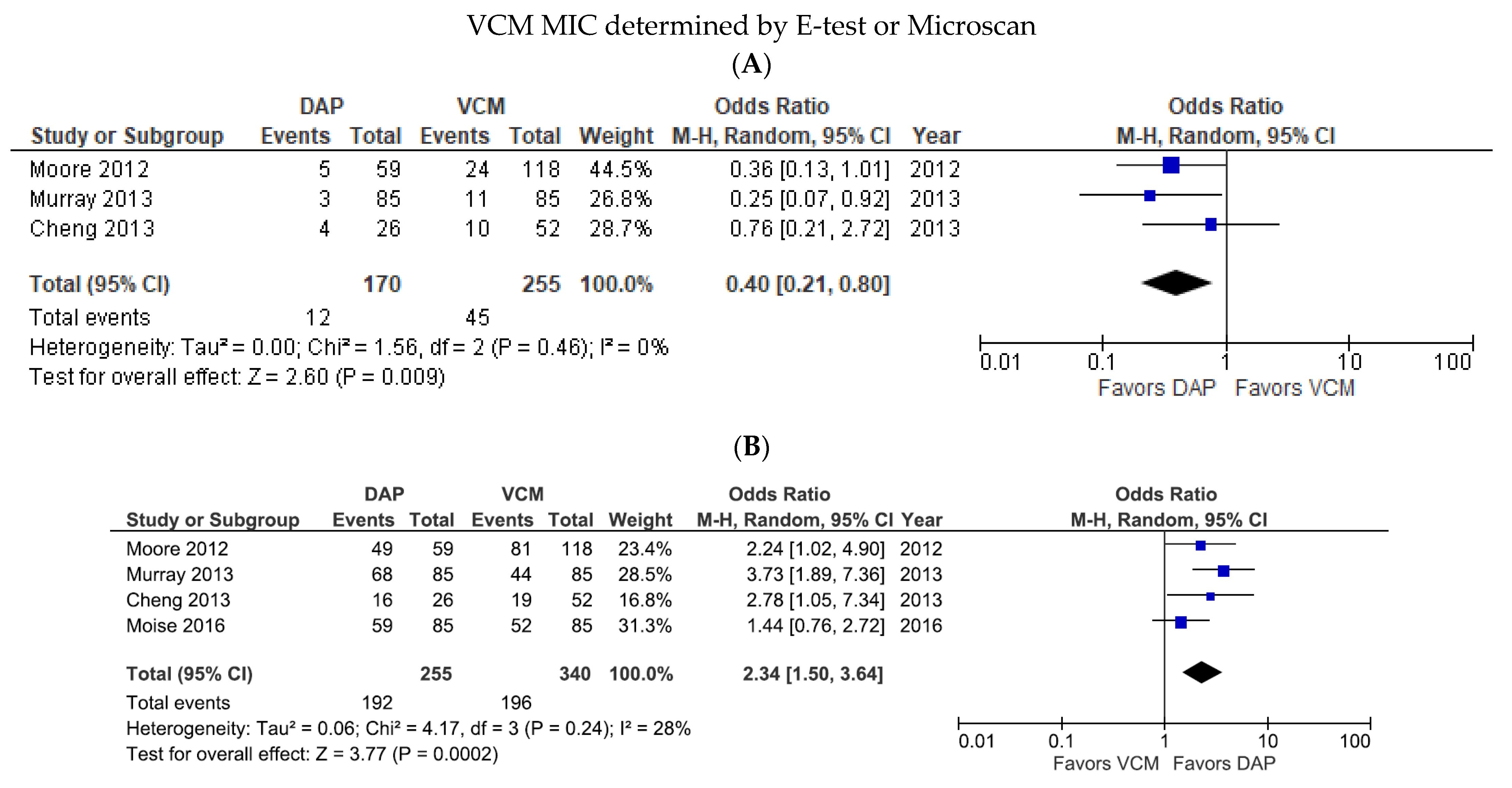
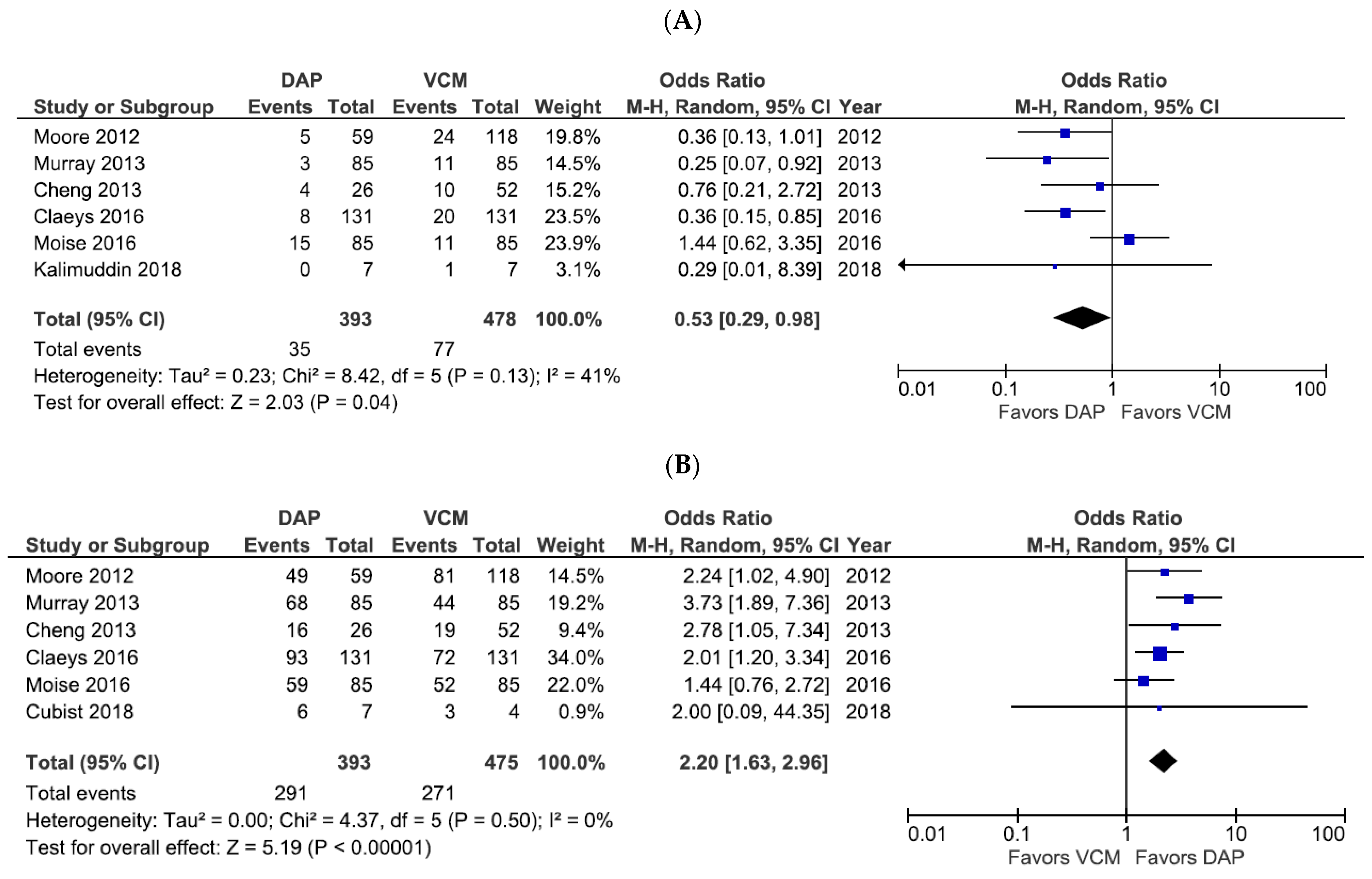
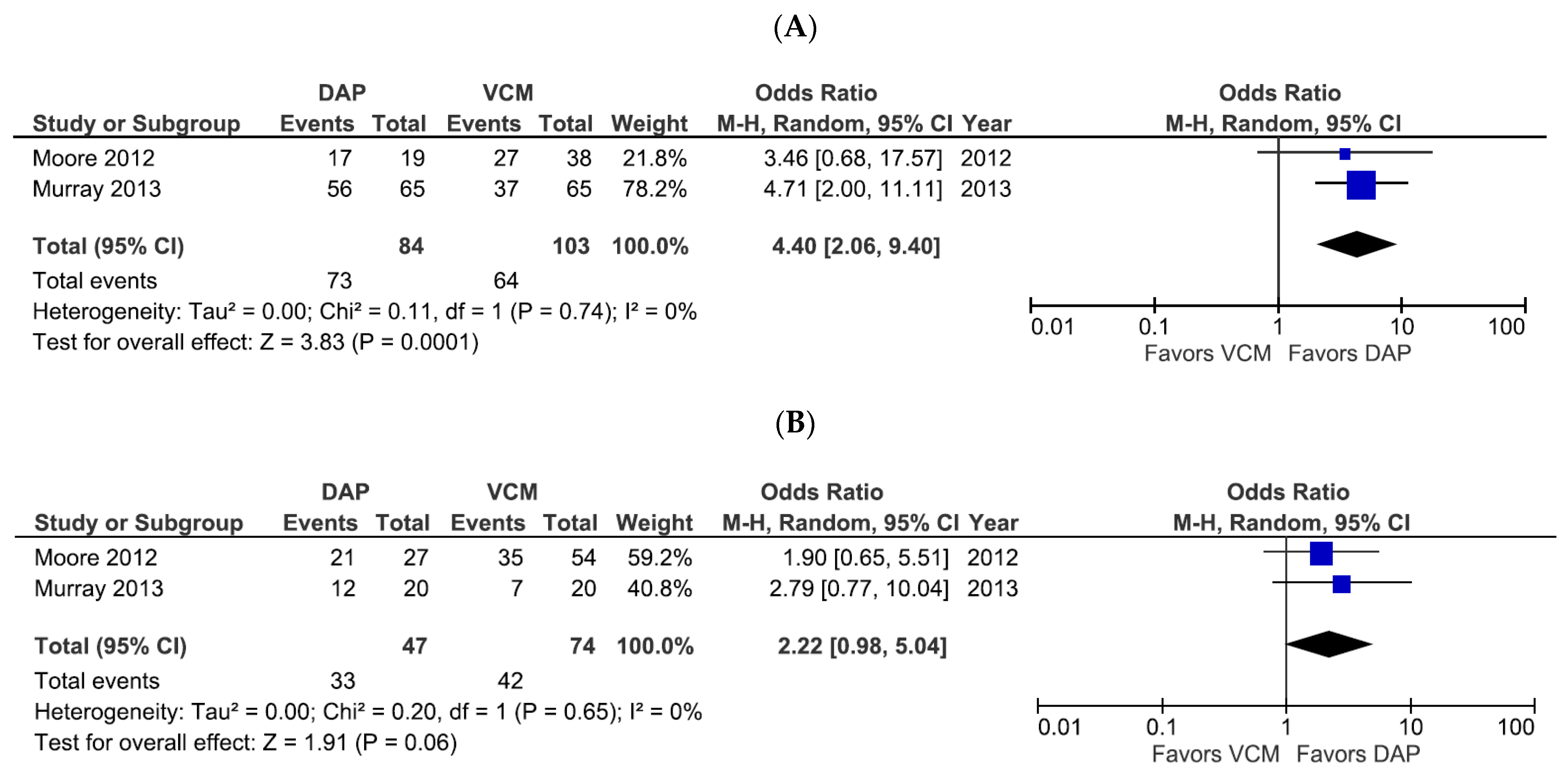
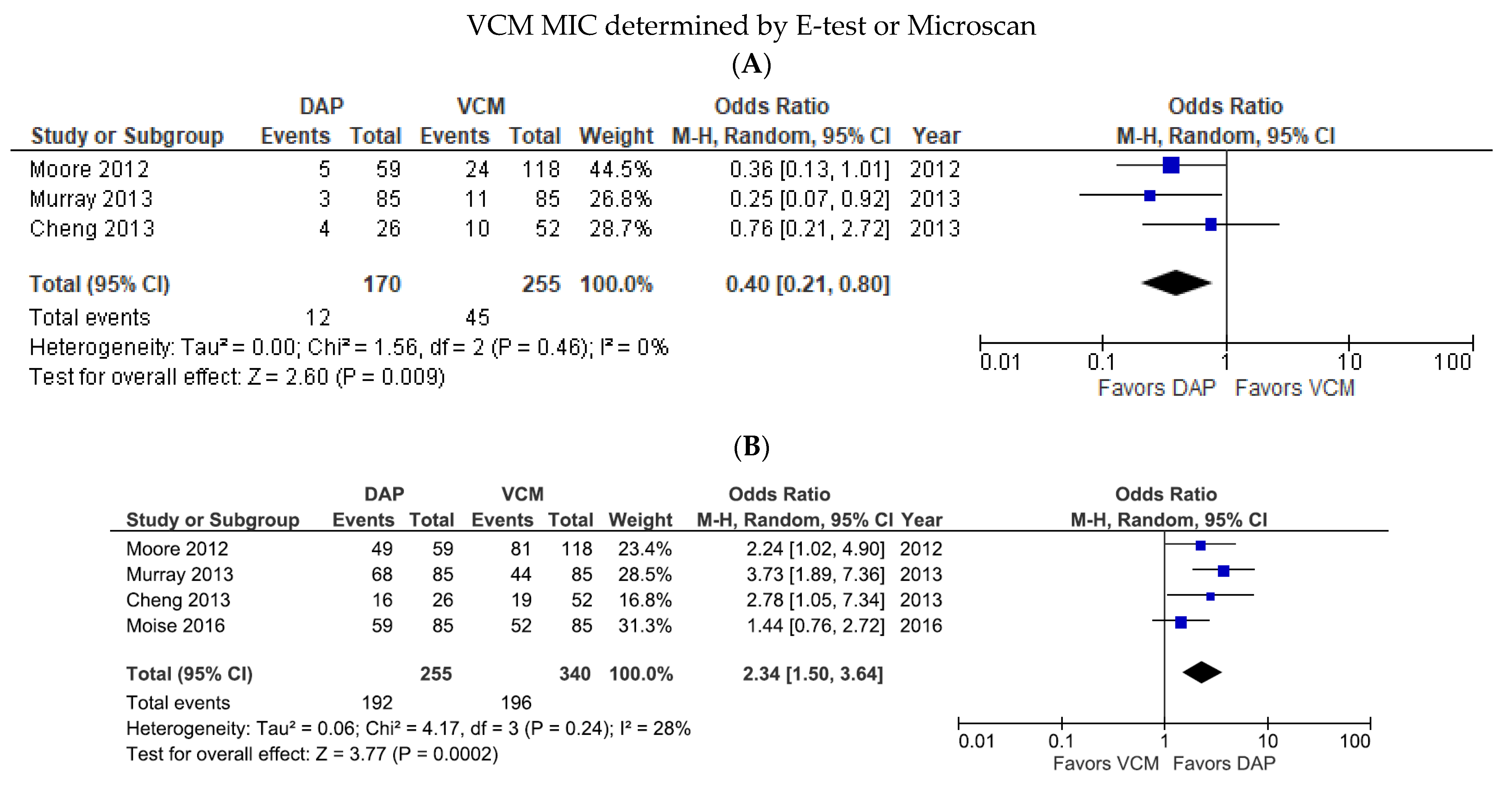
3.2. Analysis of the Mortality and Treatment Success of DAP versus VCM for Bacteremia Caused by MRSA with VCM MIC > 1 µg/mL
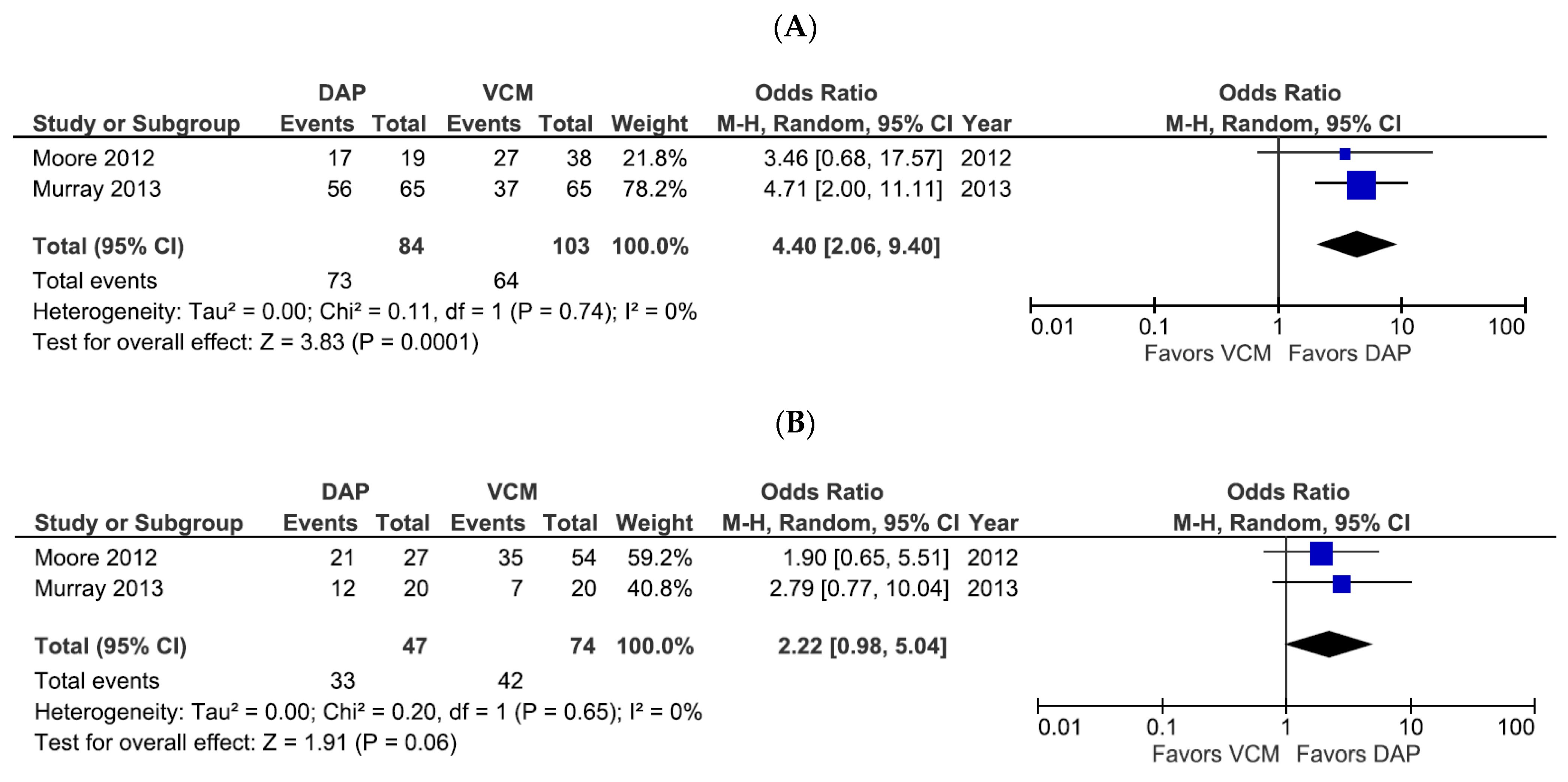
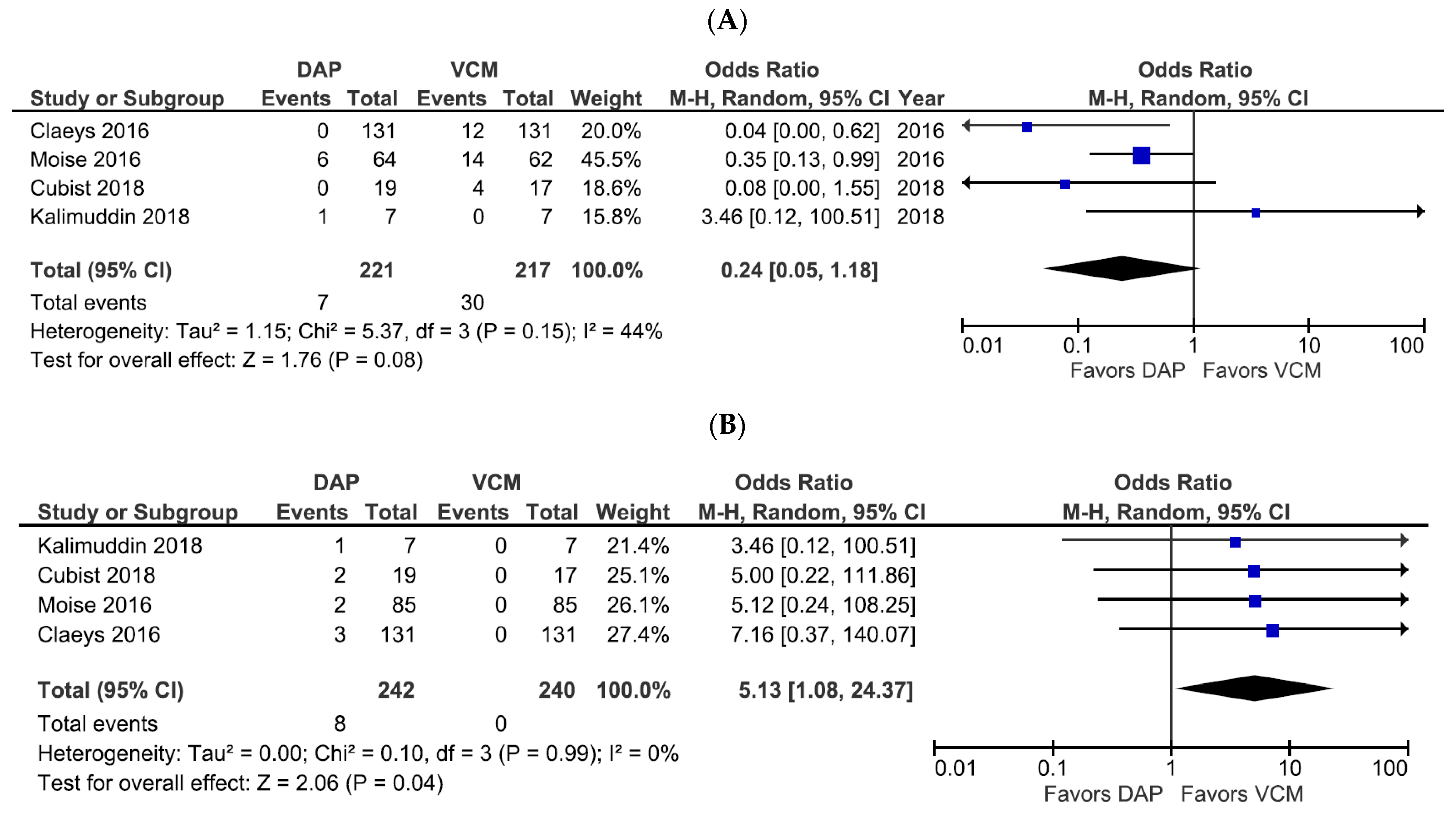
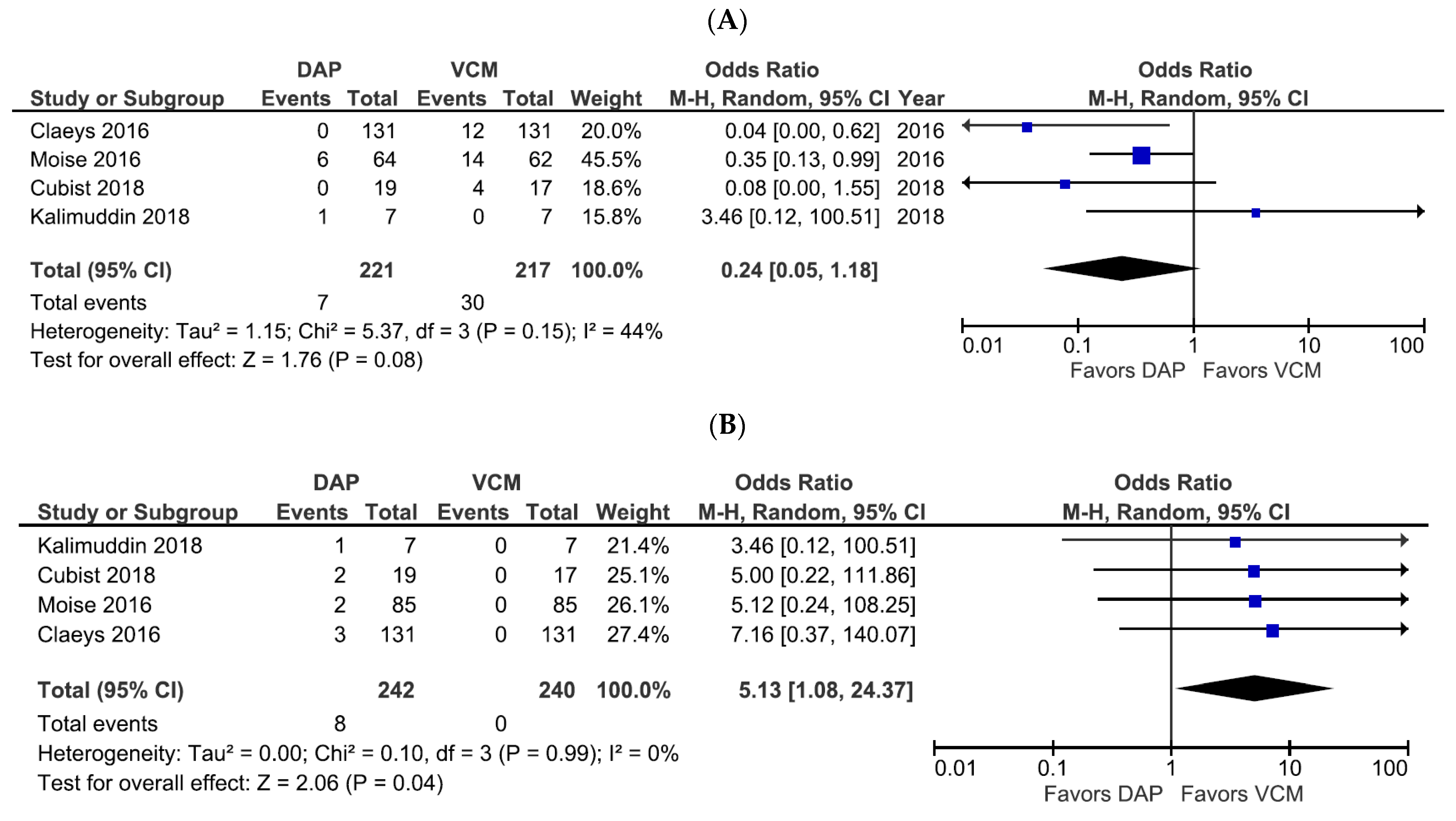
3.3. Safety Analysis of DAP versus VCM Treatment for Bacteremia Caused by MRSA with VCM MIC > 1 µg/mL
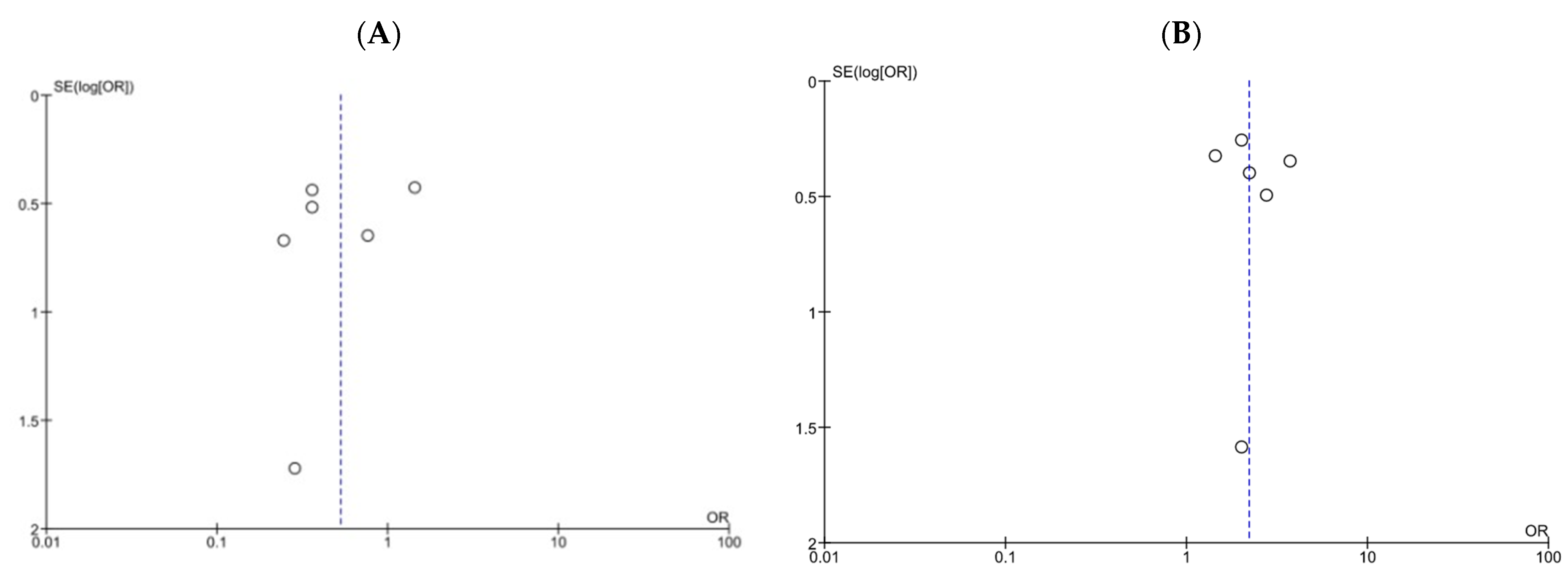
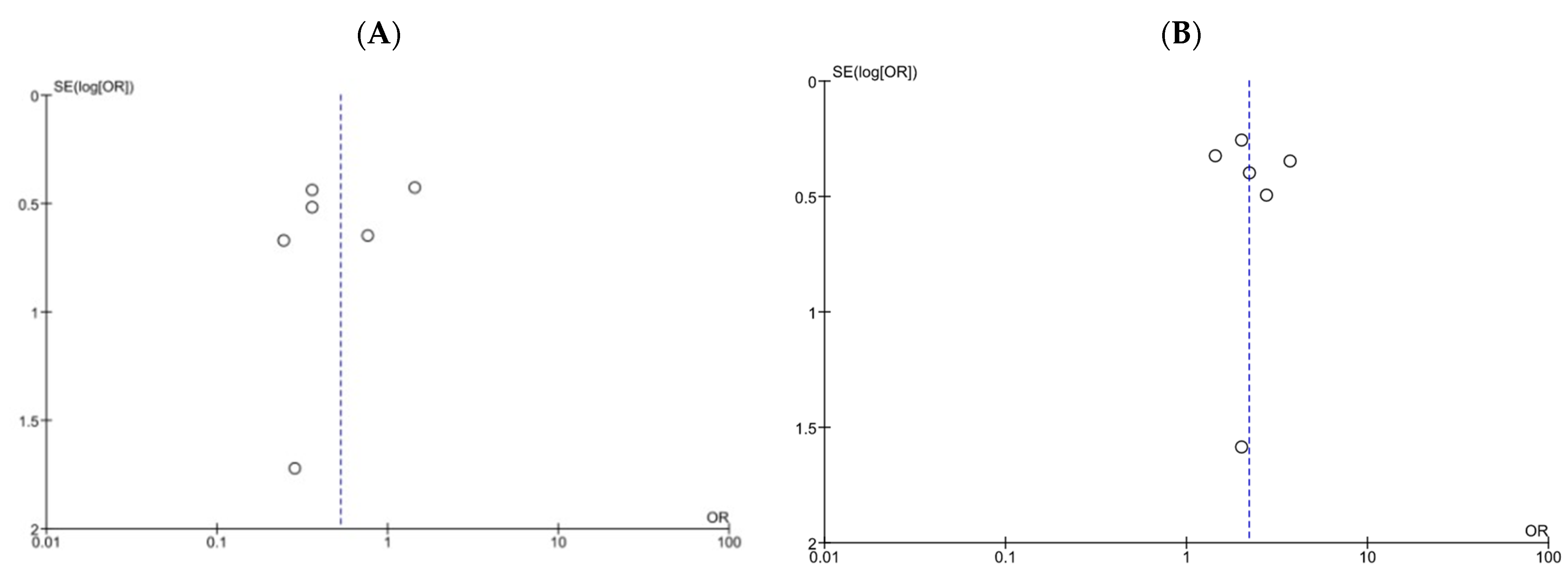
3.4. Assessment of Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nagao, M. A multicentre analysis of epidemiology of the nosocomial bloodstream infections in Japanese university hospitals. Clin. Microbiol. Infect. 2013, 19, 852–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hal, S.J.; Jensen, S.O.; Vaska, V.L.; Espedido, B.A.; Paterson, D.L.; Gosbell, I.B. Predictors of mortality in Staphylococcus aureus Bacteremia. Clin. Microbiol. Rev. 2012, 25, 362–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosgrove, S.E.; Sakoulas, G.; Perencevich, E.N.; Schwaber, M.J.; Karchmer, A.W.; Carmeli, Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: A meta-analysis. Clin. Infect. Dis. 2003, 36, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, M.; Trecarichi, E.M.; Mesini, A.; Spanu, T.; Giacobbe, D.R.; Rossi, M.; Shenone, E.; Pascale, G.D.; Molinari, M.P.; Cauda, R.; et al. Risk factors and mortality of healthcare-associated and community-acquired Staphylococcus aureus bacteraemia. Clin. Microbiol. Infect. 2012, 18, 862–869. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, T.; Takesue, Y.; Iwata, S.; Ueda, T.; Uchiyama, K.; Kobayashi, K.; Takahashi, S.; Tamura, Y.; Tomono, K.; Nakajima, K.; et al. Practical Guidelines for the Management and Treatment of Infections Caused by MRSA, 2019th ed.; Japanese Society of Chemotherapy/The Japanese Association for Infectious Diseases: Tokyo, Japan, 2019. [Google Scholar]
- Brown, N.M.; Brown, E.M. Treatment of methicillin-resistant Staphylococcus aureus (MRSA): Updated guidelines from the UK. J. Antimicrob. Chemother. 2021, 76, 1377–1378. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard, 7th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2006. [Google Scholar]
- van Hal, S.J.; Lodise, T.P.; Paterson, D.L. The clinical significance of vancomycin minimum inhibitory concentration in Staphylococcus aureus infections: A systematic review and meta-analysis. Clin. Infect. Dis. 2012, 54, 755–771. [Google Scholar] [CrossRef] [Green Version]
- Takesue, Y.; Nakajima, K.; Takahashi, Y.; Ichiki, K.; Ishihara, M.; Wada, Y.; Tsuchida, T.; Uchino, M.; Ikeuchi, H. Clinical characteristics of vancomycin minimum inhibitory concentration of 2 mug/ml methicillin-resistant Staphylococcus aureus strains isolated from patients with bacteremia. J. Infect. Chemother. 2011, 17, 52–57. [Google Scholar] [CrossRef]
- Ishaq, H.; Tariq, W.; Talha, K.M.; Palraj, B.R.V.; Sohail, M.R.; Baddour, L.M.; Mahmood, M. Association between high vancomycin minimum inhibitory concentration and clinical outcomes in patients with methicillin-resistant Staphylococcus aureus bacteremia: A meta-analysis. Infection 2021, 49, 803–811. [Google Scholar] [CrossRef]
- Ho, P.L.; Lo, P.Y.; Chow, K.H.; Lau, E.H.; Lai, E.L.; Cheng, V.C.; Kao, R.Y. Vancomycin MIC creep in MRSA isolates from 1997 to 2008 in a healthcare region in Hong Kong. J. Infect. 2010, 60, 140–145. [Google Scholar] [CrossRef]
- Diaz, R.; Afreixo, V.; Ramalheira, E.; Rodrigues, C.; Gago, B. Evaluation of vancomycin MIC creep in methicillin-resistant Staphylococcus aureus infections-a systematic review and meta-analysis. Clin. Microbiol. Infect. 2018, 24, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, D.I.; Hidayat, L.K.; Quist, R.; Hindler, J.; Karlsson, A.; Yusof, A.; Wong-Beringer, A. Comparison of method-specific vancomycin minimum inhibitory concentration values and their predictability for treatment outcome of meticillin-resistant Staphylococcus aureus (MRSA) infections. Int. J. Antimicrob. Agents 2008, 32, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.L.; Osaki-Kiyan, P.; Haque, N.Z.; Perri, M.B.; Donabedian, S.; Zervos, M.J. Daptomycin versus vancomycin for bloodstream infections due to methicillin-resistant Staphylococcus aureus with a high vancomycin minimum inhibitory concentration: A case-control study. Clin. Infect. Dis. 2012, 54, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.W.; Hsu, P.C.; Yang, C.C.; Chang, H.J.; Siu, L.K.; Wu, T.L.; Huang, C.T.; Lee, M.H. Influence of early daptomycin therapy on treatment outcome of meticillin-resistant Staphylococcus aureus bacteraemia with high vancomycin minimum inhibitory concentrations. Int. J. Antimicrob. Agents 2013, 41, 293–294. [Google Scholar] [CrossRef]
- Murray, K.P.; Zhao, J.J.; Davis, S.L.; Kullar, R.; Kaye, K.S.; Lephart, P.; Rybak, M.J. Early use of daptomycin versus vancomycin for methicillin-resistant Staphylococcus aureus bacteremia with vancomycin minimum inhibitory concentration >1 mg/L: A matched cohort study. Clin. Infect. Dis. 2013, 56, 1562–1569. [Google Scholar] [CrossRef] [Green Version]
- Weston, A.; Golan, Y.; Holcroft, C.; Snydman, D.R. The efficacy of daptomycin versus vancomycin for methicillin-resistant Staphylococcus aureus bloodstream infection in patients with impaired renal function. Clin. Infect. Dis. 2014, 58, 1533–1539. [Google Scholar] [CrossRef] [Green Version]
- Usery, J.B.; Vo, N.H.; Finch, C.K.; Cleveland, K.O.; Gelfand, M.S.; Self, T.H. Evaluation of the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Am. J. Med. Sci. 2015, 349, 36–41. [Google Scholar] [CrossRef]
- Claeys, K.C.; Zasowski, E.J.; Casapao, A.M.; Lagnf, A.M.; Nagel, J.L.; Nguyen, C.T.; Hallesy, J.A.; Compton, M.T.; Kaye, K.S.; Levine, D.P.; et al. Daptomycin Improves Outcomes Regardless of Vancomycin MIC in a Propensity-Matched Analysis of Methicillin-Resistant Staphylococcus aureus Bloodstream Infections. Antimicrob. Agents Chemother. 2016, 60, 5841–5848. [Google Scholar] [CrossRef] [Green Version]
- Moise, P.A.; Culshaw, D.L.; Wong-Beringer, A.; Bensman, J.; Lamp, K.C.; Smith, W.J.; Bauer, K.; Goff, D.A.; Adamson, R.; Leuthner, K.; et al. Comparative Effectiveness of Vancomycin Versus Daptomycin for MRSA Bacteremia With Vancomycin MIC >1 mg/L: A Multicenter Evaluation. Clin. Ther. 2016, 38, 16–30. [Google Scholar] [CrossRef]
- Maraolo, A.E.; Giaccone, A.; Gentile, I.; Saracino, A.; Bavaro, D.F. Daptomycin versus Vancomycin for the Treatment of Methicillin-Resistant Staphylococcus aureus Bloodstream Infection with or without Endocarditis: A Systematic Review and Meta-Analysis. Antibiotics 2021, 10, 1014. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Soriano, A.; Marco, F.; Martínez, J.A.; Pisos, E.; Almela, M.; Dimova, V.P.; Alamo, D.; Ortega, M.; Lopez, J.; Mensa, J. Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Clin. Infect. Dis. 2008, 46, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Lodise, T.P.; McKinnon, P.S.; Swiderski, L.; Rybak, M.J. Outcomes analysis of delayed antibiotic treatment for hospital-acquired Staphylococcus aureus bacteremia. Clin. Infect. Dis. 2003, 36, 1418–1423. [Google Scholar] [CrossRef] [Green Version]
- Rybak, M.J.; Vidaillac, C.; Sader, H.S.; Rhomberg, P.R.; Salimnia, H.; Briski, L.E.; Wanger, A.; Jones, R.N. Evaluation of vancomycin susceptibility testing for methicillin-resistant Staphylococcus aureus: Comparison of Etest and three automated testing methods. J. Clin. Microbiol. 2013, 51, 2077–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phase 2 Study of Safety, Efficacy, and Pharmacokinetics of Higher Doses of Daptomycin and Vancomycin in MRSA Bacteremia. Available online: https://clinicaltrials.gov/ct2/show/NCT00695903 (accessed on 19 December 2021).
- Kalimuddin, S.; Chan, Y.F.Z.; Phillips, R.; Ong, S.P.; Archuleta, S.; Lye, D.C.; Tan, T.T.; Low, J.G.H. A randomized phase 2B trial of vancomycin versus daptomycin for the treatment of methicillin-resistant Staphylococcus aureus bacteremia due to isolates with high vancomycin minimum inhibitory concentrations—results of a prematurely terminated study. Trials 2018, 19, 305. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Zhang, Y.; Chen, H.; Zhao, C.; Wang, H. Efficacy and safety of daptomycin for the treatment of infectious disease: A meta-analysis based on randomized controlled trials. J. Antimicrob. Chemother. 2014, 69, 3181–3189. [Google Scholar] [CrossRef] [Green Version]
- Holland, T.L.; Arnold, C.; Fowler, V.G., Jr. Clinical management of Staphylococcus aureus bacteremia: A review. JAMA 2014, 312, 1330–1341. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [Green Version]
- Bhavnani, S.M.; Ambrose, P.G.; Hammel, J.P.; Rubino, C.M.; Drusano, G.L. Evaluation of Daptomycin Exposure and Efficacy and Safety Endpoints To Support Risk-versus-Benefit Considerations. Antimicrob. Agents Chemother. 2015, 60, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Falcone, M.; Russo, A.; Venditti, M.; Novelli, A.; Pai, M.P. Considerations for higher doses of daptomycin in critically ill patients with methicillin-resistant Staphylococcus aureus bacteremia. Clin. Infect. Dis. 2013, 57, 1568–1576. [Google Scholar] [CrossRef] [Green Version]
- Urakami, T.; Hamada, Y.; Oka, Y.; Okinaka, T.; Yamakuchi, H.; Magarifuchi, H.; Aoki, Y. Clinical pharmacokinetic and pharmacodynamic analysis of daptomycin and the necessity of high-dose regimen in Japanese adult patients. J. Infect. Chemother. 2019, 25, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Samura, M.; Takada, K.; Yamamoto, R.; Ito, H.; Nagumo, F.; Uchida, M.; Kurata, T.; Koshioka, S.; Enoki, Y.; Taguchi, K.; et al. Population Pharmacokinetic Analysis and Dosing Optimization Based on Unbound Daptomycin Concentration and Cystatin C in Nonobese Elderly Patients with Hypoalbuminemia and Chronic Kidney Disease. Pharm. Res. 2021, 38, 1041–1055. [Google Scholar] [CrossRef]
- Falcone, M.; Russo, A.; Cassetta, M.I.; Lappa, A.; Tritapepe, L.; d’Ettorre, G.; Fallani, S.; Novelli, A.; Venditti, M. Variability of pharmacokinetic parameters in patients receiving different dosages of daptomycin: Is therapeutic drug monitoring necessary? J. Infect. Chemother. 2013, 19, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Fowler, V.G., Jr.; Boucher, H.W.; Corey, G.R.; Abrutyn, E.; Karchmer, A.W.; Rupp, M.E.; Levine, D.P.; Chambers, H.F.; Tally, F.P.; Vigliani, G.A.; et al. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N. Engl. J. Med. 2006, 355, 653–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G., Jr.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef] [PubMed]
- Tsutsuura, M.; Moriyama, H.; Kojima, N.; Mizukami, Y.; Tashiro, S.; Osa, S.; Enoki, Y.; Taguchi, K.; Oda, K.; Fujii, S.; et al. The monitoring of vancomycin: A systematic review and meta-analyses of area under the concentration-time curve-guided dosing and trough-guided dosing. BMC Infect. Dis. 2021, 21, 153. [Google Scholar] [CrossRef]
- Bhavnani, S.M.; Rubino, C.M.; Ambrose, P.G.; Drusano, G.L. Daptomycin exposure and the probability of elevations in the creatine phosphokinase level: Data from a randomized trial of patients with bacteremia and endocarditis. Clin. Infect. Dis. 2010, 50, 1568–1574. [Google Scholar] [CrossRef] [Green Version]
- Yamada, T.; Ooi, Y.; Oda, K.; Shibata, Y.; Kawanishi, F.; Suzuki, K.; Nishihara, M.; Nakano, T.; Yoshida, M.; Uchida, T.; et al. Observational study to determine the optimal dose of daptomycin based on pharmacokinetic/pharmacodynamic analysis. J. Infect. Chemother. 2020, 26, 379–384. [Google Scholar] [CrossRef]
- Dare, R.K.; Tewell, C.; Harris, B.; Wright, P.W.; Van Driest, S.L.; Farber-Eger, E.; Nelson, G.E.; Talbot, T.R. Effect of Statin Coadministration on the Risk of Daptomycin-Associated Myopathy. Clin. Infect. Dis. 2018, 67, 1356–1363. [Google Scholar] [CrossRef]
- Samura, M.; Hirose, N.; Kurata, T.; Takada, K.; Nagumo, F.; Koshioka, S.; Ishii, J.; Uchida, M.; Inoue, J.; Enoki, Y.; et al. Identification of risk factors for daptomycin-associated creatine phosphokinase elevation and development of a risk prediction model for incidence probability. Open Forum Infect. Dis. 2021, 8, ofab568. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am. J. Health Syst. Pharm. 2020, 77, 835–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, K.; Oda, K.; Shoji, K.; Hanai, Y.; Takahashi, Y.; Fujii, S.; Hamada, Y.; Kimura, T.; Mayumi, T.; Ueda, T.; et al. Clinical Practice Guidelines for Therapeutic Drug Monitoring of Vancomycin in the Framework of Model-Informed Precision Dosing: A Consensus Review by the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. Pharmaceutics 2022, 14, 489. [Google Scholar] [CrossRef]
- Casapao, A.M.; Lodise, T.P.; Davis, S.L.; Claeys, K.C.; Kullar, R.; Levine, D.P.; Rybak, M.J. Association between vancomycin day 1 exposure profile and outcomes among patients with methicillin-resistant Staphylococcus aureus infective endocarditis. Antimicrob. Agents Chemother. 2015, 59, 2978–2985. [Google Scholar] [CrossRef] [Green Version]
- Silverman, J.A.; Mortin, L.I.; Vanpraagh, A.D.; Li, T.; Alder, J. Inhibition of daptomycin by pulmonary surfactant: In vitro modeling and clinical impact. J. Infect. Dis. 2005, 191, 2149–2152. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Duration | Age (years) | Country | No. of Patients | Vancomycin MIC > 1 μg/mL | Dosage Regimen | Bacteremia Source | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DAP | VCM | Test Criteria | No. of Patients | DAP | VCM | DAP | VCM | ||||||
| DAP | VCM | ||||||||||||
| Moore 2012 [15] | Retrospective case-control | 2005–2009 | ≥18 | USA | 59 | 118 | E-test 1.5 μg/mL 2 μg/mL | 25 34 | 102 16 | 6 mg/kg q24h | Target Cmin 10–20 µg/mL | CRBSI 17%; IE 29%; SSTI 32%; IAI 3%; Genitourinary 5%; Graft/device: 10%; Other 3% | CRBSI:22%; IE: 29%; SSTI 28%; IAI 4%; Genitourinary 0%; Graft/device: 9%; Other 7% |
| Cheng 2013 [16] | Retrospective case-control | 2009–2010 | ≥18 | Taiwan | 26 | 52 | E-test ≥1.5 μg/mL | 26 | 52 | 8–10 mg/kg q24h | Loading 25–30 mg/kg; maintenance 15–20 mg/kg q12h | No data | No data |
| Murray 2013 [17] | Retrospective cohort | 2005–2012 | Adult | USA | 85 | 85 | 1st stage: E-test; 2nd stage Microscan >1 μg/mL | 85 | 85 | ≥6 mg/kg q24h | Target Cmin 15–20 µg/mL | IE 23.5%; B/J 34.1%; SSTI 32.9%; unknown 9.4% | IE: 23.5%; B/J 34.1%; SSTI 32.9%; unknown 9.4% |
| Claeys 2016 [20] | Retrospective cohort | 2010–2015 | ≥18 | USA | 131 | 131 | BMD >1 μg/mL | 131 | 131 | Median 8.2 mg/kg q24h (IQR, 6.4–10.0) | Cmin: median 17.7 mg/L (IQR, 13.2–22.0) | B/J 29.0%; SSTI 22.9%; deep abscess: 10.7%; IE: 19.1%; CRBSI 7.6%; others 10.7% | B/J 20.6%; SSTI 25.2%; deep abscess: 10.7%; IE 17.6%; CRBSI 11.5%; others 14.5% |
| Moise 2016 [21] | Retrospective cohort | No data | ≥18 | USA | 85 | 85 | E-test: 61%; Microscan: 27% Phoenix: 12% 1.5 μg/mL 2 μg/mL | 27 58 | 41 44 | Median 6 mg/kg q24h (IQR, 6–8) | Cmin: median 17.5 mg/L (IQR, 14.0–22.0) | IE 24%; infected aneurysm 2%; septic thrombophlebitis 1%; unknown 12%; B/J 32%; SSTI 21%; IAI/UTI 2%; CRBSI 6% | IE 13%; infected aneurysm 4%; septic thrombophlebitis 11%; unknown 12%; B/J 18%; SSTI 29%; IAI/UTI 8%; CRBSI: 6% |
| Cubist 2018 [27] | RCT | 2008–2010 | ≥18 | USA | 19 | 17 | No data >1 μg/mL | 19 (100) | 17 (100) | 10 mg/kg q24h | 15 mg/kg q12h; target trough 15–20 µg/mL | Bacteremia W/O IE | Bacteremia W/O IE |
| Kalimuddin 2018 [28] | RCT | 2014–2015 | ≥21 | Singapore | 7 | 7 | E-test or VITEK2 1.5 ≤ MIC < 2 | 7 (100) | 7 (100) | 6 or 8 mg/kg q24h | 15 mg/kg q12h; target Cmin 15–20 µg/mL | Bacteremia uncomplicated: 71.4% complicated (without IE) 28.6% | Bacteremia uncomplicated: 100% complicated (without IE) 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samura, M.; Kitahiro, Y.; Tashiro, S.; Moriyama, H.; Hamamura, Y.; Takahata, I.; Kawabe, R.; Enoki, Y.; Taguchi, K.; Takesue, Y.; et al. Efficacy and Safety of Daptomycin versus Vancomycin for Bacteremia Caused by Methicillin-Resistant Staphylococcus aureus with Vancomycin Minimum Inhibitory Concentration > 1 µg/mL: A Systematic Review and Meta-Analysis. Pharmaceutics 2022, 14, 714. https://doi.org/10.3390/pharmaceutics14040714
Samura M, Kitahiro Y, Tashiro S, Moriyama H, Hamamura Y, Takahata I, Kawabe R, Enoki Y, Taguchi K, Takesue Y, et al. Efficacy and Safety of Daptomycin versus Vancomycin for Bacteremia Caused by Methicillin-Resistant Staphylococcus aureus with Vancomycin Minimum Inhibitory Concentration > 1 µg/mL: A Systematic Review and Meta-Analysis. Pharmaceutics. 2022; 14(4):714. https://doi.org/10.3390/pharmaceutics14040714
Chicago/Turabian StyleSamura, Masaru, Yuki Kitahiro, Sho Tashiro, Hiromu Moriyama, Yuna Hamamura, Isamu Takahata, Rina Kawabe, Yuki Enoki, Kazuaki Taguchi, Yoshio Takesue, and et al. 2022. "Efficacy and Safety of Daptomycin versus Vancomycin for Bacteremia Caused by Methicillin-Resistant Staphylococcus aureus with Vancomycin Minimum Inhibitory Concentration > 1 µg/mL: A Systematic Review and Meta-Analysis" Pharmaceutics 14, no. 4: 714. https://doi.org/10.3390/pharmaceutics14040714
APA StyleSamura, M., Kitahiro, Y., Tashiro, S., Moriyama, H., Hamamura, Y., Takahata, I., Kawabe, R., Enoki, Y., Taguchi, K., Takesue, Y., & Matsumoto, K. (2022). Efficacy and Safety of Daptomycin versus Vancomycin for Bacteremia Caused by Methicillin-Resistant Staphylococcus aureus with Vancomycin Minimum Inhibitory Concentration > 1 µg/mL: A Systematic Review and Meta-Analysis. Pharmaceutics, 14(4), 714. https://doi.org/10.3390/pharmaceutics14040714