
Adverse Effects of Oral Cannabidiol: An Updated Systematic Review of Randomized Controlled Trials (2020–2022)

 , and
, and 
Abstract
1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
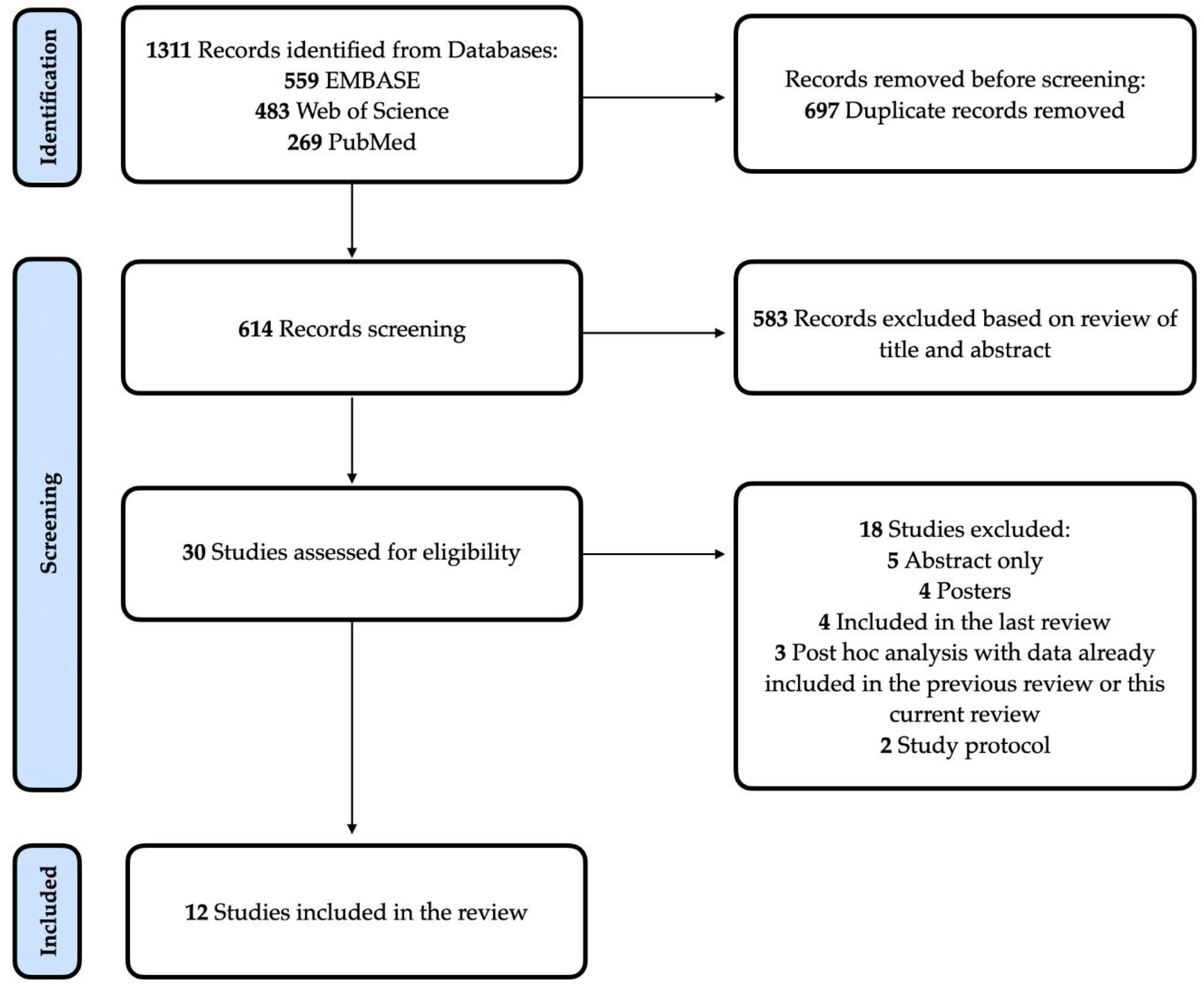
2.2. Search Strategy and Study Eligibility
2.3. Data Extraction and Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Safety Assessment
3.3. Adverse Effects of CBD
3.4. Serious Adverse Effects of CBD
3.5. Evaluation of the Studies’ Methodology and Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brunetti, P.; Pichini, S.; Pacifici, R.; Busardò, F.P.; Del Rio, A. Herbal Preparations of Medical Cannabis: A Vademecum for Prescribing Doctors. Medicina 2020, 56, 237. [Google Scholar] [CrossRef] [PubMed]
- Schlag, A.K.; O’Sullivan, S.E.; Zafar, R.R.; Nutt, D.J. Current controversies in medical cannabis: Recent developments in human clinical applications and potential therapeutics. Neuropharmacology 2021, 191, 108586. [Google Scholar] [CrossRef] [PubMed]
- Crippa, J.A.; Guimarães, F.S.; Campos, A.C.; Zuardi, A.W. Translational Investigation of the Therapeutic Potential of Cannabidiol (CBD): Toward a New Age. Front. Immunol. 2018, 9, 2009. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Naveed, S.; Mian, N.; Fida, A.; Raafey, M.A.; Aedma, K.K. The therapeutic role of Cannabidiol in mental health: A systematic review. J. Cannabis Res. 2020, 2, 2. [Google Scholar] [CrossRef]
- Wieckiewicz, G.; Stokłosa, I.; Stokłosa, M.; Gorczyca, P.; Pudlo, R. Cannabidiol (CBD) in the Self-Treatment of Depression-Exploratory Study and a New Phenomenon of Concern for Psychiatrists. Front. Psychiatry 2022, 13, 837946. [Google Scholar] [CrossRef] [PubMed]
- EPIDIOLEX. EPIDIOLEX® (Cannabidiol). Available online: https://www.epidiolex.com/ (accessed on 13 September 2022).
- Chesney, E.; Oliver, D.; Green, A.; Sovi, S.; Wilson, J.; Englund, A.; Freeman, T.; McGuire, P. Adverse effects of cannabidiol: A systematic review and meta-analysis of randomized clinical trials. Neuropsychopharmacology 2020, 45, 1799–1806. [Google Scholar] [CrossRef]
- Dos Santos, R.G.; Guimarães, F.S.; Crippa, J.A.S.; Hallak, J.E.; Rossi, G.N.; Rocha, J.M.; Zuardi, A.W. Serious adverse effects of cannabidiol (CBD): A review of randomized controlled trials. Expert. Opin. Drug Metab. Toxicol. 2020, 16, 517–526. [Google Scholar] [CrossRef]
- NHLBI; NIH. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 13 September 2022).
- Appiah-Kusi, E.; Petros, N.; Wilson, R.; Colizzi, M.; Bossong, M.G.; Valmaggia, L.; Mondelli, V.; McGuire, P.; Bhattacharyya, S. Effects of short-term cannabidiol treatment on response to social stress in subjects at clinical high risk of developing psychosis. Psychopharmacology 2020, 237, 1121–1130. [Google Scholar] [CrossRef]
- Ben-Menachem, E.; Gunning, B.; Cabrera, C.M.A.; VanLandingham, K.; Crockett, J.; Critchley, D.; Wray, L.; Tayo, B.; Morrison, G.; Toledo, M. A Phase II Randomized Trial to Explore the Potential for Pharmacokinetic Drug-Drug Interactions with Stiripentol or Valproate when Combined with Cannabidiol in Patients with Epilepsy. CNS Drugs 2020, 34, 661–672. [Google Scholar] [CrossRef]
- Efron, D.; Freeman, J.L.; Cranswick, N.; Payne, J.; Mulraney, M.; Prakash, C.; Lee, K.J.; Taylor, K.; Williams, K. A pilot randomised placebo-controlled trial of cannabidiol to reduce severe behavioural problems in children and adolescents with intellectual disability. Br. J. Clin. Pharmacol. 2021, 87, 436–446. [Google Scholar] [CrossRef]
- Freeman, T.P.; Hindocha, C.; Baio, G.; Shaban, N.D.C.; Thomas, E.M.; Astbury, D.; Freeman, A.M.; Lees, R.; Craft, S.; Morrison, P.D.; et al. Cannabidiol for the treatment of cannabis use disorder: A phase 2a, double-blind, placebo-controlled, randomised, adaptive Bayesian trial. Lancet Psychiatry 2020, 7, 865–874. [Google Scholar] [CrossRef]
- De Meneses-Gaya, C.; Crippa, J.A.; Hallak, J.E.; Miguel, A.Q.; Laranjeira, R.; Bressan, R.A.; Zuardi, A.W.; Lacerda, A.L. Cannabidiol for the treatment of crack-cocaine craving: An exploratory double-blind study. Braz. J. Psychiatry 2021, 43, 467–476. [Google Scholar] [CrossRef]
- Thiele, E.A.; Bebin, E.M.; Bhathal, H.; Jansen, F.E.; Kotulska, K.; Lawson, J.A.; O’Callaghan, F.J.; Wong, M.; Sahebkar, F.; Checketts, D.; et al. Add-on Cannabidiol Treatment for Drug-Resistant Seizures in Tuberous Sclerosis Complex: A Placebo-Controlled Randomized Clinical Trial. JAMA Neurol. 2021, 78, 285–292. [Google Scholar] [CrossRef]
- VanLandingham, K.E.; Crockett, J.; Taylor, L.; Morrison, G. A Phase 2, Double-Blind, Placebo-Controlled Trial to Investigate Potential Drug-Drug Interactions Between Cannabidiol and Clobazam. J. Clin. Pharmacol. 2020, 60, 1304–1313. [Google Scholar] [CrossRef]
- Crippa, J.A.S.; Pacheco, J.C.; Zuardi, A.W.; Guimarães, F.S.; Campos, A.C.; Osório, F.D.L.; Loureiro, S.R.; dos Santos, R.G.; Souza, J.D.S.; Ushirohira, J.M.; et al. Cannabidiol for COVID-19 Patients with Mild to Moderate Symptoms (CANDIDATE Study): A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Cannabis Cannabinoid Res. 2021, 7, 658–669. [Google Scholar] [CrossRef]
- De Almeida, C.M.; Brito, M.M.; Bosaipo, N.B.; Pimentel, A.V.; Tumas, V.; Zuardi, A.W.; Crippa, J.A.; Hallak, J.E.; Eckeli, A.L. Cannabidiol for Rapid Eye Movement Sleep Behavior Disorder. Mov. Disord. 2021, 36, 1711–1715. [Google Scholar] [CrossRef]
- Leweke, F.M.; Rohleder, C.; Gerth, C.W.; Hellmich, M.; Pukrop, R.; Koethe, D. Cannabidiol and Amisulpride Improve Cognition in Acute Schizophrenia in an Explorative, Double-Blind, Active-Controlled, Randomized Clinical Trial. Front. Pharmacol. 2021, 12, 614811. [Google Scholar] [CrossRef]
- Mongeau-Pérusse, V.; Brissette, S.; Bruneau, J.; Conrod, P.; Dubreucq, S.; Gazil, G.; Stip, E.; Jutras-Aswad, D. Cannabidiol as a treatment for craving and relapse in individuals with cocaine use disorder: A randomized placebo-controlled trial. Addiction 2021, 116, 2431–2442. [Google Scholar] [CrossRef]
- Atieh, J.; Maselli, D.; Breen-Lyles, M.; Torres, M.; Katzka, D.; Ryks, M.; Busciglio, I.; Burton, D.; Carlson, P.; Harmsen, W.S.; et al. Cannabidiol for Functional Dyspepsia with Normal Gastric Emptying: A Randomized Controlled Trial. Am. J. Gastroenterol. 2022, 117, 1296–1304. [Google Scholar] [CrossRef]
- Pertwee, R.G. Cannabinoids and the gastrointestinal tract. Gut 2001, 48, 859–867. [Google Scholar] [CrossRef]
- Graham, M.; Martin, J.; Lucas, C.; Murnion, B.; Schneider, J. Cannabidiol drug interaction considerations for prescribers and pharmacists. Expert Rev. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.; Yamaori, S.; Takeda, S.; Yamamoto, I.; Watanabe, K. Identification of cytochrome P450 enzymes responsible for metabolism of cannabidiol by human liver microsomes. Life Sci. 2011, 89, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Zendulka, O.; Dovrtělová, G.; Nosková, K.; Turjap, M.; Šulcová, A.; Hanuš, L.; Jurica, J. Cannabinoids and Cytochrome P450 Interactions. Curr. Drug Metab. 2016, 17, 206–226. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/210365lbl.pdf (accessed on 14 September 2022).
- Crippa, J.A.S.; Zuardi, A.W.; Guimarães, F.S.; Campos, A.C.; de Lima Osório, F.; Loureiro, S.R.; Dos Santos, R.G.; Souza, J.D.S.; Ushirohira, J.M.; Pacheco, J.C.; et al. Efficacy and Safety of Cannabidiol Plus Standard Care vs Standard Care Alone for the Treatment of Emotional Exhaustion and Burnout Among Frontline Health Care Workers During the COVID-19 Pandemic: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2120603. [Google Scholar] [CrossRef]
- Morrison, G.; Crockett, J.; Blakey, G.; Sommerville, K. A Phase 1, Open-Label, Pharmacokinetic Trial to Investigate Possible Drug-Drug Interactions Between Clobazam, Stiripentol, or Valproate and Cannabidiol in Healthy Subjects. Clin. Pharmacol. Drug Dev. 2019, 8, 1009–1031. [Google Scholar] [CrossRef]
- Souza, J.D.S.; Fassoni-Ribeiro, M.; Batista, R.M.; Ushirohira, J.M.; Zuardi, A.W.; Guimarães, F.S.; Campos, A.C.; Osório, F.D.L.; Elias, D.; Souza, C.S.; et al. Case Report: Cannabidiol-Induced Skin Rash: A Case Series and Key Recommendations. Front. Pharmacol. 2022, 13, 881617. [Google Scholar] [CrossRef]
- Souza, J.D.S.; Zuardi, A.W.; Guimarães, F.S.; Osório, F.D.L.; Loureiro, S.R.; Campos, A.C.; Hallak, J.E.C.; Dos Santos, R.G.; Silveira, I.L.M.; Pereira-Lima, K.; et al. Maintained anxiolytic effects of cannabidiol after treatment discontinuation in healthcare workers during the COVID-19 pandemic. Front. Pharmacol. 2022, 13, 856846. [Google Scholar] [CrossRef]
- Health Canada. Review of Cannabidiol: Report of the Science Advisory Committee on Health Products Containing Cannabis. 2022. Available online: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/health-products-containing-cannabis/review-cannabidiol-health-products-containing-cannabis.html (accessed on 14 September 2022).
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck, D.; Bohn, T.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.I.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Naska, A.; et al. Statement on safety of cannabidiol as a novel food: Data gaps and uncertainties. EFSA J. 2022, 20, e07322. [Google Scholar]


{kind=link}
| Reference | Study Design/Sample | Treatment | Investigational Product Formulation | Concomitant Therapy | Safety Assessment | Adverse Effects | Serious Adverse Effects |
| Appiah-Kusi et al., 2020 [10] | RCT, phase I, double-blind, between-groups, placebo-controlled. 33 clinical high-risk psychosis volunteers (Age 23–29 y) 16 CBD; 17 placebo 25 healthy volunteers (no use of intervention drug) (Age 23–29 y) | 600 mg/day oral CBD for 1 week. | CBD capsules (STI Pharmaceuticals, UK). | None | No adverse event scale or questionnaire was applied | None | None |
| Ben-Menachem et al., 2020 [11] | RCT, phase II, two-arm, parallel-group, double-blind, placebo-controlled. 34 patients with epilepsy receiving Stiripentol (STP) or Valproate (VPA) and no more than 2 other AEDs (16–55 y). STP arm (n = 14): 12 CBD 2 placebo VPA arm (n = 20): 16 CBD 4 placebo | CBD 20 mg/kg/d administered as two equal doses twice a day for 2 weeks. | Epidiolex® 100 mg/mL (GW Pharma, Cambridge, UK). | Carbamazepine Clobazam Clonazepam Ethosuximide Lacosamide Lamotrigine Levetiracetam Lorazepam Oxcarbazepine Rufinamide Stiripentol Topiramate VPA sodium Zonisamide | Laboratory parameters (liver enzymes) Drug abuse liability (monitored if CBD was overused or went missing) | STP arm: 8 CBD patients experienced mild AE (mostly diarrhea and fatigue). 2 CBD patients experienced ALT and AST increases (solved during the trial) VPA arm: 14 CBD patients experienced mil AE (mostly diarrhea) No AE in the placebo group. | STP arm: 1 generalized rash led to discontinuation. Rash solved after both CBD and STP discontinued. VPA arm: 1 hypertransaminasemia led to discontinuation. SAE solved by day 40. |
| Efron et al., 2020 [12] | RCT, phase I/II double-blind, parallel-group, placebo-controlled. 8 participants diagnosed with Intellectual Disability (8–16 y). 3 CBD 5 placebo | CBD was up titrated over 9 days from 5 mg/kg/day to 20 mg/kg/d in two divided doses, with a maximum dose of 500 mg twice/d for 8 weeks. | 100 mg/mL CBD oral solution. 98% CBD in grapeseed oil (Tilray, Nanaimo, BC, Canada). | Clonidine Fluoxetine Guanfacine Melatonin Methylphenidate Risperidone Sodium Valproate | Safety: Blood collection (liver enzymes) Monitoring of Side Effects Scale (MOSES). | CBD: Eyes rolled up (1), tics (1), ear ringing (1), drooling (1), abdominal pain (1), decreased appetite (1), increased appetite (1), constipation (1), decreased wight (1), increased weight (1), restlessness (1), jitter (1), acne (1), urination incontinence (1), sadness (1), drowsiness (1), excessive sleep (1), insomnia (1). Placebo: Headache (1), nose congestion (1), increased appetite (1), increased weight (3), sadness (1), insomnia (1). | None |
| Freeman et al., 2020 [13] | RCT, phase II, double-blind, placebo-controlled, parallel-group. 48 patients in 1st stage plus 34 patients in 2nd stage with DSM-V criteria for a cannabis use disorder (at least moderate severity), expressing a desire to stop using cannabis (16–60 y). 77 participants completed treatment. 1st stage: 23 Placebo 12 CBD 200 mg 12 CBD 400 mg 12 CBD 800 mg 2nd stage: 23 Placebo 24 CBD 400 mg 23 CBD 800 mg | Gelatine capsules containing microcrystalline cellulose filler and CBD (50 mg, 100 mg, or 200 mg) for 4 weeks. 2 capsules twice daily: CBD 200 mg 4 capsules 50 mg CBD 400 mg 4 capsules 100 mg CBD 800 mg 4 capsules 200 mg | Synthetic CBD 99.9% purity (STI Pharmaceuticals, UK; manufactured by Nova Laboratories, UK). | None | Participants were asked about possible adverse events at each assessment from week 1 to week 16. All adverse events were verified with a medical supervisor and an independent trial monitor throughout the trial on an ongoing basis. | CBD 200 mg (12): 42 mild and 4 moderate AE CBD 400 mg (24): 96 mild and 8 moderate CBD 800 mg (23): 78 mild and 8 moderate Placebo (23): 65 mild and 9 moderate | None |
| Meneses-Gaya et al., 2020 [14] | RCT, double-blind, placebo-controlled. 31 patients with DSM-IV diagnosis of crack-cocaine dependence (>18 y). 14 CBD 17 placebo | CBD 300 mg/d. Two 150 mg capsules/d for 10 days. | CBD 99.9% pure powder (THC-Pharm, Germany/ STI-Pharm, Brentwood, UK) dissolved in corn oil. | Benzodiazepines | UKU Side Effects Rating Scale (UKU-SERS) | Sleepiness: 5 CBD; 3 placebo Nausea: 2 CBD; 1 placebo Headache: 2 CBD; 1 placebo | None |
| Thiele et al., 2020 [15] | RCT of add-on CBD vs. placebo, Phase III, double-blind, parallel-group. 224 included patients with a clinical diagnosis of Tuberous Sclerosis Complex (1–65 y). 75 CBD25 73 CBD50 76 placebo | CBD 25 mg/kg/day (CBD25) or 50 mg/kg/d (CBD50) for 16 weeks. 4 w for dose escalation (titration period) followed by 12 w of stable dosing (maintenance period). | Epidiolex® 100 mg/mL (GW Pharma, UK). | Clobazam Valproic Acid | Safety was assessed primarily by evaluating adverse events and clinical laboratory parameters. | Most common: Diarrhea: 23 CBD25; 41 CBD50; 19 placebo. Somnolence: 10 CBD25; 19 CBD50; 7 placebo. Decreased appetite: 15 CBD25; 17 CBD50; 9 placebo. Liver transaminase level elevations: 17 CBD25; 30 CBD50 | Serum aminotransferase level elevations greater than 3 times the upper limit of the normal range: 9 CBD25 19 CBD50 Rash 2 CBD25 2 CBD50 Seizure 3 CBD25 2 CBD50 |
| VanLandingham et al., 2020 [16] | RCT, phase II, double-blind, placebo-controlled. 20 patients with epilepsy taking Clobazam and no more than 2 other antiepileptic drugs (18–65 y). Seven patients (1 taking placebo and 6 taking CBD) were excluded from the PK analysis | CBD 20 mg/kg/d coadministered with Clobazam. Patients titrated their CBD dose for 10 days (days 2 to 11) to 20 mg/kg/d CBD (twice daily). The titration period was followed by a 21d maintenance dose period (days 12 to 32). | Epidiolex® 100 mg/mL (GW Pharma, UK). | Carbamazepine Clobazam Eslicarbazepine Lacosamide Lamotrigine Levetiracetam Oxcarbazepine Perampanel Phenobarbital Valproic acid | Medical Dictionary for Regulatory Activities (MedDRA) | Diarrhea: 6 CBD 6; placebo 1 Nausea: 3 CBD Vomiting: 3 CBD Dizziness: 2 CBD Sedation: 2 CBD Somnolence: 2 CBD Skin tissue disorders: 6 CBD | Seizure cluster: 1 CBD |
| Crippa et al., 2021 [17] | RCT, phase, II double-blind, parallel-group, placebo-controlled. 105 patients diagnosed with COVID-19 (18–65 y). The data of 91 patients were included in the final analysis: 49 CBD 42 placebo | CBD 300 mg/d administered as two equal doses twice for 2 weeks. | Oral CBD 150 mg/mL 99.6% purity (PurMed Global, USA). | Dipyrone Paracetamol | Modified UKU Side Effects Scale | Somnolence:38 CBD; 33 placebo Fatigue:38 CBD; 33 placebo Decreased appetite:38 CBD; 32 placebo Lethargy:25 CBD; 15 placebo Weight loss:24 CBD; 22 placebo Nausea:23 CBD; 16 placebo Diarrhea:21 CBD; 20 placebo Increased appetite:17 CBD; 10 placebo Fever:11 CBD; 15 placebo Weight gain:10 CBD; 8 placebo | None |
| De Almeida et al., 2021 [18] | RCT, phase II/III, double-blind, placebo-controlled, parallel-group. 33 patients with Parkinson’s Disease (>18y). 17 CBD 16 placebo | 1st week 1 capsule (CBD 75mg) 2nd week 1 capsule (CBD 150 mg) the 3rd until the 12th w 2 capsules (CBD 150 mg) | CBD 99.6% pure powder form (BSPG Pharm, UK) dissolved in corn oil (capsule). | Antidepressants (SSRI or dual) Clonazepam Melatonin | Participants self-report | CBD: Epigastric pain (1), Nausea (1), headache (1), drowsiness (1), sadness (2), and dizziness (1). Placebo: Headache (1). | None |
| Leweke et al., 2021 [19] | RTC, phase II, parallel-group, active-controlled, mono-therapeutic, double-blind. 42 patients diagnosed with schizophrenia or schizophreniform psychosis (18–50 y). The data of 39 patients were included in the final analysis: 20 CBD 19 Amisulpride | Both CBD and AMI: Initial dose 200 mg/d and increased stepwise by 200 mg per day to a daily dose of 200 mg four times daily (800 mg/d) with the 1st w. Maintained for another 3 weeks (4w total). | Pharmaceutical grade not stated. | Lorazepam | No adverse event scale or questionnaire was applied | Although side effects have been reported (3 CBD; 5 AMI), they have not been described. | None |
| Mongeau-Pérusse et al., 2021 [20] | RCT: Phase II, double-blind, parallel-group, placebo-controlled. 78 diagnosed with current cocaine use disorder patients (18–65 y). Phase I: Detoxification (10 days); Phase II: 12-w outpatient follow-up. Completed Phase I: 35 CBD; 27 placebo Completed Phase II: 27 CBD; 23 placebo | CBD 300 mg/mL for 92 days. Days 2 and 3: CBD 400 mg (1.3 mL) and then increased the dose to 800 mg/day (2.7 mL) for the rest of the study. | Synthetic CBD 300 mg/mL (Insys Therapeutics, Phoenix, AZ, USA). | None | Systematic Assessment for Treatment Emergent Events (SAFTEE) tool | Diarrhea: 26 CBD; 1 placebo Nausea: 3 CBD; 3 placebo Abdominal pain: 3 CBD Hypoaesthesia: 2 CBD; 1 placebo Abdominal distension: 2 placebo Insomnia: 2 CBD | Placebo group: 1 Hepatitis |
| Atieh et al., 2022 [21] | RCT, double-blinded, placebo-controlled (1:1 ratio). 48 patients with Functional dyspepsia with normal gastric emptying (18–70 y) 25 CBD 23 placebo | CBD 20 mg/kg/d administered as two equal doses twice a day for 4 weeks. | Epidiolex® 100 mg/mL (GW Pharma, UK). | Analgesic; antibiotic; anticonvulsant; antiemetic; anti-fungal; alpha-2 adrenergic; anxiolytic; antipsychotic; antispasmodic; anti-histaminic; anti-acid secretory agent; anti-migraine; anti-hypertensive; birth control hormones; birth control IUD; bronchodilator; dopaminergic/noradrenergic; epinephrine pen available; hormones; lipid reducing agent; night sedative; NSAIDs; SSRI; topical/nasal steroids; tricyclic antidepressant. | Laboratory parameters (liver enzymes) | Elevated liver enzymes: 4 CBD; 1 placebo Abdominal distension: 6 CBD; 2 placebo Nausea: 5 CBD; 1 placebo Headache: 3 CBD; 1 placebo Diarrhea: 7 CBD; 1 placebo Dizziness: 2 CBD Fatigue: 2 CBD; 3 placebo Loss of appetite: 2 CBD | None |
| Number of Subjects Showing Adverse Effects and Frequency (%) | |||
|---|---|---|---|
| Adverse Effects | CBD | Control | Fisher’s Exact Test |
| Gastrointestinal symptoms | 270 (59.5) | 89 (30.6) | <0.0001 |
| Diarrhea | 145 (31.9) | 42 (14.4) | <0.0001 |
| Nausea | 46 (10.1) | 22 (7.6) | NS |
| Vomiting | 35 (7.7) | 11 (3.8) | 0.029 |
| Abdominal Pain | 20 (4.4) | 4 (1.4) | 0.031 |
| Constipation | 14 (3.1) | 6 (2.1) | NS |
| Abdominal Distention | 10 (2.2) | 4 (1.4) | NS |
| Somnolence | 76 (16.7) | 43 (14.8) | NS |
| Loss Appetite | 75 (16.5) | 32 (11.0) | 0.041 |
| ALT/AST Increase | 58 (12.8) | 1 (0.3) | <0.0001 |
| Fatigue | 52 (11.4) | 40 (13.8) | NS |
| Increased Appetite | 44 (9.7) | 11 (3.8) | 0.002 |
| Headache | 33 (7.8) | 17 (5.8) | NS |
| Rash | 29 (6.4) | 2 (0.7) | <0.0001 |
| Lethargy | 26 (5.7) | 15 (5.1) | NS |
| Weight Loss | 25 (5.5) | 22 (7.5) | NS |
| Nasopharyngitis | 24 (5.3) | 12 (4.1) | NS |
| Insomnia | 15 (3.3) | 5 (1.7) | NS |
| Upper respiratory tract infection | 14 (3.1) | 10 (3.4) | NS |
| Weight Gain | 11 (2.4) | 11 (3.8) | NS |
| Fever | 11 (2.4) | 21 (7.2) | 0.002 |
| Seizure | 9 (2.0) | 5 (1.7) | NS |
| Dizziness | 6 (1.3) | 0 | NS |
| Number of Subjects Showing Serious Adverse Effects and Frequency (%) | |||
|---|---|---|---|
| Serious Adverse Effects | CBD | Control | Fisher’s Exact Test |
| ALT/AST Increase | 29 (6.4) | 0 | <0.0001 |
| Seizure | 6 (1.3) | 1 | NS |
| Rash | 5 (1.1) | 0 | NS |
| References | Items Where Information Was Present | Information Not Present or Not Reported | Total Applicable Items | Percentage of Reported Items | Quality Rating |
|---|---|---|---|---|---|
| Appiah-Kusi et al., 2020 [10] | 9 | 5 | 14 | 64% | Fair |
| Ben-Menachem et al., 2020 [11] | 10 | 4 | 14 | 71% | Fair |
| Efron et al., 2020 [12] | 10 | 4 | 14 | 71% | Fair |
| Freeman et al., 2020 [13] | 14 | 0 | 14 | 100% | Good |
| Meneses-Gaya et al., 2020 [14] | 11 | 3 | 14 | 79% | Good |
| Thiele et al., 2020 [15] | 9 | 5 | 14 | 64% | Fair |
| VanLandingham et al., 2020 [16] | 7 | 7 | 14 | 50% | Fair |
| Crippa et al., 2021 [17] | 14 | 0 | 14 | 100% | Good |
| De Almeida et al., 2021 [18] | 11 | 3 | 14 | 79% | Good |
| Leweke et al., 2021 [19] | 9 | 5 | 14 | 64% | Fair |
| Mongeau-Pérusse et al., 2021 [20] | 11 | 3 | 14 | 79% | Good |
| Atieh et al., 2022 [21] | 10 | 1 | 14 | 71% | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souza, J.D.R.; Pacheco, J.C.; Rossi, G.N.; de-Paulo, B.O.; Zuardi, A.W.; Guimarães, F.S.; Hallak, J.E.C.; Crippa, J.A.; Dos Santos, R.G. Adverse Effects of Oral Cannabidiol: An Updated Systematic Review of Randomized Controlled Trials (2020–2022). Pharmaceutics 2022, 14, 2598. https://doi.org/10.3390/pharmaceutics14122598
Souza JDR, Pacheco JC, Rossi GN, de-Paulo BO, Zuardi AW, Guimarães FS, Hallak JEC, Crippa JA, Dos Santos RG. Adverse Effects of Oral Cannabidiol: An Updated Systematic Review of Randomized Controlled Trials (2020–2022). Pharmaceutics. 2022; 14(12):2598. https://doi.org/10.3390/pharmaceutics14122598
Chicago/Turabian StyleSouza, José Diogo R., Julia Cozar Pacheco, Giordano Novak Rossi, Bruno O. de-Paulo, Antonio W. Zuardi, Francisco S. Guimarães, Jaime E. C. Hallak, José Alexandre Crippa, and Rafael G. Dos Santos. 2022. "Adverse Effects of Oral Cannabidiol: An Updated Systematic Review of Randomized Controlled Trials (2020–2022)" Pharmaceutics 14, no. 12: 2598. https://doi.org/10.3390/pharmaceutics14122598
APA StyleSouza, J. D. R., Pacheco, J. C., Rossi, G. N., de-Paulo, B. O., Zuardi, A. W., Guimarães, F. S., Hallak, J. E. C., Crippa, J. A., & Dos Santos, R. G. (2022). Adverse Effects of Oral Cannabidiol: An Updated Systematic Review of Randomized Controlled Trials (2020–2022). Pharmaceutics, 14(12), 2598. https://doi.org/10.3390/pharmaceutics14122598