
Modelling Hydrocortisone Pharmacokinetics on a Subcutaneous Pulsatile Infusion Replacement Strategy in Patients with Adrenocortical Insufficiency

 ,
, 
 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Results
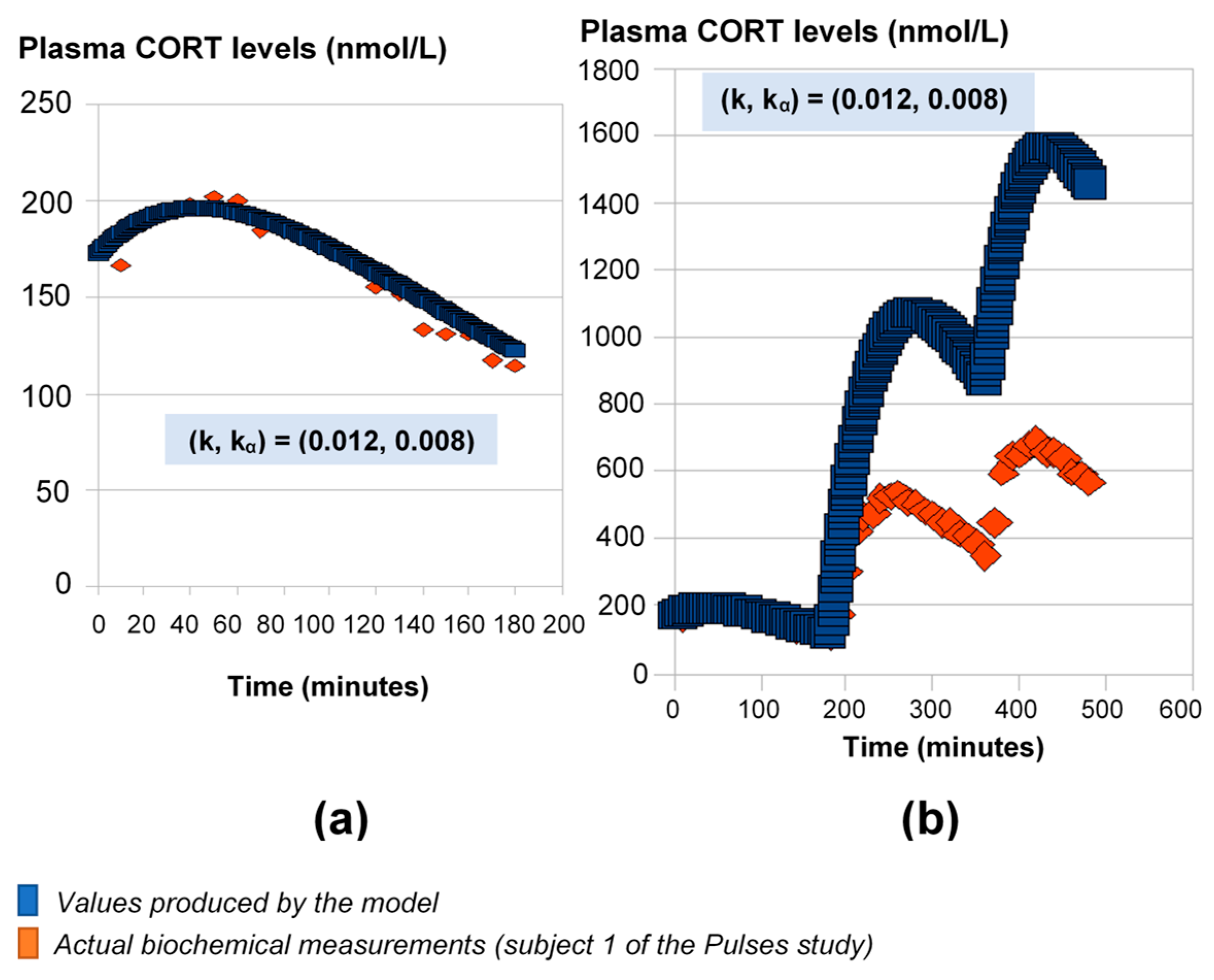
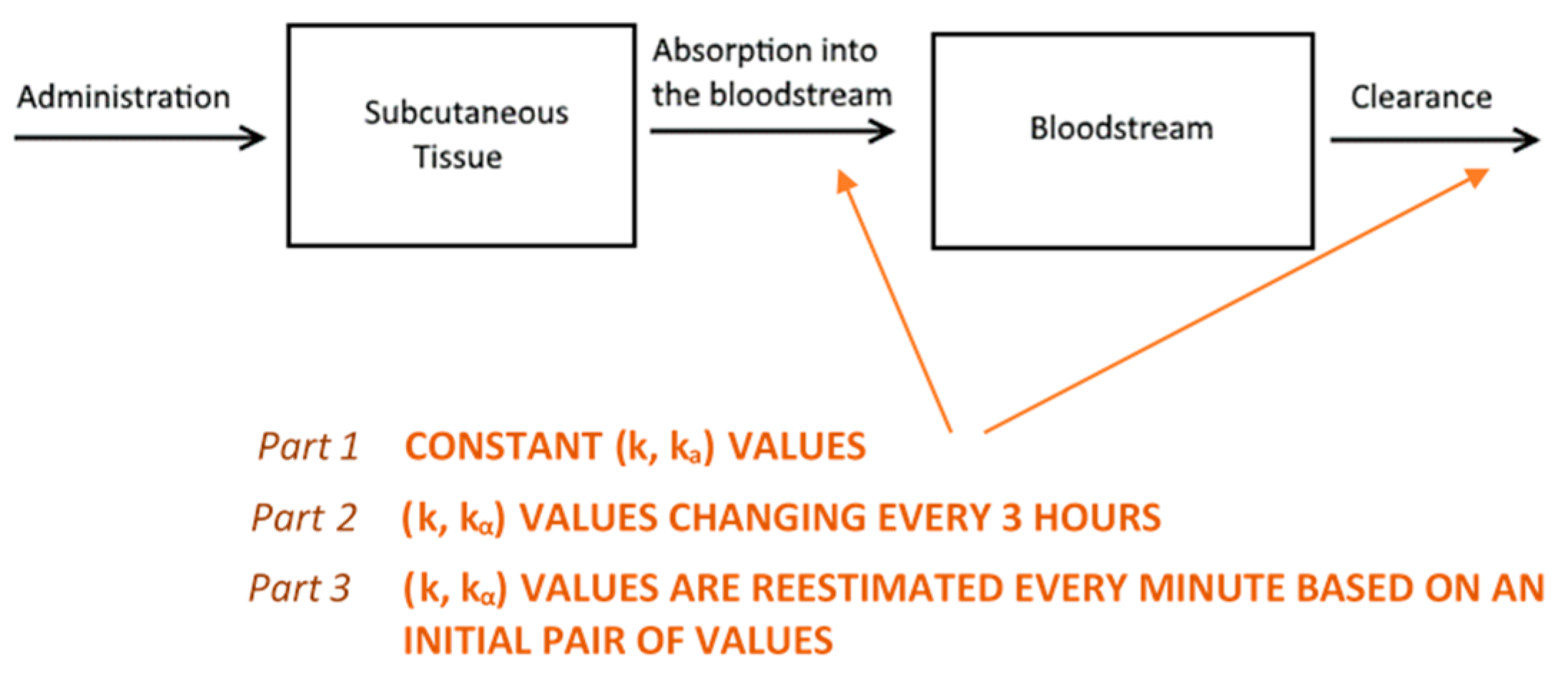
2.1. HC Delivery Assuming Constant Absorption and Clearance Rates
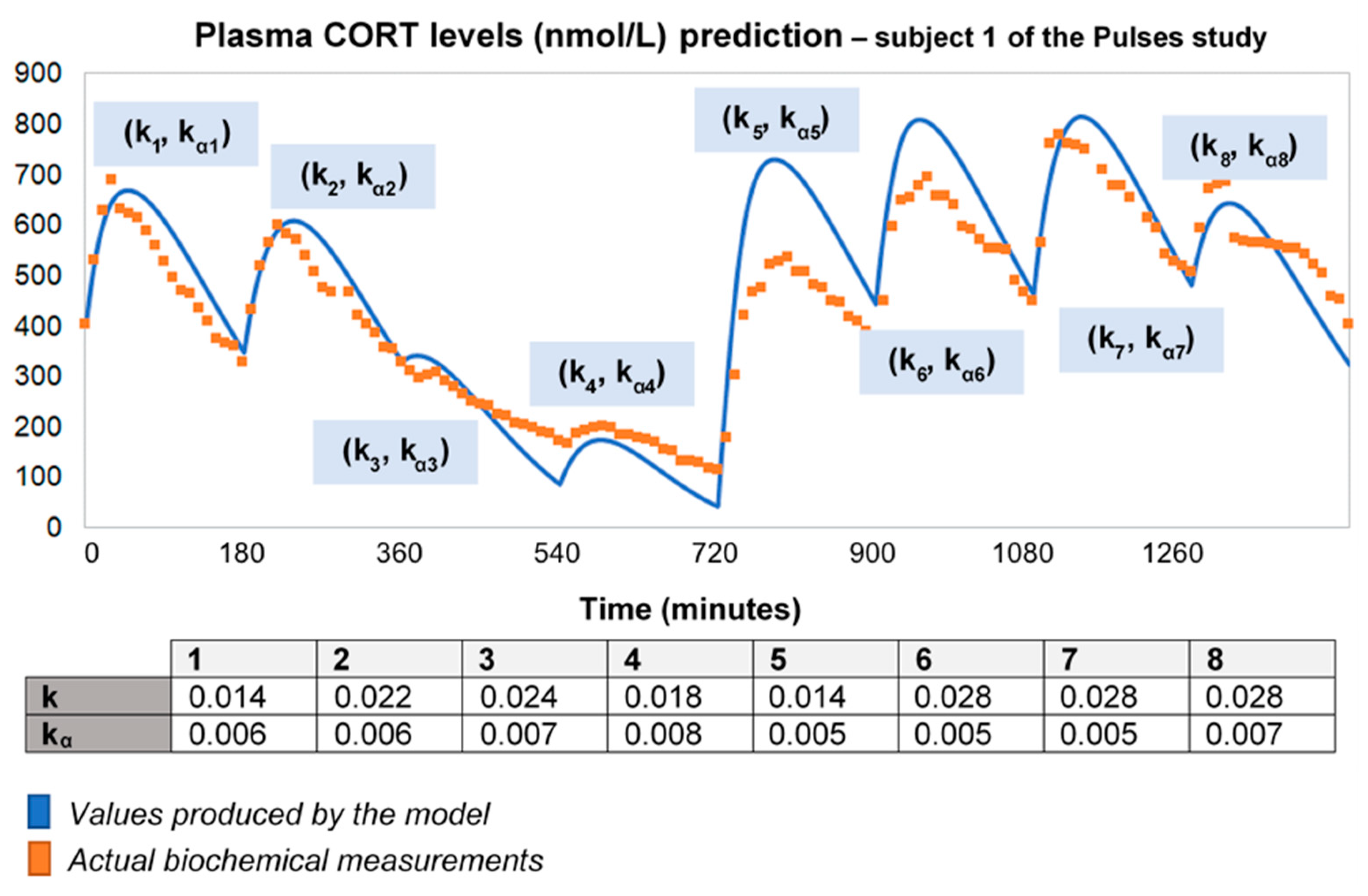
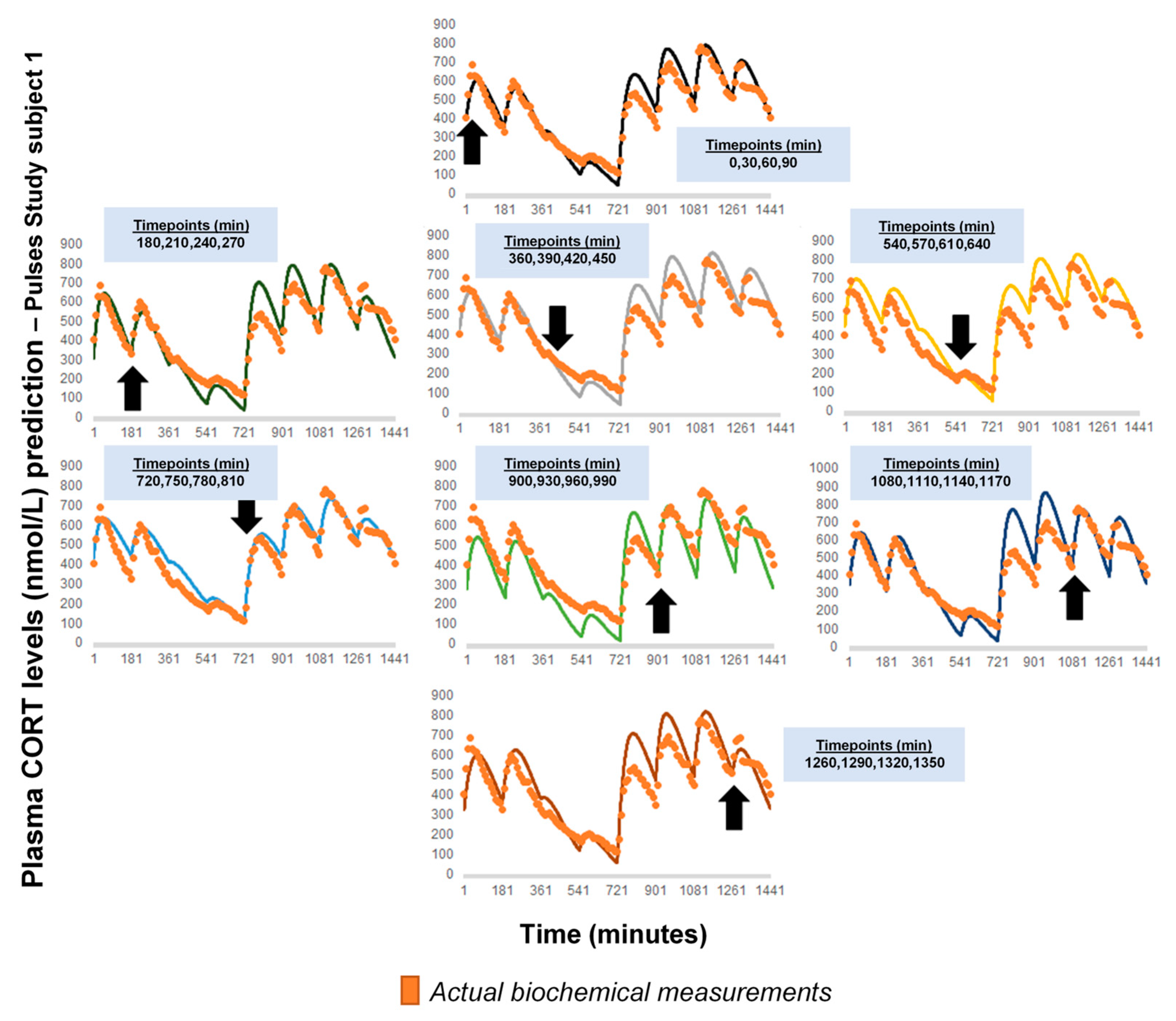
2.2. HC Delivery Assuming Piecewise Absorption and Clearance Rates That Change Every 3 h
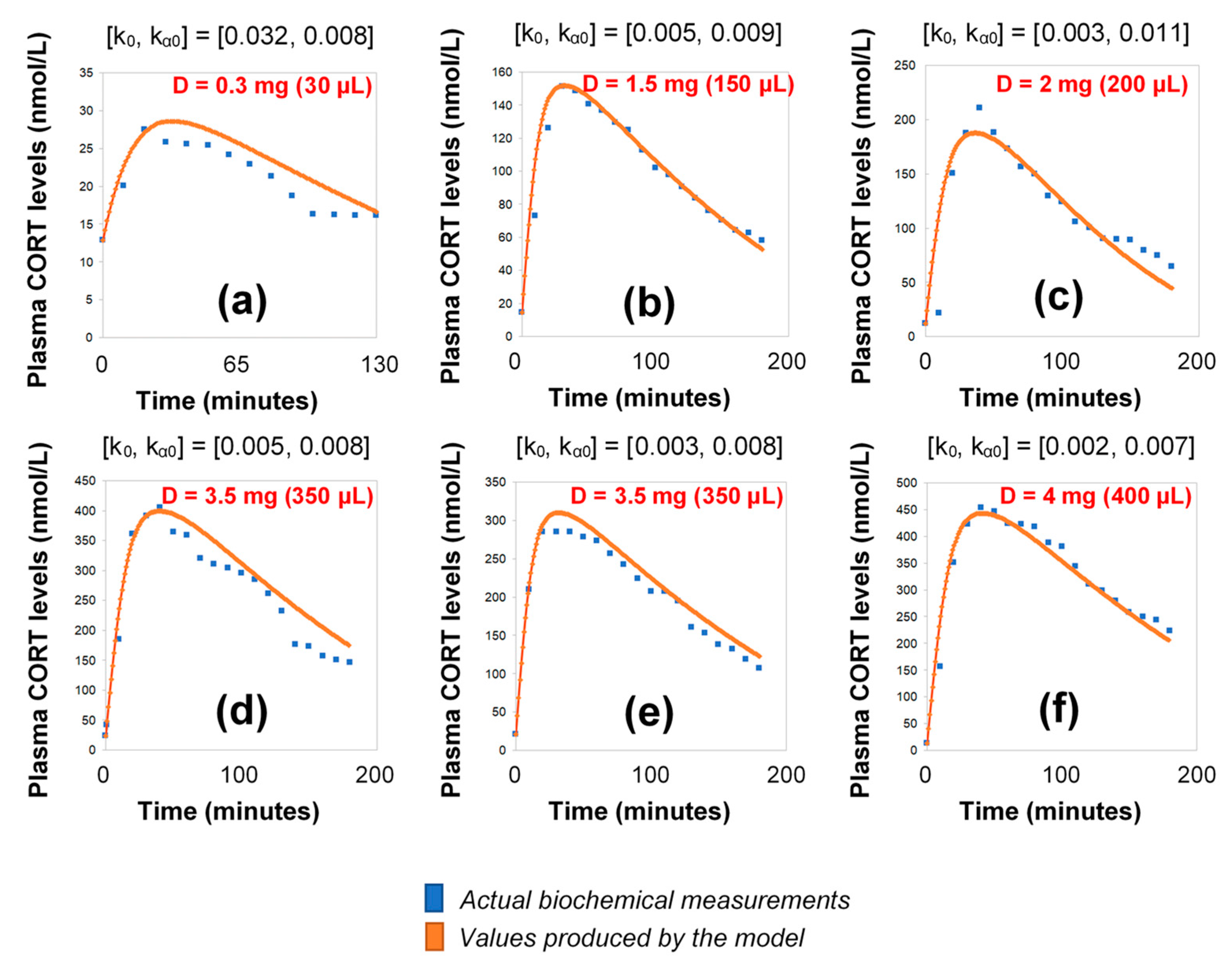
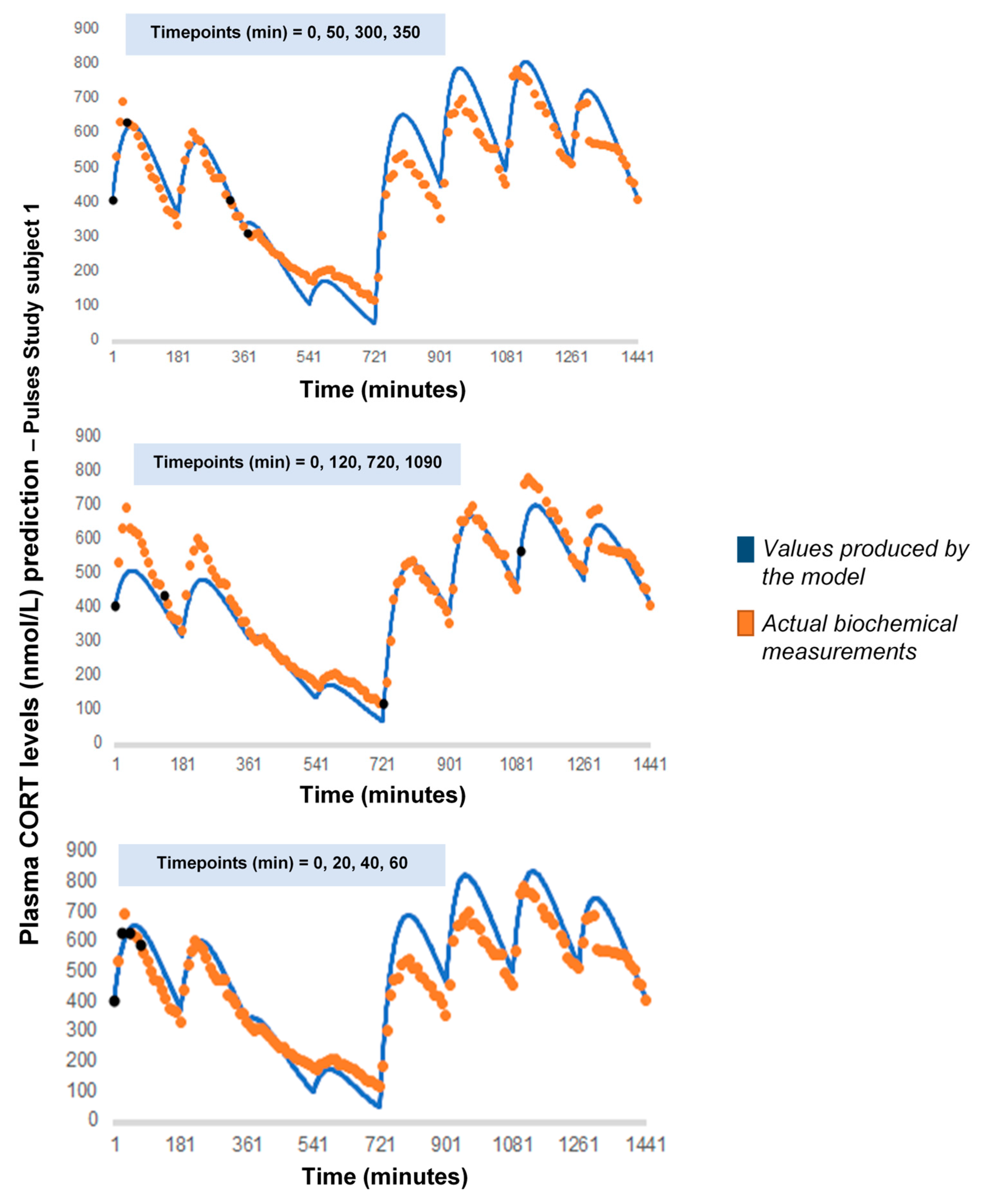
2.3. HC Delivery under Discretely Varying Absorption and Clearance Rates (Optimised Model)
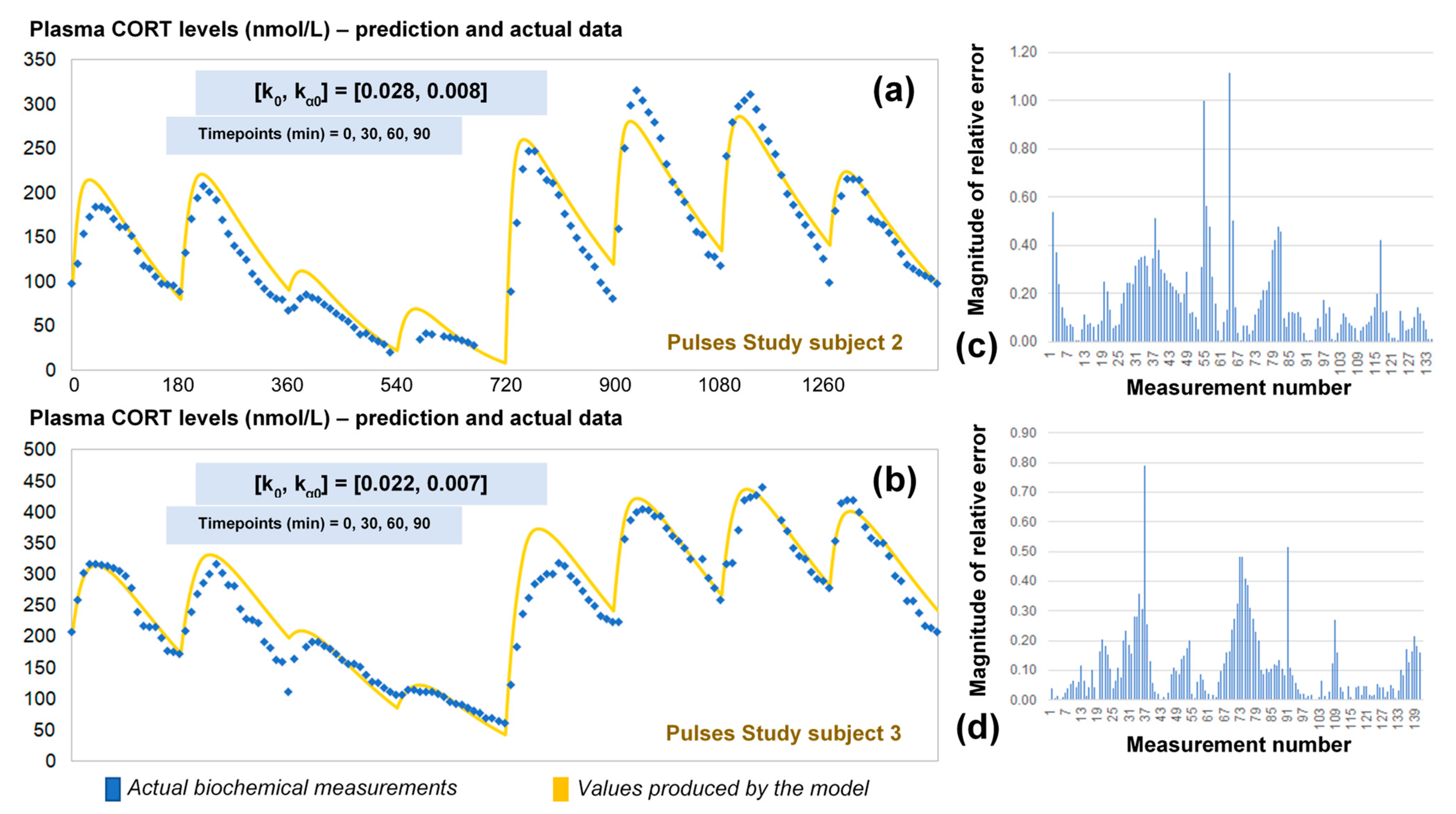
2.4. Validation of the Optimised Model for HC Delivery
2.5. Reaches and Limitations of the Model
3. Discussion
4. Materials and Methods
4.1. Participants and Interventions
4.2. Technical Specifications of Subcutaneous Hydrocortisone Delivery
4.3. Acquisition of Plasma Cortisol Data
4.4. Model Validation Strategy
4.5. Description of Parameters
4.6. Mathematical Modelling
4.6.1. Part 1
4.6.2. Part 2
4.6.3. Part 3
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

Appendix C
Appendix D
Appendix E
Appendix F
Appendix G
References
- Juszczak, G.R.; Stankiewicz, A.M. Glucocorticoids, genes and brain function. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 82, 136–168. [Google Scholar] [CrossRef]
- McEwen, B.S.; De Kloet, E.R.; Rostene, W. Adrenal steroid receptors and actions in the nervous system. Physiol. Rev. 1986, 66, 1121–1188. [Google Scholar] [CrossRef] [PubMed]
- Roozendaal, B.; Hernandez, A.; Cabrera, S.M.; Hagewoud, R.; Malvaez, M.; Stefanko, D.P.; Haettig, J.; Wood, M.A. Membrane-associated glucocorticoid activity is necessary for modulation of long-term memory via chromatin modification. J. Neurosci. 2010, 30, 5037–5046. [Google Scholar] [CrossRef] [PubMed]
- McMaster, A.; Jangani, M.; Sommer, P.; Han, N.; Brass, A.; Beesley, S.; Lu, W.; Berry, A.; Loudon, A.; Donn, R.; et al. Ultradian cortisol pulsatility encodes a distinct; biologically important signal. PLoS ONE 2011, 6, e15766. [Google Scholar] [CrossRef] [PubMed]
- Chapman, K.; Holmes, M.; Seckl, J. 11β-hydroxysteroid dehydrogenases: Intracellular gate-keepers of tissue glucocorticoid action. Physiol. Rev. 2013, 93, 1139–1206. [Google Scholar] [CrossRef] [PubMed]
- Conway-Campbell, B.L.; George, C.L.; Pooley, J.R.; Knight, D.M.; Norman, M.R.; Hager, G.L.; Lightman, S.L. The HSP90 molecular chaperone cycle regulates cyclical transcriptional dynamics of the glucocorticoid receptor and its coregulatory molecules CBP/p300 during ultradian ligand treatment. Mol. Endocrinol. 2011, 25, 944–954. [Google Scholar] [CrossRef]
- Lightman, S.L.; Conway-Campbell, B.L. The crucial role of pulsatile activity of the HPA axis for continuous dynamic equilibration. Nat. Rev. Neurosci. 2010, 11, 710–718. [Google Scholar] [CrossRef]
- Russell, G.M.; Kalafatakis, K.; Lightman, S.L. The importance of biological oscillators for hypothalamic-pituitary adrenal activity and tissue glucocorticoid response: Coordinating stress and neurobehavioural adaptation. J. Neuroendocrinol. 2015, 27, 378–388. [Google Scholar] [CrossRef]
- Meijer, O.C.; Karssen, A.M.; de Kloet, E.R. Cell- and tIssue-specific effects of corticosteroids in relation to glucocorticoid resistance: Examples from the brain. J. Endocrinol. 2003, 178, 13–18. [Google Scholar] [CrossRef]
- Walker, J.J.; Terry, J.R.; Lightman, S.L. Origin of ultradian pulsatility in the hypothalamic-pituitary-adrenal axis. Proc. Biol. Sci. 2010, 277, 1627–1633. [Google Scholar] [CrossRef]
- Kalafatakis, K.; Russell, G.M.; Zarros, A.; Lightman, S.L. Temporal control of glucocorticoid neurodynamics and its relevance for brain homeostasis; neuropathology and glucocorticoid-based therapeutics. Neurosci. Biobehav. Rev. 2016, 61, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Crown, A.; Lightman, S. Management of patients with glucocorticoid deficiency. Nat. Clin. Pract. Endocrinol. Metab. 2005, 1, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Kalafatakis, K.; Russell, G.M.; Harmer, C.J.; Munafo, M.R.; Marchant, N.; Wilson, A.; Brooks, J.C.; Thai, N.J.; Ferguson, S.G.; Stevenson, K.; et al. Effects of the pattern of glucocorticoid replacement on neural processing; emotional reactivity and well-being in healthy male individuals: Study protocol for a randomised controlled trial. Trials 2016, 17, 44. [Google Scholar] [CrossRef] [PubMed]
- Kalafatakis, K.; Russell, G.M.; Harmer, C.J.; Munafo, M.R.; Marchant, N.; Wilson, A.; Brooks, J.C.; Durant, C.; Thakrar, J.; Murphy, P.; et al. Ultradian rhythmicity of plasma cortisol is necessary for normal emotional and cognitive responses in man. Proc. Natl. Acad. Sci. USA 2018, 115, E4091–E4100. [Google Scholar] [CrossRef] [PubMed]
- Russell, G.; Kalafatakis, K.; Thakrar, J.; Hudson, E.; Alim, L.; Marchant, N.; Thirard, R.; Brooks, J.; Thai, J.; Harmer, C.; et al. Differential effects of subcutaneous pulsatile versus oral hydrocortisone replacement therapy on fMRI resting state and task based emotional processing in patients with primary adrenal insufficiency. Endocrine Abstracts 2019, 65, OC2.1. [Google Scholar] [CrossRef]
- Russell, G.M.; Durant, C.; Ataya, A.; Papastathi, C.; Bhake, R.; Woltersdorf, W.; Lightman, S. Subcutaneous pulsatile glucocorticoid replacement therapy. Clin. Endocrinol. 2014, 81, 289–293. [Google Scholar] [CrossRef]
- Kim, D.W.; Zavala, E.; Kim, J.K. Wearable technology and systems modeling for personalized chronotherapy. Curr. Opin. Syst. Biol. 2020, 21, 9–15. [Google Scholar] [CrossRef]
- Lightman, S.L.; Birnie, M.T.; Conway-Campbell, B.L. Dynamics of ACTH and Cortisol Secretion and Implications for Disease. Endocr. Rev. 2020, 41, 470–490. [Google Scholar] [CrossRef]
- Henley, D.E.; Leendertz, J.A.; Russell, G.M.; Wood, S.A.; Taheri, S.; Woltersdorf, W.W.; Lightman, S.L. Development of an automated blood sampling system for use in humans. J. Med. Eng. Technol. 2009, 33, 199–208. [Google Scholar] [CrossRef]
- Kalafatakis, K.; Russell, G.M.; Ferguson, S.G.; Grabski, M.; Harmer, C.J.; Munafo, M.R.; Marchant, N.; Wilson, A.; Brooks, J.C.; Thakrar, J.; et al. Glucocorticoid ultradian rhythmicity differentially regulates mood and resting state networks in the human brain: A randomised controlled clinical trial. Psychoneuroendocrinology 2021, 124, 105096. [Google Scholar] [CrossRef]
- Dorin, R.I.; Qiao, Z.; Qualls, C.R.; Urban, F.K., 3rd. Estimation of maximal cortisol secretion rate in healthy humans. J. Clin. Endocrinol. Metab. 2012, 97, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Jambhekar, S.S.; Breen, P.J. Basic Pharmacokinetics, 2nd ed.; Pharmaceutical Press: London, UK, 2012. [Google Scholar]
- Lemmens, H.J.M.; Bernstein, D.P.; Brodsky, J.B. Estimating blood volume in obese and morbidly obese patients. Obes. Surg. 2006, 16, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, M.; Hernandez-Garcia, A.; Mathiesen, J.; Poulsen, M.; Sørensen, D.N.; Tarnow, L.; Feidenhans’l, R. Model study of the pressure build-up during subcutaneous injection. PLoS ONE 2014, 9, e104054. [Google Scholar] [CrossRef] [PubMed]
- Leuenberger Jockel, J.P.; Roebrock, P.; Shergold, O.A. Insulin depot formation in subcutaneoue tissue. J. Diabetes. Sci. Technol. 2013, 7, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, P.; Stoeber, B. Fluid absorption by skin tissue during intradermal injections through hollow microneedles. Sci. Rep. 2018, 8, 13749. [Google Scholar] [CrossRef] [PubMed]
- Gradel, A.K.J.; Porsgaard, T.; Lykkesfeldt, J.; Seested, T.T.; Gram-Nielsen, S.; Kristensen, N.R.; Refsgaard, H.H.F. Factors Affecting the Absorption of Subcutaneously Administered Insulin: Effect on Variability. J. Diabetes Res. 2018, 1205121. [Google Scholar] [CrossRef]
- Zhu, B.; Zhang, Q.; Pan, Y.; Mace, E.M.; York, B.; Antoulas, A.C.; Dacso, C.C.; O’Malley, B.W. A Cell-Autonomous Mammalian 12 hr Clock Coordinates Metabolic and Stress Rhythms. Cell. Metab. 2017, 25, 1305–1319.e9. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Description | Means of Estimation | Units |
|---|---|---|---|
| C(t) | Plasma cortisol concentration as a function of time. | Predicted by the model | nmol/L |
| Sc(t) | Subcutaneous cortisol concentration as a function of time. | Predicted by the model | mg |
| Di | Hydrocortisone dosage | Known from the experiment | mg |
| kα(t) | Cortisol absorption rate in subcutaneous tissue. Real positive number. | Initial value fitted to data | 1/min |
| k(t) | Plasma cortisol clearance rate. Real positive number. | Initial value fitted to data | 1/min |
| t | Time | Self-explanatory | min |
| σ | Initial cortisol levels in the subjects’ bloodstream (C(0)) | Known from the experiment | nmol/L |
| h | Unit conversion factor for concentration from mg to nmol/L in plasma. Real number, constant, h = 106/(362.42 × ℓ) | Self-explanatory | nmol/mg |
| ℓ | Plasma volume of a typical subject. | Estimated from the literature. | L |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Violaris, I.G.; Kalafatakis, K.; Zavala, E.; Tsoulos, I.G.; Lampros, T.; Lightman, S.L.; Tsipouras, M.G.; Giannakeas, N.; Tzallas, A.; Russell, G.M. Modelling Hydrocortisone Pharmacokinetics on a Subcutaneous Pulsatile Infusion Replacement Strategy in Patients with Adrenocortical Insufficiency. Pharmaceutics 2021, 13, 769. https://doi.org/10.3390/pharmaceutics13060769
Violaris IG, Kalafatakis K, Zavala E, Tsoulos IG, Lampros T, Lightman SL, Tsipouras MG, Giannakeas N, Tzallas A, Russell GM. Modelling Hydrocortisone Pharmacokinetics on a Subcutaneous Pulsatile Infusion Replacement Strategy in Patients with Adrenocortical Insufficiency. Pharmaceutics. 2021; 13(6):769. https://doi.org/10.3390/pharmaceutics13060769
Chicago/Turabian StyleViolaris, Ioannis G., Konstantinos Kalafatakis, Eder Zavala, Ioannis G. Tsoulos, Theodoros Lampros, Stafford L. Lightman, Markos G. Tsipouras, Nikolaos Giannakeas, Alexandros Tzallas, and Georgina M. Russell. 2021. "Modelling Hydrocortisone Pharmacokinetics on a Subcutaneous Pulsatile Infusion Replacement Strategy in Patients with Adrenocortical Insufficiency" Pharmaceutics 13, no. 6: 769. https://doi.org/10.3390/pharmaceutics13060769
APA StyleViolaris, I. G., Kalafatakis, K., Zavala, E., Tsoulos, I. G., Lampros, T., Lightman, S. L., Tsipouras, M. G., Giannakeas, N., Tzallas, A., & Russell, G. M. (2021). Modelling Hydrocortisone Pharmacokinetics on a Subcutaneous Pulsatile Infusion Replacement Strategy in Patients with Adrenocortical Insufficiency. Pharmaceutics, 13(6), 769. https://doi.org/10.3390/pharmaceutics13060769