
Deposition of Inhaled Levofloxacin in Cystic Fibrosis Lungs Assessed by Functional Respiratory Imaging

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Aerosol Characterisation
2.2. Human-Based Cystic Fibrosis Airway Modelling
2.3. Computational Fluid Dynamic (CFD) Simulation
- (1)
- Mild CF breathing pattern: VT of 0.759 L, rate of 21 cycles/min, I:E 1:2.3, and a mean flow rate of 46.5 L/min; and
- (2)
- Moderate CF breathing pattern: VT of 0.608 L, rate of 23 cycles/min, I:E 1:2.14, and a mean flow rate of 50 L/min.
2.4. Statistical Analysis
3. Results and Discussion
3.1. Aerosol Characterisation
3.2. Morphometric Analysis of CF Airways
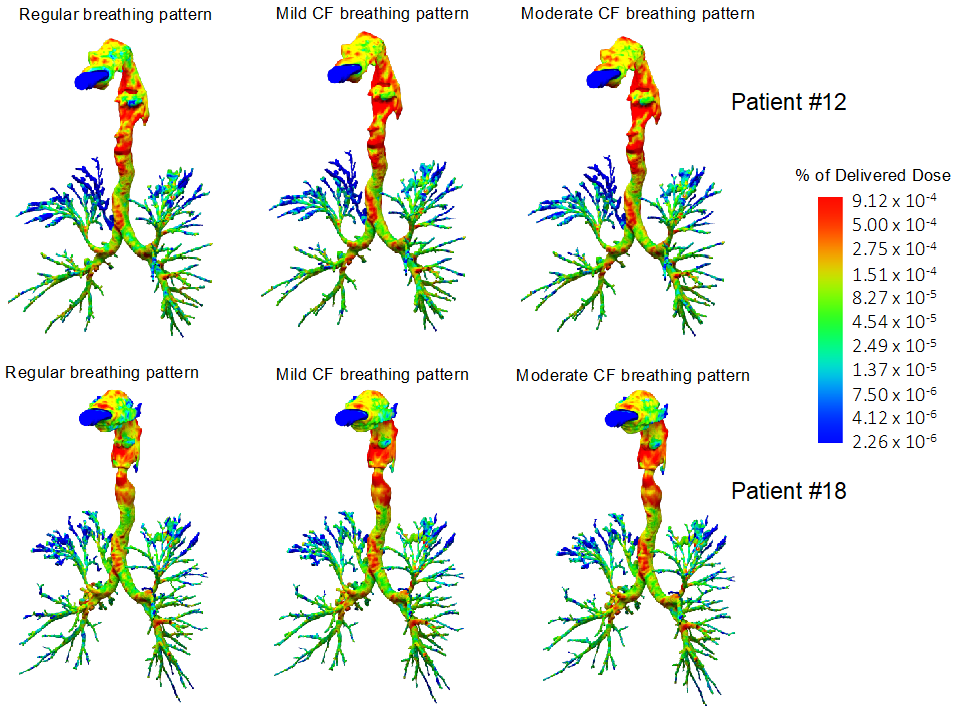
3.3. Comparison of Levofloxacin Deposition with Regular or CF Breathing Patterns
3.4. Comparison of Levofloxacin Deposition on Mild or Moderate CF Airways
3.5. Correlation between Levofloxacin Deposition and FEV1 and FEV1 (%pred)
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elborn, J.S. Cystic fibrosis. Lancet 2017, 388, 2519–2531. [Google Scholar] [CrossRef]
- Schluchter, M.D.; Konstan, M.W.; Drumm, M.L.; Yankaskas, J.R.; Knowles, M.R. Classifying severity of cystic fibrosis lung disease using longitudinal pulmonary function data. Am. J. Respir. Crit. Care Med. 2006, 174, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Loeve, M.; Van Hal, P.T.W.; Robinson, P.; De Jong, P.A.; Lequin, M.H.; Hop, W.C.; Williams, T.J.; Nossent, G.D.; Tiddens, H.A. The spectrum of structural abnormalities on CT scans from patients with CF with severe advanced lung disease. Thorax 2009, 64, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Høiby, N.; Frederiksen, B.; Pressler, T. Eradication of early Pseudomonas aeruginosa infection. J. Cyst. Fibros. 2005, 4, 49–54. [Google Scholar] [CrossRef]
- Ho, D.-K.; Nichols, B.L.B.; Edgar, K.J.; Murgia, X.; Loretz, B.; Lehr, C.-M. Challenges and strategies in drug delivery systems for treatment of pulmonary infections. Eur. J. Pharm. Biopharm. 2019, 144, 110–124. [Google Scholar] [CrossRef]
- Dalhoff, A. Pharmacokinetics and pharmacodynamics of aerosolized antibacterial agents in chronically infected cystic fibrosis patients. Clin. Microbiol. Rev. 2014, 27, 753–782. [Google Scholar] [CrossRef]
- Products for Nebulization—Characterization Tests. In The Unites States Pharmacopeia; USP: Rockville, MD, USA, 2018.
- Van Holsbeke, C.; De Backer, J.; Vos, W.; Marshall, J. Use of functional respiratory imaging to characterize the effect of inhalation profile and particle size on lung deposition of inhaled corticosteroid/long-acting β2-agonists delivered via a pressurized metered-dose inhaler. Ther. Adv. Respir. Dis. 2018, 12, 1753466618760948. [Google Scholar] [CrossRef]
- Bos, A.C.; Van Holsbeke, C.; De Backer, J.W.; Van Westreenen, M.; Janssens, H.M.; Vos, W.G.; Tiddens, H.A.W.M. Patient-specific modeling of regional antibiotic concentration levels in airways of patients with cystic fibrosis: Are we dosing high enough? PLoS ONE 2015, 10, e0118454. [Google Scholar] [CrossRef]
- Bianco, F.; Pasini, E.; Nutini, M.; Murgia, X.; Stoeckl, C.; Schlun, M.; Hetzer, U.; Bonelli, S.; Lombardini, M.; Milesi, I.; et al. Extended pharmacopeial characterization of surfactant aerosols generated by a customized eflow neos nebulizer delivered through neonatal nasal prongs. Pharmaceutics 2020, 12, 319. [Google Scholar] [CrossRef]
- European Cystic Fibrosis Foundation. ECFS Patient Registry Annual Data Report 2018; ECFS: Karup, Denmark, 2018. [Google Scholar]
- Elborn, J.S.; Vataire, A.L.; Fukushima, A.; Aballea, S.; Khemiri, A.; Moore, C.; Medic, G.; Hemels, M.E.H. Comparison of Inhaled Antibiotics for the Treatment of Chronic Pseudomonas aeruginosa Lung Infection in Patients with Cystic Fibrosis: Systematic Literature Review and Network Meta-analysis. Clin. Ther. 2016, 38, 2204–2226. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Bryson, H.M. Levofloxacin. Drugs 1994, 47, 677–700. [Google Scholar] [CrossRef] [PubMed]
- Flume, P.A.; VanDevanter, D.R.; Morgan, E.E.; Dudley, M.N.; Loutit, J.S.; Bell, S.C.; Kerem, E.; Fischer, R.; Smyth, A.R.; Aaron, S.D.; et al. A phase 3, multi-center, multinational, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of levofloxacin inhalation solution (APT-1026) in stable cystic fibrosis patients. J. Cyst. Fibros. 2016, 15, 495–502. [Google Scholar] [CrossRef]
- Elborn, J.S.; Flume, P.A.; Cohen, F.; Loutit, J.; VanDevanter, D.R. Safety and efficacy of prolonged levofloxacin inhalation solution (APT-1026) treatment for cystic fibrosis and chronic Pseudomonas aeruginosa airway infection. J. Cyst. Fibros. 2016, 15, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Stuart Elborn, J.; Geller, D.E.; Conrad, D.; Aaron, S.D.; Smyth, A.R.; Fischer, R.; Kerem, E.; Bell, S.C.; Loutit, J.S.; Dudley, M.N.; et al. A phase 3, open-label, randomized trial to evaluate the safety and efficacy of levofloxacin inhalation solution (APT-1026) versus tobramycin inhalation solution in stable cystic fibrosis patients. J. Cyst. Fibros. 2015, 14, 507–514. [Google Scholar] [CrossRef]
- Schwarz, C.; Grehn, C.; Temming, S.; Holz, F.; Eschenhagen, P.N. Clinical impact of levofloxacin inhalation solution in cystic fibrosis patients in a real-world setting. J. Cyst. Fibros. 2021. [Google Scholar] [CrossRef]
- King, P.; Lomovskaya, O.; Griffith, D.C.; Burns, J.L.; Dudley, M.N. In vitro pharmacodynamics of levofloxacin and other aerosolized antibiotics under multiple conditions relevant to chronic pulmonary infection in cystic fibrosis. Antimicrob. Agents Chemother. 2010, 54, 143–148. [Google Scholar] [CrossRef]
- Geller, D.E.; Weers, J.; Heuerding, S. Development of an inhaled dry-powder formulation of tobramycin using pulmosphereTM technology. J. Aerosol. Med. Pulm. Drug Deliv. 2011, 24, 175–183. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, C.; Barry, P.W. The science of nebulised drug delivery. Thorax 1997, 52, S31–S44. [Google Scholar] [CrossRef] [PubMed]
- Aziz, Z.A.; Davies, J.C.; Alton, E.W.; Wells, A.U.; Geddes, D.M.; Hansell, D.M. Computed tomography and cystic fibrosis: Promises and problems. Thorax 2007, 62, 181–186. [Google Scholar] [CrossRef][Green Version]
- Redondo, M.; Keyt, H.; Dhar, R.; Chalmers, J.D. Global impact of bronchiectasis and cystic fibrosis. Breathe 2016, 12, 222–235. [Google Scholar] [CrossRef]
- Newton, T.J. Respiratory care of the hospitalized patient with cystic fibrosis. Respir. Care 2009, 54, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Lenney, W.; Edenborough, F.; Kho, P.; Kovarik, J.M. Lung deposition of inhaled tobramycin with eFlow rapid/LC Plus jet nebuliser in healthy and cystic fibrosis subjects. J. Cyst. Fibros. 2011, 10, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Riccobene, T.; Scott, C. Lung deposition of inhaled colistimethate sodium in cystic fibrosis patients. Eur. Respir. J. 2014, 44, P1975. [Google Scholar]
- Taylor-Robinson, D.; Whitehead, M.; Diderichsen, F.; Olesen, H.V.; Pressler, T.; Smyth, R.L.; Diggle, P. Understanding the natural progression in %FEV1 decline in patients with cystic fibrosis: A longitudinal study. Thorax 2012, 67, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Kerem, E.; Viviani, L.; Zolin, A.; MacNeill, S.; Hatziagorou, E.; Ellemunter, H.; Drevinek, P.; Gulmans, V.; Krivec, U.; Olesen, H. Factors associated with FEV1 decline in cystic fibrosis: Analysis of the ECFS Patient Registry. Eur. Respir. J. 2014, 43, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Stanojevic, S.; Ratjen, F. Physiologic endpoints for clinical studies for cystic fibrosis. J. Cyst. Fibros. 2016, 15, 416–423. [Google Scholar] [CrossRef] [PubMed]
- De Backer, J.W.; Vos, W.G.; Vinchurkar, S.C.; Claes, R.; Drollmann, A.; Wulfrank, D.; Parizel, P.M.; Germonpré, P.; De Backer, W. Validation of computational fluid dynamics in CT-based airway models with SPECT/CT. Radiology 2010, 257, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, T.; Kozuka, T.; Nakanishi, J.; Yamada, K.; Nishiyama, O.; Sano, H.; Murakami, T.; Tohda, Y. Aerosol Deposition of Inhaled Corticosteroids/Long-Acting β2-Agonists in the Peripheral Airways of Patients with Asthma Using Functional Respiratory Imaging, a Novel Imaging Technology. Pulm. Ther. 2017, 3, 219–231. [Google Scholar] [CrossRef]
- Kappeler, D.; Sommerer, K.; Kietzig, C.; Huber, B.; Woodward, J.; Lomax, M.; Dalvi, P. Lung deposition of fluticasone propionate/formoterol administered via a breath-triggered inhaler. Eur. Respir. J. 2017, 50, PA522. [Google Scholar] [CrossRef]
- Hirst, P.H.; Bacon, R.E.; Pitcairn, G.R.; Silvasti, M.; Newman, S.P. A comparison of the lung deposition of budesonide from Easyhlaler®, Turbuhaler® and pMDI plus spacer in asthmatic patients. Respir. Med. 2001, 95, 720–727. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mild CF | Moderate CF | p-Value | |
|---|---|---|---|
| Number of patients | 7 | 13 | - |
| Sex (male/female) | 5:2 | 9:4 | 0.919 * |
| Age (years) | 23 (18–37) | 27 (19–46) | 0.248 # |
| Height (cm) | 172.5 (161–185) | 169.8 (154–187) | 0.523 # |
| FEV1 (L) | 3.6 (2.78–4.77) | 2.2 (1.54–3.28) | <0.0001 # |
| FEV1 (%pred) | 91 (72–109) | 57 (40–69) | <0.0001 # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwarz, C.; Procaccianti, C.; Mignot, B.; Sadafi, H.; Schwenck, N.; Murgia, X.; Bianco, F. Deposition of Inhaled Levofloxacin in Cystic Fibrosis Lungs Assessed by Functional Respiratory Imaging. Pharmaceutics 2021, 13, 2051. https://doi.org/10.3390/pharmaceutics13122051
Schwarz C, Procaccianti C, Mignot B, Sadafi H, Schwenck N, Murgia X, Bianco F. Deposition of Inhaled Levofloxacin in Cystic Fibrosis Lungs Assessed by Functional Respiratory Imaging. Pharmaceutics. 2021; 13(12):2051. https://doi.org/10.3390/pharmaceutics13122051
Chicago/Turabian StyleSchwarz, Carsten, Claudio Procaccianti, Benjamin Mignot, Hosein Sadafi, Nicolas Schwenck, Xabier Murgia, and Federico Bianco. 2021. "Deposition of Inhaled Levofloxacin in Cystic Fibrosis Lungs Assessed by Functional Respiratory Imaging" Pharmaceutics 13, no. 12: 2051. https://doi.org/10.3390/pharmaceutics13122051
APA StyleSchwarz, C., Procaccianti, C., Mignot, B., Sadafi, H., Schwenck, N., Murgia, X., & Bianco, F. (2021). Deposition of Inhaled Levofloxacin in Cystic Fibrosis Lungs Assessed by Functional Respiratory Imaging. Pharmaceutics, 13(12), 2051. https://doi.org/10.3390/pharmaceutics13122051