
Association between ADCY9 Gene Polymorphisms and Ritodrine Treatment Outcomes in Patients with Preterm Labor

 , ,
, , 
Abstract
:
1. Introduction
2. Methods
2.1. Patients
2.2. Drug Administration
2.3. Outcomes and Data Collection
2.4. Selection of Single Nucleotide Polymorphisms (SNPs)
2.5. Genotyping Methods
2.6. Statistical Analyses
2.7. In Silico Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Preterm Birth: Fact Sheet 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 1 August 2021).
- Scheid, C.R.; Honeyman, T.W.; Fay, F.S. Mechanism of beta-adrenergic relaxation of smooth muscle. Nature 1979, 277, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Sultatos, L.G. Mechanisms of drugs that affect uterine motility. J. Nurse Midwifery 1997, 42, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Neilson, J.P.; West, H.M.; Dowswell, T. Betamimetics for inhibiting preterm labour. Cochrane Database Syst. Rev. 2014, 2, CD004352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.Y.; Lee, N.R.; Lee, K.E.; Park, S.; Kim, Y.J.; Gwak, H.S. Effects of beta2-adrenergic receptor gene polymorphisms on ritodrine therapy in pregnant women with preterm labor: Prospective follow-up study. Int. J. Mol. Sci. 2014, 15, 12885–12894. [Google Scholar] [CrossRef] [PubMed]
- Yee, J.; Hwang, H.S.; Chung, J.E.; Park, J.Y.; Lee, K.E.; Kim, Y.J.; Gwak, H.S. Effects of PDE4 gene polymorphisms on efficacy and adverse drug events of ritodrine therapy in preterm labor patients: A prospective observational study. Eur. J. Clin. Pharmacol. 2019, 75, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; López Bernal, A. Cyclic AMP signalling pathways in the regulation of uterine relaxation. BMC Pregnancy Childbirth 2007, 7 (Suppl. 1), S10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, K.M.; Brown, K.M.; Theiss, C.T.; Seman, C.A.; Weiss, S.T.; Liggett, S.B. An Ile to Met polymorphism in the catalytic domain of adenylyl cyclase type 9 confers reduced beta2-adrenergic receptor stimulation. Pharmacogenetics 2003, 13, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Ye, Y.M.; Lee, H.Y.; Sin, H.J.; Park, H.S. Combined pharmacogenetic effect of ADCY9 and ADRB2 gene polymorphisms on the bronchodilator response to inhaled combination therapy. J. Clin. Pharm. Ther. 2011, 36, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, H.M.; Alcantara-Neves, N.M.; Barreto, M.; Figueiredo, C.A.; Costa, R.S. Adenylyl cyclase type 9 gene polymorphisms are associated with asthma and allergy in Brazilian children. Mol. Immunol. 2017, 82, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Kent, W.J.; Sugnet, C.W.; Furey, T.S.; Roskin, K.M.; Pringle, T.H.; Zahler, A.M.; Haussler, D. The human genome browser at UCSC. Genome Res. 2002, 12, 996–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, L.D.; Kellis, M. HaploReg: A resource for exploring chromatin states, conservation, and regulatory motif alterations within sets of genetically linked variants. Nucleic Acids Res. 2012, 40, D930–D934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, S.B.; Schaffner, S.F.; Nguyen, H.; Moore, J.M.; Roy, J.; Blumenstiel, B.; Higgins, J.; DeFelice, M.; Lochner, A.; Faggart, M.; et al. The structure of haplotype blocks in the human genome. Science 2012, 296, 2225–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharya, A.; Ziebarth, J.D.; Cui, Y. PolymiRTS Database 3.0: Linking polymorphisms in microRNAs and their target sites with human diseases and biological pathways. Nucleic Acids Res. 2014, 42, D86–D91. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V.; Bell, G.W.; Nam, J.W.; Bartel, D.P. Predicting effective microRNA target sites in mammalian mRNAs. Elife 2015, 4, e05005. [Google Scholar] [CrossRef] [PubMed]
- Mayr, C. Regulation by 3′-Untranslated Regions. Annu. Rev. Genet. 2017, 51, 171–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tantisira, K.G.; Small, K.M.; Litonjua, A.A.; Weiss, S.T.; Liggett, S.B. Molecular properties and pharmacogenetics of a polymorphism of adenylyl cyclase type 9 in asthma: Interaction between beta-agonist and corticosteroid pathways. Hum. Mol. Genet. 2005, 14, 1671–1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berndt, S.I.; Gustafsson, S.; Mägi, R.; Ganna, A.; Wheeler, E.; Feitosa, M.F.; Justice, A.E.; Monda, K.L.; Croteau-Chonka, D.C.; Day, F.R.; et al. Genome-wide meta-analysis identifies 11 new loci for anthropometric traits and provides insights into genetic architecture. Nat. Genet. 2013, 45, 501–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartel, D.P. MicroRNAs: Target recognition and regulatory functions. Cell 2009, 36, 215–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortensen, O.A.; Franklin, J.; Löfstrand, T.; Svanberg, B. Prediction of preterm birth. Acta Obstet. Gynecol. Scand. 1987, 6, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, P.; Rudant, J.; Chevret, S.; Boulogne, A.I.; Ville, Y. Repeat measurement of cervical length after successful tocolysis. Obstet. Gynecol. 2004, 104, 95–99. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Number of Patients | Time to Delivery Median (95% CI) | p Value |
|---|---|---|---|
| Age (years) | |||
| <30 | 59 | 1168.6 (764.3–1572.8) | 0.492 |
| ≥30 | 104 | 1040.0 (670.5–1409.5) | |
| Height (cm) | |||
| <160 | 53 | 1027.2 (580.6–1473.7) | 0.419 |
| ≥160 | 110 | 1168.6 (873.7–1463.4) | |
| Weight (kg) | |||
| <60 | 66 | 978.6 (476.1–1481.0) | 0.983 |
| ≥60 | 97 | 1230.6 (964.5–1496.7) | |
| BMI (kg/m2) | |||
| <25 | 112 | 1247.8 (940.7–1554.9) | 0.934 |
| ≥25 | 51 | 1040.0 (656.0–1424.0) | |
| Gestational age at drug therapy (weeks) | |||
| <32 | 111 | 1408.1 (1172.8–1643.5) | <0.001 |
| ≥32 | 52 | 548.0 (272.0–824.0) | |
| Modified Bishop score a | |||
| <3 | 109 | 1247.8 (1112.9–1382.8) | 0.001 |
| ≥3 | 19 | 156.9 (25.5–288.3) | |
| Multiple pregnancy b | 0.207 | ||
| Single | 125 | 1072.6 (800.2–1345.1) | |
| Multiple | 18 | 631.1 (147.2–1114.9) |
| Gene Polymorphism | Minor Allele Frequency (%) | Grouped Genotype | Number of Patients | Time to Delivery Median (95% CI) | p Value |
|---|---|---|---|---|---|
| ADCY9 | |||||
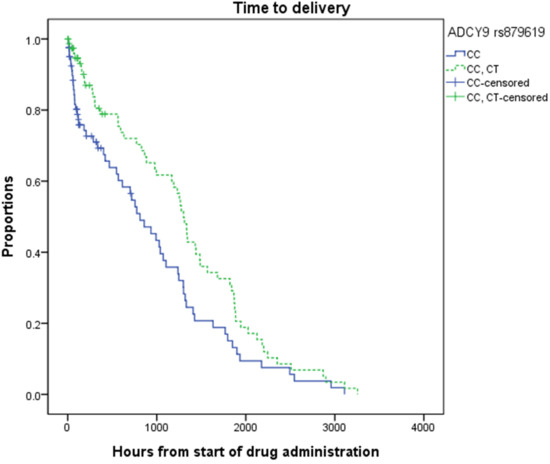
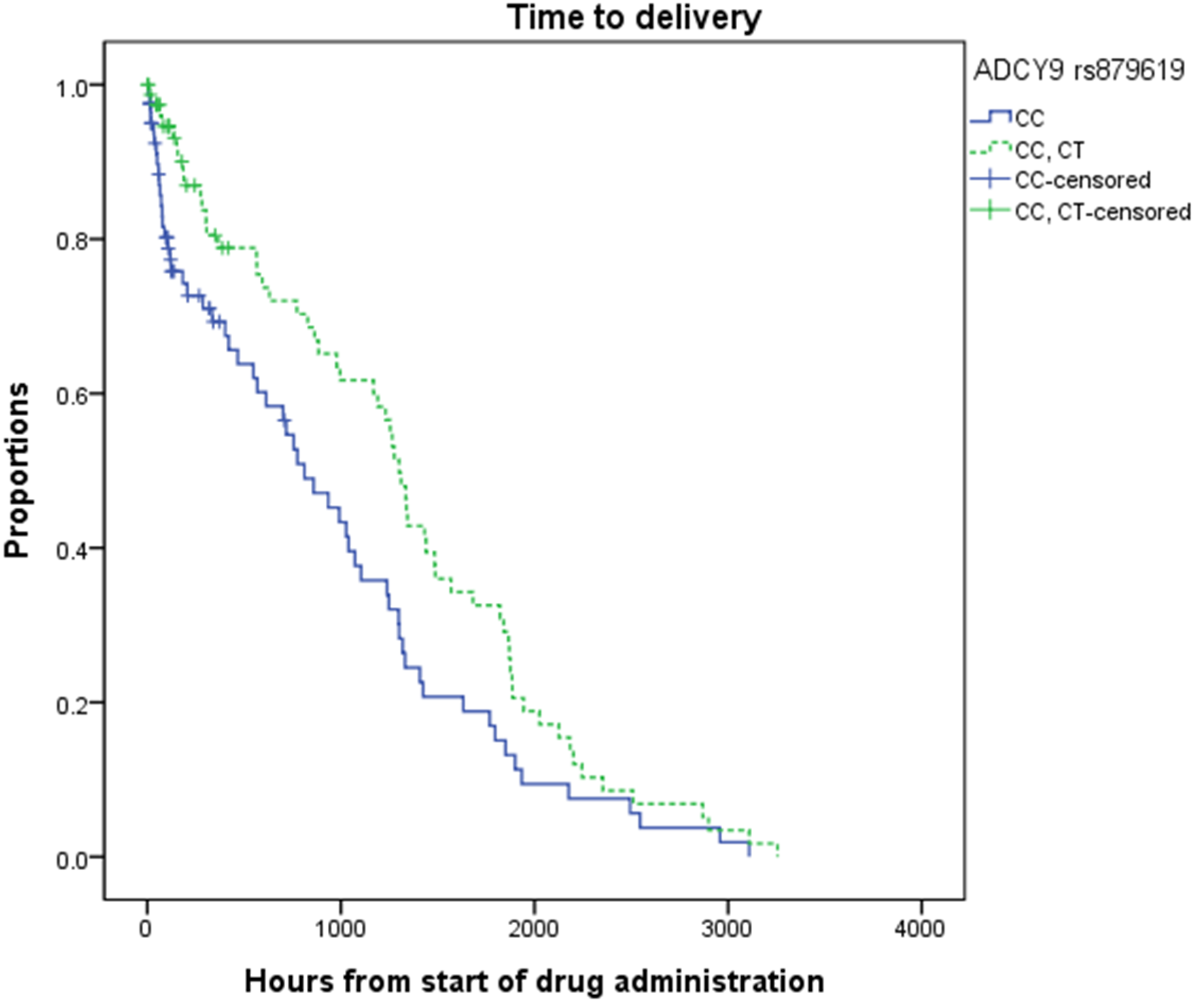
| rs879619 (C > T) a | 27.4 | CC | 82 | 811.6 (532.9–1090.4) | 0.018 |
| CT, TT | 79 | 1300.8 (1187.1–1414.5) | |||
| rs2601796 (C > T) a | 7.6 | CC, CT | 24 | 978.6 (495.4–1461.7) | 0.650 |
| TT | 137 | 1168.6 (874.4–1462.7) | |||
| rs2531988 (T > G) | 28.6 | TT, GT | 83 | 1275.4 (974.3–1576.4) | 0.565 |
| GG | 80 | 934.7 (679.5–1190.0) | |||
| rs2531995 (C > T) | 35.0 | CC, CT | 147 | 1190.7 (961.0–1420.4) | 0.039 |
| TT | 16 | 613.9 (0–1237.0) | |||
| rs2230739 (T > C) b | 38.2 | TT, CT | 142 | 1168.6 (940.2–1396.9) | 0.340 |
| CC | 20 | 613.9 (42.4–1185.5) | |||
| PDE4B | |||||
| rs598961 (G > A) c | 37.1 | GG, GA | 89 | 1298.9 (1162.2–1435.7) | 0.102 |
| AA | 58 | 828.6 (553.3–1103.9) | |||
| ADRB2 | |||||
| rs1042719 (G > C) b | 44.5 | GG | 53 | 1338.5 (950.1–1727.0) | 0.012 |
| GC,CC | 109 | 978.6 (680.5–1276.6) | |||
| ADCY9/PDE4B/ADRB2 | |||||
| rs879619/rs598961/rs1042719 d | N/A | CC/AA/ GC,CC | 20 | 568.6 (0–1261.9) | 0.004 |
| Others | 125 | 1274.8 (1077.3–1432.2) | |||
| rs2531995/rs598961/rs1042719 c | N/A | CC,CT/GG,GA/GG | 25 | 1875.5 (1084.2–2666.8) | <0.001 |
| Others | 122 | 978.6 (738.4–1218.7) |
| Factor | Model I | Model II | Model III |
|---|---|---|---|
| Adjusted HR (95% CI) | Adjusted HR (95% CI) | Adjusted HR (95% CI) | |
| Gestational age at drug therapy (≥32 weeks) | 4.0 (2.4–6.9) *** | 4.7 (2.7–8.3) *** | 4.1 (2.3–7.3) *** |
| Modified Bishop score (≥ 3) | 2.1 (1.2–3.9) * | 2.2 (1.2–4.1) * | 2.3 (1.2–4.3) * |
| ADRB2 rs1042719 (GC,CC) | 1.6 (1.0–2.6) | ||
| ADCY9 rs879619 (CC) | 2.0 (1.3–3.2) ** | 2.1 (1.3–3.3) ** | |
| ADCY9 rs879619/PDE4B rs598961 /ADRB2 rs1042719(CC/AA/GC,CC) | 3.2 (1.7–6.3) ** | ||
| ADCY9 rs2531995/PDE4B rs598961 /ADRB2 rs1042719 (CC,CT/GG,GA/GG) | 0.4 (0.2–0.7) ** |
| Characteristic | Number of Patients (%) | Adverse Drug Events | p Value | |
|---|---|---|---|---|
| Yes (n = 46) | No (n = 117) | |||
| Age (years) | ||||
| <30 | 59 (36.2) | 15 (32.6) | 44 (37.6) | 0.550 |
| ≥30 | 104 (63.8) | 31 (67.4) | 73 (62.4) | |
| Mean ± S.D | 31.0 ± 3.7 | 31.0 ± 4.4 | 30.9 ± 3.5 | 0.880 |
| Height (cm) | ||||
| <160 | 53 (32.5) | 22 (47.8) | 31 (26.5) | 0.009 |
| ≥160 | 110 (67.5) | 24 (52.2) | 86 (73.5) | |
| Mean ± S.D | 161.2 ± 4.5 | 160.3 ± 4.7 | 161.6 ± 4.4 | 0.083 |
| Weight (kg) | ||||
| <60 | 66 (40.5) | 24 (52.2) | 42 (35.9) | 0.057 |
| ≥60 | 97 (59.5) | 22 (47.8) | 75 (64.1) | |
| Mean ± S.D | 62.5 ± 8.5 | 61.0 ± 8.2 | 63.0 ± 8.6 | 0.176 |
| BMI (kg/m2) | ||||
| <25 | 112 (68.7) | 33 (71.7) | 79 (67.5) | 0.601 |
| ≥25 | 51 (31.3) | 13 (28.3) | 38 (32.5) | |
| Mean ± S.D | 24.0 ± 3.0 | 23.7 ± 2.8 | 24.1 ± 3.2 | 0.458 |
| Gestational age at drug therapy(weeks) | ||||
| <32 | 111 (68.1) | 33 (71.7) | 78 (66.7) | 0.532 |
| ≥32 | 52 (31.9) | 13 (28.3) | 39 (33.3) | |
| Mean ± S.D | 29.7 ± 3.7 | 29.0 ± 3.9 | 29.9 ± 3.6 | 0.151 |
| Modified Bishop score a | ||||
| <3 | 109 (85.2) | 32 (91.4) | 77 (82.8) | 0.221 |
| ≥3 | 19 (14.8) | 3 (8.6) | 16 (17.2) | |
| Multiple pregnancy b | 0.098 | |||
| Single | 125 (87.4) | 35 (79.5) | 90 (90.9) | |
| Multiple | 18 (12.6) | 9 (20.5) | 9 (9.1) | |
| rs879619 (C > T) c | ||||
| CC | 82 (50.9) | 22 (47.8) | 60 (52.2) | 0.618 |
| CT, TT | 79 (49.1) | 24 (52.2) | 55 (47.8) | |
| rs2601796 (C > T) c | ||||
| CC, CT | 24 (14.9) | 7 (15.6) | 17 (14.7) | 0.886 |
| TT | 137 (85.1) | 38 (84.4) | 99 (85.3) | |
| rs2531988 (T > G) | ||||
| TT, GT | 83 (50.9) | 22 (47.8) | 61 (52.1) | 0.620 |
| GG | 80 (49.1) | 24 (52.2) | 56 (47.9) | |
| rs2531995 (C > T) | ||||
| CC | 64 (39.3) | 25 (54.3) | 39 (33.3) | 0.013 |
| CT, TT | 99 (60.7) | 21 (45.7) | 78 (66.7) | |
| rs2230739 (T > C) d | ||||
| TT | 66 (40.7) | 21 (45.7) | 45 (38.8) | 0.423 |
| CT, CC | 96 (59.3) | 25 (54.3) | 71 (61.2) | |
| PDE4B rs598961 (G > A) e | ||||
| GG, GA | 89 (60.5) | 20 (52.6) | 69 (63.3) | 0.246 |
| AA | 58 (39.5) | 18 (47.4) | 40 (36.7) | |
| ADRB2 rs1042719 (G > C) d | ||||
| GG, GC | 125 (77.2) | 37 (82.2) | 88 (75.2) | 0.341 |
| CC | 37 (22.8) | 8 (17.8) | 29 (24.8) | |
| ADCY9/ADRB2 rs2531995/rs1042719 d | ||||
| CC/GG,GC | 16 (9.9) | 8 (17.8) | 8 (6.8) | 0.073 |
| Others | 146 (90.1) | 37 (82.2) | 109 (93.2) | |
| Factor | Unadjusted OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|
| Age (≥ 30) | 1.2 (0.6–2.6) | |
| Height (< 160 cm) | 2.5 (1.1–5.2) * | 2.5 (1.2–5.2) * |
| ADRB2 rs1042719 (GG,GC) | 1.5 (0.6–3.6) | |
| ADCY9 rs2531995 (CC) | 2.4 (1.2–4.8) * | 2.2 (1.1–4.2) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, N.; Yoon, H.-Y.; Park, J.-Y.; Kim, Y.-J.; Hwang, H.-S.; Yee, J.; Gwak, H.-S. Association between ADCY9 Gene Polymorphisms and Ritodrine Treatment Outcomes in Patients with Preterm Labor. Pharmaceutics 2021, 13, 1653. https://doi.org/10.3390/pharmaceutics13101653
Lee N, Yoon H-Y, Park J-Y, Kim Y-J, Hwang H-S, Yee J, Gwak H-S. Association between ADCY9 Gene Polymorphisms and Ritodrine Treatment Outcomes in Patients with Preterm Labor. Pharmaceutics. 2021; 13(10):1653. https://doi.org/10.3390/pharmaceutics13101653
Chicago/Turabian StyleLee, Nari, Ha-Young Yoon, Jin-Young Park, Young-Ju Kim, Han-Sung Hwang, Jeong Yee, and Hye-Sun Gwak. 2021. "Association between ADCY9 Gene Polymorphisms and Ritodrine Treatment Outcomes in Patients with Preterm Labor" Pharmaceutics 13, no. 10: 1653. https://doi.org/10.3390/pharmaceutics13101653
APA StyleLee, N., Yoon, H.-Y., Park, J.-Y., Kim, Y.-J., Hwang, H.-S., Yee, J., & Gwak, H.-S. (2021). Association between ADCY9 Gene Polymorphisms and Ritodrine Treatment Outcomes in Patients with Preterm Labor. Pharmaceutics, 13(10), 1653. https://doi.org/10.3390/pharmaceutics13101653