
The Association Between HIV Infection and Carotid Intima-Media Thickness in the Era of Antiretroviral Therapy: A Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection Process
2.4. Data Extraction and Management
2.5. Methodological Quality Assessment and Risk of Bias
2.6. Data Preparation and Analysis
3. Results
3.1. Overview of Search and Selection
3.2. Basic Characteristics of Included Studies
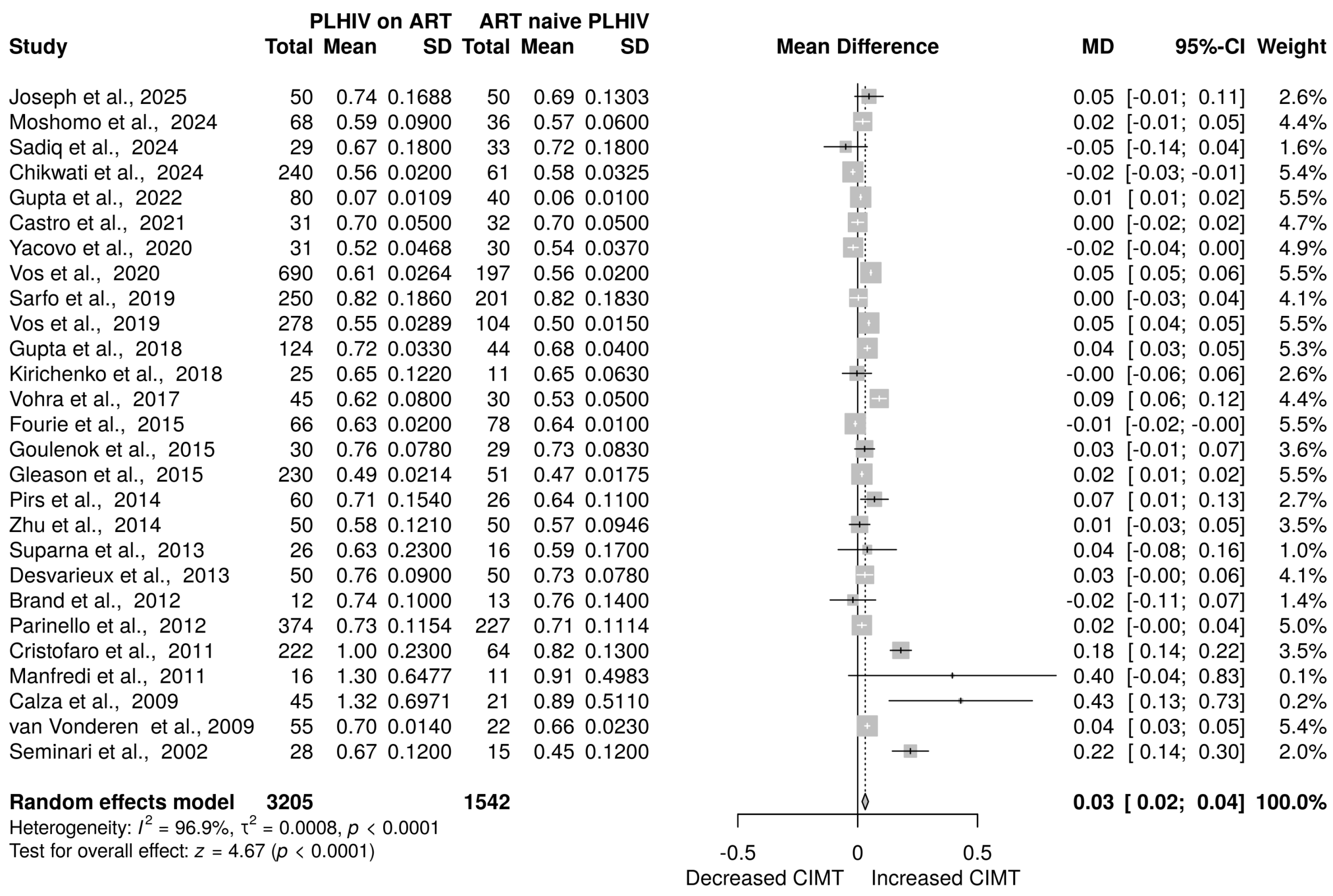
3.3. The Effect of ART on Carotid Progression in PLHIV
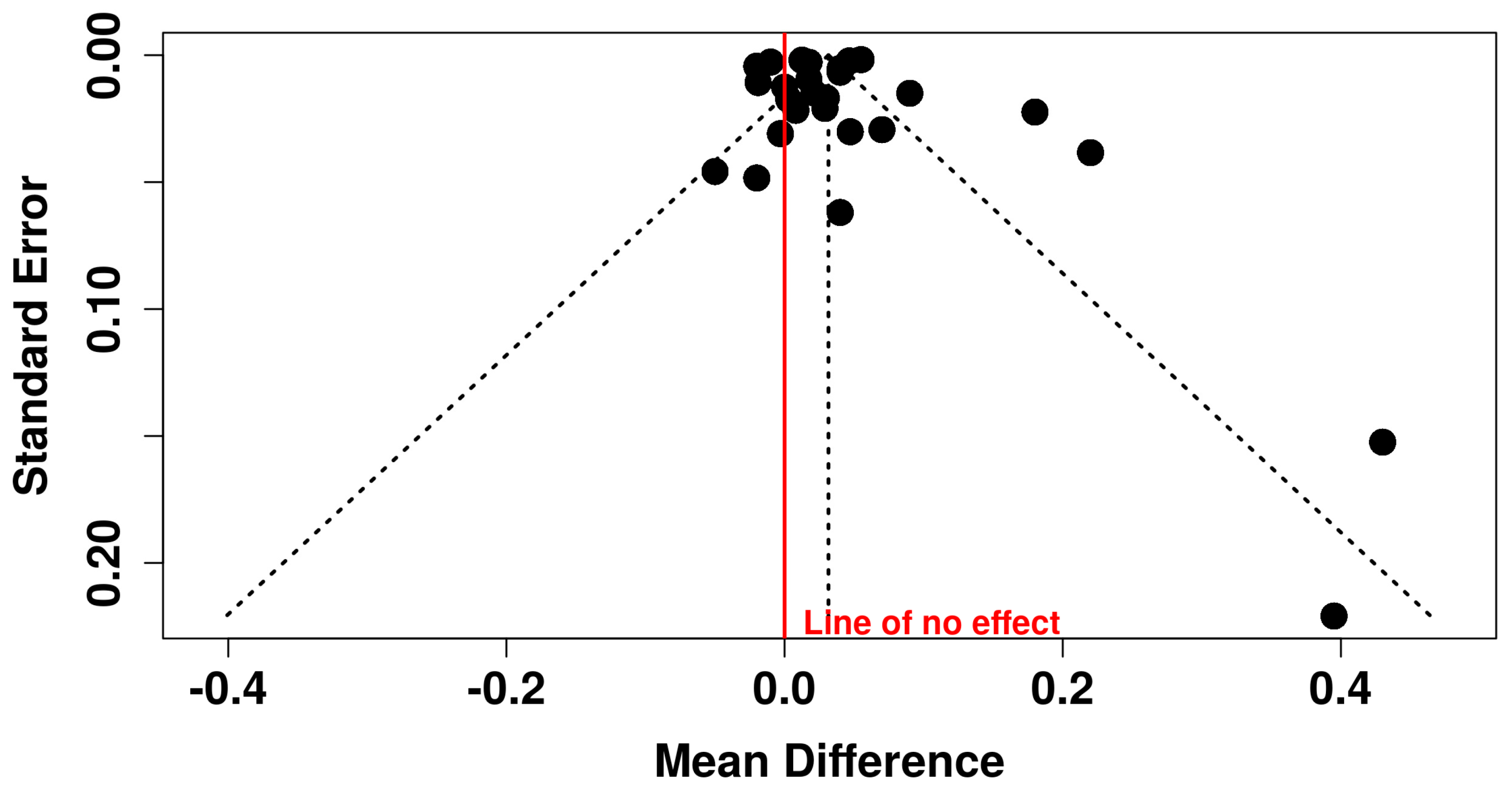
3.4. Assessment of Publication Bias
3.5. Subgroup Analysis
3.6. Sensitivity Analysis
3.7. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ART | Antiretroviral therapy |
| BMI | Body mass index |
| CIMT | Carotid-intima media thickness |
| CVD | Cardiovascular disease |
| HAART | Highly active antiretroviral therapy |
| HIV | Human immune viruses |
| Nef | Negative regulatory factors |
| PI | Protease inhibitors |
| PLHIV | People living with human immunodeficiency virus |
| ROS | Reactive oxygen species |
References
- So-Armah, K.; Benjamin, L.A.; Bloomfield, G.S.; Feinstein, M.J.; Hsue, P.; Njuguna, B.; Freiberg, M.S. HIV and Cardiovascular Disease. Lancet HIV 2020, 7, e279–e293. [Google Scholar] [CrossRef]
- HIV. Available online: https://www.who.int/data/gho/data/themes/hiv-aids (accessed on 10 May 2024).
- Ntinga, X.; Musiello, F.; Pita, T.; Mabaso, N.; Celum, C.; Szpiro, A.; van Rooyen, H.; Barnabas, R.; van Heerden, A. People Living with HIV’s Perspectives of Acceptability of Fee for Home Delivery of ART: A Qualitative Study. BMC Health Serv. Res. 2024, 24, 88. [Google Scholar] [CrossRef] [PubMed]
- Vemulapalli, A.C.; Elias, A.A.; Yerramsetti, M.D.; Olanisa, O.O.; Jain, P.; Khan, Q.S.; Butt, S.R. The Impact of Contemporary Antiretroviral Drugs on Atherosclerosis and Its Complications in People Living With HIV: A Systematic Review. Cureus 2023, 15, e47730. [Google Scholar] [CrossRef] [PubMed]
- Lacobellis, G.; Sharma, A.M.; Pellicelli, A.M.; Grisorio, B.; Barbarini, G.; Barbaro, G. Epicardial Adipose Tissue Is Related to Carotid Intima-Media Thickness and Visceral Adiposity in HIV-Infected Patients with Highly Active Antiretroviral Therapy-Associated Metabolic Syndrome. Curr. HIV Res. 2007, 5, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Hsue, Y.; Lo, J.C.; Franklin, A.; Bolger, A.F.; Martin, J.N.; Deeks, S.G.; Waters, D.D. Progression of Atherosclerosis as Assessed by Carotid Intima-Media Thickness in Patients with HIV Infection. Circulation 2004, 109, 1603–1608. [Google Scholar] [CrossRef]
- Delaney, J.A.C.; Scherzer, R.; Biggs, M.L.; Shliplak, M.G.; Polak, J.F.; Currier, J.S.; Kronmal, R.A.; Wanke, C.; Bacchetti, P.; O’leary, D.; et al. Associations of Antiretroviral Drug Use and HIV-Specific Risk Factors with Carotid Intima–Media Thickness. AIDS 2010, 24, 2201–2209. [Google Scholar] [CrossRef]
- Strauss, K.L.E.; Phoswa, W.N.; Lebelo, S.L.; Modjadji, P.; Mokgalaboni, K. Endothelial Dysfunction, a Predictor of Cardiovascular Disease in HIV Patients on Antiretroviral Therapy: A Systematic Review and Meta-Analysis. Thromb. Res. 2024, 234, 101–112. [Google Scholar] [CrossRef]
- Zanella, I.; Biasiotto, G.; Castelli, F.; Calza, S.; Carriero, C.; Degli Antoni, M.; Focà, E.; Quiros-Roldan, E. Descriptive Modification of Inflammatory Markers in HIV Patients after CART Initiation According to Gender, Smoking Habit, CMV Infection, BMI and Serum Lipids. Cytokine 2021, 143, 155547. [Google Scholar] [CrossRef]
- The DAD Study Group. Class of Antiretroviral Drugs and the Risk of Myocardial Infarction. N. Engl. J. Med. 2007, 356, 1723–1735. [Google Scholar] [CrossRef]
- Jaschinski, N.; Greenberg, L.; Neesgaard, B.; Miró, J.M.; Grabmeier-Pfistershammer, K.; Wandeler, G.; Smith, C.; De Wit, S.; Wit, F.; Pelchen-Matthews, A.; et al. Recent Abacavir Use and Incident Cardiovascular Disease in Contemporary-Treated People with HIV. AIDS 2023, 37, 467–475. [Google Scholar] [CrossRef]
- Adedokun, T.A.; Kwaghe, V.G.; Adedokun, O.; Badru, T.; Odili, A.N.; Alfa, J.; Kolade-Yunusa, H.O.; Ojji, D.B. Prevalence and Risk Factors for Subclinical Atherosclerosis amongst Adults Living with HIV in University of Abuja Teaching Hospital, Gwagwalada. Front. Reprod. Health 2023, 5, 1092211. [Google Scholar] [CrossRef] [PubMed]
- Mclaughlin, M.M.; Ma, Y.; Scherzer, R.; Rahalkar, S.; Martin, J.N.; Mills, C.; Milush, J.; Deeks, S.G.; Hsue, P.Y. Association of Viral Persistence and Atherosclerosis in Adults with Treated HIV Infection. JAMA Netw. Open 2020, 3, e2018099. [Google Scholar] [CrossRef]
- Hyle, E.P.; Mayosi, B.M.; Middelkoop, K.; Mosepele, M.; Martey, E.B.; Walensky, R.P.; Bekker, L.G.; Triant, V.A. The Association between HIV and Atherosclerotic Cardiovascular Disease in Sub-Saharan Africa: A Systematic Review. BMC Public Health 2017, 17, 954. [Google Scholar] [CrossRef]
- Calza, L.; Manfredi, R.; Colangeli, V.; Trapani, F.F.; Salvadori, C.; Magistrelli, E.; Danese, I.; Verucchi, G.; Serra, C.; Viale, P. Two-Year Treatment with Rosuvastatin Reduces Carotid Intima-Media Thickness in HIV Type 1-Infected Patients Receiving Highly Active Antiretroviral Therapy with Asymptomatic Atherosclerosis and Moderate Cardiovascular Risk. AIDS Res. Hum. Retroviruses 2013, 29, 547–556. [Google Scholar] [CrossRef]
- Nou, E.; Lo, J.; Grinspoon, S.K. Inflammation, Immune Activation, and Cardiovascular Disease in HIV. AIDS 2016, 30, 1495–1509. [Google Scholar] [CrossRef]
- Vos, A.G.; Dodd, C.N.; Delemarre, E.M.; Nierkens, S.; Serenata, C.; Grobbee, D.E.; Klipstein-Grobusch, K.; Venter, W.D.F. Patterns of Immune Activation in HIV and Non HIV Subjects and Its Relation to Cardiovascular Disease Risk. Front. Immunol. 2021, 12, 647805. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Stephan, C.; Harmjanz, A.; Staszewski, S.; Buehler, A.; Bickel, M.; von Kegler, S.; Ruhkamp, D.; Steinmetz, H.; Sitzer, M. Both Long-Term HIV Infection and Highly Active Antiretroviral Therapy Are Independent Risk Factors for Early Carotid Atherosclerosis. Atherosclerosis 2008, 196, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Sun, Y.; Zhan, Y.; Jiang, Y. Prevalence and Risk of Subclinical Carotid Atherosclerosis in the Global Population with HIV: A Systematic Review and Meta-Analysis. Int. J. STD AIDS 2021, 32, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.K.; Tyagi, S.; Sheoran, A.; Jain, P.; Koner, S.K.; Sharma, L.K.; Singh, S.K.; Khura, J. Effect of Antiretroviral Therapy on Cardiac Risk Markers in People Living with HIV/AIDS. Indian J. Sex. Transm. Dis. AIDS 2022, 43, 52–55. [Google Scholar] [CrossRef]
- Vos, A.G.; Barth, R.E.; Klipstein-Grobusch, K.; Tempelman, H.A.; Devillé, W.L.J.; Dodd, C.; Coutinho, R.A.; Grobbee, D.E. Cardiovascular Disease Burden in Rural Africa: Does Hiv and Antiretroviral Treatment Play a Role? J. Am. Heart Assoc. 2020, 9, 107812. [Google Scholar] [CrossRef]
- Majonga, E.D.; Chiesa, S.T.; McHugh, G.; Mujuru, H.; Nathoo, K.; Odland, J.O.; Kaski, J.P.; Ferrand, R.A. Carotid Intima Media Thickness in Older Children and Adolescents with HIV Taking Antiretroviral Therapy. Medicine 2020, 99, e19554. [Google Scholar] [CrossRef] [PubMed]
- Nalado, A.M.; Waziri, B.; Ismail, A.; Umar, N.; Ibrahim, Z.U.; Obiagwu, P.; Musa, B.M.; Sani, M.U.; Abdu, A.; Dankishiya, F.S.; et al. Prevalence and Determinants of Endothelial Dysfunction among Adults Living with HIV in Northwest Nigeria. Glob. Heart 2023, 18, 87. [Google Scholar] [CrossRef]
- Sadiq, E.; Woodiwiss, A.; Tade, G.; Norton, G.; Modi, G. Lack of Impact of HIV Status on Carotid Intima Media Thickness in a Cohort of Stroke Patients in South Africa. J. Neurol. Sci. 2024, 465, 123186. [Google Scholar] [CrossRef]
- Majonga, E.D.; Ferrand, R.A.; Deanfield, J.E.; Chiesa, S.T. The Effect of Perinatal HIV and Antiretroviral Therapy on Vascular Structure and Function in Young People: A Systematic Review and Meta-Analysis. Atherosclerosis 2022, 352, 53–61. [Google Scholar] [CrossRef]
- Msoka, T.F.; Van Guilder, G.P.; van Furth, M.; Smulders, Y.; Meek, S.J.; Bartlett, J.A.; Vissoci, J.R.N.; van Agtmael, M.A. The Effect of HIV Infection, Antiretroviral Therapy on Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis. Life Sci. 2019, 235, 116851. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 1–9. [Google Scholar]
- Why the HIV Epidemic Is Not Over. Available online: https://www.who.int/news-room/spotlight/why-the-hiv-epidemic-is-not-over (accessed on 15 September 2024).
- McHugh, M.L. Interrater Reliability: The Kappa Statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality If Nonrandomized Studies in Meta-Analyses. 2012. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 19 November 2024).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Doleman, B.; Freeman, S.C.; Lund, J.N.; Williams, J.P.; Sutton, A.J. Funnel Plots May Show Asymmetry in the Absence of Publication Bias with Continuous Outcomes Dependent on Baseline Risk: Presentation of a New Publication Bias Test. Res. Synth. Methods 2020, 11, 522–534. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, P. Meta-Analyses: Heterogeneity and Subgroup Analysis. BMJ 2013, 346, f4040. [Google Scholar] [CrossRef]
- Mathur, M.B.; VanderWeele, T.J. Sensitivity Analysis for Publication Bias in Meta-Analyses. J. R. Stat. Soc. Ser. C Appl. Stat. 2020, 69, 1091–1119. [Google Scholar] [CrossRef] [PubMed]
- Fekete, J.T.; Győrffy, B. MetaAnalysisOnline.Com: Web-Based Tool for the Rapid Meta-Analysis of Clinical and Epidemiological Studies. J. Med. Internet Res. 2025, 27, e64016. [Google Scholar] [CrossRef]
- Moshomo, T.; Molefe-Baikai, O.J.; Bennett, K.; Gaolathe, T.; Moyo, S.; Gaseitsewe, S.; Mohammed, T.; Lockman, S.; Mosepele, M. Cytomegalovirus Immunoglobulin G Levels and Subclinical Arterial Disease among People Living with HIV in Botswana: A Cross-Sectional Study. Biomedicines 2024, 12, 935. [Google Scholar] [CrossRef]
- Castro, G.; León, K.; Marín-Palma, D.; Oyuela, S.M.; Cataño-Bedoyam, J.U.; Duque-Botero, J.; Giraldo-Méndez, D.P.; Taborda, N.A.; Hernandez, J.C.; Rugeles, M.T.; et al. Evaluation of Differences in Metabolic and Immunologic Markers and Cardiovascular Risk in Hiv-1 Patients. Rev. Cienc. Salud 2021, 19, 1–18. [Google Scholar] [CrossRef]
- Kirichenko, T.V.; Myasoedova, V.A.; Shimonova, T.E.; Melnichenko, A.A.; Sviridov, D.; Sobenin, I.A.; Mazus, A.I.; Orekhov, A.N.; Bukrinsky, M.I. Atherosclerosis in Subjects Newly Diagnosed with Human Immunodeficiency Virus Infection. Biosci. Rep. 2018, 38, BSR20180597. [Google Scholar] [CrossRef]
- Fourie, C.M.T.; Schutte, A.E.; Smith, W.; Kruger, A.; van Rooyen, J.M. Endothelial Activation and Cardiometabolic Profiles of Treated and Never-Treated HIV Infected Africans. Atherosclerosis 2015, 240, 154–160. [Google Scholar] [CrossRef]
- Goulenok, T.; Boyd, A.; Larsen, M.; Fastenackels, S.; Boccara, F.; Meynard, J.L.; Hadour, N.; Samri, A.; Desvarieux, M.; Autrana, B.; et al. Increased Carotid Intima-Media Thickness Is Not Associated with T-Cell Activation nor with Cytomegalovirus in HIV-Infected Neversmoker Patients. AIDS 2015, 29, 287–293. [Google Scholar] [CrossRef]
- Zhu, H.; Yuan, J.; Wang, Y.; Gao, F.; Wang, X.; Wei, C.; Chen, J.; Fan, X.; Zhang, M. Long-Term Use of First-Line Highly Active Antiretroviral Therapy Is Not Associated with Carotid Artery Stiffness in Human Immunodeficiency Virus-Positive Patients. Braz. J. Infect. Dis. 2014, 18, 496–500. [Google Scholar] [CrossRef]
- Suparna, P.N.; Achappa, B.; Unnikrishnan, B.; Madi, D.; Chowta, M.N.; Ramapuram, J.T.; Rao, S.; Mahalingam, S. The Evaluation of Carotid Atherosclerosis in Patients with the HIV-1 Infection: The Role of the Antiretroviral Therapy. J. Clin. Diagn. Res. 2013, 7, 261–264. [Google Scholar] [CrossRef]
- Desvarieux, M.; Boccara, F.; Meynard, J.L.; Bastard, J.P.; Mallat, Z.; Charbit, B.; Demmer, R.T.; Haddour, N.; Fellahi, S.; Tedgui, A.; et al. Infection Duration and Inflammatory Imbalance Are Associated with Atherosclerotic Risk in HIV-Infected Never-Smokers Independent of Antiretroviral Therapy. AIDS 2013, 27, 2603–2614. [Google Scholar] [CrossRef]
- Cristofaro, M.; Cicalini, S.; Busi Rizzi, E.; Schininà, V.; Petrosillo, N.; Bibbolino, C. Valutazione Ecografica Delle Lesioni Vascolari Carotidee Nei Pazienti HIV Positivi. Radiol. Medica 2011, 116, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Van Vonderen, M.G.A.; Smulders, Y.M.; Stehouwer, C.D.A.; Danner, S.A.; Gundy, C.M.; Vos, F.; Reiss, P.; Van Agtmael, M.A. Carotid Intima-Media Thickness and Arterial Stiffness in HIV-Infected Patients: The Role of HIV, Antiretroviral Therapy, and Lipodystrophy. J. Acquir. Immune Defic. Syndr. 2009, 50, 153–161. [Google Scholar] [CrossRef]
- Di Yacovo, S.; Saumoy, M.; Sánchez-Quesada, J.L.; Navarro, A.; Sviridov, D.; Javaloyas, M.; Vila, R.; Vernet, A.; Low, H.; Peñafiel, J.; et al. Lipids, Biomarkers, and Subclinical Atherosclerosis in Treatment-Naive HIV Patients Starting or Not Starting Antiretroviral Therapy: Comparison with a Healthy Control Group in a 2-Year Prospective Study. PLoS ONE 2020, 15, e0237739. [Google Scholar] [CrossRef] [PubMed]
- Sarfo, F.S.; Nichols, M.; Agyei, B.; Singh, A.; Ennin, E.; Nyantakyi, A.D.; Asibey, S.O.; Tagge, R.; Gebregziabher, M.; Jenkins, C.; et al. Burden of Subclinical Carotid Atherosclerosis and Vascular Risk Factors among People Living with HIV in Ghana. J. Neurol. Sci. 2019, 397, 103–111. [Google Scholar] [CrossRef]
- Chikwati, R.P.; Jaff, N.G.; Mahyoodeen, N.G.; Micklesfield, L.K.; Ramsay, M.; Gómez-Olivé, F.X.; Mohamed, S.F.; Choma, S.S.R.; George, J.A.; Crowther, N.J. The Association of Menopause with Cardiometabolic Disease Risk Factors in Women Living with and without HIV in Sub-Saharan Africa: Results from the AWI-Gen 1 Study. Maturitas 2024, 187, 108069. [Google Scholar] [CrossRef] [PubMed]
- Vos, A.G.; Hoeve, K.; Barth, R.E.; Peper, J.; Moorhouse, M.; Crowther, N.J.; Venter, W.D.F.; Grobbee, D.E.; Bots, M.L.; Klipstein-Grobusch, K. Cardiovascular Disease Risk in an Urban African Population: A Cross-Sectional Analysis on the Role of HIV and Antiretroviral Treatment. Retrovirology 2019, 16, 37. [Google Scholar] [CrossRef]
- Gleason, R.L.; Caulk, A.W.; Seifu, D.; Parker, I.; Vidakovic, B.; Getenet, H.; Assefa, G.; Amogne, W. Current Efavirenz (EFV) or Ritonavir-Boosted Lopinavir (LPV/r) Use Correlates with Elevate Markers of Atherosclerosis in HIV-Infected Subjects in Addis Ababa, Ethiopia. PLoS ONE 2015, 10, e0117125. [Google Scholar] [CrossRef]
- Brand, M.; Woodiwiss, A.J.; Michel, F.; Booysen, H.L.; Majane, O.H.I.; Maseko, M.J.; Veller, M.G.; Norton, G.R. Carotid Intima-Media Thickness in African Patients with Critical Lower Limb Ischemia Infected with the Human Immunodeficiency Virus. J. AIDS Clin. Res. 2012, 3, 1000167. [Google Scholar] [CrossRef]
- Pirs, M.; Eržen, B.; Šabović, M.; Karner, P.; Vidmar, L.; Poljak, M.; Jug, B.; Mikac, M.; Tomažič, J. Early Atherosclerosis in HIV-Infected Patients below the Age of 55 Years: Slovenian National Study. Wien. Klin. Wochenschr. 2014, 126, 263–269. [Google Scholar] [CrossRef]
- Calza, L.; Verucchi, G.; Pocaterra, D.; Pavoni, M.; Alfieri, A.; Cicognani, A.; Manfredi, R.; Serra, C.; Chiodo, F. Cardiovascular Risk Factors and Ultrasound Evaluation of Carotid Atherosclerosis in Patients with HIV-1 Infection. Int. J. STD AIDS 2009, 20, 683–689. [Google Scholar] [CrossRef]
- Parrinello, C.M.; Sinclair, E.; Landay, A.L.; Lurain, N.; Sharrett, A.R.; Gange, S.J.; Xue, X.; Hunt, P.W.; Deeks, S.G.; Hodis, H.N.; et al. Cytomegalovirus Immunoglobulin G Antibody Is Associated with Subclinical Carotid Artery Disease among HIV-Infected Women. J. Infect. Dis. 2012, 205, 1788–1796. [Google Scholar] [CrossRef] [PubMed]
- Vohra, S.; Bharti, V.; Sharma, A.; Jaret, P.K.; Marwaha, R.; Balraj; Sachdeva, A. Comparison of CIMT among HIV Seropositive and HIV Seronegative Subjects: A Case-Control Study. Int. J. Curr. Adv. Res. 2017, 6, 6442–6447. [Google Scholar] [CrossRef]
- Seminari, E.; Pan, A.; Voltini, G.; Carnevale, G.; Maserati, R.; Minoli, L.; Meneghetti, G.; Tinelli, C.; Testa, S. Assessment of Atherosclerosis Using Carotid Ultrasonography in a Cohort of HIV-Positive Patients Treated with Protease Inhibitors. Atherosclerosis 2002, 162, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, R. HIV Disease, Antiretroviral Therapy Safety and the Cardiovascular System. Clinical-Instrumental Assessment of Antiretroviral-Naïve Versus Subjects Already Treated with Antiretroviral Agents. Open Drug Saf. J. 2011, 2, 1–8. [Google Scholar] [CrossRef]
- Gupta, P.K.; Gupta, M.; Lal, A.K.; Taneja, A.; Taneja, R.S.; Rewari, B.B. Markers of Subclinical Atherosclerotic Disease in HIV-Infected Individuals. J. Virus Erad. 2018, 4, 21–25. [Google Scholar] [CrossRef]
- Joseph, J.; Boban, S.M. Study of Cardiovascular Risks and Carotid Intimal Thickness (CIMT) And The Effect Of Antiretroviral Therapy In The Cardiovascular Profile Among HIV Patients. Int. J. Sci. Res. 2025, 14, 1–3. [Google Scholar] [CrossRef]
- Ozdemir, S.; Ozdemir, E.; Birlik, B.; Demirdal, T. The Value of Carotid Intima-Media Thickness in the Detection of Atherosclerosis in HIV+ Patients Subclinical Atherosclerosis in HIV+. J. Coll. Physicians Surg. Pak. 2021, 31, 759–764. [Google Scholar] [CrossRef]
- Li, J.Z.; Segal, F.P.; Bosch, R.J.; Lalama, C.M.; Roberts-Toler, C.; Delagreverie, H.; Getz, R.; Garcia-Broncano, P.; Kinslow, J.; Tressler, R.; et al. Antiretroviral Therapy Reduces T-Cell Activation and Immune Exhaustion Markers in Human Immunodeficiency Virus Controllers. Clin. Infect. Dis. 2020, 70, 1636–1642. [Google Scholar] [CrossRef]
- Strauss, K.-L.E.; Phoswa, W.N.; Mokgalaboni, K. The Impact of Antiretroviral Therapy on Liver Function Among 2 HIV Infected Pregnant Women with and Without Pre-Eclampsia. Viruses 2024, 17, 28. [Google Scholar] [CrossRef] [PubMed]
- Obare, L.M.; Temu, T.; Mallal, S.A.; Wanjalla, C.N. Inflammation in HIV and Its Impact on Atherosclerotic Cardiovascular Disease. Circ Res 2024, 134, 1515–1545. [Google Scholar] [CrossRef]
- Kearns, A.; Gordon, J.; Burdo, T.H.; Qin, X. HIV-1–Associated Atherosclerosis: Unraveling the Missing Link. J. Am. Coll. Cardiol. 2017, 69, 3084–3098. [Google Scholar] [CrossRef]
- Qu, B.; Qu, T. Causes of Changes in Carotid Intima-Media Thickness: A Literature Review. Cardiovasc. Ultrasound 2015, 13, 46. [Google Scholar] [CrossRef]
- Alfaddagh, A.; Martin, S.S.; Leucker, T.M.; Michos, E.D.; Blaha, M.J.; Lowenstein, C.J.; Jones, S.R.; Toth, P.P. Inflammation and Cardiovascular Disease: From Mechanisms to Therapeutics. Am. J. Prev. Cardiol. 2020, 4, 100130. [Google Scholar] [CrossRef] [PubMed]
- Harshithkumar, R.; Shah, P.; Jadaun, P.; Mukherjee, A. ROS Chronicles in HIV Infection: Genesis of Oxidative Stress, Associated Pathologies, and Therapeutic Strategies. Curr. Issues Mol. Biol. 2024, 46, 8852–8873. [Google Scholar] [CrossRef] [PubMed]
- Nzuza, S.; Zondi, S.; Hurchund, R.; Owira, P.M. Highly Active Antiretroviral Therapy-Associated Metabolic Syndrome and Lipodystrophy: Pathophysiology and Current Therapeutic Interventions. J. Endocrinol. Metab. 2017, 7, 103–116. [Google Scholar] [CrossRef]
- Dirajlal-Fargo, S.; Funderburg, N. HIV and Cardiovascular Disease: The Role of Inflammation. Curr. Opin. HIV AIDS 2022, 17, 286–292. [Google Scholar] [CrossRef]
- Hunt, P.W. Very Early ART and Persistent Inflammation in Treated HIV. Clin. Infect. Dis. 2017, 64, 132–133. [Google Scholar] [CrossRef]
- Di Pino, A.; Defronzo, R.A. Insulin Resistance and Atherosclerosis: Implications for Insulin-Sensitizing Agents. Endocr. Rev. 2019, 40, 1447–1467. [Google Scholar] [CrossRef]
- The RESPOND Study Group. Incidence of Dyslipidemia in People with HIV Who Are Treated with Integrase Inhibitors versus Other Antiretroviral Agents. AIDS 2021, 35, 869–882. [Google Scholar] [CrossRef] [PubMed]
- Dressman, J.; Kincer, J.; Matveev, S.V.; Guo, L.; Greenberg, R.N.; Guerin, T.; Meade, D.; Li, X.-A.; Zhu, W.; Uittenbogaard, A.; et al. HIV Protease Inhibitors Promote Atherosclerotic Lesion Formation Independent of Dyslipidemia by Increasing CD36-Dependent Cholesteryl Ester Accumulation in Macrophages. J. Clin. Investig. 2003, 111, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Velichkovska, M.; Surnar, B.; Nair, M.; Dhar, S.; Toborek, M. Targeted Mitochondrial COQ 10 Delivery Attenuates Antiretroviral-Drug-Induced Senescence of Neural Progenitor Cells. Mol. Pharm. 2019, 16, 724–736. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, F.; Belmonti, S.; Sanfilippo, A.; Borghetti, A.; Iannone, V.; Salvo, P.F.; Fabbiani, M.; Visconti, E.; Giambenedetto, S. Di Factors Associated with Oxidative Stress in Virologically Suppressed People Living with HIV on Long-Term Antiretroviral Therapy. AIDS Res. Ther. 2024, 21, 100. [Google Scholar] [CrossRef]
- Ivanov, A.V.; Valuev-Elliston, V.T.; Ivanova, O.N.; Kochetkov, S.N.; Starodubova, E.S.; Bartosch, B.; Isaguliants, M.G. Oxidative Stress during HIV Infection: Mechanisms and Consequences. Oxid. Med. Cell Longev. 2016, 2016, 8910396. [Google Scholar] [CrossRef]
- Alikhani, A.; Morin, H.; Matte, S.; Alikhani, P.; Tremblay, C.; Durand, M. Association between Lipodystrophy and Length of Exposure to ARTs in Adult HIV-1 Infected Patients in Montreal. BMC Infect. Dis. 2019, 19, 820. [Google Scholar] [CrossRef]
- Buthelezi, L.M.; Munsamy, A.J.; Mashige, K.P. Inflammatory Mechanisms Contributing to Retinal Alterations in HIV Infection and Long-Term ART. S. Afr. J. HIV Med. 2024, 25, 1548. [Google Scholar] [CrossRef]
- Vos, A.G.; Venter, W.D.F. Cardiovascular Toxicity of Contemporary Antiretroviral Therapy. Curr. Opin. HIV AIDS 2021, 16, 286–291. [Google Scholar] [CrossRef]
- Babu, H.; Ambikan, A.T.; Gabriel, E.E.; Akusjärvi, S.S.; Palaniappan, A.N.; Sundaraj, V.; Mupanni, N.R.; Sperk, M.; Cheedarla, N.; Sridhar, R.; et al. Systemic Inflammation and the Increased Risk of Inflamm-Aging and Age-Associated Diseases in People Living with HIV on Long Term Suppressive Antiretroviral Therapy. Front. Immunol. 2019, 10, 1965. [Google Scholar] [CrossRef]
- Wu, T.W.; Hung, C.L.; Liu, C.C.; Wu, Y.J.; Wang, L.Y.; Yeh, H.I. Associations of Cardiovascular Risk Factors with Carotid Intima-Media Thickness in Middle-Age Adults and Elders. J. Atheroscler. Thromb. 2017, 24, 677–686. [Google Scholar] [CrossRef]
- Vickhoff, B. Why Art? The Role of Arts in Arts and Health. Front. Psychol. 2023, 14, 765019. [Google Scholar] [CrossRef] [PubMed]
- Millard, E.; Medlicott, E.; Cardona, J.; Priebe, S.; Carr, C. Preferences for Group Arts Therapies: A Cross-Sectional Survey of Mental Health Patients and the General Population. BMJ Open 2021, 11, e051173. [Google Scholar] [CrossRef] [PubMed]
- González-Cordón, A.; Assoumou, L.; Camafort, M.; Domenech, M.; Guaraldi, G.; Domingo, P.; Rusconi, S.; Raffi, F.; Katlama, C.; Masia, M.; et al. Switching from Boosted PIs to Dolutegravir in HIV-Infected Patients with High Cardiovascular Risk: 48 Week Effects on Subclinical Cardiovascular Disease. J. Antimicrob. Chemother. 2020, 75, 3334–3343. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Authors, Year of Publication | Countries | When the Study Was Conducted | Design | Population Size | Duration Since HIV Diagnosis (Years) | Male. N (%) | Age (Years) Mean ± SD | BMI (kg/m 2) Mean ± SD | CD4 Count Mean and SD | Key Findings | ROB |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Joseph et al., 2025 [61] | India | NR | Comparative cross-sectional | PLHIV on ART (50) PLHIV on ART (50) | NR | NR | NR | NR | NR | No significant difference in CIMT between the groups | Low |
| Chikwati et al., 2024 [50] | Kenya, South Africa | 2013 and 2016 | Cross-sectional | PLHIV on ART (240) ART-naive (61) | NR | ART: 0 (0) ART-naive: 0 (0) | ART: 47.6 ± 5.5 ART-naive: 47.5 ± 6.0 | ART: 26.1 ± 6.3 ART-naive: 30.8 ± 8.3 | NR | Significant decrease in CIMT in ART compared to ART-naive patients | Low |
| Sadiq et al., 2024 [24] | South Africa | 2014 to 2017 | Cross-sectional | ART (29) ART-naive (33) | NR | ART: 17 (48.3) ART-naive: 16 (48.3) | ART: 41.9 ± 10.7 ART-naive: 43.6 ± 13.5 | ART: 27.5 ± 6.4 ART-naive: 26.7 ± 5.2 | 385 ± 255 304 ± 190 | There were no significant differences between the ART-exposed and ART-naive groups | Low |
| Moshomo et al., 2024 [38] | Botswana | 2014 and 2015 | Cross-sectional | ART (68) ART-naive (36) | 9.8 ± 3.2 NR | ART: 33 (48.5) ART-naive: 15 (41.7) | ART: 38.7 ± 4.6 ART-naive: 37.8 ± 5.4 | NR | 540.2 ± 230.8 381.5 ± 236.6 | There was no statistically significant difference in CIMT between the two groups | Low |
| Gupta et al., 2022 [20] | India | 2020 | Cross-sectional | ART (80) ART-naive (40) | NR | NR | ART: 37.09 ± 6.09 ART-naive: 33.85 ± 8.84 | ART: 24.68 ± 3.18 ART-naive: 21.87 ± 2.84 | 357.38 ± 220.34 505.25 ± 268.97 | CIMT was significantly higher in the ART groups than in the ART-naive group | Moderate |
| Castro et al., 2021 [39] | Colombia | 2016 and 2017 | Cross-sectional | ART (31) ART-naive (32) | 6.5 ± 1.9 (78 ± 22.75) a 2.0 ± 0.93 (23.98 ± 11.1) a | ART: 17 (55) ART-naive: 12 (63) | ART: 35.5 ± 9.8 ART-naive e: 30.2 ± 8.7 | ART: 21.9 ± 0.835 ART-naive: 22.8 ± 0.83 | 705 ± 139.25 588.29 ± 274.26 | There were no significant differences in CIMT between groups | Moderate |
| Vos et al., 2020 [21] | South Africa | 2014 to 2017 | Cross-sectional | HIV on ART (690) ART-naive (197) | 70.58 ± 15.47 a (5.88 ± 1.29) 0.0 ± 1.17 | ART: 285 (41.3) ART-naive: 73 (37.1) | ART: 41.2 ± 2.24 ART-naive: 35 ± 2.8 | ART: 22.72 ± 1.21 ART-naive: 22.5 ± 1.27 | 490.98 ± 57.0 399 ± 46.33 | There was a significant increase in CIMT in the ART group compared to the ART-naive group | Low |
| Yacovo et al., 2020 [48] | Spain | 2012 and 2013 | Prospective, longitudinal cohort | ART (31) ART-naive (30) | 19.5 ± 9.26 a (1.63 ± 0.77) 23.1 ± 11.98 a (1.93 ± 0.99) | ART: 26 (83.9) ART-naive: 26 (83.9) | ART: 37.3 ± 7.99 ART-naive: 36.3 ± 9.06 | ART: 24.5 ± 3.1 ART-naive: 24.6 ± 5.64 | 415 ± 216 734 ± 193 | CIMT was lower in ART compared to ART-naive patients | Low |
| Sarfo et al., 2019 [49] | Ghana | NR | Cross-sectional | PLHIV on CART (250) CART-naive (201) | 8.6 ± 4.4 1.3 ± 2.6 | CART: 47 (18.8) CART-naive: 37 (18.4) | ART: 45.7 ± 8.6 CART-naive: 42.9 ± 8.8 | CART: 27.1 ± 5.5 CART-naive: 24.5 ± 5.1 | 641.9 ± 331.5 315.9 ± 271.2 | No significant differences in CIMT among CART, ART-naive patients | Low |
| Vos et al., 2019 [51] | South Africa | 2016 to 2017 | Cross-sectional | HIV on ART (287) ART-naive (104) | 77.59 ± 27.73 a (6.47 ± 2.31) 0 ± 0.0 | ART: 95 (32.6) ART-naive: 39 (37.5) | ART: 41.03 ± 8.03 ART-naive: 33.9 ± 8.4 | ART: 25.62 ± 1.75 ART-naive: 23.6 ± 1.02 | 552.78 ± 112 281 ± 34.83 | Significant increase in CIMT in ART compared to ART-naive patients | Low |
| Gupta et al., 2018 [60] | India | 2013 and 2015 | Cross-sectional | PLHIV on ART (124) ART-naive (44) | 4.08 ± 2.58 1.63 ± 1.36 | NR | ART: 32.96 ± 6.72 ART-naive: 33.25 ± 5.77 | ART: 20.66 ± 2.53 ART-naive: 20.66 ± 2.15 | 330 ± 153 339 ± 213 | CIMT was significantly higher in ART compared to ART-naive patients | Low |
| Kirichenko et al., 2018 [40] | Russia | NR | Cross-sectional | ART (25) ART-naive (11) | NR | NR | ART: 39 ± 7 ART-naive: 38 ± 6 | NR | 547 ± 261 460 ± 177 | There was no significant difference in CIMT among the groups | Low |
| Vohra & Bharti, 2017 [57] | India | 2015 to 2016 | Case–control | ART (45) ART-naive (30) | 5.6 ± 3.3 1.9 ± 1.6 | ART: 23 (51.1) ART-naive: 19 (63.3) | ART: 39.2 ± 5.3 ART-naive: 35.5 ± 7.2 | ART: 21.4 ± 3.3 ART-naive: 20.4 ± 4.2 | 443 ± 225 566 ± 207 | CIMT was significantly higher in ART-treated than ART-naive individuals | Low |
| Gleason et al., 2015 [52] | Ethiopia | NR | Cross-sectional | HIV ART (230) ART-naive (51) | 5.98 ± 0.61 1.6 ± 0.85 | ART: 58 (25.2) ART-naive: 14 (27) | ART: 37.78 ± 1.99 ART-naive: 38 ± 3.25 | ART: 22.02 ± 1.39 ART-naive: 22 ± 1.5 | 353.69 ± 63.45 395 ± 51 | There were no significant differences in CIMT between the groups | Low |
| Goulenok et al., 2015 [42] | France | 2008 to 2009 | Cross-sectional | ART (30) ART-naive (29) | 12.0 ± 4.9 6.3 ± 4.9 | ART: 30 (100) ART-naive: 29 (100) | ART: 41.3 ± 5.9 ART-naive: 40.0 ± 7.6 | ART: 23.8 ± 4.5 ART-naive: 23.8 ± 3.3 | 585 ± 136 454 ± 220 | There were no significant differences in CIMT between the groups | Low |
| Fourie et al., 2015 [41] | South Africa | 2005 to 2010 | Observational cohort | PLHIV on ART (66) ART-naive (78) | 5 | ART: 17 (25.8) ART-naive: 27 (34.6) | ART: 48.5 ± 0.96 ART-naive: 48.0 ± 0.89 | ART: 22.3 ± 0.76 ART-naive: 23.8 ± 0.69 | 398 ± 220 335 ± 192 | CIMT did not show a significant difference between the groups | Low |
| Pirs et al., 2014 [54] | Slovenia | NR | Cross-sectional study | PLHIV on ART (60) ART-naive (26) | NR | ART: 60 (100) ART-naive: 26 (100) | ART: 39.3 ± 8.537 ART-naive: 37.9 ± 9.366 | ART: 25.4 ± 3.436 ART-naive: 23.9 ± 2.119 | 269.9 ± 248.814 426.3 ± 199.414 | CIMT increased significantly in ART compared to ART-naive patients | Low |
| Zhu et al., 2014 [43] | China | 2013 | Cross-sectional | PLHIV on HAART (50) HAART-naive (50) | 14.68 ± 3.70 14.93 ± 3.82 | HAART: 26 (52) HAART-naive: 25 (50) | ART: 49.43 ± 5.42 HAART-naive: 48.03 ± 7.81 | ART: 21.57 ± 1.99 HAART-naive: 21.22 ± 1.97 | 413.07 ± 163.610 443.62 ± 213.647 | There were no significant differences in CIMT between the therapy and untreated groups | Low |
| Desvarieux et al., 2013 [45] | USA | 2008 and 2009 | Cross-sectional | ART (50) ART-naive (50) | 12.1 ± 5.2 5.8 ± 4.4 | ART: 50 (100) ART-naive: 50 (100) | ART: 40.2 ± 6.2 ART-naive: 40.4 ± 7.3 | ART: 23.5 ± 3.7 ART-naive: 23.8 ± 3.3 | 592 ± 187 429 ± 162 | CIMT increased significantly in ART compared to ART-naive patients | Low |
| Suparna et al., 2013 [44] | India | NR | Cross-sectional | ART (26) ART-naive (16) | 6.43 ± 4.11 2.2 ± 2.24 | NR | ART: 38.6 ± 7.015 ART-naive: 34.13 ± 6.90 | ART: 20.59 ± 3.2 ART-naive: 20.76 ± 4.2 | 437.62 ± 227.99 387.33 ± 317.9 | There was no significant difference in CIMT between the groups | Moderate |
| Parrinello et al., 2012 [56] | United States of America | 2004 | Observational study | PLHIV on ART (374) ART-naive (227) | NR | ART: 0 (0) ART-naive: 0 (0) | ART: 42.1 ± 8.1 ART-naive: 40.3 ± 8.3 | ART: 28.4 ± 6.9 ART-naive: 29.7 ± 8.3 | 508.04 ± 309.22 464.1 ± 280.3 | CIMT increased significantly in ART compared to ART-naive patients | Low |
| Manfredi et al., 2011 [59] | Italy | 2007 | Cross-sectional | PLHIV on ART (16) ART-naive (11) | 9.5 + 4.3 4.7 + 2.2 | ART: 12 (75) ART-naive: 8 (72.7) | ART: 44 ± 21 ART-naive: 42 ± 18 | ART: 24.4 + 10.8 ART-naive: 23.9 + 11.2 | 635 ± 299 530 ± 211 | There was no significant difference in CIMT between the groups | Low |
| Brand et al., 2011 [53] | South Africa | NR | Cross-sectional | HIV HAART (12) HAART-naive (13) | NR | HAART: 10 (83.3) HAART-naive: 11 (84.6) | HAART: 46 ± 8 HAART-naive: 52 ± 11 | HAART: 23.0 ± 5.0 HAART-naive: 24.5 ± 3.1 | 334 ± 95 316 ± 149 | No significant decrease in CIMT in HAART compared to HAART-naive patients | Low |
| Cristofaro et al., 2011 [46] | Italy | 2004 and 2008 | Cross-sectional | HIV HAART (222) HAART-naive (64) | 9 5 | HAART: 134 (66.7) HAART-naive: 27 (42.2) | HAART: 43.8 ± 7.98 HAART-naive: 35.6 ± 7.26 | NR | 462 ± 342.83 293 ± 270.75 | There was no significant difference in CIMT between the groups | Low |
| Calza et al., 2009 [55] | Italy | 2007 | Cross-sectional study | PLHIV on ART (45) ART-naive (21) | 9.2 + 4.6 4.9 + 2.7 | ART: 38 (84.4) ART-naive: 18 (85.7) | ART: 45 + 26 ART-naive: 43 ± 21 | ART: 24.8 ± 11.2 ART-naive: 23.7 ± 11.5 | 656 ± 315 549 ± 254 | Significantly higher CIMT in ART compared to ART-naive patients | Low |
| Van Vonderen et al., 2009 [47] | Netherlands | 2004 and 2005 | Case–control | ART (55) ART-naive (22) | NR | ART: 55 (100) ART-naive: 22 (100) | ART: 45.30 ± 4.3 ART-naive: 37.73 ± 1.63 | ART: 23.316 ± 0.89 ART-naive: 23.75 ± 1.2 | 609.27 ± 106.9 431.25 ± 76.489 | Significantly higher CIMT in ART compared to ART-naive patients | Low |
| Seminari et al., 2002 [58] | Italy | NR | Cross-sectional | ART (28) ART-naive (15) | NR | ART: 21 (75) ART-naive: 9 (60) | ART: 36 ± 7 ART-naive: 33 ± 5 | ART: 22 ART-naive: 23 | 570 ± 258 534 ± 228 | PI-treated patients had higher CIMT compared to both ART-naive patients | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nieuwoudt, A.; Strauss, K.-L.E.; Phoswa, W.N.; Mokgalaboni, K. The Association Between HIV Infection and Carotid Intima-Media Thickness in the Era of Antiretroviral Therapy: A Meta-Analysis. Viruses 2025, 17, 894. https://doi.org/10.3390/v17070894
Nieuwoudt A, Strauss K-LE, Phoswa WN, Mokgalaboni K. The Association Between HIV Infection and Carotid Intima-Media Thickness in the Era of Antiretroviral Therapy: A Meta-Analysis. Viruses. 2025; 17(7):894. https://doi.org/10.3390/v17070894
Chicago/Turabian StyleNieuwoudt, Angelina, Kay-Lee E. Strauss, Wendy N. Phoswa, and Kabelo Mokgalaboni. 2025. "The Association Between HIV Infection and Carotid Intima-Media Thickness in the Era of Antiretroviral Therapy: A Meta-Analysis" Viruses 17, no. 7: 894. https://doi.org/10.3390/v17070894
APA StyleNieuwoudt, A., Strauss, K.-L. E., Phoswa, W. N., & Mokgalaboni, K. (2025). The Association Between HIV Infection and Carotid Intima-Media Thickness in the Era of Antiretroviral Therapy: A Meta-Analysis. Viruses, 17(7), 894. https://doi.org/10.3390/v17070894