
Genomic Epidemiology of SARS-CoV-2 in Ukraine from May 2022 to March 2024 Reveals Omicron Variant Dynamics

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Genomic Data Acquisition
2.2. Epidemiological Analysis
2.3. VOC Lineage Distribution
2.4. Sequencing
2.5. Phylogenetics
3. Results
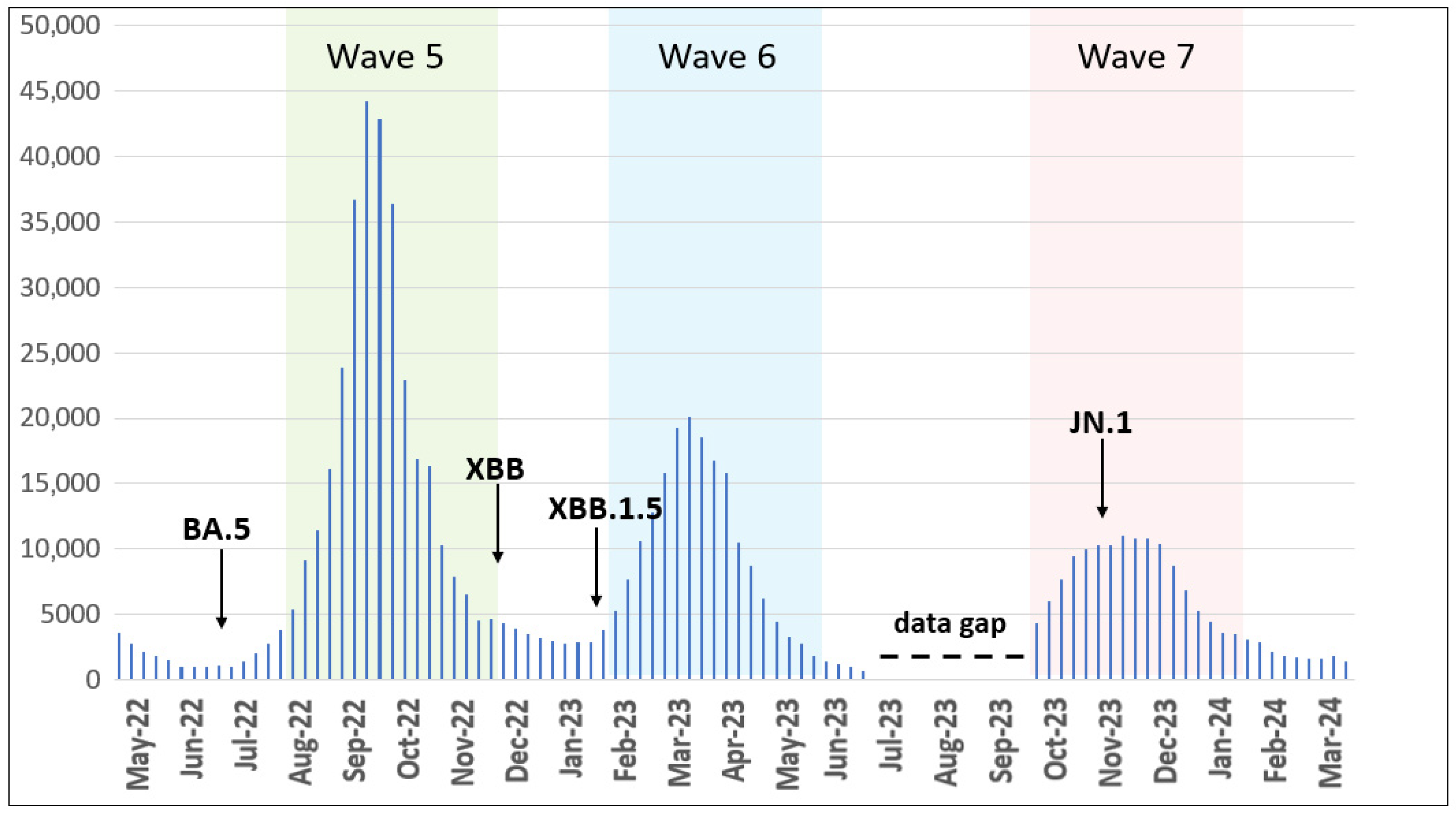
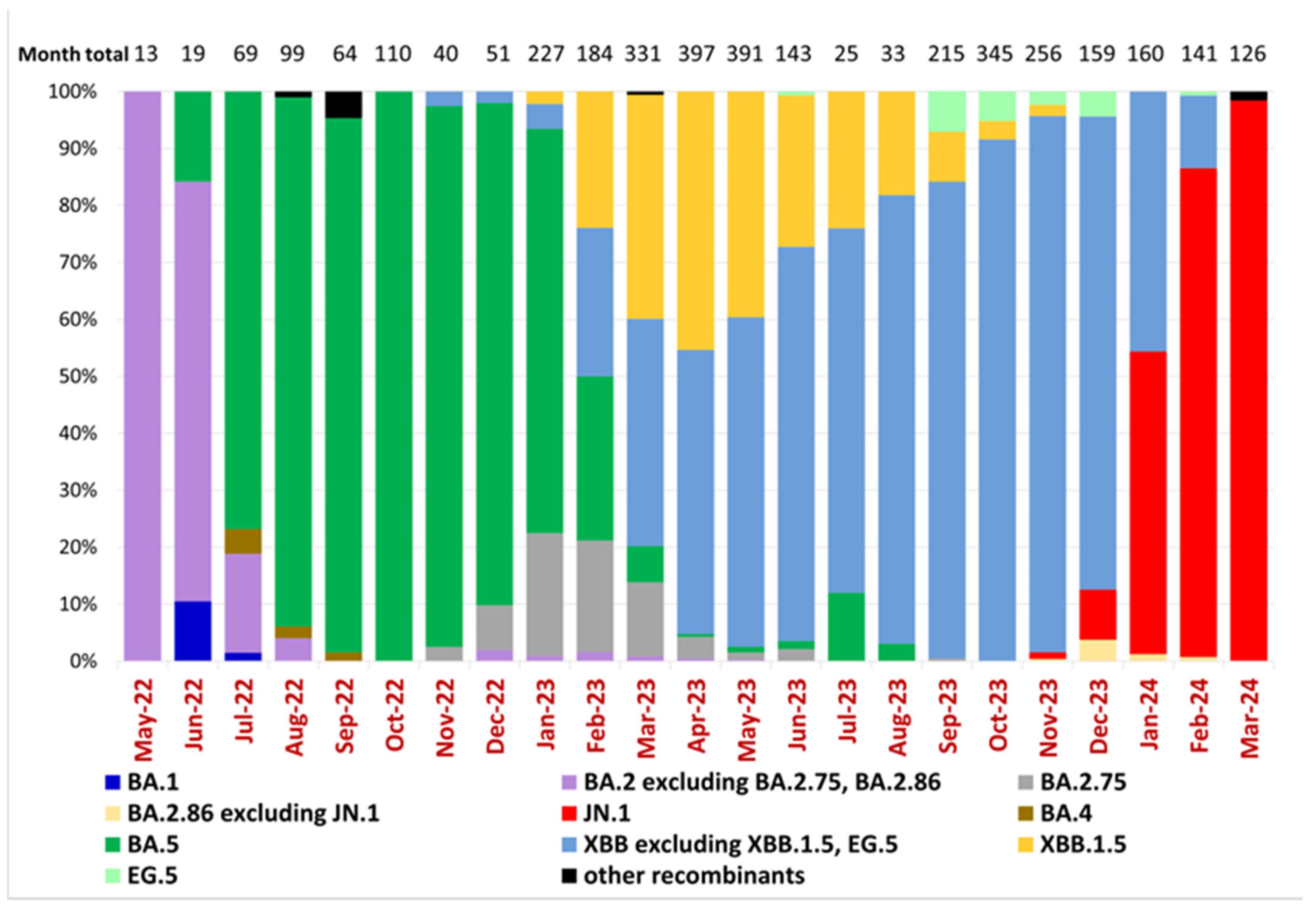
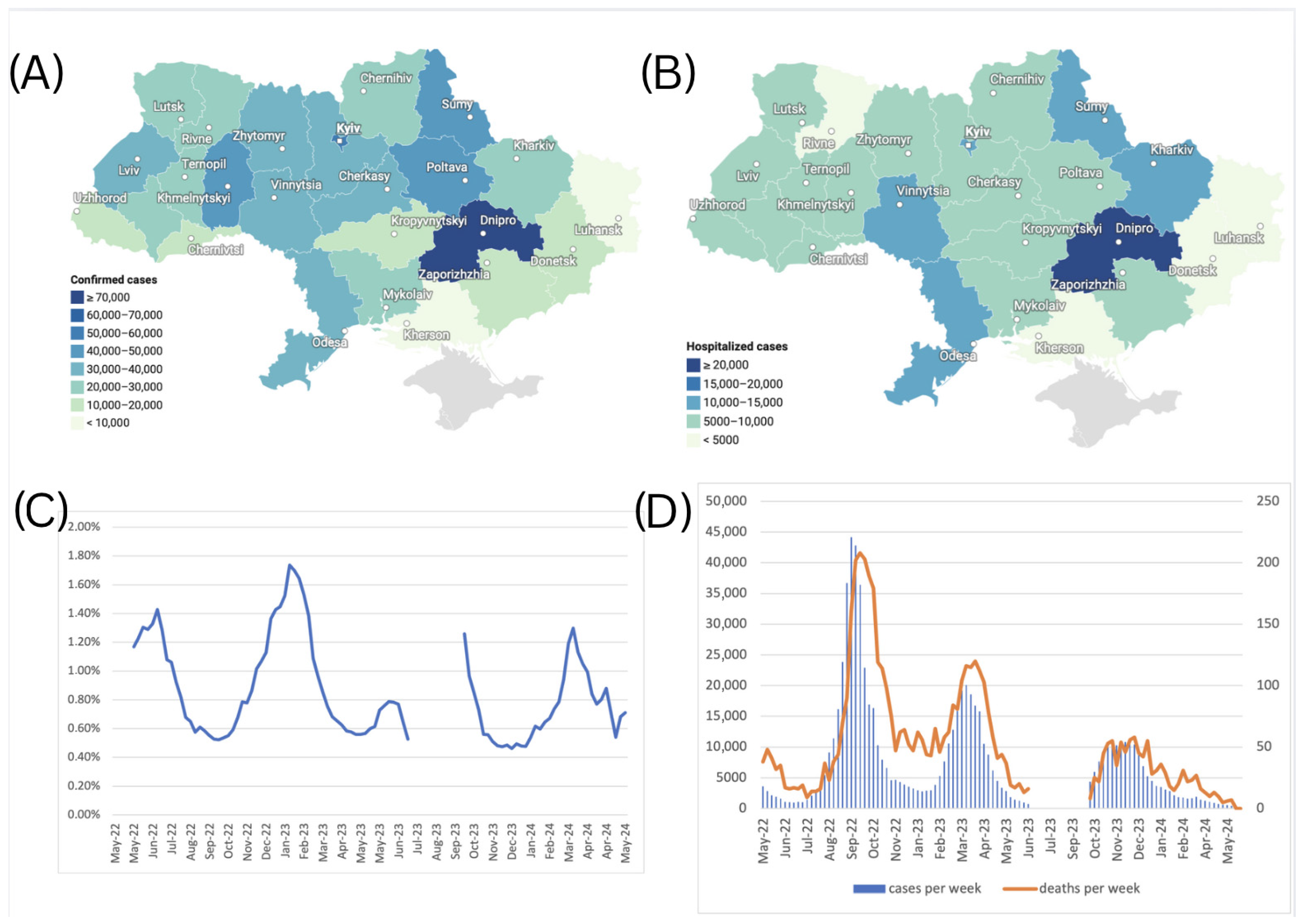
3.1. Dynamics of COVID-19 Cases and SARS-CoV-2 VOCs in Ukraine
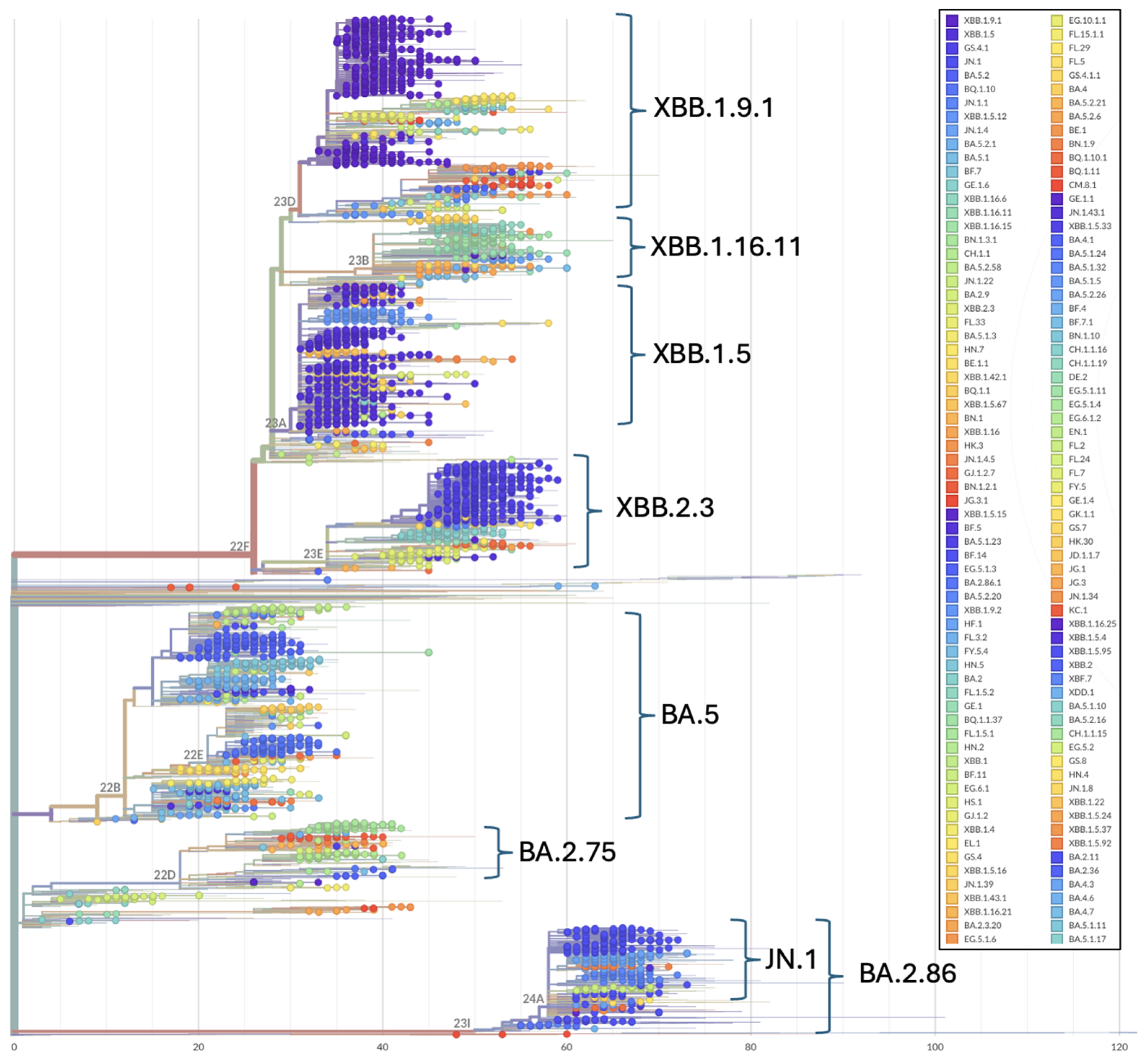
3.2. Evolutionary Relationships of SARS-CoV-2 in Ukraine
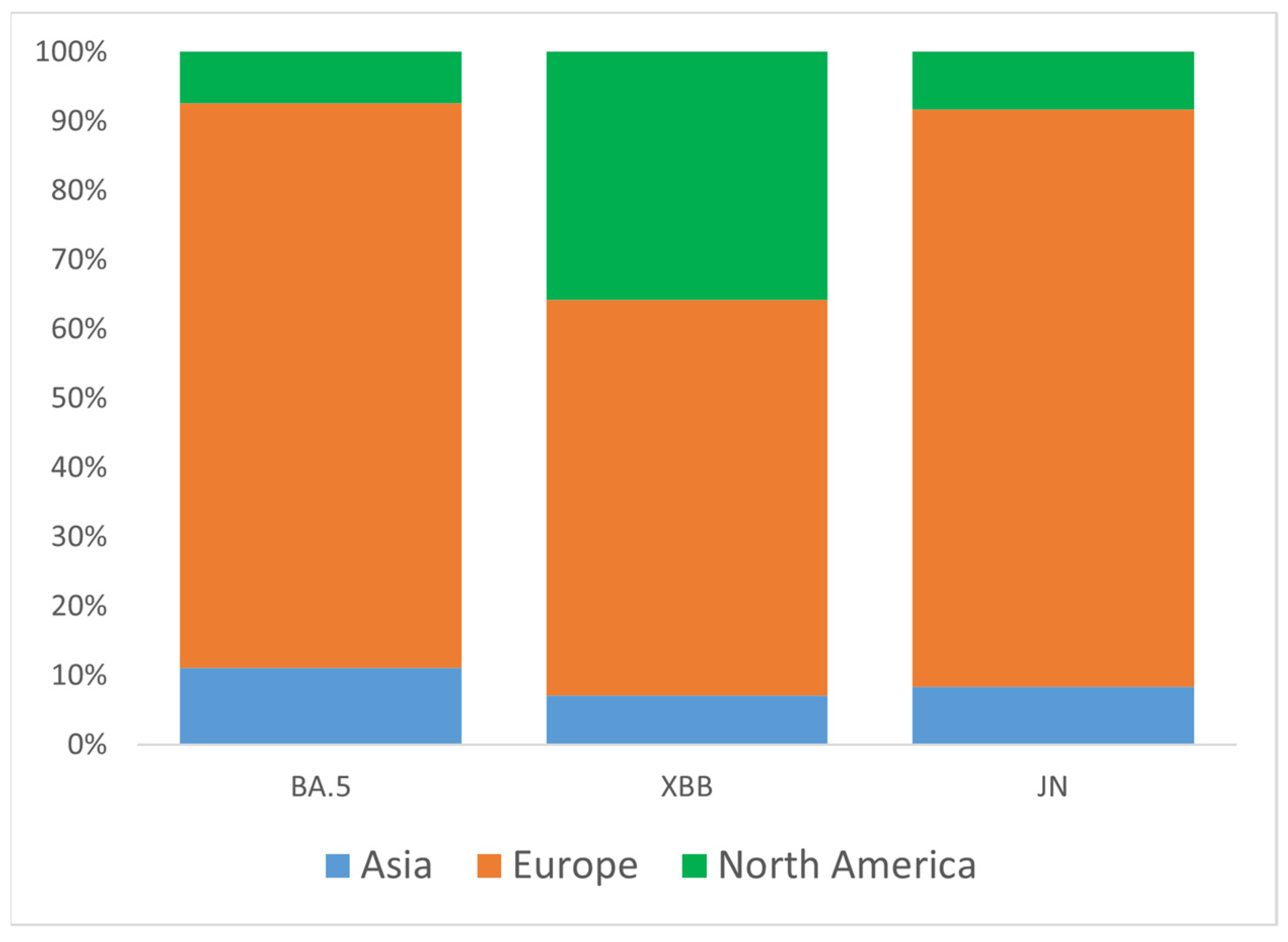
3.3. Introduction of Omicron Variants into Ukraine
3.4. Confirmed COVID-19 Cases by Oblast
3.5. Hospitalization Cases by Oblast
3.6. Case Fatality Rates
3.7. VOCs and Disease Severity
4. Discussion
4.1. Epidemiological Data Collection
4.2. Impact of Russian Invasion During the COVID-19 Pandemic
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFR | Case Fatality Rate |
| COVID-19 | Coronavirus Disease 2019 |
| EIDSS | Electronic Integrated Disease Surveillance System |
| GISAID | Global Initiative on Sharing All Influenza Data |
| HIV/AIDS | Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome |
| HR | Hospitalization Rate |
| NGS | Next Generation Sequencing |
| PANGO | Phylogenetic Assignment of Named Global Outbreak Lineages |
| QC | Quality Control |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| UPHC | Public Health Center of the Ministry of Health of Ukraine |
| VOC | Variant of Concern |
| VOI | Variant of Interest |
| WHO | World Health Organization |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 15 November 2024).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://data.who.int/dashboards/covid19 (accessed on 15 November 2024).
- World Health Organization. Updated Working Definitions and Primary Actions for SARS-CoV-2 Variants (4 October 2023). Available online: https://www.who.int/publications/m/item/updated-working-definitions-and-primary-actions-for--sars-cov-2-variants (accessed on 15 November 2024).
- Lai, A.; Bergna, A.; Della Ventura, C.; Zehender, G. Genomic epidemiology and phylogenetics applied to the study of SARS-CoV-2 pandemic. New Microbiol. 2023, 46, 1–8. [Google Scholar] [PubMed]
- World Health Organization. Genomic Sequencing of SARS-CoV-2: A Guide to Implementation for Maximum Impact on Public Health; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240018440 (accessed on 15 November 2024).
- Maurano, M.T.; Ramaswami, S.; Zappile, P.; Dimartino, D.; Boytard, L.; Ribeiro-Dos-Santos, A.M.; Vulpescu, N.A.; Westby, G.; Shen, G.; Feng, X.; et al. Sequencing identifies multiple early introductions of SARS-CoV-2 to the New York City region. Genome Res. 2020, 30, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Shu, Y.; McCauley, J. GISAID: Global initiative on sharing all influenza data—From vision to reality. Euro. Surveill. 2017, 22, 30494. [Google Scholar] [CrossRef] [PubMed]
- Khare, S.; Gurry, C.; Freitas, L.; Schultz, M.B.; Bach, G.; Diallo, A.; Akite, N.; Ho, J.; Lee, R.T.C.; Yeo, W.; et al. GISAID’s role in pandemic response. China CDC Wkly. 2021, 3, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Hong, V.X.; Lee, J. Clinical outcomes among patients infected with Omicron compared with previous SARS-CoV-2 variants in Southern California. Nat. Med. 2022, 28, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalization and death associated with Omicron (B.1.1.529) and Delta (B.1.617.2) SARS-CoV-2 variants in England. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- World Health Organization. Statement on the Fifteenth Meeting of the IHR. Emergency Committee on the COVID-19 Pandemic. 2005. Available online: https://www.who.int/news (accessed on 15 November 2024).
- Public Health Centre of Ukraine. Confirmed First Case of COVID-19 in Ukraine. Available online: https://phc.org.ua/news/pidtverdzheno-pershiy-vipadok-covid-19-v-ukraini (accessed on 15 November 2024). (In Ukrainian)
- Ministry of Health of Ukraine. Three Years of the Pandemic in Ukraine in Numbers. Available online: https://moz.gov.ua/uk/tri-roki-pandemii-v-ukraini-v-cifrah (accessed on 15 November 2024).
- Yakovleva, A.; Kovalenko, G.; Redlinger, M.; Liulchuk, M.G.; Bortz, E.; Zadorozhna, V.I.; Scherbinska, A.M.; Wertheim, J.O.; Goodfellow, I.; Meredith, L.; et al. Tracking SARS-CoV-2 variants using Nanopore sequencing in Ukraine in 2021. Sci. Rep. 2022, 12, 15749. [Google Scholar] [CrossRef] [PubMed]
- Gerashchenko, G.V.; Hryshchenko, N.V.; Melnichuk, N.S.; Marchyshak, T.V.; Chernushyn, S.Y.; Demchyshina, I.V.; Cher-nenko, L.M.; Kuzin, I.V.; Tkachuk, Z.Y.; Kashuba, V.I.; et al. Genetic characteristics of SARS-CoV-2 virus variants observed upon three waves of the COVID-19 pandemic in Ukraine between February 2021–January 2022. Heliyon 2024, 10, e25618. [Google Scholar] [CrossRef] [PubMed]
- Hadfield, J.; Megill, C.; Bell, S.M.; Huddleston, J.; Potter, B.; Callender, C.; Sagulenko, P.; Bedford, T.; Neher, R.A. Nextstrain: Real-time tracking of pathogen evolution. Bioinformatics 2018, 34, 4121–4123. [Google Scholar] [PubMed]
- Aksamentov, I.; Roemer, C.; Hodcroft, E.B.; Neher, R.A. Nextclade: Clade assignment, mutation calling and quality control for viral genomes. J. Open Source Softw. 2021, 6, 3773. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard—Variants. Available online: https://data.who.int/dashboards/covid19/variants (accessed on 15 November 2024).
- GISAID. Audacity Instant App. Available online: https://gisaid.org/database-features/audacity-instant-app/ (accessed on 29 September 2024).
- Konishi, T. A Comparative Analysis of COVID-19 Response Measures and Their Impact on Mortality Rate. COVID 2024, 4, 130–150. [Google Scholar] [CrossRef]
- Miller, R.R.; Brown, C.S.; Alexander, S.; Coates, T.; Harrison, T.G. Integration of genomic and epidemiological data to inves-tigate COVID-19 outbreaks in closed settings. Microb. Genom. 2023, 9, 001120. [Google Scholar]
- Zhao, H.; Liu, Z.; Chen, Y. Molecular evolution and transmission dynamics of SARS-CoV-2 variants in East Asia. Infect. Genet. Evol. 2025, 119, 105747. [Google Scholar]
- Public Health Centre of Ukraine. COVID-19 Digest: Numbers and Facts. Available online: https://phc.org.ua/promociya-zdorovya/daydzhest-pro-covid-19-cifri-i-fakti (accessed on 15 November 2024). (In Ukrainian).
- World Health Organization. HeRAMS Ukraine Status Update Report: A Comprehensive Mapping of the Operational Status of Health Facilities, March 2024; WHO: Geneva, Switzerland, 2024. [Google Scholar]
- World Health Organization. HeRAMS Ukraine Status Update Report October 2024—Operational Status of the Health System: A Comprehensive Mapping of the Operational Status of Health Facilities; WHO: Geneva, Switzerland, 2024. [Google Scholar]
- International Organization for Migration (IOM). Displacement Tracking Matrix (DTM) Ukraine. Updated 2025. Available online: https://dtm.iom.int/ukraine (accessed on 18 June 2025).
- World Health Organization. Surveillance System for Attacks on Health Care (SSA). Available online: https://extranet.who.int/ssa (accessed on 1 April 2025).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iaruchyk, A.; Farlow, J.; Skrypnyk, A.; Matchyshyn, S.; Kovalchuk, A.; Demchyshyna, I.; Rosada, M.; Aregay, A.K.; Habicht, J. Genomic Epidemiology of SARS-CoV-2 in Ukraine from May 2022 to March 2024 Reveals Omicron Variant Dynamics. Viruses 2025, 17, 1000. https://doi.org/10.3390/v17071000
Iaruchyk A, Farlow J, Skrypnyk A, Matchyshyn S, Kovalchuk A, Demchyshyna I, Rosada M, Aregay AK, Habicht J. Genomic Epidemiology of SARS-CoV-2 in Ukraine from May 2022 to March 2024 Reveals Omicron Variant Dynamics. Viruses. 2025; 17(7):1000. https://doi.org/10.3390/v17071000
Chicago/Turabian StyleIaruchyk, Anna, Jason Farlow, Artem Skrypnyk, Serhii Matchyshyn, Alina Kovalchuk, Iryna Demchyshyna, Mykhailo Rosada, Aron Kassahun Aregay, and Jarno Habicht. 2025. "Genomic Epidemiology of SARS-CoV-2 in Ukraine from May 2022 to March 2024 Reveals Omicron Variant Dynamics" Viruses 17, no. 7: 1000. https://doi.org/10.3390/v17071000
APA StyleIaruchyk, A., Farlow, J., Skrypnyk, A., Matchyshyn, S., Kovalchuk, A., Demchyshyna, I., Rosada, M., Aregay, A. K., & Habicht, J. (2025). Genomic Epidemiology of SARS-CoV-2 in Ukraine from May 2022 to March 2024 Reveals Omicron Variant Dynamics. Viruses, 17(7), 1000. https://doi.org/10.3390/v17071000