
Seroconversion Is Misleading as a Test for HSV-2 Infection in Prophylactic Genital Herpes Vaccine Trials: Results of Vaccine Studies in Guinea Pigs

 , , and
, , and
Abstract
1. Introduction
2. Methods
Seroconversion Assays
3. Statistics
Institutional Animal Care and Use Study Approval
4. Results
4.1. Guinea Pig Studies
4.2. Assays Used to Diagnose Infection
4.3. Assays Used to Detect Seroconversion
4.4. Accuracy of Seroconversion to Detect HSV-2 Genital Infection
4.5. Using Lesions/Latency to Diagnose Infection
4.6. Seroconversion Accuracy Using Lesions/Latency Criteria to Diagnose Infection
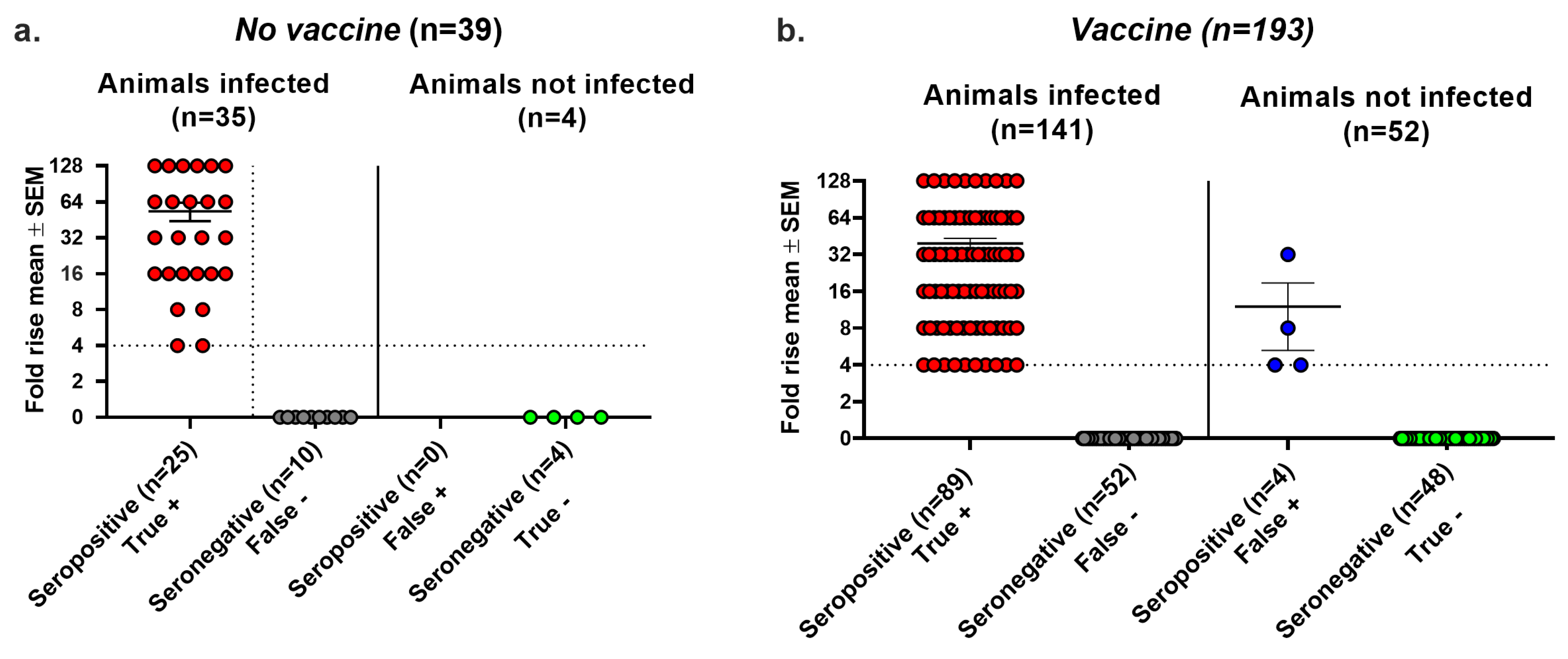
4.7. Seroconversion Accuracy Using Virus Replication to Diagnose Infection
5. Combined Criteria
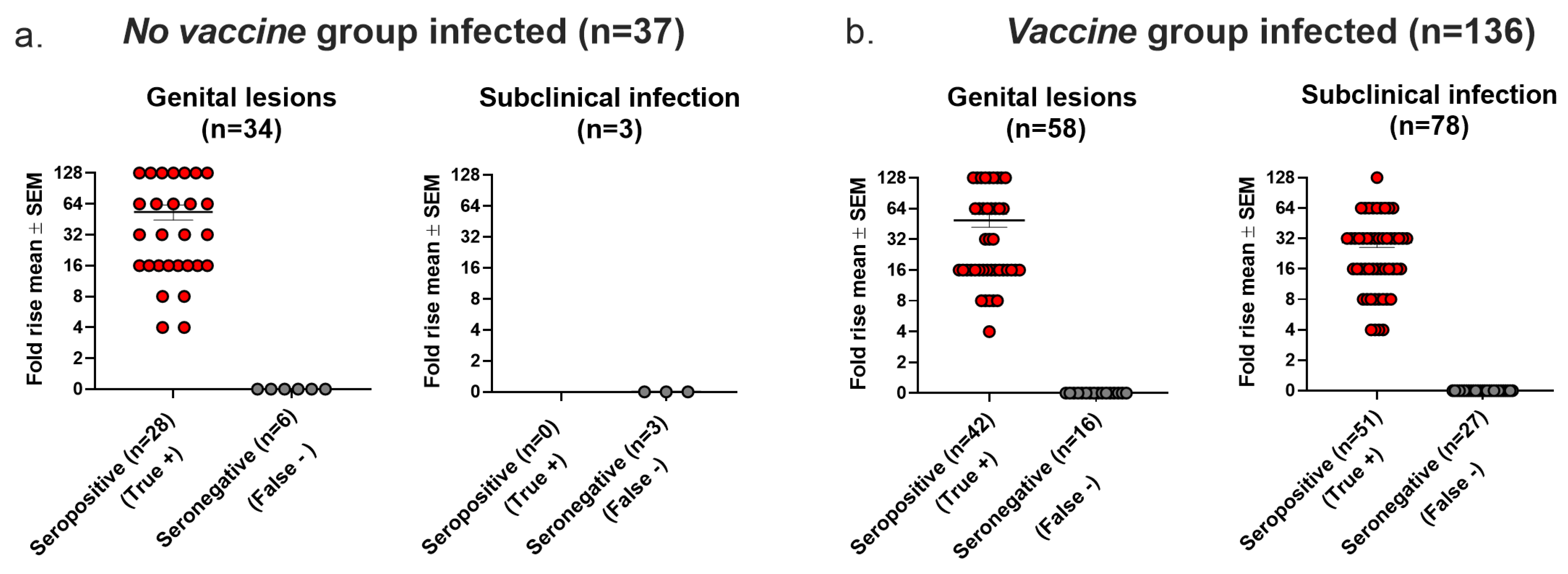
5.1. The Accuracy of Seroconversion as a Confirmatory Test for Genital Lesions or Subclinical (Latent) Infection
5.2. Accuracy of Seroconversion Increases as Vaccine Efficacy Improves
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Corey, L.; Langenberg, A.G.; Ashley, R.; Sekulovich, R.E.; Izu, A.E.; Douglas, J.M., Jr.; Handsfield, H.H.; Warren, T.; Marr, L.; Tyring, S.; et al. Recombinant glycoprotein vaccine for the prevention of genital HSV-2 infection: Two randomized controlled trials. JAMA 1999, 282, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Stanberry, L.R.; Spruance, S.L.; Cunningham, A.L.; Bernstein, D.I.; Mindel, A.; Sacks, S.; Tyring, S.; Aoki, F.Y.; Slaoui, M.; Denis, M.; et al. Glycoprotein-D-adjuvant vaccine to prevent genital herpes. N. Engl. J. Med. 2002, 347, 1652–1661. [Google Scholar] [CrossRef] [PubMed]
- Belshe, R.B.; Leone, P.A.; Bernstein, D.I.; Wald, A.; Levin, M.J.; Stapleton, J.T.; Gorfinkel, I.; Morrow, R.L.; Ewell, M.G.; Stokes-Riner, A.; et al. Efficacy results of a trial of a herpes simplex vaccine. N. Engl. J. Med. 2012, 366, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Mertz, K.J.; Trees, D.; Levine, W.C.; Lewis, J.S.; Litchfield, B.; Pettus, K.S.; Morse, S.A.; St Louis, M.E.; Weiss, J.B.; Schwebke, J.; et al. Etiology of genital ulcers and prevalence of human immunodeficiency virus coinfection in 10 US cities. J. Infect. Dis. 1998, 178, 1795–1798. [Google Scholar] [CrossRef]
- Singh, A.; Preiksaitis, J.; Ferenczy, A.; Romanowski, B. The laboratory diagnosis of herpes simplex virus infections. Can. J. Infect. Dis. Med. Microbiol. 2005, 16, 92–98. [Google Scholar] [CrossRef]
- Workowski, K.A.; Bachmann, L.H.; Chan, P.A.; Johnston, C.M.; Muzny, C.A.; Park, I.; Reno, H.; Zenilman, J.M.; Bolan, G.A. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm. Rep. 2021, 70, 1–187. [Google Scholar]
- Langenberg, A.G.; Corey, L.; Ashley, R.L.; Leong, W.P.; Straus, S.E. A prospective study of new infections with herpes simplex virus type 1 and type 2. N. Engl. J. Med. 1999, 341, 1432–1438. [Google Scholar] [CrossRef]
- Stanberry, L.R.; Kern, E.R.; Richards, J.T.; Abbott, T.M.; Overall, J.C., Jr. Genital herpes in guinea pigs: Pathogenesis of the primary infection and description of recurrent disease. J. Infect. Dis. 1982, 146, 397–404. [Google Scholar] [CrossRef]
- Bernstein, D.I.; Ashley, R.L.; Stanberry, L.R.; Myers, M.G. Detection of asymptomatic initial herpes simplex virus (HSV) infections in animals immunized with subunit HSV glycoprotein vaccines. J. Clin. Microbiol. 1990, 28, 11–15. [Google Scholar] [CrossRef]
- Diaz, F.M.; Knipe, D.M. Protection from genital herpes disease, seroconversion and latent infection in a non-lethal murine genital infection model by immunization with an HSV-2 replication-defective mutant virus. Virology 2016, 488, 61–67. [Google Scholar] [CrossRef]
- McGraw, H.M.; Friedman, H.M. Herpes simplex virus type 1 glycoprotein E mediates retrograde spread from epithelial cells to neurites. J. Virol. 2009, 83, 4791–4799. [Google Scholar] [CrossRef] [PubMed]
- Awasthi, S.; Knox, J.J.; Desmond, A.; Alameh, M.G.; Gaudette, B.T.; Lubinski, J.M.; Naughton, A.; Hook, L.M.; Egan, K.P.; Tam, Y.K.; et al. Trivalent nucleoside-modified mRNA vaccine yields durable memory B cell protection against genital herpes in preclinical models. J. Clin. Investig. 2021, 131, e152310. [Google Scholar] [CrossRef] [PubMed]
- Egan, K.P.; Hook, L.M.; Naughton, A.; Pardi, N.; Awasthi, S.; Cohen, G.H.; Weissman, D.; Friedman, H.M. An HSV-2 nucleoside-modified mRNA genital herpes vaccine containing glycoproteins gC, gD, and gE protects mice against HSV-1 genital lesions and latent infection. PLoS Pathog. 2020, 16, e1008795. [Google Scholar] [CrossRef]
- Awasthi, S.; Lubinski, J.M.; Shaw, C.E.; Barrett, S.M.; Cai, M.; Wang, F.; Betts, M.; Kingsley, S.; Distefano, D.J.; Balliet, J.W.; et al. Immunization with a Vaccine Combining Herpes Simplex Virus 2 (HSV-2) Glycoprotein C (gC) and gD Subunits Improves the Protection of Dorsal Root Ganglia in Mice and Reduces the Frequency of Recurrent Vaginal Shedding of HSV-2 DNA in Guinea Pigs Compared to Immunization with gD Alone. J. Virol. 2011, 85, 10472–10486. [Google Scholar] [PubMed]
- Liljeqvist, J.A.; Trybala, E.; Svennerholm, B.; Jeansson, S.; Sjögren-Jansson, E.; Bergström, T. Localization of type-specific epitopes of herpes simplex virus type 2 glycoprotein G recognized by human and mouse antibodies. J. Gen. Virol. 1998, 79 Pt 5, 1215–1224. [Google Scholar] [CrossRef]
- Awasthi, S.; Onishi, M.; Lubinski, J.M.; Fowler, B.T.; Naughton, A.M.; Hook, L.M.; Egan, K.P.; Hagiwara, M.; Shirai, S.; Sakai, A.; et al. Novel Adjuvant S-540956 Targets Lymph Nodes and Reduces Genital Recurrences and Vaginal Shedding of HSV-2 DNA When Administered with HSV-2 Glycoprotein D as a Therapeutic Vaccine in Guinea Pigs. Viruses 2023, 15, 1148. [Google Scholar] [CrossRef]
- Awasthi, S.; Hook, L.M.; Shaw, C.E.; Pahar, B.; Stagray, J.A.; Liu, D.; Veazey, R.S.; Friedman, H.M. An HSV-2 Trivalent Vaccine Is Immunogenic in Rhesus Macaques and Highly Efficacious in Guinea Pigs. PLoS Pathog. 2017, 13, e1006141. [Google Scholar] [CrossRef]
- Awasthi, S.; Hook, L.M.; Pardi, N.; Wang, F.; Myles, A.; Cancro, M.P.; Cohen, G.H.; Weissman, D.; Friedman, H.M. Nucleoside-modified mRNA encoding HSV-2 glycoproteins C, D, and E prevents clinical and subclinical genital herpes. Sci. Immunol. 2019, 4, eaaw7083. [Google Scholar] [CrossRef]
- US Preventive Services Task Force; Mangione, C.M.; Barry, M.J.; Nicholson, W.K.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Jaén, C.R.; et al. Serologic Screening for Genital Herpes Infection: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA 2023, 329, 502–507. [Google Scholar]
- Crawford, K.H.D.; Selke, S.; Pepper, G.; Goecker, E.; Sobel, A.; Wald, A.; Johnston, C.; Greninger, A.L. Performance characteristics of highly automated HSV-1 and HSV-2 IgG testing. J. Clin. Microbiol. 2024, 62, e0026324. [Google Scholar] [CrossRef]
- Nath, P.; Kabir, M.A.; Doust, S.K.; Ray, A. Diagnosis of Herpes Simplex Virus: Laboratory and Point-of-Care Techniques. Infect. Dis. Rep. 2021, 13, 518–539. [Google Scholar] [CrossRef] [PubMed]
- Ashley, R.L.; Militoni, J.; Lee, F.; Nahmias, A.; Corey, L. Comparison of Western blot (immunoblot) and glycoprotein G-specific immunodot enzyme assay for detecting antibodies to herpes simplex virus types 1 and 2 in human sera. J. Clin. Microbiol. 1988, 26, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Agyemang, E.; Magaret, A.S.; Selke, S.; Johnston, C.; Corey, L.; Wald, A. Herpes Simplex Virus Shedding Rate: Surrogate Outcome for Genital Herpes Recurrence Frequency and Lesion Rates, and Phase 2 Clinical Trials End Point for Evaluating Efficacy of Antivirals. J. Infect. Dis. 2018, 218, 1691–1699. [Google Scholar] [CrossRef]
- Bernstein, D.I.; Flechtner, J.B.; McNeil, L.K.; Heineman, T.; Oliphant, T.; Tasker, S.; Wald, A.; Hetherington, S.; Genocea Study Group. Therapeutic HSV-2 vaccine decreases recurrent virus shedding and recurrent genital herpes disease. Vaccine 2019, 37, 3443–3450. [Google Scholar] [CrossRef]
- McNicholl, J.M.; Leelawiwat, W.; Whitehead, S.; Hanson, D.L.; Evans-Strickfaden, T.; Cheng, C.Y.; Chonwattana, W.; Mueanpai, F.; Kittinunvorakoon, C.; Markowitz, L.; et al. Self-collected genital swabs compared with cervicovaginal lavage for measuring HIV-1 and HSV-2 and the effect of acyclovir on viral shedding. Int. J. STD AIDS 2017, 28, 372–379. [Google Scholar] [CrossRef]
- Graseck, A.S.; Secura, G.M.; Allsworth, J.E.; Madden, T.; Peipert, J.F. Home compared with clinic-based screening for sexually transmitted infections: A randomized controlled trial. Obstet. Gynecol. 2010, 116, 1311–1318. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conditions | No Vaccine (n = 43) | Vaccine (n = 224) |
|---|---|---|
| HSV-2 inoculum | 4 × 105 PFU | 5 × 105 PFU |
| Vaccine and dose | None (n = 43) | gD2 protein, 10 μg (n = 25) gC2/gD2/gE2 proteins, 10 μg each (n = 62) gC2/gD2/gE2 mRNA, 5, 10, or 20 μg each (n = 137) |
| Days scored for genital lesions | ≥41 | ≥41 |
| Days tested for vaginal shedding of HSV-2 DNA after day 28 | ≥20 | ≥20 |
| Interval between acute and convalescent sera | 2 months | 2 months |
| Indicator of Infection | No Vaccine (n = 43) | Vaccine (n = 224) |
|---|---|---|
| Genital lesions | 34 (79%) | 58 (26%) |
| Vaginal shedding HSV-2 DNA | 30 (70%) | 112 (50%) |
| HSV-2 DNA in DRG | 24 (56%) | 40 (18%) |
| Any positive assay (animal considered infected) | 37 (86%) | 136 (61%) |
| All assays negative (animal considered uninfected) | 6 (14%) | 88 (39%) |
| Condition | No Vaccine (n = 8) | Vaccine (n = 10) |
|---|---|---|
| Peak vaginal titers on day 2 or day 4 | Neg 8/8 animals | Neg 10/10 animals |
| Days with genital lesions | 0/160 days | 0/310 days |
| Days with vaginal shedding HSV-2 DNA | ND * | 0/90 days |
| HSV-2 DNA in DRG | ND | 0/10 animals |
| gG2 seroconversion | 0/8 animals | 0/10 animals |
| Seroconversion | No Vaccine | Vaccine | ||||
|---|---|---|---|---|---|---|
| Lesion/Lat. (n = 43) | Replication (n = 39) | Combined (n = 39) | Lesion/Lat. (n = 224) | Replication (n = 193) | Combined (n = 193) | |
| False neg. | 9/37 (24%) | 8/33 (24%) | 10/35 (29%) | 43/136 (32%) | 37/121 (31%) | 52/141 (37%) |
| False pos. | 0/6 (0%) | 0/6 (0%) | 0/4 (0%) | 19/88 (22%) | 9/72 (13%) | 4/52 (8%) |
| Accuracy | 34/43 (79%) | 31/39 (79%) | 29/39 (74%) | 162/224 (72%) | 147/193 (76%) | 137/193 (71%) |
| Vaccine | Infected ^ | Not Infected | Total Protected | Seroconversion Accuracy | ||
|---|---|---|---|---|---|---|
| Seropos (True +) | Seroneg (False −) | Seropos (False +) | Seroneg (True −) | |||
| gD2 (n = 25) | 10 | 10 | 2 | 3 | 5/25 (20%) | 13/25 (52%) |
| Tri-protein (n = 62) | 26 | 15 | 5 | 16 | 21/62 (34%) | 42/62 (68%) |
| Tri-mRNA (n = 137) | 57 | 18 | 12 | 50 | 62/137 (45%) | 107/137 (78%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bromberg, V.; Hook, L.M.; Lubinski, J.M.; Syeda, Z.; Egan, K.P.; Cohen, G.H.; Awasthi, S.; Friedman, H.M. Seroconversion Is Misleading as a Test for HSV-2 Infection in Prophylactic Genital Herpes Vaccine Trials: Results of Vaccine Studies in Guinea Pigs. Viruses 2025, 17, 773. https://doi.org/10.3390/v17060773
Bromberg V, Hook LM, Lubinski JM, Syeda Z, Egan KP, Cohen GH, Awasthi S, Friedman HM. Seroconversion Is Misleading as a Test for HSV-2 Infection in Prophylactic Genital Herpes Vaccine Trials: Results of Vaccine Studies in Guinea Pigs. Viruses. 2025; 17(6):773. https://doi.org/10.3390/v17060773
Chicago/Turabian StyleBromberg, Valerie, Lauren M. Hook, John M. Lubinski, Zauraiz Syeda, Kevin P. Egan, Gary H. Cohen, Sita Awasthi, and Harvey M. Friedman. 2025. "Seroconversion Is Misleading as a Test for HSV-2 Infection in Prophylactic Genital Herpes Vaccine Trials: Results of Vaccine Studies in Guinea Pigs" Viruses 17, no. 6: 773. https://doi.org/10.3390/v17060773
APA StyleBromberg, V., Hook, L. M., Lubinski, J. M., Syeda, Z., Egan, K. P., Cohen, G. H., Awasthi, S., & Friedman, H. M. (2025). Seroconversion Is Misleading as a Test for HSV-2 Infection in Prophylactic Genital Herpes Vaccine Trials: Results of Vaccine Studies in Guinea Pigs. Viruses, 17(6), 773. https://doi.org/10.3390/v17060773