
Comprehensive Diagnosis of Viral Hepatitis in Spain: Bases for Implementation

 , , , , , and
on behalf of Task Force Spanish Group for Comprehensive Hepatitis Diagnosis
, , , , , and
on behalf of Task Force Spanish Group for Comprehensive Hepatitis Diagnosis
Abstract
1. Introduction
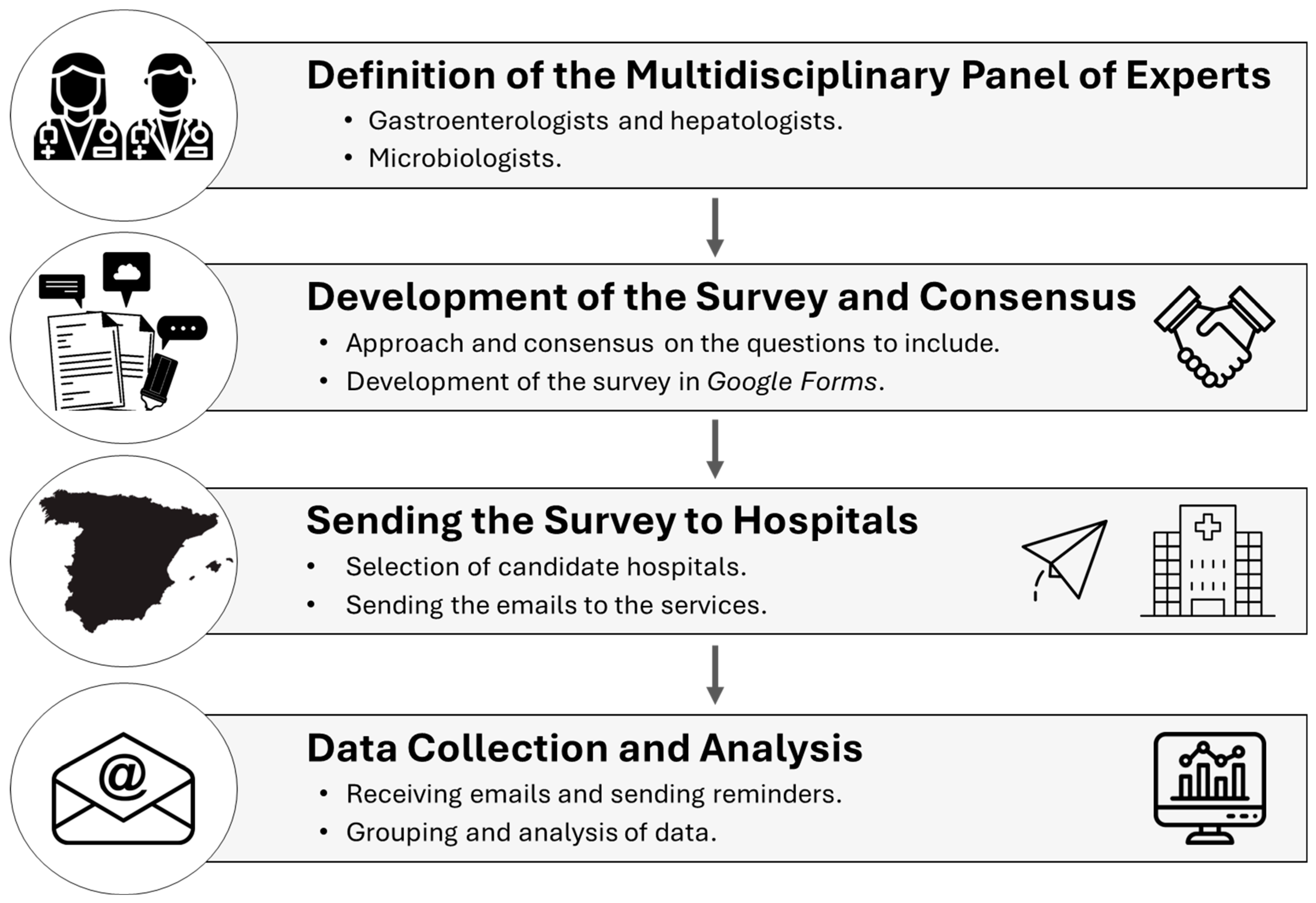
2. Materials and Methods
Survey and Collection Parameters
3. Results
3.1. Respondent and Hospital Center Information
3.2. Reflex Testing of HBV, HCV, and HDV
3.3. POC Testing, Integration of Screening Programs and Continuity of Care
3.4. Comprehensive Diagnosis Needs and Qualitative Information
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AEEH | Spanish Association for the Study of the Liver |
| AEHVE | Alliance for the Elimination of Viral Hepatitis in Spain |
| GEHEP | Study Group of Viral Hepatitis |
| HAV | hepatitis A virus |
| HBV | hepatitis B virus |
| HCV | hepatitis C virus |
| HDV | hepatitis D virus |
| HIV | human immunodeficiency virus |
| NCH | National Catalogue of Hospitals |
| PCR | Polymerase chain reaction |
| POC | Point-of-care |
| SEIMC | Spanish Society of Infectious Diseases and Clinical Microbiology |
| SEPD | Spanish Society of Digestive Pathology |
| STI | sexually transmitted infections |
| WHO | World Health Organization |
References
- World Health Organization. Global Hepatitis Report 2024: Action for Access in Low-and Middle-Income Countries. Available online: https://www.who.int/publications/i/item/9789240091672 (accessed on 8 April 2024).
- Ministerio de Sanidad. Hepatitis Víricas. Available online: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/hepatitis/ciudadanosMenu.htm (accessed on 8 April 2024).
- World Health Organization. Interim Guidance for Country Validation of Viral Hepatitis Elimination. Available online: https://www.who.int/publications-detail-redirect/9789240028395 (accessed on 8 April 2024).
- Sinclair, S.; Shearen, S.; Ghobrial, Y.; Trad, G.; Abdul Basit, S.; Shih, D.; Ryan, J.K. Review of the Effects of Antiviral Therapy on Hepatitis B/C-Related Mortality and the Regression of Fibrosis. Viruses 2024, 16, 1531. [Google Scholar] [CrossRef]
- Roade, L.; Riveiro-Barciela, M.; Esteban, R.; Buti, M. Long-term efficacy and safety of nucleos(t)ides analogues in patients with chronic hepatitis B. Ther. Adv. Infect. Dis. 2021, 8, 204993612098595. [Google Scholar] [CrossRef] [PubMed]
- Crespo, J.; Cabezas, J.; Calleja, J.L.; Buti, M.; Lazarus, J.V. The path to successful hepatitis C elimination in Spain. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 689–690. [Google Scholar] [CrossRef]
- Picchio, C.A.; Lens, S.; Hernandez-Guerra, M.; Arenas, J.; Andrade, R.J.; Crespo, J.; García-Samaniego, J.; Romero-Gómez, M.; Turnes, J.; Calleja, J.L.; et al. Late presentation of chronic HBV and HCV patients seeking first time specialist care in Spain: A 2-year registry review. Sci. Rep. 2021, 11, 24133. [Google Scholar] [CrossRef] [PubMed]
- Miao, Z.; Zhang, S.; Ou, X.; Li, S.; Ma, Z.; Wang, W.; Peppelenbosch, M.P.; Liu, J.; Pan, Q. Estimating the Global Prevalence, Disease Progression, and Clinical Outcome of Hepatitis Delta Virus Infection. J. Infect. Dis. 2020, 221, 1677–1687. [Google Scholar] [CrossRef] [PubMed]
- GeSida. Documento de Consenso de GeSIDA/División de Control de VIH, ITS, Hepatitis Virales y Tuberculosis del Ministerio de Sanidad Respecto al Tratamiento Antirretroviral en Adultos Infectados por el Virus de la Inmunodeficiencia Humana (Actualización enero 2023). Panel de Expertos de GeSIDA y de la División de Control de VIH, ITS, Hepatitis Virales y Tuberculosis del Ministerio de Sanidad. January 2023. Available online: https://gesida-seimc.org/wp-content/uploads/2023/06/Guia_TAR_V12.pdf (accessed on 4 April 2024).
- Ministerio de Sanidad. Enfermedades Transmisibles. Nuevos diagnósticos de infección por VIH en España. Available online: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/queesSidaVih.htm (accessed on 8 April 2024).
- World Health Organization. Global Health Sector Strategies on HIV, Viral Hepatitis and Sexually Transmitted Infections for the Period 2022–2030. Available online: https://www.who.int/publications-detail-redirect/9789240053779 (accessed on 8 April 2024).
- Beard, N.; Hill, A. Combined “Test and Treat” Campaigns for Human Immunodeficiency Virus, Hepatitis B, and Hepatitis C: A Systematic Review to Provide Evidence to Support World Health Organization Treatment Guidelines. Open Forum Infect. Dis. 2024, 11, ofad666. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Documento de Consenso Sobre Diagnóstico y Tratamiento de las Infecciones de Transmisión Sexual en Adultos, Niños y Adolescentes. Marzo de 2017. Grupo de Expertos del Grupo de Estudio de SIDA de la SEIMC (GESIDA), Secretaria del Plan Nacional sobre el SIDA (SPNS), Grupo de Estudio de ITS de la SEIMC (GEITS), Grupo Español para la Investigación de las Enfermedades de Transmisión Sexual de la Academia Española de Dermatología y Venereología, y de la Sociedad Española de Infectología Pediátrica (GEIP). Available online: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/RECOMENDACIONES/ciudadanos.htm (accessed on 13 May 2024).
- Crespo, J.; Cabezas, J.; Aguilera, A.; Berenguer, M.; Buti, M.; Forns, X.; García, F.; García-Samaniego, J.; Hernández-Guerra, M.; Jorquera, F.; et al. Recomendaciones para el diagnóstico integral de las hepatitis virales crónicas en una única extracción analítica. Gastroenterol. Hepatol. 2023, 46, 150–162. [Google Scholar] [CrossRef]
- Crespo, J.; Calleja, J.L.; Cabezas, J.; García, F.; Aguilera, A.; Jorquera, F.; Lazarus, J.V. A call for the comprehensive diagnosis of viral hepatitis as a key step towards its elimination. Liver Int. 2023, 43, 1145–1147. [Google Scholar] [CrossRef]
- Crespo, J.; Lázaro De Mercado, P.; Blasco Bravo, A.J.; Aguilera Guirao, A.; García-Samaniego Rey, J.; Eiros Bouza, J.M.; Luis Calleja Panero, J.; García, F. El diagnóstico de la infección por el virus de la hepatitis C en España: Una oportunidad para mejorar. Enfermedades Infecc. Microbiol. Clínica 2019, 37, 231–238. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Catálogo Nacional de Hospitales 2022. Portal Estadístico del SNS. Búsqueda de Microdatos. Available online: https://www.sanidad.gob.es/estadisticas/microdatos.do (accessed on 20 October 2022).
- Pérez-Latorre, L.; Berenguer, J.; Micán, R.; Montero, M.; Cifuentes, C.; Puig, T.; Sanz, J.; Ferrero, O.L.; De La Fuente, B.; Rodríguez, C.; et al. HIV/HBV coinfection: Temporal trends and patient characteristics, Spain, 2002 to 2018. Euro Surveill 2021, 26, 2000236. [Google Scholar] [CrossRef]
- Cossiga, V.; Brusa, S.; Montalti, R.; De Conte, A.; Jannuzzi, G.; Ranieri, L.; Sorrentino, R.; Vallefuoco, L.; Pignata, L.; Guarino, M.; et al. Anti-HDV reflex testing in HBsAg-positive subjects: An efficacious strategy to identify HDV infection. Liver Int. Off. J. Int. Assoc. Study Liver 2024, 44, 148–154. [Google Scholar] [CrossRef]
- Palom, A.; Rando-Segura, A.; Vico, J.; Pacín, B.; Vargas, E.; Barreira-Díaz, A.; Rodríguez-Frías, F.; Riveiro-Barciela, M.; Esteban, R.; Buti, M. Implementation of anti-HDV reflex testing among HBsAg-positive individuals increases testing for hepatitis D. JHEP Rep. Innov. Hepatol. 2022, 4, 100547. [Google Scholar] [CrossRef]
- Stockdale, A.J.; Kreuels, B.; Henrion, M.Y.R.; Giorgi, E.; Kyomuhangi, I.; de Martel, C.; Hutin, Y.; Geretti, A.M. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J. Hepatol. 2020, 73, 523–532. [Google Scholar] [CrossRef]
- Aguilera, A.; Trastoy, R.; Rodríguez-Calviño, J.; Manso, T.; de Mendoza, C.; Soriano, V. Prevalence and incidence of hepatitis delta in patients with chronic hepatitis B in Spain. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1060–1062. [Google Scholar] [CrossRef]
- Ordieres, C.; Navascués, C.A.; González-Diéguez, M.L.; Rodríguez, M.; Cadahía, V.; Varela, M.; Rodrigo, L.; Rodríguez, M. Prevalence and epidemiology of hepatitis D among patients with chronic hepatitis B virus infection: A report from Northern Spain. Eur. J. Gastroenterol. Hepatol. 2017, 29, 277–283. [Google Scholar] [CrossRef] [PubMed]
- García-Herola, A.; Domínguez-Hernández, R.; Casado, M.Á. Clinical and economic impact of an alert system in primary care for the detection of patients with chronic hepatitis C. PLoS ONE 2021, 16, e0260608. [Google Scholar] [CrossRef]
- Cabezas, J.; Torres-Sangiao, E.; Llerena, S.; Ribes, C.; Gutierrez, C.; Alonso, S.; Echavarria, V.; Antón, Á.; González, A.; Cano, M.E.; et al. The evaluation of people suspected of sexually transmitted diseases requires tools for the comprehensive diagnosis of viral hepatitis and HIV. J. Hepatol. 2023, 78, S911–S912. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Public Health Guidance on HIV, Hepatitis B and C Testing in the EU/EEA: An Integrated Approach; Publications Office: Stockholm, Sweden, 2018; ISBN 978-92-9498-286-5. [Google Scholar]
- World Health Organization. Consolidated Guidelines on HIV, Viral Hepatitis and STI Prevention, Diagnosis, Treatment and Care for Key Populations; World Health Organization: Geneva, Switzerland, 2022; ISBN 978-92-4-005239-0. [Google Scholar]
- Taylor, M.M.; Wi, T.; Gerbase, A.; Thwin, S.S.; Gottlieb, S.; Babovic, M.T.; Low-Beer, D.; Alonso, M.; Mello, M.B.; Ishikawa, N.; et al. Assessment of country implementation of the WHO global health sector strategy on sexually transmitted infections (2016–2021). PLoS ONE 2022, 17, e0263550. [Google Scholar] [CrossRef]
- Matulionytė, R.; Jakobsen, M.L.; Grecu, V.I.; Grigaitiene, J.; Raudonis, T.; Stoniene, L.; Olteanu, M.; de la Mora, L.; Raben, D.; Sullivan, A.K. Increased integrated testing for HIV, hepatitis C and sexually transmitted infections in health care facilities: Results from the INTEGRATE Joint Action pilots in Lithuania, Romania and Spain. BMC Infect. Dis. 2021, 21 (Suppl. 2), 845. [Google Scholar] [CrossRef]
- Coomes, D.; Green, D.; Barnabas, R.; Sharma, M.; Barr-DiChiara, M.; Jamil, M.S.; Baggaley, R.; Owiredu, M.N.; Macdonald, V.; Nguyen, V.T.T.; et al. Cost-effectiveness of implementing HIV and HIV/syphilis dual testing among key populations in Viet Nam: A modelling analysis. BMJ Open 2022, 12, e056887. [Google Scholar] [CrossRef]
- Hutton, D.W.; Toy, M.; Salomon, J.A.; Conners, E.E.; Nelson, N.P.; Harris, A.M.; So, S. Cost-Effectiveness of Hepatitis B Testing and Vaccination of Adults Seeking Care for Sexually Transmitted Infections. Sex. Transm. Dis. 2022, 49, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad. Prevención de la salud. Programa vacunación. Condiciones de Riesgo. B. Vacunaciones en Situaciones de Riesgo. Available online: https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/programasDeVacunacion/riesgo/home.htm (accessed on 15 April 2024).
- Crespo, J.; Lázaro, P.; Blasco, A.J.; Aguilera, A.; García-Samaniego, J.; Eiros, J.M.; Calleja, J.L.; García, F. Diagnóstico en un solo paso de la hepatitis C en 2019: Una realidad en España. Enfermedades Infecc. Microbiol. Clínica 2021, 39, 119–126. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Reflex Testing Type | Systematic Determination of the Same Analytical Sample |
|---|---|
| HBV | Systematic determination of HBV-DNA in the same analytical sample when HBsAg is first detected in the patient. |
| HDV | Systematic determination of antibodies against HDV (anti-HDV) in the same analytical sample when HBsAg is first detected in the patient. |
| Dual HBV-HDV | Systematic determination of HDV antibodies (anti-HDV) when HBsAg is first detected in the patient, together with the systematic determination of HDV-RNA in the same sample in all patients in whom anti-HDV is detected for the first time. |
| HCV | Systematic determination of HCV by PCR in all patients in whom anti-HCV is detected for the first time in the same sample. |
| Variables | Response Alternatives | n | % |
|---|---|---|---|
| Consent to Participate in the Project (n = 129) | |||
| Guest centers | Total | 129 | 100% |
| Consent | No | 50 | 39% |
| Yes | 79 | 61% | |
| |||
| Specialty | Microbiology | 78 | 99% |
| Infectious Diseases | 1 | 1% | |
| Number of hospital beds | Group 2 (200–500 beds) | 27 | 34% |
| Group 3 (501–1000 beds) | 37 | 47% | |
| Group 4 (>1000 beds) | 15 | 19% | |
| Reference population (number of inhabitants) | Minimum | 16,000 | |
| Maximum | 2,000,000 | ||
| University teaching hospital | No | 2 | 3% |
| Yes | 77 | 97% | |
| |||
| Determinations of anti-HDV in the center | No | 29 | 37% |
| Yes | 50 | 63% | |
| HDV-RNA determination in the center | No | 57 | 72% |
| No, because it is outsourced | 53 | 93% | |
| No, it is not outsourced either | 4 | 7% | |
| Yes | 22 | 28% | |
| |||
| Reflex testing is performed | No | 8 | 10% |
| Yes | 71 | 90% | |
| Type of reflex testing (n = 71) | HCV | 70 | 99% |
| HBV | 50 | 70% | |
| HDV | 34 | 48% | |
| Dual HBV-HDV | 31 | 44% | |
| |||
| Hepatitis A | |||
| In patients with chronic hepatitis B, the level of anti-HAV IgG or total IgG was determined | No | 59 | 75% |
| Yes | 20 | 25% | |
| In the same sample | 15 | 75% | |
| In another sample | 5 | 25% | |
| In patients with chronic hepatitis C, anti-HAV IgG or total IgG is determined | No | 53 | 67% |
| Yes | 16 | 20% | |
| In the same sample | 12 | 75% | |
| In another sample | 4 | 25% | |
| Human Immunodeficiency Virus (HIV) | |||
| In patients with chronic hepatitis B, anti-HIV is determined | No | 53 | 67% |
| Yes | 26 | 33% | |
| In the same sample | 19 | 73% | |
| In another sample | 7 | 27% | |
| In patients with chronic hepatitis C, anti-HIV is determined | No | 49 | 62% |
| Yes | 30 | 38% | |
| In the same sample | 19 | 63% | |
| In another sample | 11 | 37% | |
| |||
| Point-of-Care (POC) tests | No | 60 | 76% |
| Yes | 19 | 24% | |
| Type of tests in the POC (n = 19) | GeneXpert® HCV | 11 | 58% |
| Dried Blood Sample | 9 | 47% | |
| Rapid capillary blood antibody test | 6 | 32% | |
| Oraquick® HCV (capillary blood or saliva) | 1 | 5% | |
| Central Microbiology laboratories monitor POC results (n = 19) | No | 3 | 16% |
| Yes | 16 | 84% | |
| POC results integrated in the clinical history (n = 19) | No | 1 | 5% |
| Yes | 18 | 95% | |
| |||
| Community or regional plan | No | 18 | 23% |
| Yes | 61 | 77% | |
| Systematic screening in addiction centers | No | 23 | 29% |
| Yes | 56 | 71% | |
| Screening in previously treated patients at risk of reinfection | Conventional extraction | 68 | 86% |
| Dried Blood Sample | 18 | 23% | |
| GeneXpert® | 9 | 11% | |
| |||
| The specialist physician is alerted on the existence of active viral hepatitis (alerts for the following types: HBV, HDV, or HCV) | No | 18 | 23% |
| Yes | 61 | 77% | |
| HBV | 30 | 49% | |
| HDV | 19 | 31% | |
| HCV | 61 | 100% | |
| Automated system for scheduling an appointment with a specialist physician for patients with active infection | No | 63 | 80% |
| Yes | 16 | 20% | |
| Yes, alert to appointment management | 15 | 94% | |
| No, alert to appointment management | 1 | 6% | |
| |||
| If HBV+ or HCV+, HAV screening should be performed on the same blood sample | No | 25 | 32% |
| Yes | 54 | 68% | |
| If HBV+ or HCV+, HIV screening should be performed on the same blood sample | No | 7 | 9% |
| Yes | 72 | 91% | |
| If STIs are suspected, a comprehensive screen for viral hepatitis should be performed | No | 3 | 4% |
| Yes | 76 | 96% | |
| Yes, a blood sample must be available | 74 | 99% | |
| No, blood sample should be available | 1 | 1% | |
| If STIs are suspected, HIV screening should be performed | No | 1 | 1% |
| Yes | 78 | 99% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabezas, J.; Aguilera, A.; García, F.; Domínguez-Hernández, R.; Casado-Gómez, A.; Espinoza-Cámac, N.; Casado, M.Á.; Crespo, J., on behalf of Task Force Spanish Group for Comprehensive Hepatitis Diagnosis. Comprehensive Diagnosis of Viral Hepatitis in Spain: Bases for Implementation. Viruses 2025, 17, 667. https://doi.org/10.3390/v17050667
Cabezas J, Aguilera A, García F, Domínguez-Hernández R, Casado-Gómez A, Espinoza-Cámac N, Casado MÁ, Crespo J on behalf of Task Force Spanish Group for Comprehensive Hepatitis Diagnosis. Comprehensive Diagnosis of Viral Hepatitis in Spain: Bases for Implementation. Viruses. 2025; 17(5):667. https://doi.org/10.3390/v17050667
Chicago/Turabian StyleCabezas, Joaquin, Antonio Aguilera, Federico García, Raquel Domínguez-Hernández, Araceli Casado-Gómez, Nataly Espinoza-Cámac, Miguel Ángel Casado, and Javier Crespo on behalf of Task Force Spanish Group for Comprehensive Hepatitis Diagnosis. 2025. "Comprehensive Diagnosis of Viral Hepatitis in Spain: Bases for Implementation" Viruses 17, no. 5: 667. https://doi.org/10.3390/v17050667
APA StyleCabezas, J., Aguilera, A., García, F., Domínguez-Hernández, R., Casado-Gómez, A., Espinoza-Cámac, N., Casado, M. Á., & Crespo, J., on behalf of Task Force Spanish Group for Comprehensive Hepatitis Diagnosis. (2025). Comprehensive Diagnosis of Viral Hepatitis in Spain: Bases for Implementation. Viruses, 17(5), 667. https://doi.org/10.3390/v17050667