
Initial Establishment of Warning Model for Epidemic Intensity of Norovirus GII Associated with Acute Gastroenteritis in Beijing Based on Synthetic Index Method

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Research Method
2.2.1. Surveillance Indicators
2.2.2. Normalized Threshold of Surveillance Indicators
2.2.3. Determination of Synthetic Index Classification
2.2.4. Calculation of Synthetic Index
3. Results and Discussion
3.1. The Result of Normalized Threshold for Surveillance Indicators
3.2. Assigning Weight Coefficients to Monitor Indicators and Calculating Synthetic Index
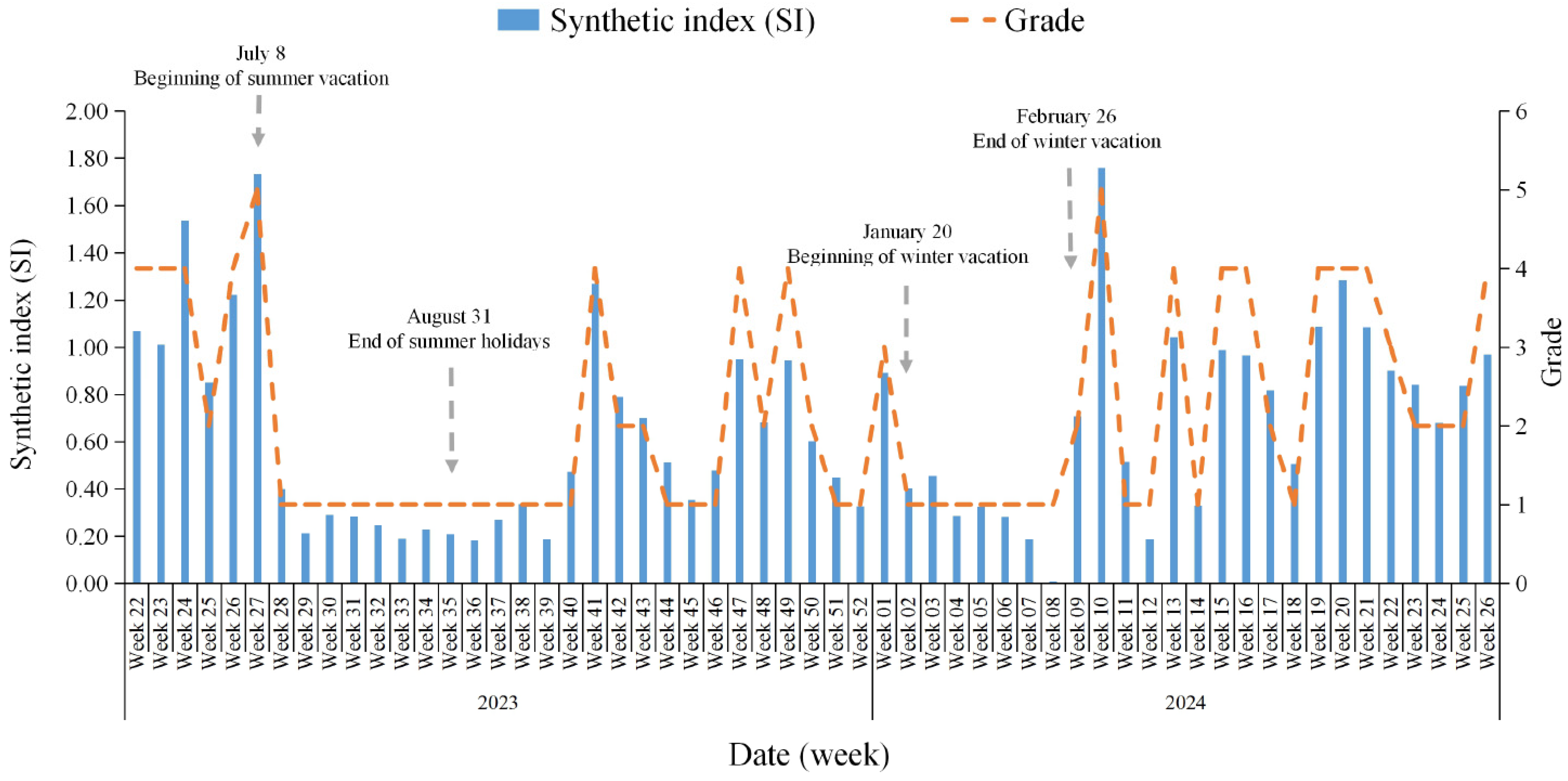
3.3. Epidemic Intensity of Norovirus GII for AGE
3.4. Early Warning Classification of Norovirus GII AGE for the First Time with the Data of Cases and Environmental Surveillance
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lopman, B.A.; Steele, D.; Kirkwood, C.D.; Parashar, U.D. The vast and varied global burden of norovirus: Prospects for prevention and control. PLoS Med. 2016, 13, e1001999. [Google Scholar] [CrossRef]
- Pires, S.M.; Fische-Walker, C.L.; Lanata, C.F.; Devleesschauwer, B.; Hall, A.J.; Kirk, M.D.; Duarte, A.S.R.; Black, R.E.; Angulo, F.J. Aetiology-specific estimates of the global and regional incidence and mortality of diarrhoeal diseases commonly transmitted through food. PLoS ONE 2015, 10, e0142927. [Google Scholar] [CrossRef]
- Hassan, F.; Kanwar, N.; Harrison, C.J.; Halasa, N.B.; Chappell, J.D.; A Englund, J.; Klein, E.J.; A Weinberg, G.; Szilagyi, P.G.; E Moffatt, M.; et al. Viral Etiology of Acute Gastroenteritis in <2-Year-Old US Children in the Post-Rotavirus Vaccine Era. J. Pediatric Infect. Dis. Soc. 2019, 8, 414–421. [Google Scholar] [CrossRef]
- Chhabra, P.; de Graaf, M.; Parra, G.I.; Chan, M.C.-W.; Green, K.; Martella, V.; Wang, Q.; White, P.A.; Katayama, K.; Vennema, H.; et al. Updated classification of norovirus genogroups and genotypes. J. Gen. Virol. 2019, 100, 1393–1406. [Google Scholar] [CrossRef] [PubMed]
- Beck-Friis, T.; Sundell, N.; Gustavsson, L.; Lindh, M.; Westin, J.; Andersson, L.-M. Outdoor Absolute Humidity Predicts the Start of Norovirus GII Epidemics. Microbiol. Spectr. 2023, 11, e0243322. [Google Scholar] [CrossRef]
- Carlson, K.B.; Dilley, A.; O’Grady, T.; Johnson, J.A.; Lopman, B.; Viscidi, E. A narrative review of norovirus epidemiology, biology, and challenges to vaccine development. NPJ Vaccines 2024, 9, 94. [Google Scholar] [CrossRef]
- Anderson, M.S.; Mosby-Tourtellot, C.A.; Cer, R.Z.; Crouch, D.J.; Underwood, R.S.; La Claire, C.S.; Pan, R.W.; Mahugu, E.W.; Smith, H.J.; Bishop-Lilly, K.A.; et al. Molecular Characterization of Noroviruses Causing Acute Gastroenteritis Outbreaks among US Military Recruits, 2013–2023. Emerg. Infect. Dis. 2024, 30, 71–79. [Google Scholar] [CrossRef]
- Yang, S.; Dong, Q.; Li, S.; Cheng, Z.; Kang, X.; Ren, D.; Xu, C.; Zhou, X.; Liang, P.; Sun, L.; et al. Persistence of SARS-CoV-2 RNA in wastewater after the end of the COVID-19 epidemics. J. Hazard. Mater. 2022, 429, 128358. [Google Scholar] [CrossRef]
- Deng, Y.; Xu, X.; Zheng, X.; Ding, J.; Li, S.; Chui, H.-K.; Wong, T.-K.; Poon, L.L.; Zhang, T. Use of sewage surveillance for COVID-19 to guide public health response: A case study in Hong Kong. Sci. Total Environ. 2022, 821, 153250. [Google Scholar] [CrossRef]
- Hrudey, S.E.; Bischel, H.N.; Charrois, J.; Chik, A.H.S.; Conant, B.; Delatolla, R.; Dorner, S.; Graber, T.E.; Hubert, C.; Isaac-Renton, J.; et al. Wastewater Surveillance for SARS-CoV-2 RNA in Canada; The Royal Society of Canada: Ottawa, ON, Canada, 2022; Available online: https://rsc-src.ca/sites/default/files/WWS%20PB_EN_3.pdf (accessed on 1 January 2025).
- International Water Association. COVID-19 Wastewater-Based Epidemiology; IWA: London, UK, 2020; Available online: https://iwa-network.org/learn/covid-19-wastewater-based-epidemiology/ (accessed on 1 January 2025).
- Zhou, S.X.; Zhang, H.Y.; Wang, L.P.; Liu, W.; Fang, L. Exploration of the association between meteorological factors and positive rate of norovirus infectious diarrhea based on the distributed lag non-linear model in Shanghai. Chin. J. Dis. Control Prev. 2021, 25, 1180–1185. [Google Scholar]
- Zhai, M.Y.; Tang, Q.Y.; Li, Y.H.; Ly, L.; Wang, Y.; Shi, X.; Ran, L.; Wang, J. Influence of climatic factors on the outbreaks of acute gastroenteritis caused by norovirus in China. J. Environ. Hyg. 2023, 13, 154–161. [Google Scholar] [CrossRef]
- AbdElGawad, B.; Vega, T.; El Houssinie, M.; Mohsen, A.; Fahim, M.; Abu ElSood, H.; Jabbour, J.; Eid, A.; Refaey, S. Evaluating tools to define influenza baseline and threshold values using surveillance data, Egypt, season 2016/17. J. Infect. Public Heal. 2020, 13, 430–437. [Google Scholar] [CrossRef]
- Vega, T.; Lozano, J.E.; Meerhoff, T.; Snacken, R.; Beauté, J.; Jorgensen, P.; de Lejarazu, R.O.; Domegan, L.; Mossong, J.; Nielsen, J.; et al. Influenza surveillance in Europe: Comparing intensity levels calculated using the moving epidemic method. Influenza Other Respir. Viruses 2015, 9, 234–246. [Google Scholar] [CrossRef]
- Jiao, Y.; Han, T.; Qi, X.; Gao, Y.; Zhao, J.; Zhang, Y.; Li, B.; Zhang, Z.; Du, J.; Sun, L. Genotypes Diversity of Acute Gastroenteritis Outbreaks Caused by Human Sapovirus—Beijing Municipality, China, 2015–2021. China CDC Wkly. 2023, 5, 625–631. [Google Scholar] [CrossRef]
- Chinese Centre for Disease Control and Prevention (CDC). National Viral Diarrhoea Surveillance Programme (2021). [EB/OL]. Available online: https://www.chinacdc.cn/jkyj/crb2/bl/grxfxb/jswj_fxb/202409/P020240907592486658798.pdf (accessed on 18 September 2021).
- Vega, T.; Lozano, J.E.; Meerhoff, T.; Snacken, R.; Mott, J.; Ortiz de Lejarazu, R.; Nunes, B. Influenza surveillance in Europe: Establishing epidemic thresholds by the moving epidemic method. Influenza Other Respir. Viruses 2013, 7, 546–558. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hu, X.; Sun, L.; Han, T.; Zhao, J.; Qi, X.; Zhang, Y.; Lu, P.; Zhao, J.; Gao, Y.; Zhang, Z.; et al. The genetic diversity of genogroup I noroviruses causing acute gastroenteritis outbreaks in Beijing between 2014 and 2023. Heliyon 2024, 10, e39202. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Liu, B.; Yan, H.; Li, W.; Jia, L.; Tian, Y.; Chen, Y.; Wang, Q.; Pang, X. Norovirus outbreaks in Beijing, China, from 2014 to 2017. J. Infect. 2019, 79, 159–166. [Google Scholar] [CrossRef]
- Zhang, L.; Wu, S.S.; Shi, W.X.; Duan, W.; Sun, Y.; Zhang, M.; Zhang, X.X.; Wang, Q.Y.; Yang, P. Establishment of the classified evaluation system on the levels of influenza epidemics through a synthetic index method, in Beijing. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 1096–1099. [Google Scholar]
- O’Brien, E.; Xagoraraki, I. A water-focused one-health approach for early detection and prevention of viral outbreaks. One Health 2019, 7, 100094. [Google Scholar] [CrossRef]
- Sein, C. Evaluating surveillance indicators supporting the global polio eradication initiative, 2011–2012. Morb. Mortal. Wkly. Rep. 2013, 62, 270–274. [Google Scholar]
- Polio Eradication Strategy 2022–2026: Delivering on a Promise. Available online: https://www.who.int/publications/i/item/9789240031937 (accessed on 26 December 2024).
- World Health Organization. WHO Guidelines for Environmental Surveillance for Poliovirus Circulation; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Huang, Y.; Zhou, N.; Zhang, S.; Yi, Y.; Han, Y.; Liu, M.; Han, Y.; Shi, N.; Yang, L.; Wang, Q.; et al. Norovirus detection in wastewater and its correlation with human gastroenteritis: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. Int. 2022, 29, 22829–22842. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, S.; Malla, B.; Haramoto, E. Estimation of Norovirus infections in Japan: An application of wastewater-based epidemiology for enteric disease assessment. Sci. Total Environ. 2024, 912, 169334. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Zhao, K.; Xue, B.; Deng, Y.; Xu, X.; Yan, W.; Rong, C.; Leung, K.; Wu, J.T.; Leung, G.M.; et al. Tracking diarrhea viruses and mpox virus using the wastewater surveillance network in Hong Kong. Water Res. 2024, 255, 121513. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Grade | Thresholds | Epidemic Intensity | Definition | Prevention and Control Suggestions * |
|---|---|---|---|---|
| Class 1 | SI ≤ 0.52 | Non-epidemic risk | The number of reported outbreaks of AGE caused by NoV GII and the positive detection rate of NoV GII in sentinel surveillance are low. The outbreak of AGE caused by NoV GII is less likely to spread. |
|
| Class 2 | 0.52 < SI ≤ 0.87 | General risk | The number of reported outbreaks of AGE caused by NoV GII and the positive detection rate of NoV GII in sentinel surveillance has gradually increased. The outbreak of AGE caused by NoV GII is more likely to occur. | Based on Class 1:
|
| Class 3 | 0.87 < SI ≤ 0.92 | Moderate risk | The number of reported outbreaks of AGE caused by NoV GII and the positive detection rate of NoV GII in sentinel surveillance is high. The outbreak of AGE caused by NoV GII is easy to transmit. | Based on Class 2:
|
| Class 4 | 0.92 < SI ≤ 1.71 | High risk | The number of reported outbreaks of AGE caused by NoV GII and the positive detection rate of NoV GII in sentinel surveillance is higher. The outbreak of AGE caused by NoV GII is greatly vulnerable to transmission. | Based on Class 3:
|
| Class 5 | SI > 1.71 | Ultra-high risk | The number of reported outbreaks of AGE caused by NoV GII and the positive detection rate of NoV GII in sentinel surveillance is quite high. The outbreak of AGE caused by NoV GII is extremely susceptible to transmission and could potentially disrupt school order, lifestyles, production, etc. | Based on Class 4:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, T.; Gao, Y.; Zhang, S.; Jiao, Y.; Zhao, J.; Zhao, J.; Liu, Y.; Liu, K.; Lu, P.; Fan, R.; et al. Initial Establishment of Warning Model for Epidemic Intensity of Norovirus GII Associated with Acute Gastroenteritis in Beijing Based on Synthetic Index Method. Viruses 2025, 17, 473. https://doi.org/10.3390/v17040473
Han T, Gao Y, Zhang S, Jiao Y, Zhao J, Zhao J, Liu Y, Liu K, Lu P, Fan R, et al. Initial Establishment of Warning Model for Epidemic Intensity of Norovirus GII Associated with Acute Gastroenteritis in Beijing Based on Synthetic Index Method. Viruses. 2025; 17(4):473. https://doi.org/10.3390/v17040473
Chicago/Turabian StyleHan, Taoli, Yan Gao, Shiyao Zhang, Yang Jiao, Jianhong Zhao, Jiaxin Zhao, Yujie Liu, Kuankuan Liu, Pan Lu, Ru Fan, and et al. 2025. "Initial Establishment of Warning Model for Epidemic Intensity of Norovirus GII Associated with Acute Gastroenteritis in Beijing Based on Synthetic Index Method" Viruses 17, no. 4: 473. https://doi.org/10.3390/v17040473
APA StyleHan, T., Gao, Y., Zhang, S., Jiao, Y., Zhao, J., Zhao, J., Liu, Y., Liu, K., Lu, P., Fan, R., Zhang, Y., Ren, X., Wang, M., Gao, Z., Li, W., Li, B., Su, T., & Sun, L. (2025). Initial Establishment of Warning Model for Epidemic Intensity of Norovirus GII Associated with Acute Gastroenteritis in Beijing Based on Synthetic Index Method. Viruses, 17(4), 473. https://doi.org/10.3390/v17040473