
Seroprevalence and Epidemiological Insights into Severe Fever with Thrombocytopenia Syndrome on Jeju Island, Republic of Korea
 , ,
, ,  , ,
, ,
Abstract
1. Introduction
1.1. Background
1.2. Objective
2. Materials and Methods
2.1. Study Population and Sample Collection
2.2. Serological Testing and Double-Antigen Enzyme-Linked Immunosorbent Assay (ELISA) Method
2.3. Data Collection and Analysis
2.4. Statistical Analysis
2.5. Ethical Statement
3. Results
3.1. Overall Seroprevalence
3.2. Sex- and Age-Specific Seroprevalence
3.3. Regional Seroprevalence
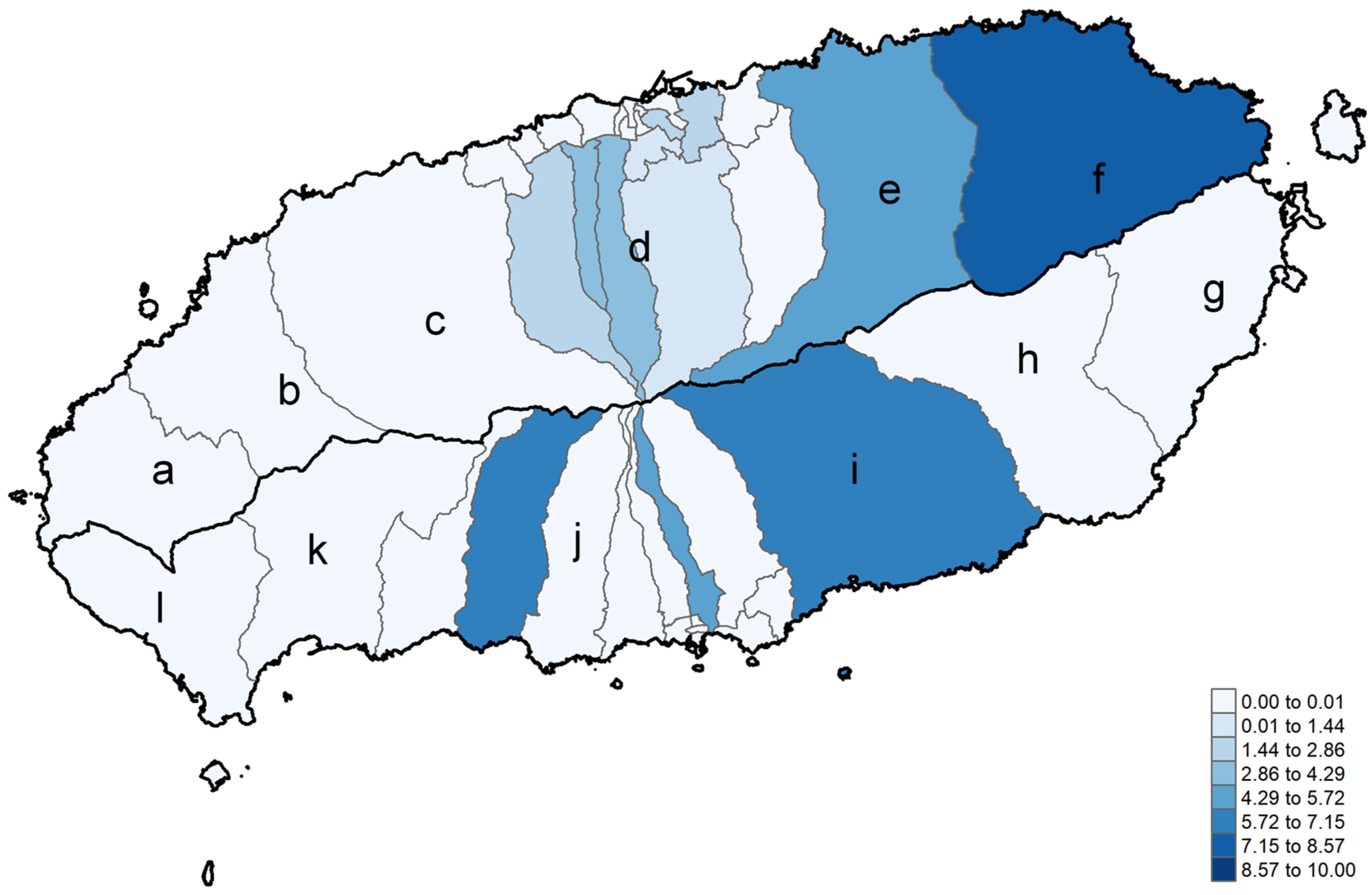
3.4. Seroprevalence by Detailed Administrative Divisions (Eup/Myeon/Dong)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ELISA | Enzyme-linked immunosorbent assay |
| SFTS | Severe Fever with Thrombocytopenia Syndrome |
| SFTSV | SFTS virus |
References
- Yu, X.-J.; Liang, M.-F.; Zhang, S.-Y.; Liu, Y.; Li, J.-D.; Sun, Y.-L.; Zhang, L.; Zhang, Q.-F.; Popov, V.L.; Li, C.; et al. Fever with Thrombocytopenia Associated with a Novel Bunyavirus in China. N. Engl. J. Med. 2011, 364, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Yi, J.; Kim, G.; Choi, S.J.; Jun, K.I.; Kim, N.H.; Choe, P.G.; Kim, N.J.; Lee, J.K.; Oh, M.D. Severe fever with thrombocytopenia syndrome, South Korea, 2012. Emerg. Infect. Dis. 2013, 19, 1892–1894. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Maeda, K.; Suzuki, T.; Ishido, A.; Shigeoka, T.; Tominaga, T.; Kamei, T.; Honda, M.; Ninomiya, D.; Sakai, T.; et al. The first identification and retrospective study of Severe Fever with Thrombocytopenia Syndrome in Japan. J. Infect. Dis. 2014, 209, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.; Shen, S.; Chen, L.; Fan, Z.; Wen, Q.; Xing, Y.; Wang, Z.; Zhang, J.; Chen, J.; La, B.; et al. Global epidemiology of severe fever with thrombocytopenia syndrome virus in human and animals: A systematic review and meta-analysis. Lancet Reg. Health West. Pac. 2024, 48, 101133. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Wang, B.; Li, Y.; Du, Y.; Ma, H.; Li, X.; Guo, W.; Xu, B.; Huang, X. Severe fever with thrombocytopenia syndrome: A systematic review and meta-analysis of epidemiology, clinical signs, routine laboratory diagnosis, risk factors, and outcomes. BMC Infect. Dis. 2020, 20, 575. [Google Scholar] [CrossRef]
- Yoo, J.R.; Heo, S.T.; Song, S.W.; Bae, S.G.; Lee, S.; Choi, S.; Lee, C.; Jeong, S.; Kim, M.; Sa, W.; et al. Severe Fever with Thrombocytopenia Syndrome Virus in Ticks and SFTS Incidence in Humans, South Korea. Emerg. Infect. Dis. 2020, 26, 2292–2294. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.-J.; Hwang, J.H.; Kim, H.S.; Kwon, G.-Y. Epidemiological characteristics of patients with Severe Fever with Thrombocytopenia Syndrome (SFTS) from 2013 to 2020. Public Health Wkly. Rep. 2021, 14, 2561–2572. [Google Scholar]
- Jiao, Y.; Zeng, X.; Guo, X.; Qi, X.; Zhang, X.; Shi, Z.; Zhou, M.; Bao, C.; Zhang, W.; Xu, Y.; et al. Preparation and evaluation of recombinant severe fever with thrombocytopenia syndrome virus nucleocapsid protein for detection of total antibodies in human and animal sera by double-antigen sandwich enzyme-linked immunosorbent assay. J. Clin. Microbiol. 2012, 50, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-H.; Ko, M.K.; Kim, N.; Kim, H.H.; Yi, J. Seroprevalence of Severe Fever with Thrombocytopenia Syndrome in Southeastern Korea, 2015. J. Korean Med. Sci. 2017, 32, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.M.; Han, M.A.; Yun, N.R.; Bang, M.S.; Lee, Y.M.; Lee, B.; Kim, D.M. Seroprevalence of severe fever with thrombocytopenia syndrome using specimens from the Korea National Health & Nutrition Examination Survey. PLoS Negl. Trop. Dis. 2023, 17, e0011097. [Google Scholar] [CrossRef]
- Lyu, Y.; Ding, F.; Sun, J.; Xu, P.P.; Hu, J.Y.; Xie, S.Y.; Li, K.C.; Chang, H.W.; Qin, W.; Yu, L.; et al. Seroprevalence and risk factors of severe fever with thrombocytopenia syndrome virus infection in endemic areas. Infect. Dis. 2016, 48, 544–549. [Google Scholar] [CrossRef]
- Sun, J.M.; Zhang, Y.J.; Gong, Z.Y.; Zhang, L.; Lv, H.K.; Lin, J.F.; Chai, C.L.; Ling, F.; Liu, S.L.; Gu, S.P.; et al. Seroprevalence of severe fever with thrombocytopenia syndrome virus in southeastern China and analysis of risk factors. Epidemiol. Infect. 2015, 143, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Gokuden, M.; Fukushi, S.; Saijo, M.; Nakadouzono, F.; Iwamoto, Y.; Yamamoto, M.; Hozumi, N.; Nakayama, K.; Ishitani, K.; Nishi, N.; et al. Low Seroprevalence of Severe Fever with Thrombocytopenia Syndrome Virus Antibodies in Individuals Living in an Endemic Area in Japan. Jpn. J. Infect. Dis. 2018, 71, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Tong, Z.-D.; Li, K.-F.; Tang, A.; Dai, Y.-X.; Yan, J.-B. Seroprevalence of severe fever with thrombocytopenia syndrome virus in China: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0175592. [Google Scholar] [CrossRef]
- Han, M.A.; Kim, C.M.; Kim, D.M.; Yun, N.R.; Park, S.W.; Han, M.G.; Lee, W.J. Seroprevalence of Severe Fever with Thrombocytopenia Syndrome Virus Antibodies in Rural Areas, South Korea. Emerg. Infect. Dis. 2018, 24, 872–874. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Bao, C.; Zhou, M.; Hu, J.; Tang, F.; Guo, X.; Jiao, Y.; Zhang, W.; Luo, P.; Li, L.; et al. Seroprevalence and risk factors for severe fever with thrombocytopenia syndrome virus infection in Jiangsu Province, China, 2011. Am. J. Trop. Med. Hyg. 2014, 90, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.R.; Heo, S.T.; Kim, M.; Song, S.W.; Boo, J.W.; Lee, K.H. Seroprevalence of Severe Fever with Thrombocytopenia Syndrome in the Agricultural Population of Jeju Island, Korea, 2015–2017. Infect. Chemother. 2019, 51, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.B.; Cui, N.; Hu, J.G.; Chen, W.W.; Xu, W.; Li, H.; Zhang, X.A.; Ly, H.; Liu, W.; Cao, W.C. Characterization of immunological responses in patients with severe fever with thrombocytopenia syndrome: A cohort study in China. Vaccine 2015, 33, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Korea Meteorological Administration. Regional Climate Characteristics: Jeju. Available online: https://www.weather.go.kr/w/climate/statistics/regional-char.do?area=9 (accessed on 27 January 2025).

{kind=link}
| Demographic Group | Total Samples (N) | Positive Samples (N) | Seropositivity Rate (%) | p-Value |
|---|---|---|---|---|
| Sex | ||||
| Male | 466 | 6 | 1.29 | 0.4638 |
| Female | 535 | 11 | 2.06 | |
| Age Group (years) | 0.2358 * | |||
| 10–19 | 1 | 0 | 0.00 | |
| 20–29 | 30 | 0 | 0.00 | |
| 30–39 | 185 | 2 | 1.08 | |
| 40–49 | 411 | 7 | 1.70 | |
| 50–59 | 254 | 5 | 1.97 | |
| ≥60 | 120 | 3 | 2.50 |
| Region | Total Samples (N) | Positive Samples (N) | Seropositivity Rate (%) | p-Value |
|---|---|---|---|---|
| Broad Region | ||||
| Jeju City | 800 | 14 | 1.75 | 0.8489 |
| Seogwipo City | 183 | 3 | 1.64 | |
| Detailed Region | ||||
| Eastern Coastal Area | 68 | 3 | 4.41 | 0.5418 |
| Western Coastal Area | 77 | 0 | 0.00 | |
| Central mid-mountain area | 21 | 0 | 0.00 | |
| Jeju Coastal Area | 692 | 12 | 1.73 | |
| Seogwipo Coastal Area | 125 | 2 | 1.60 |
| Region | Total Samples (N) | Positive Samples (N) | Seropositivity Rate (%) | p-Value |
|---|---|---|---|---|
| Urban (Dong) | 829 | 14 | 1.69 | 0.7395 |
| Rural (Eup/Myeon) | 154 | 3 | 1.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.-H.; Kim, A.; Noh, M.; Kim, C.; Son, H.; Ko, M.K.; Yi, J. Seroprevalence and Epidemiological Insights into Severe Fever with Thrombocytopenia Syndrome on Jeju Island, Republic of Korea. Viruses 2025, 17, 466. https://doi.org/10.3390/v17040466
Kim K-H, Kim A, Noh M, Kim C, Son H, Ko MK, Yi J. Seroprevalence and Epidemiological Insights into Severe Fever with Thrombocytopenia Syndrome on Jeju Island, Republic of Korea. Viruses. 2025; 17(4):466. https://doi.org/10.3390/v17040466
Chicago/Turabian StyleKim, Kye-Hyung, Ahreum Kim, Maengseok Noh, Changhoon Kim, Hyunjin Son, Mee Kyung Ko, and Jongyoun Yi. 2025. "Seroprevalence and Epidemiological Insights into Severe Fever with Thrombocytopenia Syndrome on Jeju Island, Republic of Korea" Viruses 17, no. 4: 466. https://doi.org/10.3390/v17040466
APA StyleKim, K.-H., Kim, A., Noh, M., Kim, C., Son, H., Ko, M. K., & Yi, J. (2025). Seroprevalence and Epidemiological Insights into Severe Fever with Thrombocytopenia Syndrome on Jeju Island, Republic of Korea. Viruses, 17(4), 466. https://doi.org/10.3390/v17040466