

Congenital Oropouche in Humans: Clinical Characterization of a Possible New Teratogenic Syndrome
 , , , , , , , , , , , ,
, , , , , , , , , , , ,  ,
,  , , and add
Show full author list
, , and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
3. Case Reports
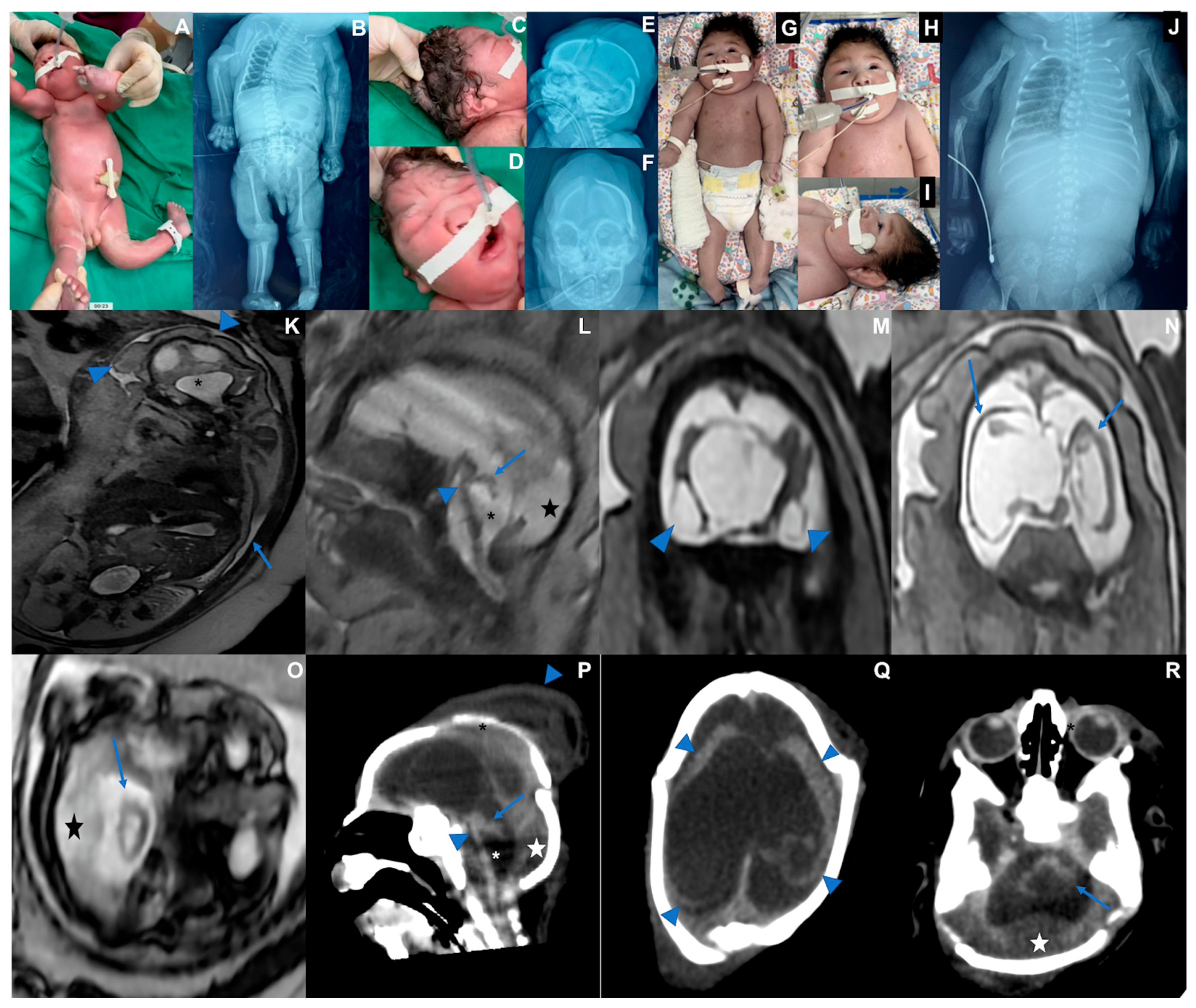
3.1. Case 1 (Figure 1)

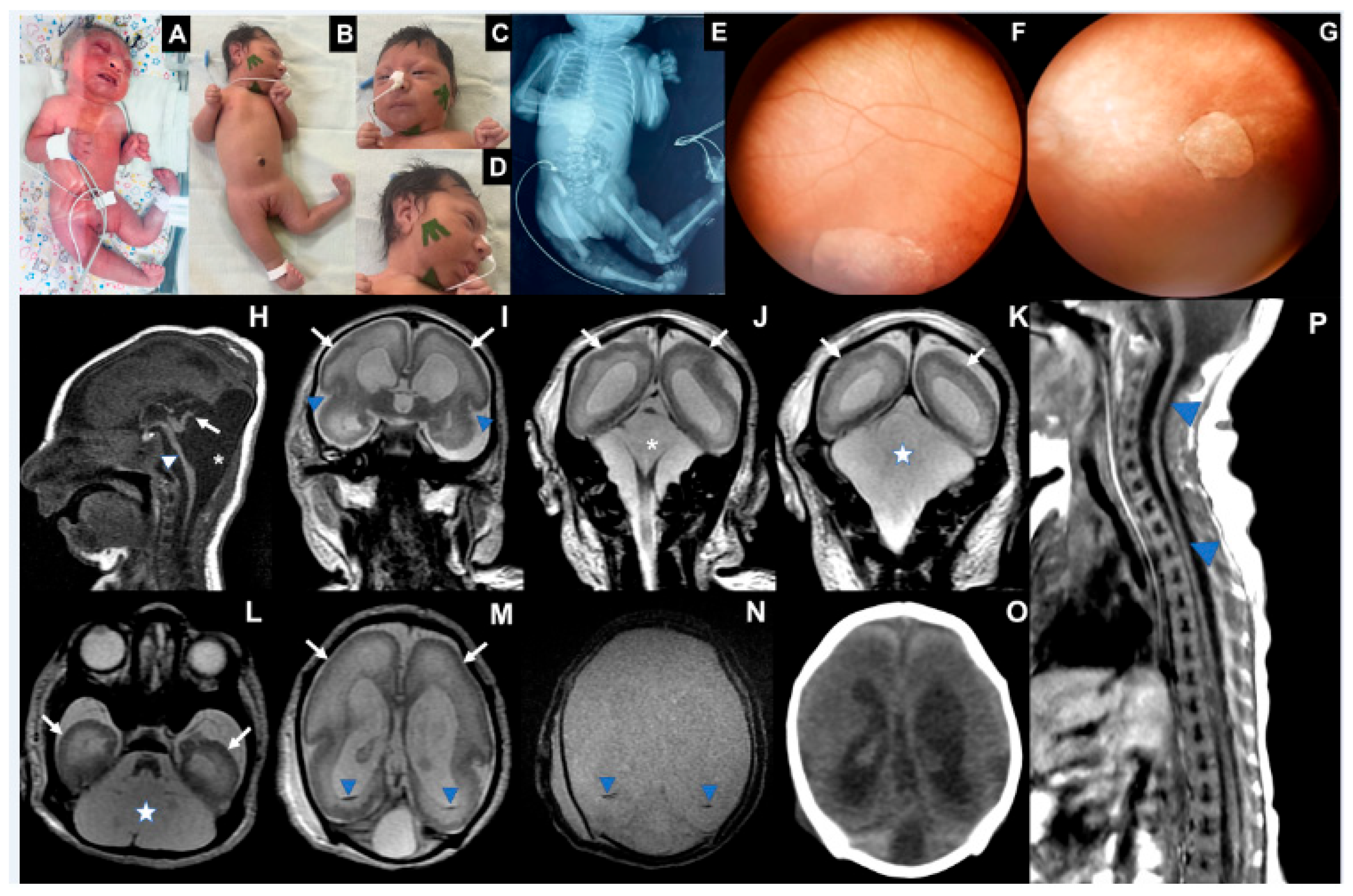
3.2. Case 2 (Figure 2)
3.3. Case 3 (Figure 3)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CLIA | Chemiluminescent immunoassay |
| CHKV | Chikungunya virus |
| CMV | Cytomegalovirus |
| CSF | Cerebrospinal fluid |
| CT scan | Computed tomography scan |
| CT | Cycle Threshold |
| CZS | Congenital Zika syndrome |
| DENV | Dengue virus |
| Det | Detected |
| FBDS | Fetal brain disruption sequence |
| HIV | Human immunodeficiency virus |
| ELISA | Capture immunoenzymatic assay |
| MoH | Brazilian Ministry of Health |
| MRI | Magnetic resonance imaging |
| NA | Not available |
| NDet | Not detected |
| OD | Optical density |
| OROV | Oropouche virus |
| RT-qPCR | Real-time reverse quantitative transcription–polymerase chain reaction |
| Toxo | Toxoplasmosis |
| US | Ultrasound |
| WG | Weeks of gestation |
| ZIKV | Zika virus |
References
- Anderson, C.R.; Spence, L.; Downs, W.G.; Aitken, T.H.G. Oropouche virus: A new human disease agent from Trinidad, West Indies. Am. J. Trop. Med. Hyg. 1961, 10, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, E.d.A.N.; da Silva, A.F.; da Silva, V.G.; Machado, L.C.; de Lima, G.B.; Ishigami, B.I.M.; Silva, K.M.P.e.; Costa, M.M.d.O.M.d.; Falcão, D.A.; Vasconcelos, A.P.; et al. Genomic and phenotypic characterization of the Oropouche virus strain implicated in the 2022–24 large-scale outbreak in Brazil. J. Med. Virol. 2024, 96, e70012. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.O.; Justino, M.C.A.; Matos, H.J.; Cabeça, H.L.S.; Silva, S.P.; Henriques, D.F.; Silva, E.V.P.; Andrade, G.S.S.; Vasconcelos, P.F.; Martins, L.C.; et al. Neurological disease caused by Oropouche virus in northern Brazil: Should it be included in the scope of clinical neurological diseases? J. Neurovirology 2021, 27, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Brazil, Secretaria de Vigilância em Saúde e Ambiente. Recomendação para Intensificação da Vigilância de Transmissão Vertical do Vírus Oropouche. Nota Técnica Nº 15/2024-SVSA/MS. Brasil. Ministério da Saúde. 2024. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/notas-tecnicas/2024/nota-tecnica-no-15-2024-svsa-ms.pdf/view (accessed on 5 August 2024).
- Pan American Health Organization; World Health Organization. Epidemiological Update Oropouche in the Americas Region—6 September 2024; OPS/OMS: Washington, DC, USA, 2024; Available online: https://www.paho.org/en/documents/epidemiological-update-oropouche-americas-region-6-september-2024 (accessed on 9 September 2024).
- Martins, F.E.d.N.; Chiang, J.O.; Nunes, B.T.D.; Ribeiro, B.d.F.R.; Martins, L.C.; Casseb, L.M.N.; Henriques, D.F.; de Oliveira, C.S.; Maciel, E.L.N.; Cravo, L.d.C.C.; et al. Newborns with microcephaly in Brazil and potential vertical transmission of Oropouche virus: A case series. Lancet Infect. Dis. 2024, 25, 155–165. [Google Scholar] [CrossRef]
- Liu, B.M. Epidemiological and clinical overview of the 2024 Oropouche virus disease outbreaks, an emerging/re-emerging neurotropic arboviral disease and global public health threat. J. Med. Virol. 2024, 96, e29897. [Google Scholar] [CrossRef]
- Scachetti, G.C.; Forato, J.; Claro, I.M.; Hua, X.; Salgado, B.B.; Vieira, A.; Simeoni, C.L.; Barbosa, A.R.C.; Rosa, I.L.; de Souza, G.F.; et al. Re-emergence of Oropouche virus between 2023 and 2024 in Brazil: An observational epidemiological study. Lancet Infect. Dis. 2025, 25, 166–175. [Google Scholar] [CrossRef]
- del Campo, M.; Feitosa, I.M.L.; Ribeiro, E.M.; Horovitz, D.D.G.; Pessoa, A.L.S.; França, G.V.A.; García-Alix, A.; Doriqui, M.J.R.; Wanderley, H.Y.C.; Sanseverino, M.V.T.; et al. The phenotypic spectrum of congenital Zika syndrome. Am. J. Med. Genet. Part A 2017, 173, 841–857. [Google Scholar] [CrossRef]
- Moore, C.A.; Weaver, D.D.; Bull, M.J. Fetal brain disruption sequence. J. Pediatr. 1990, 116, 383–386. [Google Scholar] [CrossRef]
- De Rose, D.U.; Gallini, F.; Battaglia, D.I.; Tiberi, E.; Gaudino, S.; Contaldo, I.; Veredice, C.; Romeo, D.M.; Massimi, L.; Asaro, A.; et al. A novel homozygous variant in JAM3 gene causing hemorrhagic destruction of the brain, subependymal calcification, and congenital cataracts (HDBSCC) with neonatal onset. Neurol. Sci. 2021, 42, 4759–4765. [Google Scholar] [CrossRef]
- Doobin, D.J.; Kemal, S.; Dantas, T.J.; Vallee, R.B. Severe NDE1-mediated microcephaly results from neural progenitor cell cycle arrests at multiple specific stages. Nat. Commun. 2016, 7, 12551. [Google Scholar] [CrossRef]
- Thomas, A.X.; Link, N.; Robak, L.A.; Demmler-Harrison, G.; Pao, E.C.; Squire, A.E.; Michels, S.; Cohen, J.S.; Comi, A.; Prontera, P.; et al. ANKLE2-related microcephaly: A variable microcephaly syndrome resembling Zika infection. Ann. Clin. Transl. Neurol. 2022, 9, 1276–1288. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C.V.; Da Fonseca, E.B.; Ribeiro, E.M.; Ventura, L.O.; Neto, N.N.; Arena, J.F.; et al. Characterizing the Pattern of Anomalies in Congenital Zika Syndrome for Pediatric Clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Barreto, A.R.F.; Carrasco, M.; Dabrowski, A.K.; Sun, L.R.; Tekes, A. Subpial Hemorrhage in Neonates: What Radiologists Need to Know. Am. J. Roentgenol. 2021, 216, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.; Jin, K.; Li, J.; Yin, Y.; He, S. Subpial hemorrhages in neonates: Imaging features, clinical factors and outcomes. Sci. Rep. 2023, 13, 3408. [Google Scholar] [CrossRef]
- Wesselmann, K.M.; Postigo-Hidalgo, I.; Pezzi, L.; de Oliveira-Filho, E.F.; Fischer, C.; de Lamballerie, X.; Drexler, J.F. Emergence of Oropouche fever in Latin America: A narrative review. Lancet Infect. Dis. 2024, 24, e439–e452. [Google Scholar] [CrossRef]
- Cramer, J.; Rassner, U.; Hedlund, G. Limitations of T2*–Gradient Recalled-Echo and Susceptibility-Weighted Imaging in Characterizing Chronic Subdural Hemorrhage in Infant Survivors of Abusive Head Trauma. Am. J. Neuroradiol. 2016, 37, 1752–1756. [Google Scholar] [CrossRef]
- van der Linden, H.; Carvalho, M.D.; van der Linden, V.; Lacerda, K.M.; Pessoa, A.; Carneiro, M.L.; Cordeiro, M.T.; Valente, K.D. Epilepsy Profile in Infants with Congenital Zika Virus Infection. N. Engl. J. Med. 2018, 379, 891–892. [Google Scholar] [CrossRef]
- Pessoa, A.; van der Linden, V.; Yeargin-Allsopp, M.; Carvalho, M.D.C.G.; Ribeiro, E.M.; Braun, K.V.N.; Durkin, M.S.; Pastula, D.M.; Moore, J.T.; Moore, C.A. Motor Abnormalities and Epilepsy in Infants and Children with Evidence of Congenital Zika Virus Infection. Pediatrics 2018, 141 (Suppl. S2), S167–S179. [Google Scholar] [CrossRef]
- Leal, M.C.; van der Linden, V.; Bezerra, T.P.; de Valois, L.; Borges, A.C.; Antunes, M.M.; Brandt, K.G.; Moura, C.X.; Rodrigues, L.C.; Ximenes, C.R. Characteristics of Dysphagia in Infants with Microcephaly Caused by Congenital Zika Virus Infection, Brazil, 2015. Emerg. Infect. Dis. 2017, 23, 1253–1259. [Google Scholar] [CrossRef]
- Ventura, C.V.; Zin, A.; Freitas, B.d.P.; Ventura, L.O.; Rocha, C.; Costa, F.; Nery, N.; De Senna, T.C.; Moreira, M.E.L.; Maia, M.; et al. Ophthalmological manifestations in congenital Zika syndrome in 469 Brazilian children. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2021, 25, 158.e1–158.e8. [Google Scholar] [CrossRef]
- Singh, S.; Kumar, A. Ocular Manifestations of Emerging Flaviviruses and the Blood-Retinal Barrier. Viruses 2018, 10, 530, Erratum in Viruses 2019, 11, 475. [Google Scholar] [CrossRef] [PubMed]
- da Hora, L.C.D.; Muniz, L.F.; Venâncio, L.G.A.; Advíncula, K.P.; da Silva, J.D.; Britto, D.B.L.d.A.; Filho, D.d.B.M.; Brickley, E.B.; Ximenes, R.A.d.A.; Neto, S.d.S.C.; et al. Cortical Auditory Evoked Potentials in Children with Prenatal Exposure to Zika Virus. Viruses 2022, 14, 1923. [Google Scholar] [CrossRef] [PubMed]
- De Regge, N.; Berg, T.v.D.; Georges, L.; Cay, B. Diagnosis of Schmallenberg virus infection in malformed lambs and calves and first indications for virus clearance in the fetus. Vet. Microbiol. 2013, 162, 595–600. [Google Scholar] [CrossRef]
- Peperkamp, N.H.; Luttikholt, S.J.; Dijkman, R.; Vos, J.H.; Junker, K.; Greijdanus, S.; Roumen, M.P.; van Garderen, E.; Meertens, N.; van Maanen, C.; et al. Ovine and Bovine Congenital Abnormalities Associated with Intrauterine Infection with Schmallenberg Virus. Vet. Pathol. 2015, 52, 1057–1066. [Google Scholar] [CrossRef]
- Hartley, W.J.; Wanner, R.A.; Della-Porta, A.J.; Snowdon, W.A. Serological evidence for the association of Akabane virus with epizootic bovine congenital arthrogryposis and hydranencephaly syndromes in New South Wales. Aust. Vet. J. 1975, 51, 103–104. [Google Scholar] [CrossRef]
- Agerholm, J.S.; Hewicker-Trautwein, M.; Peperkamp, K.; Windsor, P.A. Virus-induced congenital malformations in cattle. Acta Vet. Scand. 2015, 57, 54. [Google Scholar] [CrossRef]
- Hughes, H.R.; Kenney, J.L.; Calvert, A.E. Cache Valley virus: An emerging arbovirus of public and veterinary health importance. J. Med. Entomol. 2023, 60, 1230–1241. [Google Scholar] [CrossRef]
- Edwards, J.F.; Collisson, E.W.; Bermejillo, A.d.l.C.; Karabatsos, N. Ovine fetal malformations induced by in utero inoculation with Main Drain, San Angelo, and Lacrosse viruses. Am. J. Trop. Med. Hyg. 1997, 56, 171–176. [Google Scholar] [CrossRef]
- Calisher, C.H.; Sever, J.L. Are North American Bunyamwera Serogroup viruses etiologic agents of human congenital defects of the central nervous system? Emerg. Infect. Dis. 1995, 1, 147–151. [Google Scholar] [CrossRef]
- Borborema, C.A.T.; Pinheiro, F.P.; Albuquerque, B.C.; Rosa, A.P.A.T.d.; Dourado, H.V. Primeiro registro de epidemias causadas pelo vírus Oropouche no estado do Amazonas. Rev. Inst. Med. Trop. São Paulo 1982, 24, 132–139. Available online: https://www.revistas.usp.br/rimtsp/article/view/196741 (accessed on 12 December 2024).
- Naveca, F.G.; de Almeida, T.A.P.; Souza, V.; Nascimento, V.; Silva, D.; Nascimento, F.; Mejía, M.; de Oliveira, Y.S.; Rocha, L.; Xavier, N.; et al. Human outbreaks of a novel reassortant Oropouche virus in the Brazilian Amazon region. Nat. Med. 2024, 30, 3509–3521. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A. Novel Reassortants of Oropouche Virus (OROV) Are Causing Maternal–Fetal Infection During Pregnancy, Stillbirth, Congenital Microcephaly and Malformation Syndromes. Genes 2025, 16, 87. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Dashraath, P.; Baud, D. Oropouche Virus (OROV) in Pregnancy: An Emerging Cause of Placental and Fetal Infection Associated with Stillbirth and Microcephaly following Vertical Transmission. Viruses 2024, 16, 1435. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Maternal | |||
| Prenatal Oropouche Fever (WG *) | 21–22 | 8–9 | 8–9 |
| Maternal age (years) | 22 | 33 | 37 |
| Drugs/Health conditions | No | No | Diabetes (from 33 WG) |
| Consanguinity | No | 2° degree | No |
| Previous pregnancies | 0 | 3 | 1 |
| Positive family history | No | No | No |
| Birth | |||
| Gestational age (weeks) | 38 | 36 | 37 |
| Head circumference (cm, Z-score **) | 30 (−2.66) | 26 (−4.40) | 28 |
| Weight (grams, Z-score) | 2740 (−0.75) | 2108 (−1.46) | 1826 |
| Length (cm, Z-score) | 45 (−1.8) | 45 (−1.06) | 45 |
| Physical findings | |||
| Microcephaly/Craniofacial disproportion/Skull collapse/short neck | Yes | Yes | Yes |
| Arthrogryposis multiplex | No | Yes | Yes |
| Fetal hydrops | No | Yes | Yes |
| Neurologic findings | Hypotonia, deep tendon hyperreflexia, dystonia, and epileptic seizures | Severe hypotonia (flaccid paralysis), no primitive or deep tendon reflexes, lack of suction, slow swallowing | Hypotonia, no deep tendon reflexes, lack of suction, slow swallowing |
| Ophthalmological findings | Visual impairment and nystagmus at 3 months | Corneal edema, optic disc atrophy, and chorioretinal scar in OU | Optic disc pallor and increased disc cupping (OS), chorioretinal macular scar and focal pigment mottling (OU), and vascular attenuation (OS) |
| Additional Exams | |||
| G-Banded Karyotype | NA | 46, XY | 46, XX |
| Array-SNP | NA | NA | Normal |
| Abdominal US *** | Normal | Pleural Effusion | Ascites |
| Echocardiogram | Patent oval foramen | Normal | Normal |
| Brainstem evoked response | Normal | NA | Normal |
| Electroneuromyography | Normal | NA | Normal |
| Brain and Spinal Cord Images | Overlapping sutures, marked cerebral atrophy, partial lissencephaly, absent corpus callosum, brain cysts (cystic encephalomalacia and/or chronic subpial hemorrhages), subdural effusion, suspected striatal fusion, normal posterior fossa, normal spinal cord | Overlapping sutures, marked cerebral atrophy, absent corpus callosum, diffuse lissencephaly, severe brainstem and cerebellar hypoplasia, brain cysts (cystic encephalomalacia and/or chronic subpial hemorrhages), subdural effusion | Overlapping sutures, moderate cerebral atrophy, hypoplastic corpus callosum, diffuse lissencephaly, severe brainstem and cerebellar hypoplasia with Dandy–Walker-like features, intraventricular hemorrhage Global thinning of the spinal cord, mainly on the thoracic segment |
| Biological Sample | Time of Sampling (Postpartum Days) | RT-qPCR | OROV ELISA IgM | Titer (HI) | Additional Serological Data | |
|---|---|---|---|---|---|---|
| Case 1 Infant | Serum | 2 | Not Detected | Positive OD 0.485 | 1:640 | Toxo (CLIA IgG/IgM): negative Rubella, CMV, Herpes (CLIA IgG): positive Rubella, CMV, Herpes (CLIA IgM): negative DENV, CHKV, ZIKV (ELISA IgM and and RT-qPCR): negative |
| Urine | 7 | Not Detected | NA | NA | NA | |
| Case 1 Mother | Serum | 1 | Not Detected | Positive OD 1.020 | ≥1:1280 | ** HIV, Syphilis, Hepatitis B and C: negative Toxo (CLIA IgG/IgM): negative Rubella, CMV, Herpes (CLIA IgG): positive ZIKV (ELISA IgG): positive Rubella, CMV, Herpes (CLIA IgM): negative DENV, CHKV, ZIKV (ELISA IgM and RT-qPCR): negative |
| Case 2 Infant | Serum | 1 | Not Detected | Positive OD 0.725 | 1:80 | Toxo (CLIA IgG/IgM): negative Rubella, CMV, Herpes (CLIA IgG): positive Rubella, CMV, Herpes (CLIA IgM): negative DENV, CHKV, ZIKV (ELISA IgM and RT-qPCR): negative |
| Post-Mortem tissues | CSF | 47 | Detected CT 31.7 | Positive OD 1.029 | DENV, CHKV, ZIKV (RT-qPCR): negative | |
| Pleural Fluid | Detected CT 33.7 | NA | DENV, CHKV, ZIKV (RT-qPCR): negative | |||
| Brain | Detected CT 20.4 | NA | DENV, CHKV, ZIKV (RT-q-PCR): negative | |||
| Lung | Detected CT 36.9 | NA | NA | |||
| Kidney | Detected CT 31.4 | NA | NA | |||
| Liver | Not Detected | NA | NA | |||
| Spleen | Not Detected | NA | NA | |||
| Heart | Inconclusive | NA | NA | |||
| Case 2 Mother | Serum | 1 | NA | Positive OD 0.363 | 1:320 | ** HIV, Syphilis, Hepatitis B and C: negative Toxo (CLIA IgG/IgM): negative Rubella, CMV, Herpes (CLIA IgG): positive Rubella, CMV, Herpes (CLIA IgM): negative DENV, CHKV, ZIKV (ELISA IgM): negative |
| Case 3 Infant | Serum | 5 | Not Detected | Positive OD 0.789 | 1:160 | Toxo, Rubella, CMV, Herpes (CLIA IgG): positive Toxo, Rubella, CMV, Herpes (CLIA IgM): negative DENV, ZIKV, CHKV (ELISA IgM and RT-qPCR): negative |
| CSF | 19 | Not Detected | Positive OD 0.653 | DENV, ZIKV, CHKV (ELISA IgM): negative | ||
| Case 3 Mother | Serum | 2 | NA | Positive OD 0.368 | 1:160 | ** HIV, Syphilis, Hepatitis B and C: negative Toxo, CMV, Rubella (CLIA IgG): positive Toxo, CMV, Rubella (CLIA IgM): negative DENV, CHKV, ZIKV (ELISA IgM): negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, B.d.F.R.; Barreto, A.R.F.; Pessoa, A.; Azevedo, R.d.S.d.S.; Rodrigues, F.d.F.; Borges, B.d.C.B.; Mantilla, N.P.M.; Muniz, D.D.; Chiang, J.O.; Fraga, L.R.; et al. Congenital Oropouche in Humans: Clinical Characterization of a Possible New Teratogenic Syndrome. Viruses 2025, 17, 397. https://doi.org/10.3390/v17030397
Ribeiro BdFR, Barreto ARF, Pessoa A, Azevedo RdSdS, Rodrigues FdF, Borges BdCB, Mantilla NPM, Muniz DD, Chiang JO, Fraga LR, et al. Congenital Oropouche in Humans: Clinical Characterization of a Possible New Teratogenic Syndrome. Viruses. 2025; 17(3):397. https://doi.org/10.3390/v17030397
Chicago/Turabian StyleRibeiro, Bethânia de Freitas Rodrigues, André Rodrigues Façanha Barreto, André Pessoa, Raimunda do Socorro da Silva Azevedo, Flávia de Freitas Rodrigues, Bruna da Cruz Beyruth Borges, Natália Pimentel Moreno Mantilla, Davi Dantas Muniz, Jannifer Oliveira Chiang, Lucas Rosa Fraga, and et al. 2025. "Congenital Oropouche in Humans: Clinical Characterization of a Possible New Teratogenic Syndrome" Viruses 17, no. 3: 397. https://doi.org/10.3390/v17030397
APA StyleRibeiro, B. d. F. R., Barreto, A. R. F., Pessoa, A., Azevedo, R. d. S. d. S., Rodrigues, F. d. F., Borges, B. d. C. B., Mantilla, N. P. M., Muniz, D. D., Chiang, J. O., Fraga, L. R., Vianna, F. S. L., Sanseverino, M. T. V., Faccini, L. S., Martins, F. E. d. N., Azevedo, R. d. S., Martins, L. C., Casseb, L. M. N., Oliveira, C. S., Vasconcelos, P. F. d. C., ... Schuler-Faccini, L. (2025). Congenital Oropouche in Humans: Clinical Characterization of a Possible New Teratogenic Syndrome. Viruses, 17(3), 397. https://doi.org/10.3390/v17030397