
Long COVID Complicated by Fatal Cytomegalovirus and Aspergillus Infection of the Lungs: An Autopsy Case Report

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
2.1. Clinical Course
2.2. Autopsy Investigation
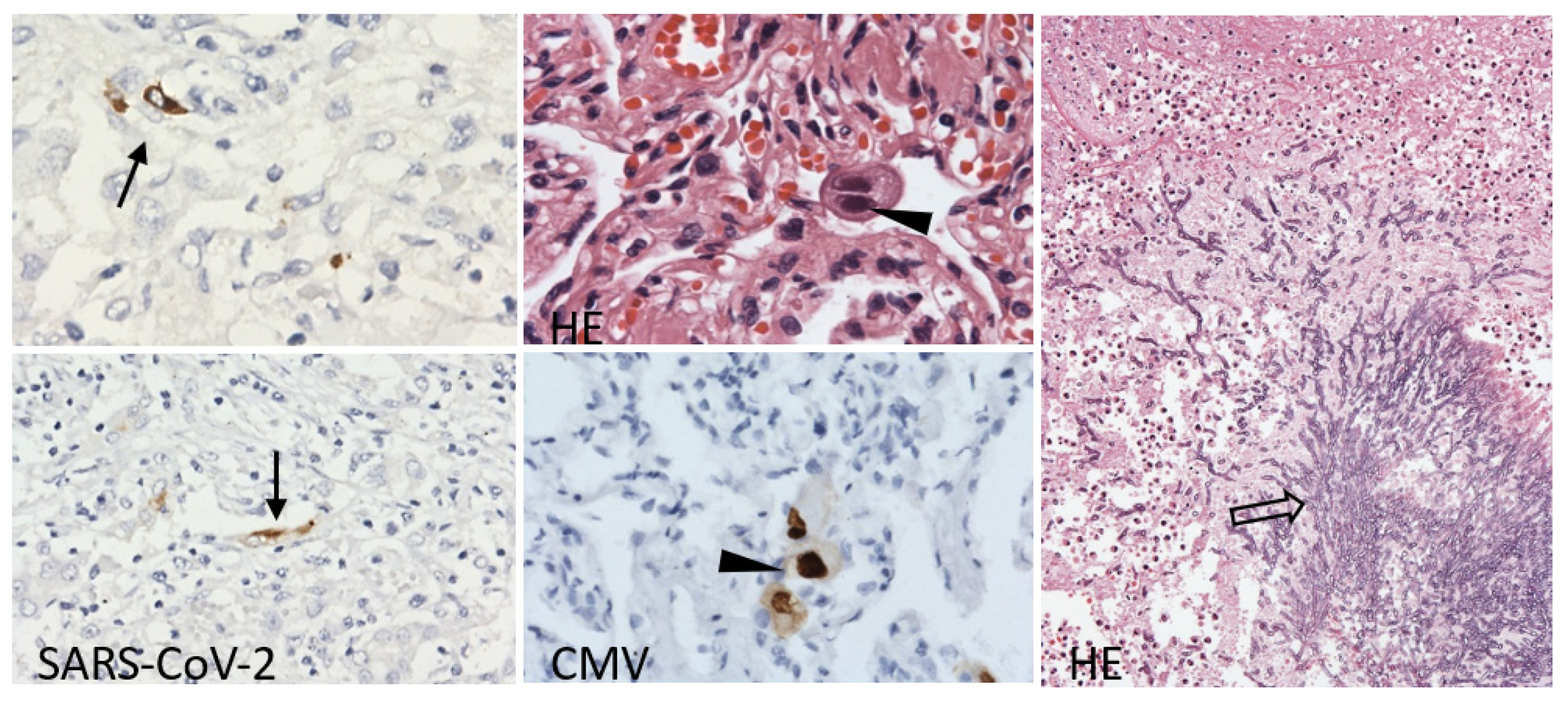
Histological Findings
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krivosíkova, L.; Horak, S.; Mikus-Kuracinova, K.; Janega, P.; Palkovic, M.; Babal, P. Contribution of immunohistochemistry to histomorphological diagnostics of COVID-19 pneumonia. Newslab 2021, 12, 12–16. [Google Scholar]
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; Howe, A.; Munier, C.M.L.; Patel, S.K.; Juno, J.A.; Burrell, L.M.; Kent, S.J.; Dore, G.J.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat. Immunol. 2022, 23, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Davitt, E.; Davitt, C.; Mazer, M.B.; Areti, S.S.; Hotchkiss, R.S.; Remy, K.E. COVID-19 disease and immune dysregulation. Best Pract. Res. Clin. Haematol. 2022, 35, 101401. [Google Scholar] [CrossRef]
- Alanio, C.; Verma, A.; Mathew, D.; Gouma, S.; Liang, G.; Dunn, T.; Oldridge, D.A.; Weaver, J.; Kuri-Cervantes, L.; Pampena, M.B.; et al. Cytomegalovirus latent infection is associated with an increased risk of COVID-19-related hospitalization. J. Infect. Dis. 2022, 226, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Niitsu, T.; Shiroyama, T.; Hirata, H.; Noda, Y.; Adachi, Y.; Enomoto, T.; Hara, R.; Amiya, S.; Uchiyama, A.; Takeda, Y.; et al. Cytomegalovirus infection in critically ill patients with COVID-19. J. Infect. 2021, 83, 496–522. [Google Scholar] [CrossRef]
- Kuehn, B.M. Aspergillosis is common among COVID-19 patients in the ICU. JAMA 2021, 326, 1573. [Google Scholar] [CrossRef]
- Salmanton-Garcia, J.; Sprute, R.; Stemler, J.; Bartoletti, M.; Dupont, D.; Valerio, M.; Garcia-Vidal, C.; Falces-Romero, I.; Machado, M.; de la Villa, S.; et al. COVID-19-associated pulmonary aspergillosis, March-August 2020. Emerg. Infect. Dis. 2021, 27, 1077–1086. [Google Scholar] [CrossRef]
- Kitayama, T.; Tone, K.; Makimura, K.; Takagi, M.; Kuwano, K. COVID-19-associated pulmonary aspergillosis complicated by severe coronavirus disease: Is detection of aspergillus in airway specimens before disease onset an indicator of antifungal prophylaxis? Cureus 2023, 15, e36212. [Google Scholar] [CrossRef]
- Choutka, J.; Jansari, V.; Hornig, M.; Iwasaki, A. Unexplained post-acute infection syndromes. Nat. Med. 2022, 28, 911–923. [Google Scholar] [CrossRef]
- Brandi, N.; Ciccarese, F.; Rimondi, M.R.; Balacchi, C.; Modolon, C.; Sportoletti, C.; Renzulli, M.; Coppola, F.; Golfieri, R. An imaging overview of COVID-19 ARDS in ICU patients and its complications: A pictorial review. Diagnostics 2022, 12, 846. [Google Scholar] [CrossRef]
- Halawa, S.; Pullamsetti, S.S.; Bangham, C.R.M.; Stenmark, K.R.; Dorfmuller, P.; Frid, M.G.; Butrous, G.; Morrell, N.W.; de Jesus Perez, V.A.; Stuart, D.I.; et al. Potential long-term effects of SARS-CoV-2 infection on the pulmonary vasculature: A global perspective. Nat. Rev. Cardiol. 2022, 19, 314–331. [Google Scholar] [CrossRef] [PubMed]
- Augusto, D.G.; Hollenbach, J.A. HLA variation and antigen presentation in COVID-19 and SARS-CoV-2 infection. Curr. Opin. Immunol. 2022, 76, 102178. [Google Scholar] [CrossRef] [PubMed]
- Mouliou, D.S.; Gourgoulianis, K.I. False-positive and false-negative COVID-19 cases: Respiratory prevention and management strategies, vaccination, and further perspectives. Expert Rev. Respir. Med. 2021, 15, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Luo, Q.; Mo, F.; Long, L.; Zheng, W. SARS-CoV-2 RNA more readily detected in induced sputum than in throat swabs of convalescent COVID-19 patients. Lancet Infect. Dis. 2020, 20, 655–656. [Google Scholar] [CrossRef]
- Stein, S.R.; Ramelli, S.C.; Grazioli, A.; Chung, J.Y.; Singh, M.; Yinda, C.K.; Winkler, C.W.; Sun, J.; Dickey, J.M.; Ylaya, K.; et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature 2022, 612, 758–763. [Google Scholar] [CrossRef]
- Babal, P.; Krivosikova, L.; Sarvaicova, L.; Deckov, I.; Szemes, T.; Sedlackova, T.; Palkovic, M.; Kalinakova, A.; Janega, P. Intrauterine fetal demise after uncomplicated COVID-19: What can we learn from the case? Viruses 2021, 13, 2545. [Google Scholar] [CrossRef]
- Natarajan, A.; Zlitni, S.; Brooks, E.F.; Vance, S.E.; Dahlen, A.; Hedlin, H.; Park, R.M.; Han, A.; Schmidtke, D.T.; Verma, R.; et al. Gastrointestinal symptoms and fecal shedding of SARS-CoV-2 RNA suggest prolonged gastrointestinal infection. Med 2022, 3, 371–387.e379. [Google Scholar] [CrossRef]
- Diaz, M.A.; Catalan-Caceres, N.; Beauperthuy, T.C.; Domingo, C.; Ibanez, E.; Morata, C.; De Diego, A. Clinical features and outcomes associated with bronchial asthma among COVID-19 hospitalized patients. J. Asthma Allergy 2022, 15, 775–781. [Google Scholar] [CrossRef]
- Philip, K.E.J.; Buttery, S.; Williams, P.; Vijayakumar, B.; Tonkin, J.; Cumella, A.; Renwick, L.; Ogden, L.; Quint, J.K.; Johnston, S.L.; et al. Impact of COVID-19 on people with asthma: A mixed methods analysis from a UK wide survey. BMJ Open Respir. Res. 2022, 9, e001056. [Google Scholar] [CrossRef]
- Ryan, F.J.; Hope, C.M.; Masavuli, M.G.; Lynn, M.A.; Mekonnen, Z.A.; Yeow, A.E.L.; Garcia-Valtanen, P.; Al-Delfi, Z.; Gummow, J.; Ferguson, C.; et al. Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection. BMC Med. 2022, 20, 26. [Google Scholar] [CrossRef]
- Abdoli, A.; Falahi, S.; Kenarkoohi, A. COVID-19-associated opportunistic infections: A snapshot on the current reports. Clin. Exp. Med. 2022, 22, 327–346. [Google Scholar] [CrossRef] [PubMed]
- Sathirareuangchai, S.; Bychkov, A. Aspergillus. PathologyOutlines.com Website. Available online: www.pathologyoutlines.com/topic/lungnontumoraspergillosis.html (accessed on 8 March 2023).
- Schauwvlieghe, A.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Kula, B.E.; Clancy, C.J.; Hong Nguyen, M.; Schwartz, I.S. Invasive mould disease in fatal COVID-19: A systematic review of autopsies. Lancet Microbe 2021, 2, e405–e414. [Google Scholar] [CrossRef] [PubMed]
- Platt, A.P.; Bradley, B.T.; Nasir, N.; Stein, S.R.; Ramelli, S.C.; Ramos-Benitez, M.J.; Dickey, J.M.; Purcell, M.; Singireddy, S.; Hays, N.; et al. Pulmonary co-infections detected premortem underestimate postmortem findings in a COVID-19 autopsy case series. Pathogens 2023, 12, 932. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Bussini, L.; Hoenigl, M.; Bartoletti, M. Prevalence of COVID-19-associated pulmonary aspergillosis: Critical review and conclusions. J. Fungi 2022, 8, 390. [Google Scholar] [CrossRef]
- Brandi, N.; Ciccarese, F.; Balacchi, C.; Rimondi, M.R.; Modolon, C.; Sportoletti, C.; Capozzi, C.; Renzulli, M.; Paccapelo, A.; Castelli, A.; et al. Co-infections and superinfections in COVID-19 critically ill patients are associated with CT imaging abnormalities and the worst outcomes. Diagnostics 2022, 12, 1617. [Google Scholar] [CrossRef]
- Weber, S.; Kehl, V.; Erber, J.; Wagner, K.I.; Jetzlsperger, A.M.; Burrell, T.; Schober, K.; Schommers, P.; Augustin, M.; Crowell, C.S.; et al. CMV seropositivity is a potential novel risk factor for severe COVID-19 in non-geriatric patients. PLoS ONE 2022, 17, e0268530. [Google Scholar] [CrossRef]
- Fonseca Brito, L.; Brune, W.; Stahl, F.R. Cytomegalovirus (CMV) pneumonitis: Cell tropism, inflammation, and immunity. Int. J. Mol. Sci. 2019, 20, 3865. [Google Scholar] [CrossRef]
- Chen, L.; Shen, L.; Wu, W.; Guan, W.; Zhou, J.; Luo, G.; Chen, Q.; Zhou, H.; Deng, Z.; Chen, Y.; et al. Co-infecting pathogens can contribute to inflammatory responses and severe symptoms in COVID-19. J. Thorac. Dis. 2022, 14, 355–370. [Google Scholar] [CrossRef]
- Pourabdollah Toutkaboni, M.; Hakamifard, A.; Abtahian, Z.; Mirahmadian, A.; Rahdar, M.; Mokhber Dezfuli, M.; Tabarsi, P. Co-infection of Klebsiella pneumonia, Cytomegalovirus, Aspergillus and Zygomycete in a patient with SARS-CoV-2. Clin. Case Rep. 2022, 10, e6033. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krivosikova, L.; Kuracinova, T.; Martanovic, P.; Hyblova, M.; Kaluzay, J.; Uhrinova, A.; Janega, P.; Babal, P. Long COVID Complicated by Fatal Cytomegalovirus and Aspergillus Infection of the Lungs: An Autopsy Case Report. Viruses 2023, 15, 1810. https://doi.org/10.3390/v15091810
Krivosikova L, Kuracinova T, Martanovic P, Hyblova M, Kaluzay J, Uhrinova A, Janega P, Babal P. Long COVID Complicated by Fatal Cytomegalovirus and Aspergillus Infection of the Lungs: An Autopsy Case Report. Viruses. 2023; 15(9):1810. https://doi.org/10.3390/v15091810
Chicago/Turabian StyleKrivosikova, Lucia, Tereza Kuracinova, Peter Martanovic, Michaela Hyblova, Jozef Kaluzay, Alexandra Uhrinova, Pavol Janega, and Pavel Babal. 2023. "Long COVID Complicated by Fatal Cytomegalovirus and Aspergillus Infection of the Lungs: An Autopsy Case Report" Viruses 15, no. 9: 1810. https://doi.org/10.3390/v15091810
APA StyleKrivosikova, L., Kuracinova, T., Martanovic, P., Hyblova, M., Kaluzay, J., Uhrinova, A., Janega, P., & Babal, P. (2023). Long COVID Complicated by Fatal Cytomegalovirus and Aspergillus Infection of the Lungs: An Autopsy Case Report. Viruses, 15(9), 1810. https://doi.org/10.3390/v15091810