
Comparative Analysis of Clinical Outcomes for COVID-19 and Influenza among Cardiac Transplant Recipients in the United States

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Covariates
- Patient: age, race, sex, comorbidities, insurance status, mean income in patient’s zip code, and disposition.
- Hospital: location, teaching status, bed size, and region.
- Illness severity: length of stay, mortality, hospitalization cost, Elixhauser comorbidity score.
- In-hospital complications: as below.
2.2. Study Outcomes
2.3. Statistical Methods
3. Results
3.1. Demographics and Baseline Comorbidities
3.2. In-Hospital Mortality
3.3. In-Hospital Complications
3.4. In-Hospital Quality Measures and Disposition
4. Discussion
5. Future Implications
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cimato, T.R.; Jessup, M. Recipient selection in cardiac transplantation: Contraindications and risk factors for mortality. J. Heart Lung Transplant. 2002, 21, 1161–1173. [Google Scholar] [CrossRef] [PubMed]
- Lund, L.H.; Edwards, L.B.; Kucheryavaya, A.Y.; Dipchand, A.I.; Benden, C.; Christie, J.D.; Dobbels, F.; Kirk, R.; Rahmel, A.O.; Yusen, R.D.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirtieth Official Adult Heart Transplant Report—2013; focus theme: Age. J. Heart Lung Transplant. 2013, 32, 951–964. [Google Scholar] [CrossRef] [PubMed]
- Deng, M.C. Cardiac transplantation. Heart 2002, 87, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Dengler, T.J.; Strnad, N.; Bühring, I.; Zimmermann, R.; Girgsdies, O.; Kubler, W.E.; Zielen, S. Differential immune response to influenza and pneumococcal vaccination in immunosuppressed patients after heart transplantation. Transplantation 1998, 66, 1340–1347. [Google Scholar] [CrossRef]
- Yamani, M.H.; Avery, R.K.; Mawhorter, S.D.; Young, J.B.; Ratliff, N.B.; Hobbs, R.E.; McCarthy, P.M.; Smedira, N.G.; Goormastic, M.; Pelegrin, D.; et al. Hypogammaglobulinemia following cardiac transplantation: A link between rejection and infection. J. Heart Lung Transplant. 2001, 20, 425–430. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Oseltamivir-resistant novel influenza A (H1N1) virus infection in two immunosuppressed patients—Seattle, Washington, 2009. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 893–896. [Google Scholar]
- Ng, B.J.H.; Glanville, A.R.; Snell, G.; Musk, M.; Holmes, M.; Chambers, D.C.; Hopkins, P.M.A. The impact of pandemic influenza A H1N1 2009 on Australian lung transplant recipients. Am. J. Transplant. 2011, 11, 568–574. [Google Scholar] [CrossRef]
- Whimbey, E.; Champlin, R.E.; Couch, R.B.; Englund, J.A.; Goodrich, J.M.; Raad, I.; Przepiorka, D.; Lewis, V.A.; Mirza, N.; Yousuf, H.; et al. Community respiratory virus infections among hospitalized adult bone marrow transplant recipients. Clin. Infect. Dis. 1996, 22, 778–782. [Google Scholar] [CrossRef]
- Rivinius, R.; Kaya, Z.; Schramm, R.; Boeken, U.; Provaznik, Z.; Heim, C.; Knosalla, C.; Schoenrath, F.; Rieth, A.; Berchtold-Herz, M.; et al. COVID-19 among heart transplant recipients in Germany: A multicenter survey. Clin. Res. Cardiol. 2020, 109, 1531–1539. [Google Scholar] [CrossRef]
- Singhvi, A.; Barghash, M.; Lala, A.; Mitter, S.S.; Parikh, A.; Oliveros, E.; Rollins, B.M.; Brunjes, D.L.; Alvarez-Garcia, J.; Johnston, E.; et al. Challenges in heart transplantation during COVID-19: A single-center experience. J. Heart Lung Transplant. 2020, 39, 894–903. [Google Scholar] [CrossRef]
- Latif, F.; Farr, M.A.; Clerkin, K.J.; Habal, M.V.; Takeda, K.; Naka, Y.; Restaino, S.; Sayer, G.; Uriel, N. Characteristics and outcomes of recipients of heart transplant with coronavirus disease 2019. JAMA Cardiol. 2020, 5, 1165–1169. [Google Scholar] [CrossRef]
- Pereira, M.R.; Mohan, S.; Cohen, D.J.; Husain, S.A.; Dube, G.; Ratner, L.E.; Arcasoy, S.; Aversa, M.M.; Benvenuto, L.J.; Dadhania, D.M.; et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am. J. Transplant. 2020, 20, 1800–1808. [Google Scholar] [CrossRef]
- NIS Database Documentation. Available online: https://hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp (accessed on 25 November 2022).
- Thompson, W.W.; Shay, D.K.; Weintraub, E.; Brammer, L.; Cox, N.; Anderson, L.J.; Fukuda, K. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA 2003, 289, 179–186. [Google Scholar] [CrossRef]
- Van Sickels, N.J.; Mave, V.; Zhang, R.; Killackey, M.; Paramesh, A.; Regenstein, F. Three organ transplant patients infected with 2009 novel H1N1 influenza in early fall, 2009. J. La. State Med. Soc. 2010, 162, 206, 208–213. [Google Scholar]
- Meyer, S.; Ilchmann, C.; Adam, M.; Sattinger, E.; Siamkouris, D.; Arunagirinathan, U.; Deuse, T.; Wagner, F.M.; Reichenspurner, H.; Costard-Jaeckle, A. Asymptomatic infection with novel influenza A/H1N1 virus in a heart transplant recipient. J. Heart Lung Transplant. 2010, 29, 585–586. [Google Scholar] [CrossRef]
- Kumar, D.; Michaels, M.G.; Morris, M.I.; Green, M.; Avery, R.K.; Liu, C.; Danziger-Isakov, L.; Stosor, V.; Estabrook, M.; Gantt, S.; et al. Outcomes from pandemic influenza A H1N1 infection in recipients of solid-organ transplants: A multicentre cohort study. Lancet Infect. Dis. 2010, 10, 521–526. [Google Scholar] [CrossRef]
- Gainer, S.M.; Patel, S.J.; Seethamraju, H.; Moore, L.W.; Knight, R.; Gaber, A.O. Increased mortality of solid organ transplant recipients with H1N1 infection: A single center experience. Clin. Transplant. 2012, 26, 229–237. [Google Scholar] [CrossRef]
- Montoya, J.G.; Giraldo, L.F.; Efron, B.; Stinson, E.B.; Gamberg, P.; Hunt, S.; Giannetti, N.; Miller, J.; Remington, J.S. Infectious complications among 620 consecutive heart transplant patients at Stanford University Medical Center. Clin. Infect. Dis. 2001, 33, 629–640. [Google Scholar] [CrossRef]
- Diaz-Arocutipa, C.; Carvallo-Castañeda, D.; Luis-Ybañez, O.; Pariona, M.; Rivas-Lasarte, M.; Alvarez-Garcia, J. COVID-19 in heart transplant recipients during February-August 2020: A systematic review. Clin. Transplant. 2021, 35, e14390. [Google Scholar] [CrossRef]
- Genuardi, M.V.; Moss, N.; Najjar, S.S.; Houston, B.A.; Shore, S.; Vorovich, E.; Atluri, P.; Molina, M.; Chambers, S.; Sharkoski, T.; et al. Coronavirus disease 2019 in heart transplant recipients: Risk factors, immunosuppression, and outcomes. J. Heart Lung Transplant. 2021, 40, 926–935. [Google Scholar] [CrossRef]
- View Data Reports—OPTN. Available online: https://optn.transplant.hrsa.gov/data/view-data-reports/ (accessed on 6 March 2023).
- Wolfe, S.B.; Calero, T.; Osho, A.A.; Michel, E.; Sundt, T.M.; D’Alessandro, D.A. Racial disparities in coronavirus disease 2019 mortality are present in heart transplant recipients. Ann. Thorac. Surg. 2022, 115, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Bottio, T.; Bagozzi, L.; Fiocco, A.; Nadali, M.; Caraffa, R.; Bifulco, O.; Ponzoni, M.; Lombardi, C.M.; Metra, M.; Russo, C.F.; et al. COVID-19 in Heart Transplant Recipients: A Multicenter Analysis of the Northern Italian Outbreak. JACC Heart Fail. 2021, 9, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Yang, J.; Zhao, F.; Zhi, L.; Wang, X.; Liu, L.; Bi, Z.; Zhao, Y. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 2020, 109, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G. COVID-19 and diabetes: Can DPP4 inhibition play a role? Diabetes Res. Clin. Pract. 2020, 162, 108125. [Google Scholar] [CrossRef] [PubMed]
- Pinto, B.G.G.; Oliveira, A.E.R.; Singh, Y.; Jimenez, L.; Goncalves, A.N.A.; Ogava, R.L.T.; Creighton, R.; Peron, J.P.S.; Nakaya, H.I. ACE2 Expression Is Increased in the Lungs of Patients With Comorbidities Associated With Severe COVID-19. J. Infect. Dis. 2020, 222, 556–563. [Google Scholar] [CrossRef]
- Wu, F.; Wang, A.; Liu, M.; Wang, Q.; Chen, J.; Xia, S.; Ling, Y.; Zhang, Y.; Xun, J.; Lu, L.; et al. Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications. medRxiv 2020. [Google Scholar] [CrossRef]
- Marcondes-Braga, F.G.; Murad, C.M.; Belfort, D.S.P.; Dantas, R.C.T.; Lira, M.T.S.S.; Aragao, C.A.S.; Siciliano, R.F.; Mangini, S.; Seguro, L.F.B.C.; Campos, I.W.; et al. Characteristics and Outcomes of Heart Transplant Recipients With Coronavirus-19 Disease in a High-volume Transplant Center. Transplantation 2022, 106, 641–647. [Google Scholar] [CrossRef]
- Piroth, L.; Cottenet, J.; Mariet, A.-S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: A nationwide, population-based retrospective cohort study. Lancet Respir. Med. 2021, 9, 251–259. [Google Scholar]
- Ludwig, M.; Jacob, J.; Basedow, F.; Anderson, F.; Walker, J. Clinical outcomes and characteristics of patients hospitalized for Influenza or COVID-19 in Germany. Int. J. Infect. Dis. 2021, 103, 316–322. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Nimkar, A.; Naaraayan, A.; Hasan, A.; Pant, S.; Durdevic, M.; Suarez, C.N.; Elenius, H.; Hambardzumyan, A.; Lakshmi, K.; Mandel, M.; et al. Incidence and Risk Factors for Acute Kidney Injury and Its Effect on Mortality in Patients Hospitalized From COVID-19. Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 4, 687–695. [Google Scholar] [CrossRef]
- Hadi, Y.B.; Naqvi, S.F.Z.; Kupec, J.T.; Sofka, S.; Sarwari, A. Outcomes of COVID-19 in Solid Organ Transplant Recipients: A Propensity-matched Analysis of a Large Research Network. Transplantation 2021, 105, 1365–1371. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- Lavery, A.M.; Preston, L.E.; Ko, J.Y.; Chevinsky, J.R.; DeSisto, C.L.; Pennington, A.F.; Kompaniyets, L.; Datta, S.D.; Click, E.S.; Golden, T.; et al. Characteristics of Hospitalized COVID-19 Patients Discharged and Experiencing Same-Hospital Readmission—United States, March-August 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1695–1699. [Google Scholar] [CrossRef]
- Akama-Garren, E.H.; Li, J.X. Prior immunosuppressive therapy is associated with mortality in COVID-19 patients: A retrospective study of 835 patients. J. Med. Virol. 2021, 93, 5768–5776. [Google Scholar] [CrossRef]
- Fraund, S.; Wagner, D.; Pethig, K.; Drescher, J.; Girgsdies, O.E.; Haverich, A. Influenza vaccination in heart transplant recipients. J. Heart Lung Transplant. 1999, 18, 220–225. [Google Scholar] [CrossRef]
- Peled, Y.; Ram, E.; Lavee, J.; Sternik, L.; Segev, A.; Wieder-Finesod, A.; Mandelboim, M.; Indendaum, V.; Levy, I.; Raanani, E.; et al. BNT162b2 vaccination in heart transplant recipients: Clinical experience and antibody response. J. Heart Lung Transplant. 2021, 40, 759–762. [Google Scholar] [CrossRef]
- Vilchez, R.A.; McCurry, K.; Dauber, J.; Lacono, A.; Griffith, B.; Fung, J.; Kusne, S. Influenza virus infection in adult solid organ transplant recipients. Am. J. Transplant. 2002, 2, 287–291. [Google Scholar] [CrossRef]
- Weinberg, A.; Lyu, D.M.; Li, S.; Marquesen, J.; Zamora, M.R. Incidence and morbidity of human metapneumovirus and other community-acquired respiratory viruses in lung transplant recipients. Transpl. Infect. Dis. 2010, 12, 330–335. [Google Scholar] [CrossRef]
- Mauch, T.J.; Bratton, S.; Myers, T.; Krane, E.; Gentry, S.R.; Kashtan, C.E. Influenza B virus infection in pediatric solid organ transplant recipients. Pediatrics 1994, 94 Pt 1, 225–229. [Google Scholar] [CrossRef]
- Evans, R.A.; McAuley, H.; Harrison, E.M.; Shikotra, A.; Singapuri, A.; Sereno, M.; Elneima, O.; Docherty, A.B.; Lone, N.I.; Leavy, O.C.; et al. Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): A UK multicentre, prospective cohort study. Lancet Respir. Med. 2021, 9, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.; Auerbach, S.R.; Richmond, M.E.; Sharp, B.; Pahl, E.; Feingold, B.; Azeka, E.; Dryer, W.J.; Cantor, R.S.; Kirklin, J.K.; et al. Early report from the Pediatric Heart Transplant Society on COVID-19 infections in pediatric heart transplant candidates and recipients. J. Heart Lung Transplant. 2022, 41, 327–333. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Heart Transplant Patients with COVID-19 | Heart Transplant Patients with Influenza | p-Value |
|---|---|---|---|
| n = 2460 | n = 1155 (47.0%) | n = 1305 (53.0%) | |
| Sex (Female) | 24.2% | 23.4% | 0.828 |
| Mean age years (SD) | 0.249 | ||
| Male | 61.3 (14.2) | 59.8 (14.8) | |
| Female | 57.4 (14.4) | 54.9 (15.5) | |
| Age Groups | 0.150 | ||
| ≥18–29 | 3.9% | 7.3% | |
| 30–49 | 17.3% | 15.3% | |
| 50–69 | 48.5% | 54.0% | |
| ≥70 | 30.3% | 23.4% | |
| Race | 0.282 | ||
| Caucasians | 49.3% | 55.1% | |
| African American | 31.7% | 25.6% | |
| Hispanics | 15.9% | 13.0% | |
| Asian or Pacific Islander | 0.9% | 3.2% | |
| Native American | 0.4% | 1.2% | |
| Others | 1.8% | 2.0% | |
| Median Household Income | 0.075 | ||
| 0–25th percentile | 27.1% | 29.3% | |
| 26–50th percentile | 30.1% | 21.1% | |
| 51–75th percentile | 26.2% | 26.2% | |
| ≥76th percentile | 16.6% | 23.4% | |
| Insurance Status | 0.521 | ||
| Medicare | 65.3% | 63.0% | |
| Medicaid | 9.8% | 7.0% | |
| Private | 24.0% | 28.8% | |
| Self-pay | 0.9% | 1.2% | |
| Hospital Division | 0.753 | ||
| New England | 2.6% | 5.8% | |
| Middle Atlantic | 19.1% | 13.8% | |
| East North Central | 14.7% | 17.6% | |
| West North Central | 9.1% | 7.7% | |
| South Atlantic | 16.5% | 20.3% | |
| East South Central | 6.9% | 6.5% | |
| West South Central | 15.6% | 12.6% | |
| Mountain | 6.1% | 5.4% | |
| Pacific | 9.5% | 10.3% | |
| Hospital Bedsize | 0.960 | ||
| Small | 9.1% | 8.4% | |
| Medium | 17.3% | 18.0% | |
| Large | 73.6% | 73.6% | |
| Hosptal Teaching Status | 0.030 | ||
| Rural | 5.6% | 2.3% | |
| Urban non-teaching | 4.3% | 8.8% | |
| Urban teaching | 90.0% | 88.9% | |
| Comorbidities Mean Elixhauser Score (SD) | 4.8 (1.9) | 4.2 (1.9) | |
| Pulmonary Circulation Disorder | 5.6% | 6.1% | 0.816 |
| Peripheral Vascular Disorder | 13.4% | 14.6% | 0.714 |
| Hypertension | 64.5% | 60.5% | 0.360 |
| Chronic Pulmonary Disease | 16.9% | 23.0% | 0.094 |
| Diabetes | 53.7% | 54.0% | 0.930 |
| Hypothyroidism | 18.2% | 16.1% | 0.533 |
| Liver Disease | 6.5% | 4.2% | 0.262 |
| Lymphoma | 0.9% | 1.5% | 0.502 |
| Metastatic Cancer | 1.3% | 0.4% | 0.295 |
| Solid Tumor without Metastasis | 3.5% | 1.5% | 0.185 |
| Rheumatoid Arthritis | 3.0% | 0.4% | 0.020 |
| Coagulopathy | 18.6% | 11.9% | 0.038 |
| Obesity | 22.5% | 11.9% | 0.001 |
| Weight Loss | 10.0% | 8.1% | 0.465 |
| Alcohol Abuse | 2.2% | 0.4% | 0.077 |
| Drug Abuse | 1.7% | 1.5% | 0.862 |
| Depression | 14.7% | 17.6% | 0.408 |
| Chronic Kidney Disease | 39.8% | 26.8% | 0.003 |
| Variable | Heart Transplant Patients with COVID-19 | Heart Transplant Patients with Influenza | p-Value |
|---|---|---|---|
| In-hospital mortality (n = 120) | 9.5% | 0.8% | |
| Adjusted odds ratio 1 51.6 (4.3–615.9) | 0.002 | ||
| Mechanical ventilation | 13.9% | 5.4% | |
| Adjusted odds ratio 1 4.0 (1.2–13.1) | 0.021 | ||
| Acute kidney injury on hemodialysis | 6.9% | 1.9% | |
| Adjusted odds ratio 1 3.7 (0.7–21.3) | 0.137 | ||
| Acute heart failure | 3.5% | 4.6% | |
| Adjusted odds ratio 1 0.2 (0.1–0.9) | 0.031 | ||
| Pulmonary embolism | 1.3% | 0.4% | |
| Adjusted odds ratio 2 1.5 (0.0–72.6) | 0.829 | ||
| Cerebrovascular accident | 1.3% | 0.8% | |
| Adjusted odds ratio 1 1.1 (0.2–6.9) | 0.948 | ||
| Atrial arrhythmia | 15.6% | 10.7% | |
| Adjusted odds ratio 1 1.3 (0.5–3.4) | 0.576 | ||
| Ventricular arrhythmias | 1.7% | 1.5% | |
| Adjusted odds ratio 1 31.3 (1.6–608.5) | 0.023 | ||
| Conduction abnormalities | 10.0% | 6.9% | |
| Adjusted odds ratio 1 1.9 (0.7–5.1) | 0.231 | ||
| Sudden cardiac arrest | 0.4% | 0.8% | |
| Adjusted odds ratio 2 1.4 (0.1–24.1) | 0.809 | ||
| Cardiogenic shock | 1.3% | 0.8% | |
| Adjusted odds ratio 2 0.1 (0.0–4.4) | 0.201 | ||
| Heart transplant rejection | 1.3% | 0.4% | |
| Adjusted odds ratio 3 7.2 (0.9–57.1) | 0.062 | ||
| Myocardities | 0.43% | 0.38 | |
| Adjusted odds ratio 3 0.83 (0.07–10.1) | 0.08 | ||
| Mean total hospitalization charge (USD) | 138,967 | 52,803 | |
| 84,623 higher | 0.001 | ||
| Mean length of stay (days) | 9.4 | 5.9 | |
| 0.6 days lower | 0.877 | ||
| Disposition | 0.036 | ||
| Home/Routine | 67.2% | 78.8% | |
| SNF 4/LTAC 5/Nursing home | 14.1% | 9.6% | |
| Home health | 18.8% | 11.2% | |
| AMA 6 | - | 0.4% | |
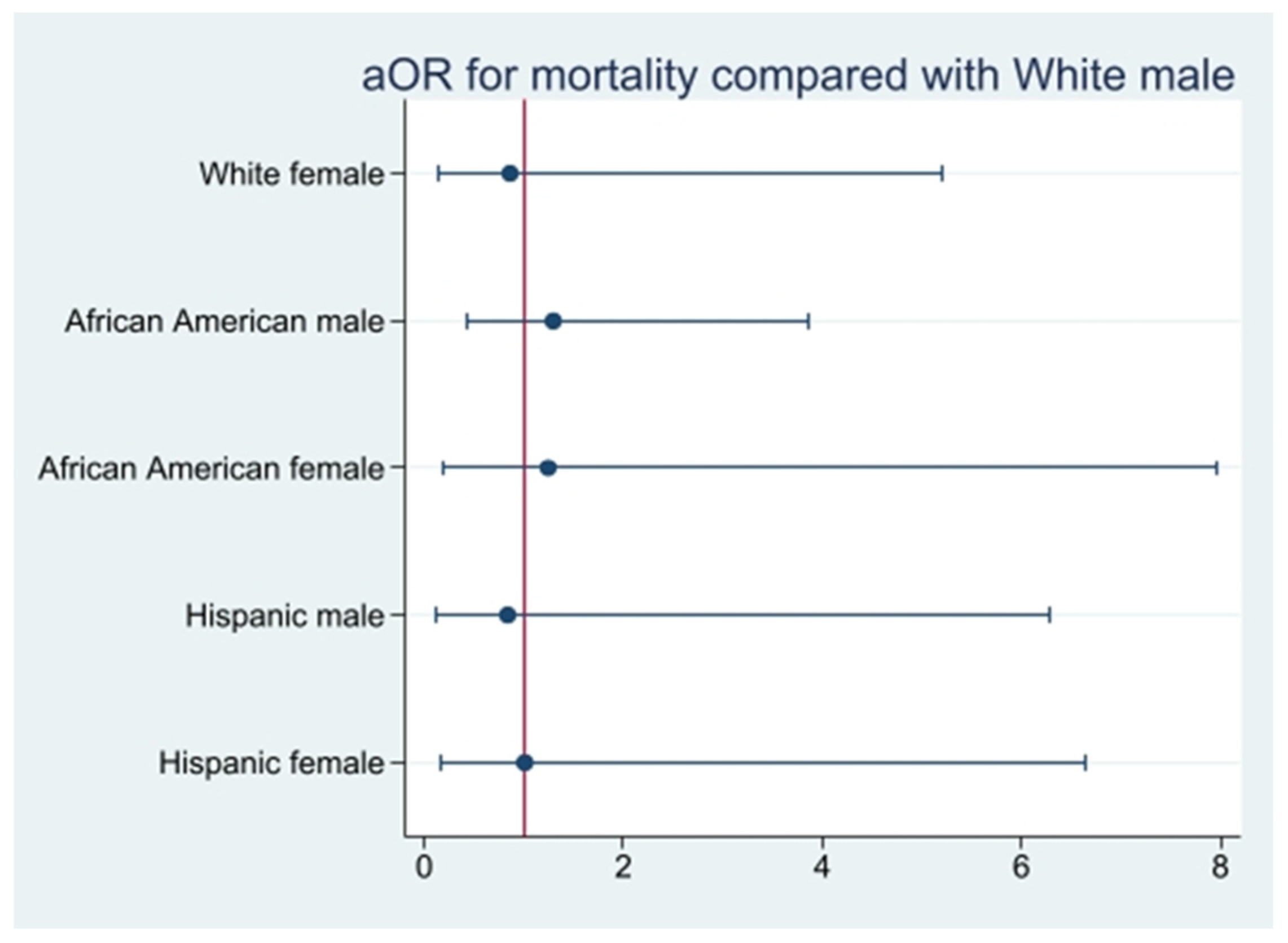
| aOR | 95% CI (LL-UL) | p-Value | |
|---|---|---|---|
| White female | 0.9 | 0.1-5.2 | 0.870 |
| Black male | 1.3 | 0.4-3.9 | 0.630 |
| Black female | 1.2 | 0.2-8.0 | 0.810 |
| Hispanic male | 0.8 | 0.1-6.3 | 0.860 |
| Hispanic female | 1.0 | 0.2-6.6 | 0.980 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chavarin, D.J.; Bobba, A.; Davis, M.G.; Roth, M.A.; Kasdorf, M.; Nasrullah, A.; Chourasia, P.; Gangu, K.; Avula, S.R.; Sheikh, A.B. Comparative Analysis of Clinical Outcomes for COVID-19 and Influenza among Cardiac Transplant Recipients in the United States. Viruses 2023, 15, 1700. https://doi.org/10.3390/v15081700
Chavarin DJ, Bobba A, Davis MG, Roth MA, Kasdorf M, Nasrullah A, Chourasia P, Gangu K, Avula SR, Sheikh AB. Comparative Analysis of Clinical Outcomes for COVID-19 and Influenza among Cardiac Transplant Recipients in the United States. Viruses. 2023; 15(8):1700. https://doi.org/10.3390/v15081700
Chicago/Turabian StyleChavarin, Daniel J., Aniesh Bobba, Monique G. Davis, Margaret A. Roth, Michelle Kasdorf, Adeel Nasrullah, Prabal Chourasia, Karthik Gangu, Sindhu Reddy Avula, and Abu Baker Sheikh. 2023. "Comparative Analysis of Clinical Outcomes for COVID-19 and Influenza among Cardiac Transplant Recipients in the United States" Viruses 15, no. 8: 1700. https://doi.org/10.3390/v15081700
APA StyleChavarin, D. J., Bobba, A., Davis, M. G., Roth, M. A., Kasdorf, M., Nasrullah, A., Chourasia, P., Gangu, K., Avula, S. R., & Sheikh, A. B. (2023). Comparative Analysis of Clinical Outcomes for COVID-19 and Influenza among Cardiac Transplant Recipients in the United States. Viruses, 15(8), 1700. https://doi.org/10.3390/v15081700