
Efficacy and Safety of Two-Drug Regimens with Dolutegravir plus Rilpivirine or Lamivudine in HIV-1 Virologically Suppressed People Living with HIV

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Material and Methods
2.1. Patients and Study Design
2.2. Outcomes
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Virological Suppression
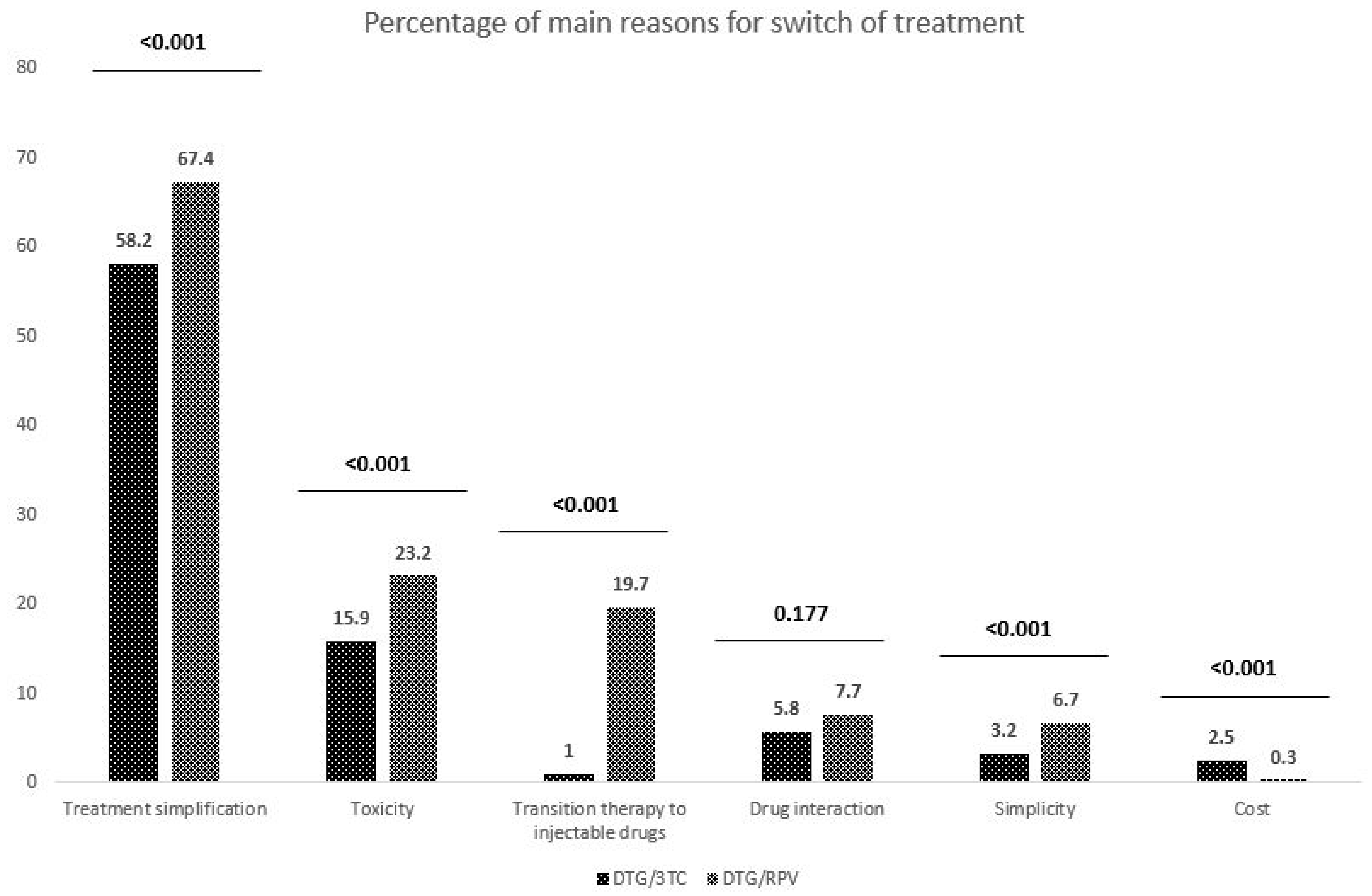
3.3. Treatment Discontinuation
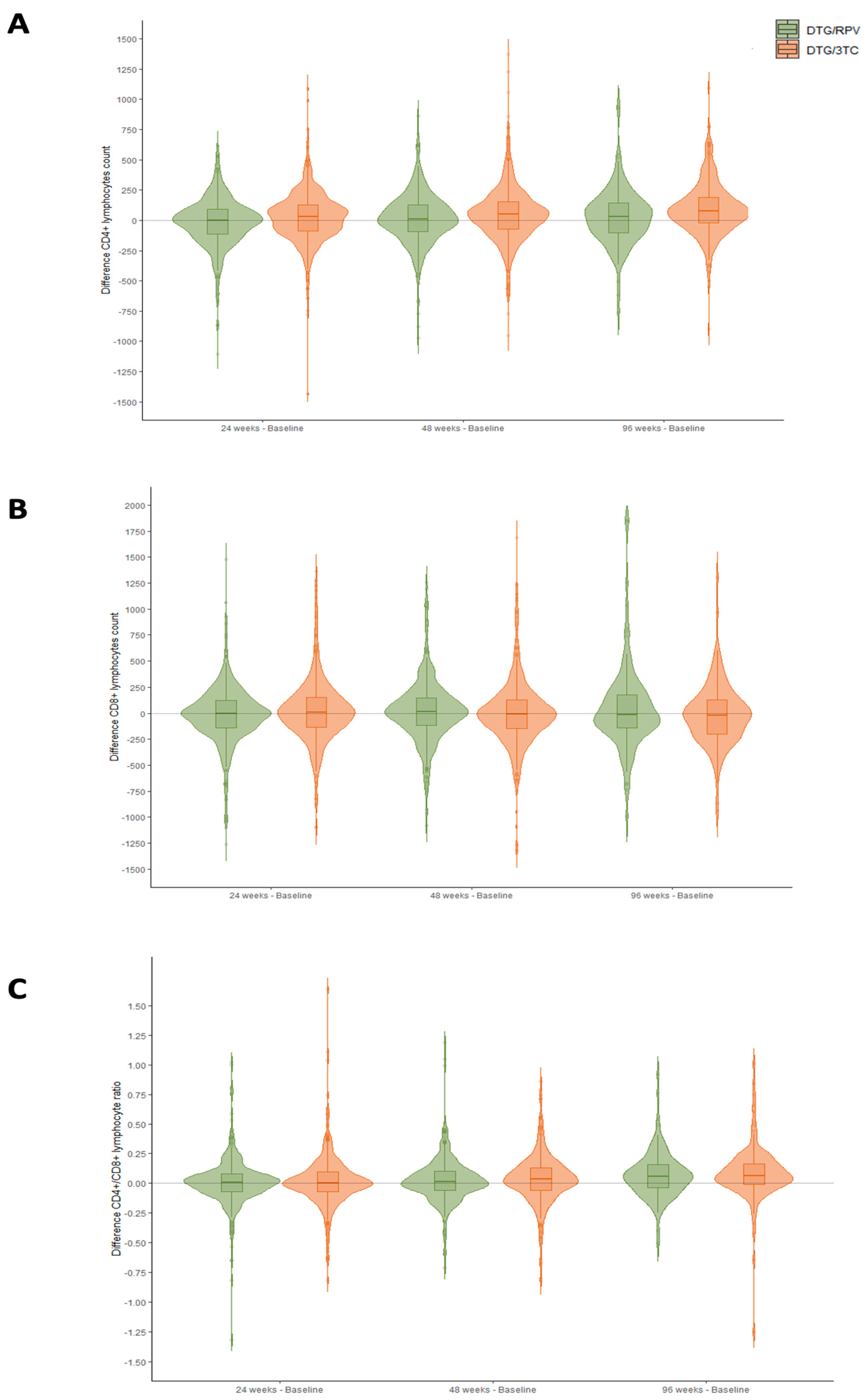
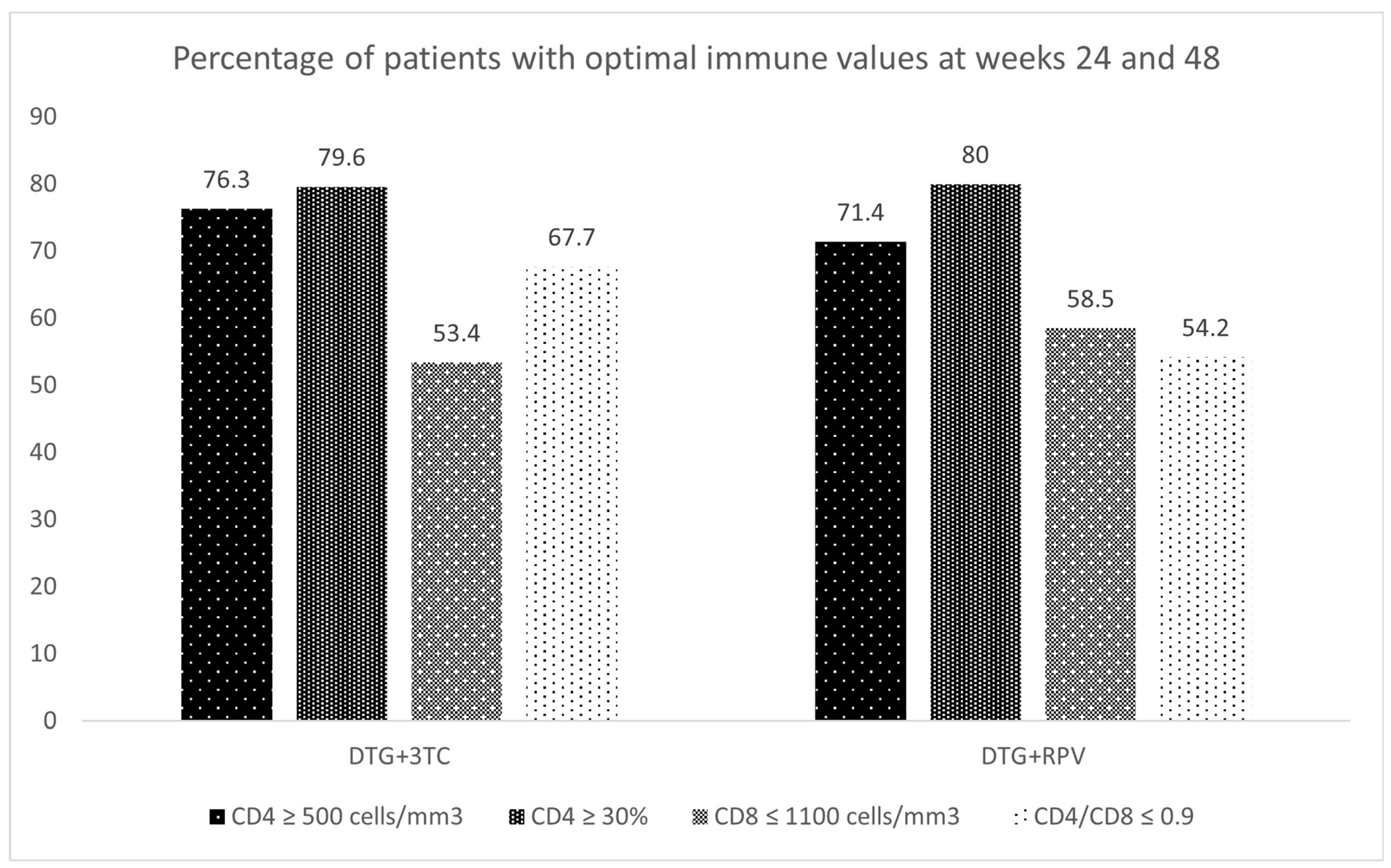
3.4. Immune Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
SPADE Study Group
DORIPEX Study Group
Appendix A

{kind=link}
{kind=link}
{kind=link}
| DTG/3TC | DTG/RPV | ||
|---|---|---|---|
| Variable | Median [IQR] | Median [IQR] | p-Value |
| CD4 (cells/mm3) week 24–baseline CD4 (cells/mm3) | 31.5 [−87.8, 128.2] | −0.5 [−116.0, 90.0] | <0.001 |
| CD4 (cells/mm3) week 48–baseline CD4 (cells/mm3) | 49.0 [−74.0, 155.0] | 11.5 [−94.0, 126.0] | 0.017 |
| CD4 (cells/mm3) week 96–baseline CD4 (cells/mm3) | 78.0 [−21.5, 189.5] | 29.0 [−104.0, 142.0] | 0.003 |
| CD8 (cells/mm3) week 24–baseline CD8 (cells/mm3) | 10.0 [−136.0, 152.0] | −4.0 [−143.8, 122.2] | 0.087 |
| CD8 (cells/mm3) week 48–baseline CD8 (cells/mm3) | −9.5 [−143.8, 128.5] | 16.0 [−115.5, 147.0] | 0.084 |
| CD8 (cells/mm3) week 96–baseline CD8 (cells/mm3) | −14.5 [−200.5, 132.2] | −15.0 [−143.0, 180.0] | 0.451 |
| CD4/CD8 week 24–baseline CD4/CD8 | 0.0 [−0.1, 0.1] | 0.0 [−0.1, 0.1] | 0.972 |
| CD4/CD8 week 48–baseline CD4/CD8 | 0.0 [−0.1, 0.1] | 0.0 [−0.1, 0.1] | 0.066 |
| CD4/CD8 week 96–baseline CD4/CD8 | 0.1 [0.0, 0.2] | 0.1 [−0.1, 0.2] | 0.216 |
References
- Department of Health and Human Services. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Available online: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/AdultandAdolescentGL.pdf (accessed on 6 September 2021).
- European AIDS Clinical Society. Guidelines Version 11, October 2021. Available online: https://www.eacsociety.org/files/guidelines-10.1_finaljan2021_1.pdf (accessed on 2 November 2021).
- Saag, M.S.; Gandhi, R.T.; Hoy, J.F.; Landovitz, R.J.; Thompson, M.A.; Sax, P.E.; Smith, D.M.; Benson, C.A.; Buchbinder, S.P.; Del Rio, C.; et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2020 recommendations of the international antiviral society-USA panel. JAMA 2020, 324, 1651–1669. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Updated Recommendations on First-Line and Second-Line Antiretroviral Regimens and Postexposure Prophylaxis and Recommendations on Early Infant Diagnosis of HIV: Interim Guidance, 2018. Available online: https://www.who.int/hiv/pub/guidelines/ARV2018update (accessed on 2 November 2021).
- Kanters, S.; Vitoria, M.; Doherty, M.; Socias, M.E.; Ford, N.; Forrest, J.I.; Popoff, E.; Bansback, N.; Nsanzimana, S.; Thorlund, K.; et al. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of HIV infection: A systematic review and network meta-analysis. Lancet HIV 2016, 3, e510–e520. [Google Scholar] [CrossRef] [PubMed]
- Cahn, P.; Madero, J.S.; Arribas, J.R.; Antinori, A.; Ortiz, R.; Clarke, A.E.; Hung, C.-C.; Rockstroh, J.K.; Girard, P.-M.; Sievers, J.; et al. Dolutegravir plus lamivudine versus dolutegravir plus tenofovir disoproxil fumarate and emtricitabine in antiretroviral-naive adults with HIV-1 infection (GEMINI-1 and GEMINI-2): Week 48 results from two multicentre, double-blind, randomised, non-inferiority, phase 3 trials. Lancet 2019, 393, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Van Wyk, J.; Ajana, F.; Bisshop, F.; De Wit, S.; Osiyemi, O.; Portilla, J.; Routy, J.; Wyen, C.; Ait-Khaled, M.; Nascimento, M.; et al. Switching to DTG/3TC fixed-dose combination (FDC) is non-inferior to continuing a TAF-based regimen in maintaining virologic suppression through 48 weeks (TANGO study, Oral Presentation). In Proceedings of the 10th International AIDS Society Conference on HIV Science, Mexico City, Mexico, 21–24 July 2019. [Google Scholar]
- Llibre, J.M.; Hung, C.-C.; Brinson, C.; Castelli, F.; Girard, P.-M.; Kahl, L.P.; Blair, E.A.; Angelis, K.; Wynne, B.; Vandermeulen, K.; et al. Efficacy, safety, and tolerability of dolutegravir-rilpivirine for the maintenance of virological suppression in adults with HIV-1: Phase 3, randomised, non-inferiority SWORD-1 and SWORD-2 studies. Lancet 2018, 391, 839–849. [Google Scholar] [CrossRef]
- Clotet, B.; Feinberg, J.; van Lunzen, J.; Khuong-Josses, M.-A.; Antinori, A.; Dumitru, I.; Pokrovskiy, V.; Fehr, J.; Ortiz, R.; Saag, M.; et al. Once-daily dolutegravir versus darunavir plus ritonavir in antiretroviral-naive adults with HIV-1 infection (FLAMINGO): 48 week results from the randomised open-label phase 3b study. Lancet 2014, 383, 2222–2231. [Google Scholar] [CrossRef]
- Walmsley, S.L.; Antela, A.A.; Clumeck, N.; Duiculescu, D.; Eberhard, A.A.; Gutiérrez, F.; Hocqueloux, L.L.; Maggiolo, F.F.; Sandkovsky, U.U.; Granier, C.C.; et al. Dolutegravir plus Abacavir–Lamivudine for the Treatment of HIV-1 Infection. N. Engl. J. Med. 2013, 369, 1807–1818. [Google Scholar] [CrossRef]
- Gubavu, C.; Prazuck, T.; Niang, M.; Buret, J.; Mille, C.; Guinard, J.; Avettand-Fènoël, V.; Hocqueloux, L. Dolutegravir-based monotherapy or dual therapy maintains a high proportion of viral suppression even in highly experienced HIV-1-infected patients. J. Antimicrob. Chemother. 2015, 71, 1046–1050. [Google Scholar] [CrossRef]
- Maggiolo, F.; Gulminetti, R.; Pagnucco, L.; Digaetano, M.; Benatti, S.; Valenti, D.; Callegaro, A.; Ripamonti, D.; Mussini, C. Lamivudine/dolutegravir dual therapy in HIV-infected, virologically suppressed patients. BMC Infect. Dis. 2017, 17, 215. [Google Scholar] [CrossRef]
- Joly, V., Burdet, C., Landman, R., Raffi, R., Katlama, C., Cabié, A., Eds.; Promising results of dolutegravir + lamivudine maintenance in ANRS 167 LAMIDOL trial [Abstract 458]. In Proceedings of the 24th Conference on Retroviruses and Opportunistic Infections (CROI), Seattle, DC, USA, 13–16 February 2017. [Google Scholar]
- Llibre, J.M.; Brites, C.; Cheng, C.Y.; Osiyemi, O.; Galera, C.; Hocqueloux, L.; Maggiolo, F.; Degen, O.; Taylor, S.; Blair, E.; et al. Efficacy and Safety of Switching to the 2-Drug Regimen Dolutegravir/Lamivudine Versus Continuing a 3- or 4-Drug Regimen for Maintaining Virologic Suppression in Adults Living with Human Immunodeficiency Virus 1 (HIV-1): Week 48 Results from the Phase 3, Noninferiority SALSA Randomized Trial. Clin. Infect. Dis. 2023, 76, 720–729. [Google Scholar] [CrossRef]
- Wandeler, G.; Buzzi, M.; Anderegg, N.; Sculier, D.; Béguelin, C.; Egger, M.; Calmy, A. Virologic failure and HIV drug resistance on simplified, dolutegravir-based maintenance therapy: Systematic review and meta-analysis. F1000Research 2018, 7, 1359. [Google Scholar] [CrossRef]
- Serrano-Villar, S.; Pérez-Elías, M.J.; Dronda, F.; Casado, J.L.; Moreno, A.; Royuela, A.; Pérez-Molina, J.A.; Sainz, T.; Navas, E.; Hermida, J.M.; et al. Increased risk of serious non-AIDS-related events in HIV-infected subjects on antiretroviral therapy associated with a low CD4/CD8 ratio. PLoS ONE 2014, 9, e85798. [Google Scholar] [CrossRef] [PubMed]
- Mussini, C.; Lorenzini, P.; Cozzi-Lepri, A.; Lapadula, G.; Marchetti, G.; Nicastri, E.; Cingolani, A.; Lichtner, M.; Antinori, A.; Gori, A.; et al. CD4/CD8 ratio normalisation and non-AIDS-related events in individuals with HIV who achieve viral load suppression with antiretroviral therapy: An observational cohort study. Lancet HIV 2015, 2, e98–e106. [Google Scholar] [CrossRef] [PubMed]
- Wada, N.I.; Jacobson, L.P.; Margolick, J.B.; Breen, E.C.; Macatangay, B.; Penugonda, S.; Martínez-Maza, O.; Bream, J.H. The effect of HAART-induced HIV suppression on circulating markers of inflammation and immune activation. Aids 2015, 29, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Olearo, F.; Nguyen, H.; Bonnet, F.; Yerly, S.; Wandeler, G.; Stoeckle, M.; Cavassini, M.; Scherrer, A.; Costagiola, D.; Schmid, P.; et al. Impact of the m184v/I mutation on the Efficacy of abacavir/lamivudine/dolutegravir therapy in hiv treatment-experienced patients. Open Forum. Infect Dis. 2019, 6, ofz330. [Google Scholar] [CrossRef] [PubMed]
- Restelli, S.; Romeri, F.; Piscaglia, M.; Rizzelli, D.; Gallazzi, I.; Paladini, L.; Cossu, M.; Micheli, V.; Capetti, A. Determinants and Outcomes of the Choice to Switch to Dolutegravir within Different Three- or Two-Drug Regimens in a Single-Centre Cohort: The Dolutility Study; International Congress of Drug Therapy in HIV Infection: Glasgow, UK, 2018. [Google Scholar]
- Sangare, M.; Baril, J.; Pokomandy, A.D. Virological outcome after switching a suppressive haart to dolutegravir (dtg) with 2 nrtis among hiv-1 infected patients: Potential effects of previous suboptimal therapies or previous virologic failures. J. Int. AIDS Soc. 2018, 21, e25187. [Google Scholar]
- Noe, S.; Ummard-Berger, K.; Hillenbrand, H.; Beer, D.; Wyen, C.; Pauli, R.; Postel, N.; Dymek, K.M.; Westermayer, B.; Scherzer, J. 12-month outcome of Dolutegravir/Rilpivirine in virologically suppressed HIV-infected patients:real-world data from the German JUNGLE cohort (poster). In Proceedings of the HIV Drug Therapy 2020, Virtual, 5–8 October 2020. [Google Scholar]
- Capetti, A.F.; Sterrantino, G.; Cossu, M.V.; Orofino, G.; Barbarini, G.; De Socio, G.V.; Di Giambenedetto, S.; Di Biagio, A.; Celesia, B.M.; Argenteri, B.; et al. Switch to Dolutegravir plus Rilpivirine dual therapy in cART-experienced subjects: An observational cohort. PLoS ONE 2016, 11, e0164753. [Google Scholar] [CrossRef]
- Troya, J.; Dueñas, C.; Irazola, I.; de Los Santos, I.; de la Fuente, S.; Gil, D.; Hernández, C.; Galindo, M.J.; Gómez, J.; Delgado, E.; et al. Dolutegravir plus rilpivirine: Benefits beyond viral suppression: DORIPEX retrospective study. Medicine 2022, 101, e29252. [Google Scholar] [CrossRef]
- Joly, V.; Burdet, C.; Landman, R.; Vigan, M.; Charpentier, C.; Katlama, C.; Cabié, A.; Benalycherif, A.; Peytavin, G.; Yeni, P.; et al. Dolutegravir and lamivudine maintenance therapy in HIV-1 virologically suppressed patients: Results of the ANRS 167 trial (LAMIDOL). J. Antimicrob. Chemother. 2019, 74, 739–745. [Google Scholar] [CrossRef]
- Hidalgo-Tenorio, C.; Cortés, L.L.; Gutiérrez, A.; Santos, J.; Omar, M.; Gálvez, C.; Sequera, S.; De Jesús, S.E.; Téllez, F.; Fernández, E.; et al. DOLAMA study: Effectiveness, safety and pharmacoeconomic analysis of dual therapy with dolutegravir and lamivudine in virologically suppressed HIV-1 patients. Medicine 2019, 98, e16813. [Google Scholar] [CrossRef]
- Galizzi, N.; Poli, A.; Galli, L.; Muccini, C.; Mastrangelo, A.; Dell’Acqua, R.; Maillard, M.; Bossolasco, S.; Cinque, P.; Lazzarin, A.; et al. Retrospective study on the outcome of two-drug regimens based on dolutegravir plus one reverse transcriptase inhibitor in virologically-suppressed HIV-infected patients. Int. J. Antimicrob. Agents 2020, 55, 105893. [Google Scholar] [CrossRef] [PubMed]
- Deschanvres, C.; Raffi, F.; Reynes, J. Virologic failure and resistance in dolutegravir-based maintenance dual regimens. (poster). In Proceedings of the Conference on Retroviruses and Opportunistic Infections 2020, Boston, MA, USA, 8–11 March 2020. [Google Scholar]
- Gagliardini, R.; Lorenzini, P.; Cozzi-Lepri, A. Effect of past virological failure on dolutegravir+lamivudine as maintenance regimen (poster). In Proceedings of the Conference on Retroviruses and Opportunistic Infections 2020, Boston, MA, USA, 8–11 March 2020. [Google Scholar]
- Diaz, A.; Casado, J.L.; Dronda, F.; Gomez-Ayerbe, C.; Vivancos, M.J.; Banon, S.; Quereda, C.; Serrano, S.; Moreno, A.; Navas, E.; et al. Dolutegravir plus rilpivirina in suppressed heavily pretreated HIV-infected patients [abstract tupdb0 106]. In Proceedings of the 21st International AIDS Conference, Durban, South Africa, 18–22 July 2016. [Google Scholar]
- Achhra, A.C.; Mwasakifwa, G.; Amin, J.; Boyd, M.A. Efficacy and safety of contemporary dual-drug antiretroviral regimens as first-line treatment or as a simplification strategy: A systematic review and meta-analysis. Lancet HIV 2016, 3, e351–e360. [Google Scholar] [CrossRef]
- Hidalgo-Tenorio, C.; Vinuesa, D.; García-Vallecillos, C.; Muñoz-Medina, L.; Sequera, S.; Javier, R.; López-Ruz, M.Á.; Sadyrbaeva-Dolgova, S.; Pasquau, J. Rildo: Real-World Multicenter Study on the Effectiveness and Safety of Single-Tablet Regimen of Dolutegravir plus Rilpivirine in Treatment-Experienced People Living with HIV. Viruses 2022, 14, 2626. [Google Scholar] [CrossRef] [PubMed]
- Taiwo, B.O.; Marconi, V.C.; Berzins, B.; Moser, C.B.; Nyaku, A.N.; Fichtenbaum, C.J.; Benson, C.A.; Wilkin, T.; Koletar, S.L.; Colasanti, J.; et al. Dolutegravir Plus Lamivudine Maintains Human Immunodeficiency Virus-1 Suppression Through Week 48 in a Pilot Randomized Trial. Clin. Infect. Dis. 2017, 66, 1794–1797. [Google Scholar] [CrossRef] [PubMed]
- Gantner, P.; Cuzin, L.; Allavena, C.; Cabie, A.; Pugliese, P.; Valantin, M.-A.; Bani-Sadr, F.; Joly, V.; Ferry, T.; Poizot-Martin, I.; et al. Efficacy and safety of dolutegravir and rilpivirine dual therapy as a simplification strategy: A cohort study. HIV Med. 2017, 18, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Borghetti, A.; Baldin, G.; Lombardi, F.; Ciccullo, A.; Capetti, A.; Rusconi, S.; Sterrantino, G.; Latini, A.; Cossu, M.; Gagliardini, R.; et al. Efficacy and tolerability of lamivudine plus dolutegravir as a switch strategy in a multicentre cohort of patients with suppressed HIV-1 replication. HIV Med. 2018, 19, 452–454. [Google Scholar] [CrossRef]
- Gagliardini, R.; Ciccullo, A.; Borghetti, A.; Maggiolo, F.; Bartolozzi, D.; Borghi, V.; Pecorari, M.; Di Biagio, A.; Callegaro, A.P.; Bruzzone, B.; et al. Impact of the M184V Resistance Mutation on Virological Efficacy and Durability of Lamivudine-Based Dual Antiretroviral Regimens as Maintenance Therapy in Individuals With Suppressed HIV-1 RNA: A Cohort Study. Open Forum Infect. Dis. 2018, 5, ofy113. [Google Scholar] [CrossRef]
- Ciccullo, A.; Baldin, G.; Capetti, A.; Rusconi, S.; Sterrantino, G.; D’Ettorre, G.; Colafigli, M.; Modica, S.; Lagi, F.; Giacomelli, A.; et al. A Comparison between two Dolutegravir-Based two-drug Regimens as Switch Strategies in a Multicentre Cohort of HIV-1-Infected Patients. Antivir. Ther. 2019, 24, 63–67. [Google Scholar] [CrossRef]
- de Boer, M.G.; van den Berk, G.E.; van Holten, N.; Oryszcyn, J.E.; Dorama, W.; Brinkman, K. Intolerance of dolutegravir-containing combination antiretroviral therapy regimens in real-life clinical practice. AIDS 2016, 30, 2831–2834. [Google Scholar] [CrossRef]
- Hoffmann, C.; Welz, T.; Sabranski, M.; Kolb, M.; Wolf, E.; Stellbrink, H.-J.; Wyen, C. Higher rates of neuropsychiatric adverse events leading to dolutegravir discontinuation in women and older patients. HIV Med. 2016, 18, 56–63. [Google Scholar] [CrossRef]
- Baldin, G.; Ciccullo, A.; Rusconi, S.; Capetti, A.; Sterrantino, G.; Colafigli, M.; d’Ettorre, G.; Giacometti, A.; Cossu, M.V.; Borghetti, A.; et al. Long-term data on the efficacy and tolerability of lamivudine plus dolutegravir as a switch strategy in a multicenter cohort of HIV-1-infected, virologically suppressed patients. Int. J. Antimicrob Agents 2019, 54, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Evitt, L.; Mariolis, I.; Di Giambenedetto, S.; d’Arminio Monforte, A.; Casado, J.; Cabello Úbeda, A.; Hocqueloux, L.; Allavena, C.; Barber, T.; et al. Multicenter study to evaluate the effectiveness and safety of dolutegravir and lamivudine dual therapy in real life (poster). In Proceedings of the XI Congreso Nacional GeSIDA, Toledo, Spain, 10–13 December 2019. [Google Scholar]
- Postel, N.; Schneeweiss, S.; Wyen, C.; Schabaz, F.; Degen, O.; Weinberg, G.; Sabranski, M.; Ummard-Berger, K.; Dymek, K.M.; Westermayer10, B.; et al. Real-world data from the prospective URBAN cohort study on the use of dolutegravir (DTG) + lamivudine (3TC) in ART-naïve and pretreated people living with HIV in Germany (Oral presentation). In Proceedings of the HIV Drug Therapy Glasgow 2020, Virtual, 5–8 October 2020. [Google Scholar]
- Bonijoly, T.; Cabie, A.; Cotte, L. Week-48 Efficacy and safety of dolutegravir + rilpivirine dual therapy as a switch strategy in a real-life cohort study (Oral presentation). In Proceedings of the 16th European AIDS Conference, Milan, Italy, 18–21 October 2017. [Google Scholar]
- Reeves, A.A.; Fuentes, A.V.; Caballero, J.; Thomas, J.E.; Ii, J.F.M.; Harrington, C. Neurotoxicities in the treatment of HIV between dolutegravir, rilpivirine and dolutegravir/rilpivirine: A meta-analysis. Sex. Transm. Infect. 2021, 97, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Jenks, J.D.; Hoenigl, M. CD4:CD8 ratio and CD8+ cell count for prognosticating mortality in HIV-infected patients on antiretroviral therapy. J. Lab. Precis. Med. 2018, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Monsalvo, M.; Vallejo, A.; Fontecha, M.; Vivancos, M.J.; Vizcarra, P.; Casado, J.L. CD4/CD8 ratio improvement in HIV-1-infected patients receiving dual antiretroviral treatment. Int. J. STD AIDS 2019, 30, 656–662. [Google Scholar] [CrossRef] [PubMed]



| DTG Plus 3TC | DTG Plus RPV | p-Value | |
|---|---|---|---|
| DEMOGRAPHIC | |||
| Age, median [IQR] | 50.0 [40.0, 58.0] | 53.0 [43.0, 58.0] | <0.001 |
| Male sex n (%) | 737/943 (78.2) | 475/638 (74.5) | 0.099 |
| Spanish nationality n (%) | 705/910 (77.5) | 534/630 (84.8) | <0.001 |
| COMORBIDITIES n (%) | |||
| Arterial hypertension | 109/943 (11.6) | 124/638 (19.4) | <0.001 |
| Diabetes | 44/943 (4.7) | 67/638 (10.5) | <0.001 |
| Dyslipidemia | 197/943 (20.9) | 198/638 (31.0) | <0.001 |
| Heart Disease | 26/943 (2.8) | 34/638 (5.3) | 0.013 |
| Cerebrovascular disease | 9/943 (1.0) | 10/638 (1.6) | 0.389 |
| Peripheral vascular disease | 10/943 (1.1) | 13/638 (2.0) | 0.168 |
| Kidney failure | 37/943 (3.9) | 55/638 (8.6) | <0.001 |
| Osteoporosis/Osteopenia | 27/943 (2.9) | 83/638 (13.0) | <0.001 |
| Chronic pulmonary disease | 42/943 (4.5) | 55/638 (8.6) | 0.001 |
| Psychiatric disorders | 74/943 (7.8) | 67/638 (10.5) | 0.084 |
| Cancer | 13/943 (1.4) | 17/638 (2.7) | 0.099 |
| Chronic liver disease | 98/943 (10.4) | 94/638 (14.7) | 0.012 |
| HIV INFECTION | |||
| Transmission pathways n (%) | |||
| Sexual intercourse | 641/923 (69.1) | 371/621 (58.8) | <0.001 |
| Intravenous drug injectors | 178/923 (19.2) | 163/621 (25.8) | <0.001 |
| Immune status, median [IQR] | |||
| Nadir CD4 (cells/mm3) | - | 283.47 (232.39) | - |
| Baseline CD4 (cells/mm3) | 759.0 [556.0, 983.8] | 701.0 [516.0, 933.0] | 0.003 |
| 24 weeks CD4 (cells/mm3) | 777.5 [596.0, 980.0] | 686.0 [509.5, 893.5] | <0.001 |
| 48 weeks CD4 (cells/mm3) | 789.0 [583.5, 1015.5] | 702.0 [513.0, 937.0] | <0.001 |
| 96 weeks CD4 (cells/mm3) | 832.0 [608.0, 1059.0] | 666.0 [494.0, 939.0] | <0.001 |
| Baseline CD8 (cells/mm3) | 866.0 [628.5, 1173.5] | 839.0 [618.0, 1148.0] | 0.392 |
| 24 weeks CD8 (cells/mm3) | 894.0 [647.0, 1203.5] | 841.0 [594.0, 1132.0] | 0.008 |
| 48 weeks CD8 (cells/mm3) | 889.0 [623.2, 1200.0] | 862.8 [644.0, 1119.8] | 0.627 |
| 96 weeks CD8 (cells/mm3) | 909.5 [624.5, 1239.2] | 890.5 [664.5, 1185.0] | 0.868 |
| Baseline CD4/CD8 ratio | 0.9 [0.6, 1.2] | 0.8 [0.6, 1.2] | 0.017 |
| 24 weeks CD4/CD8 ratio | 0.9 [0.6, 1.2] | 0.8 [0.6, 1.2] | 0.053 |
| 48 weeks CD4/CD8 ratio | 0.9 [0.6, 1.3] | 0.8 [0.6, 1.2] | 0.004 |
| 96 weeks CD4/CD8 ratio | 0.9 [0.7, 1.3] | 0.8 [0.5, 1.1] | 0.002 |
| AIDS diagnosis n (%) | 759.0 [556.0, 983.8] | 701.0 [516.0, 933.0] | 0.003 |
| Age of diagnosis, median [IQR] | |||
| Global cohort | 37.0 [27.0, 47.0] | 34.0 [25.0, 42.0] | <0.001 |
| AIDS patients | 46.0 [32.0, 54.0] | 36.0 [28.0, 47.0] | <0.001 |
| Non-AIDS patients | 34.0 [24.0, 46.0] | 33.0 [24.0, 41.0] | 0.319 |
| Previous treatment n (%) | |||
| Backbone | |||
| - ABC/3TC | 353/943 (37.4) | 105/504 (20.8) | <0.001 |
| - FTC/TDF | 432/943 (45.8) | 126/504 (25.0) | <0.001 |
| - FTC/TAF | 137/943 (14.5) | 221/504 (43.8) | <0.001 |
| Third agent | |||
| - bPI | 246/943 (26.1) | 176/638 (27.6) | 0.546 |
| - INSTI | 435/943 (46.1) | 260/638 (40.8) | 0.039 |
| - NNRTI | 316/943 (33.5) | 334/638 (52.4) | <0.001 |
| CO-INFECTIONS, n(%) | |||
| HBV diagnosis | 180/631 (28.5) | 158/615 (25.7) | 0.225 |
| HBsAg positive | 9/177 (5.1) | 3/157 (1.9) | 0.080 |
| HCV positive ELISA | 144/635 (22.7) | 198/614 (32.2) | <0.001 |
| HCV positive PCR | 47/136 (34.6) | 55/196 (28.1) | 0.135 |
| ALL POPULATION | |||||||
|---|---|---|---|---|---|---|---|
| Overall | DTG/3TC | DTG/RPV | |||||
| N | % | N | % | N | % | p-Value | |
| 24 weeks < 50 copies/mL | 1357/1400 | 96.9 | 840/860 | 97.7 | 517/540 | 95.7 | 0.041 |
| 48 weeks < 50 copies/mL | 1126/1156 | 97.4 | 697/711 | 98.0 | 429/445 | 96.4 | 0.091 |
| 96 weeks < 50 copies/mL | 552/557 | 99.1 | 401/404 | 99.3 | 151/153 | 98.7 | 0.528 |
| Non-AIDS POPULATION | |||||||
| 24 weeks < 50 copies/mL | 887/913 | 97.2 | 497/511 | 97.3 | 390/402 | 97.0 | 0.825 |
| 48 weeks < 50 copies/mL | 692/710 | 97.5 | 366/376 | 97.3 | 326/334 | 97.6 | 0.823 |
| 96 weeks < 50 copies/mL | 221/223 | 99.1 | 119/121 | 98.3 | 102/102 | 100.0 | 0.192 |
| AIDS POPULATION | |||||||
| 24 weeks < 50 copies/mL | 216/230 | 93.9 | 95/98 | 96.9 | 121/132 | 91.7 | 0.098 |
| 48 weeks < 50 copies/mL | 177/188 | 94.1 | 76/79 | 96.2 | 101/109 | 92.7 | 0.307 |
| 96 weeks < 50 copies/mL | 89/89 | 96.6 | 38/39 | 97.4 | 48/50 | 96.0 | 0.710 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dueñas-Gutiérrez, C.; Buzón, L.; Pedrero-Tomé, R.; Iribarren, J.A.; De los Santos, I.; De la Fuente, S.; Pousada, G.; Moran, M.A.; Moreno, E.; Ferreira, E.; et al. Efficacy and Safety of Two-Drug Regimens with Dolutegravir plus Rilpivirine or Lamivudine in HIV-1 Virologically Suppressed People Living with HIV. Viruses 2023, 15, 936. https://doi.org/10.3390/v15040936
Dueñas-Gutiérrez C, Buzón L, Pedrero-Tomé R, Iribarren JA, De los Santos I, De la Fuente S, Pousada G, Moran MA, Moreno E, Ferreira E, et al. Efficacy and Safety of Two-Drug Regimens with Dolutegravir plus Rilpivirine or Lamivudine in HIV-1 Virologically Suppressed People Living with HIV. Viruses. 2023; 15(4):936. https://doi.org/10.3390/v15040936
Chicago/Turabian StyleDueñas-Gutiérrez, Carlos, Luis Buzón, Roberto Pedrero-Tomé, José A. Iribarren, Ignacio De los Santos, Sara De la Fuente, Guillermo Pousada, Miguel Angel Moran, Estela Moreno, Eva Ferreira, and et al. 2023. "Efficacy and Safety of Two-Drug Regimens with Dolutegravir plus Rilpivirine or Lamivudine in HIV-1 Virologically Suppressed People Living with HIV" Viruses 15, no. 4: 936. https://doi.org/10.3390/v15040936
APA StyleDueñas-Gutiérrez, C., Buzón, L., Pedrero-Tomé, R., Iribarren, J. A., De los Santos, I., De la Fuente, S., Pousada, G., Moran, M. A., Moreno, E., Ferreira, E., Gómez, J., & Troya, J. (2023). Efficacy and Safety of Two-Drug Regimens with Dolutegravir plus Rilpivirine or Lamivudine in HIV-1 Virologically Suppressed People Living with HIV. Viruses, 15(4), 936. https://doi.org/10.3390/v15040936