
Investigation of Dengue Infection in Asymptomatic Individuals during a Recent Outbreak in La Réunion

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical Definitions and Laboratory Diagnosis
2.3. Laboratory Diagnosis
2.4. Identification of Index Cases
2.5. Sample Size
2.6. Cluster Definitions and Data Collection
2.7. Statistical Methods
2.8. Ethics and Confidentiality
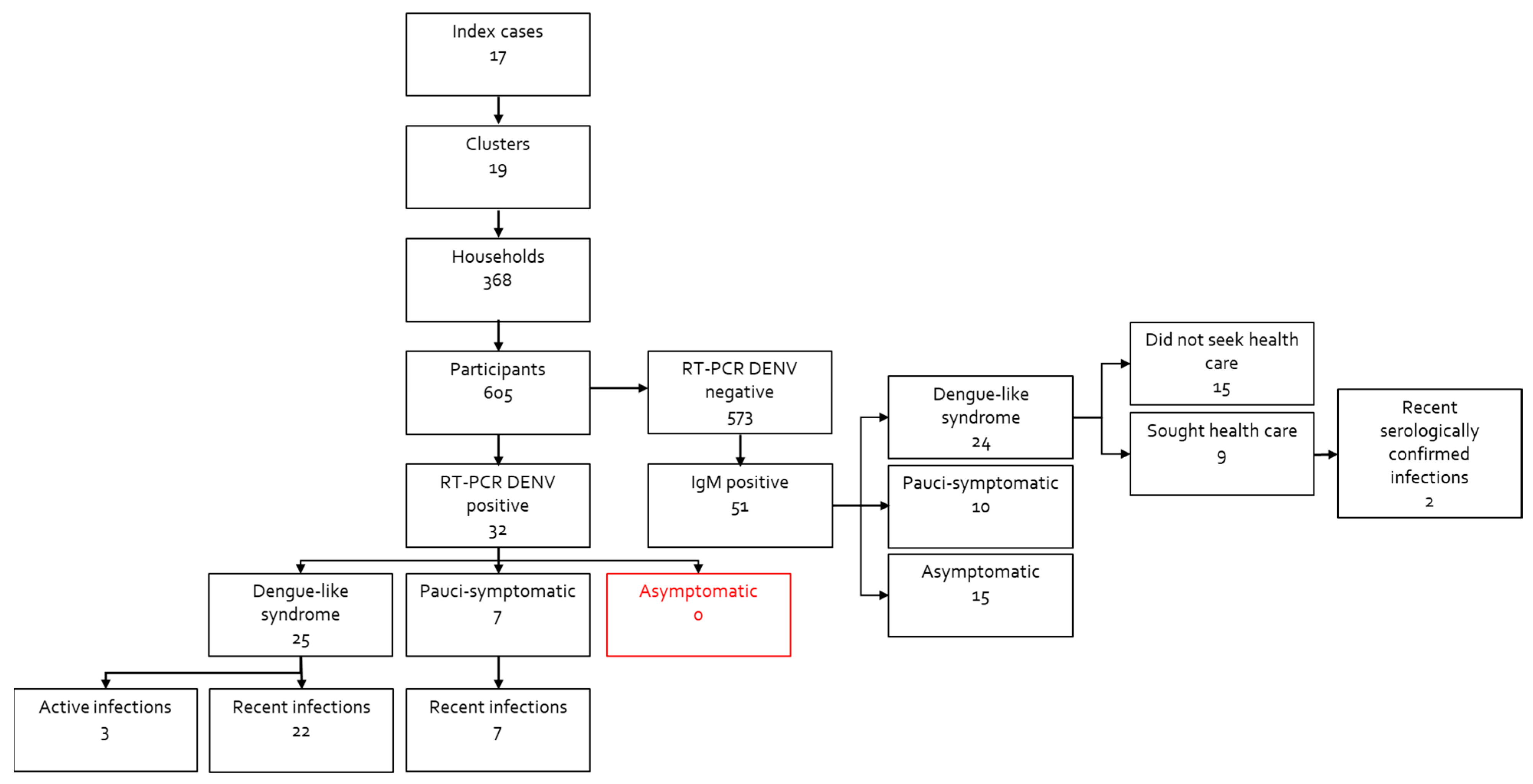
3. Results
3.1. Cluster Investigation
3.2. Demographic Characteristics
3.3. Detection of Dengue Virus by RT-PCR
3.4. Dengue-Positive RT-PCR in Households
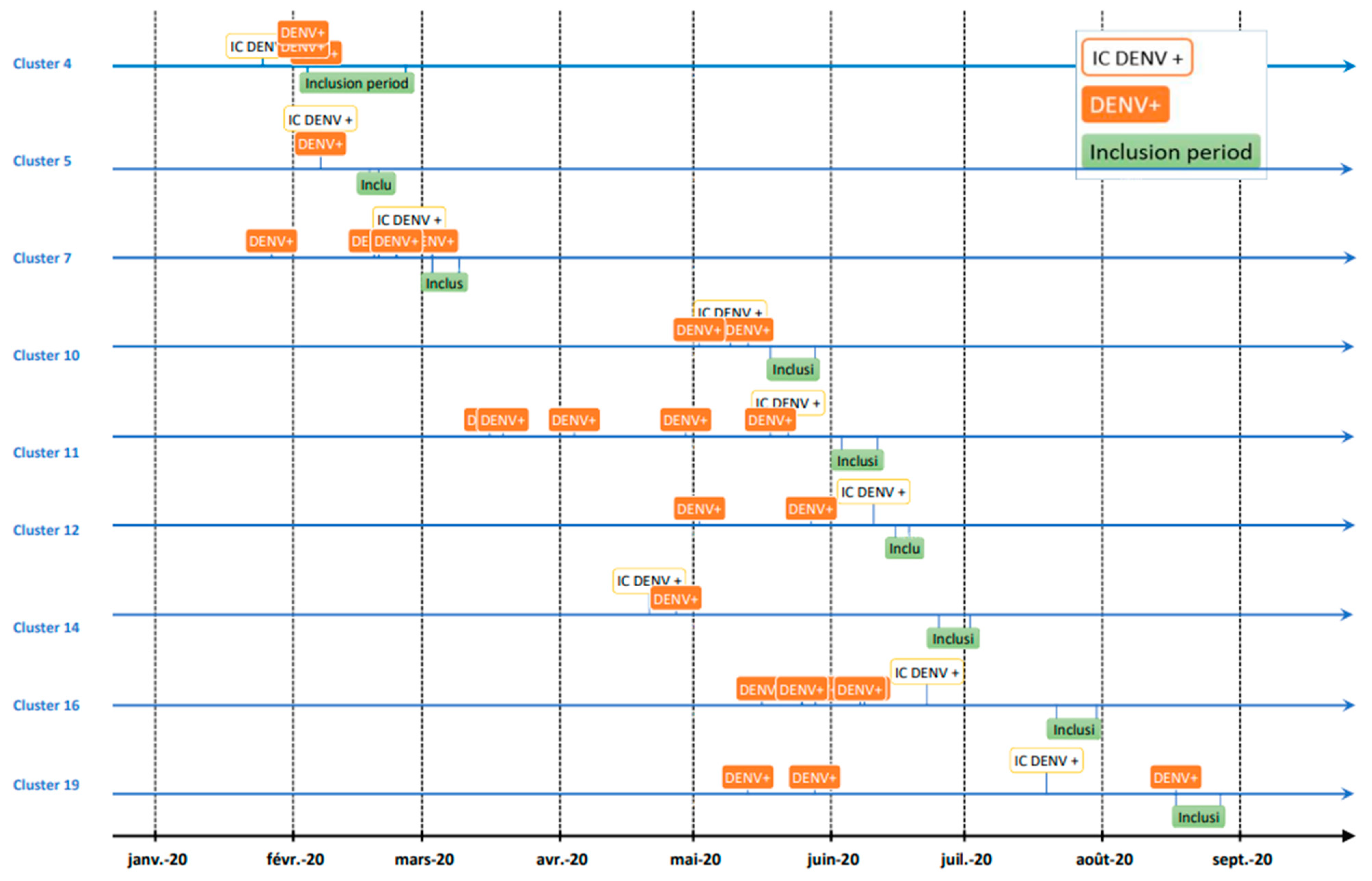
3.5. Time Interval between Dengue Infections within Clusters
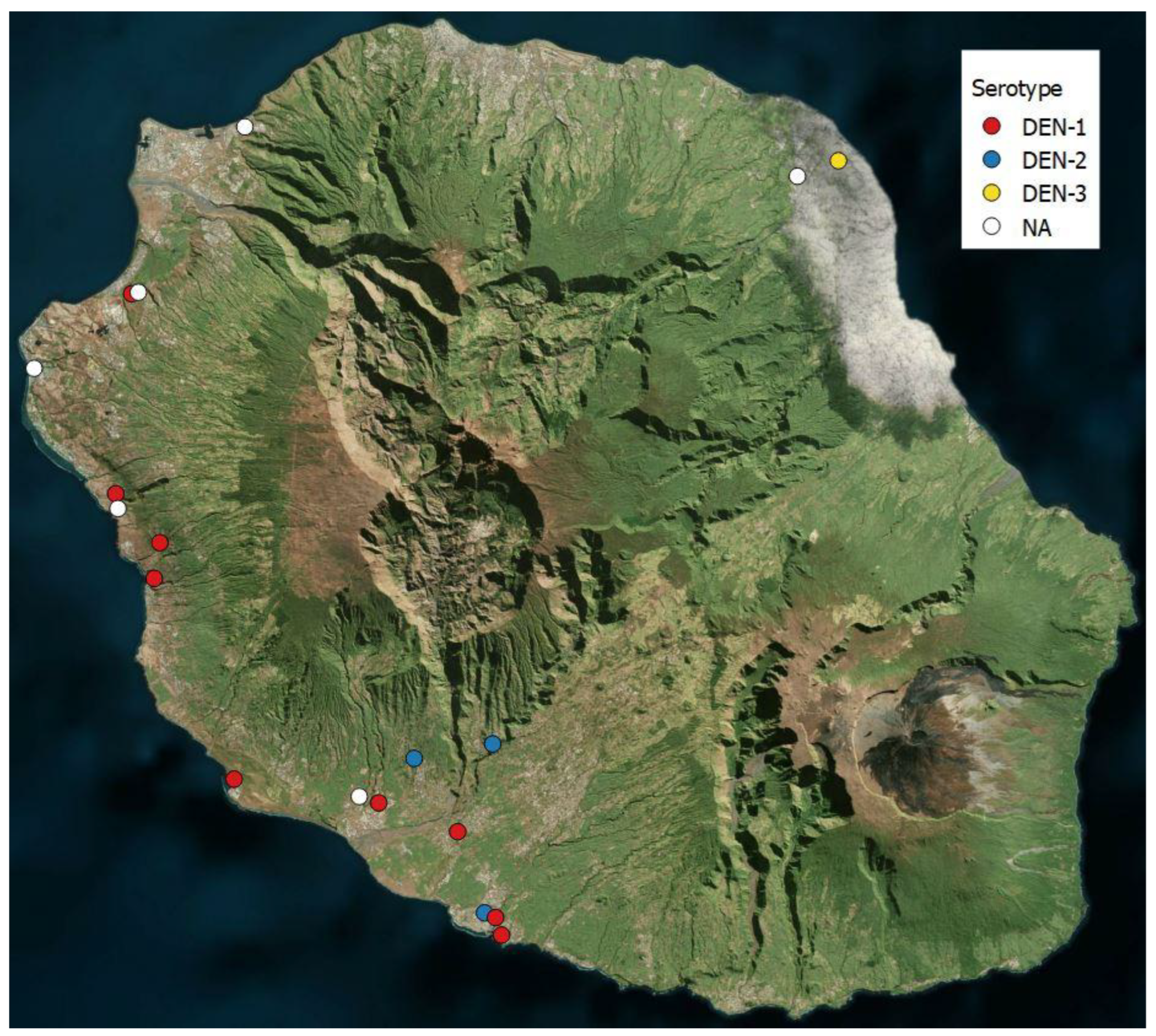
3.6. Dengue Serotypes
3.7. Clinical Presentation of Dengue RT-PCR Confirmed Infections
3.8. Detection of Anti-Dengue IgM and IgG Antibodies in Blood Samples
3.9. IgG Anti-Dengue Antibodies in Households
3.10. Risk Factors for Dengue Infection Confirmed by RT-PCR and Parameters Associated with Past Dengue Infection Detected by the Presence of Anti-Dengue IgG
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dengue and Severe Dengue. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 24 September 2022).
- Brady, O.J.; Gething, P.W.; Bhatt, S.; Messina, J.P.; Brownstein, J.S.; Hoen, A.G.; Moyes, C.L.; Farlow, A.W.; Scott, T.W.; Hay, S.I. Refining the Global Spatial Limits of Dengue Virus Transmission by Evidence-Based Consensus. PLoS Negl. Trop. Dis. 2012, 6, e1760. [Google Scholar] [CrossRef] [PubMed]
- Dash, A.P.; Bhatia, R.; Sunyoto, T.; Mourya, D.T. Emerging and Re-Emerging Arboviral Diseases in Southeast Asia. J. Vector Borne Dis. 2013, 50, 77–84. [Google Scholar] [PubMed]
- Gubler, D.J. Epidemic Dengue/Dengue Hemorrhagic Fever as a Public Health, Social and Economic Problem in the 21st Century. Trends Microbiol. 2002, 10, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Flahault, A. Emerging infectious diseases: The example of the Indian Ocean chikungunya outbreak (2005-2006). Bull. Acad. Natl. Méd. 2007, 191, 113–124; discussion 125–128. [Google Scholar] [PubMed]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The Global Distribution and Burden of Dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Coffeng, L.E.; Brady, O.J.; Hay, S.I.; Bedi, N.; Bensenor, I.M.; Castañeda-Orjuela, C.A.; et al. The Global Burden of Dengue: An Analysis from the Global Burden of Disease Study 2013. Lancet Infect. Dis. 2016, 16, 712–723. [Google Scholar] [CrossRef]
- Jaenisch, T.; Junghanss, T.; Wills, B.; Brady, O.J.; Eckerle, I.; Farlow, A.; Hay, S.I.; McCall, P.J.; Messina, J.P.; Ofula, V.; et al. Dengue Expansion in Africa—Not Recognized or Not Happening? Emerg. Infect. Dis. 2014, 20, 717. [Google Scholar] [CrossRef]
- Neumayr, A.; Muñoz, J.; Schunk, M.; Bottieau, E.; Cramer, J.; Calleri, G.; López-Vélez, R.; Angheben, A.; Zoller, T.; Visser, L.; et al. Sentinel Surveillance of Imported Dengue via Travellers to Europe 2012 to 2014: TropNet Data from the DengueTools Research Initiative. Eurosurveillance 2017, 22, 30433. [Google Scholar] [CrossRef]
- Amarasinghe, A.; Kuritsky, J.N.; Letson, G.W.; Margolis, H.S. Dengue Virus Infection in Africa. Emerg. Infect. Dis. 2011, 17, 1349–1354. [Google Scholar] [CrossRef]
- La Réunion—La France et Ses Territoires | Insee. Available online: https://www.insee.fr/fr/statistiques/5039941?sommaire=5040030 (accessed on 24 September 2022).
- Boyer, S.; Foray, C.; Dehecq, J.-S. Spatial and Temporal Heterogeneities of Aedes Albopictus Density in La Reunion Island: Rise and Weakness of Entomological Indices. PLoS ONE 2014, 9, e91170. [Google Scholar] [CrossRef]
- Kles, V.; Michault, A.; Rodhain, F.; Mevel, F.; Chastel, C. A serological survey regarding Flaviviridae infections on the island of Réunion (1971–1989). Bull. Soc. Pathol. Exot. 1990 1994, 87, 71–76. [Google Scholar]
- Michault, A. Insularity and epidemic risks in Réunion. Bull. Soc. Pathol. Exot. 1990 1998, 91, 52–55. [Google Scholar]
- Zeller, H.G. Dengue, arbovirus and migrations in the Indian Ocean. Bull. Soc. Pathol. Exot. 1990 1998, 91, 56–60. [Google Scholar]
- DiSera, L.; Sjödin, H.; Rocklöv, J.; Tozan, Y.; Súdre, B.; Zeller, H.; Muñoz, Á.G. The Mosquito, the Virus, the Climate: An Unforeseen Réunion in 2018. GeoHealth 2020, 4, e2020GH000253. [Google Scholar] [CrossRef] [PubMed]
- SPF Surveillance de la dengue à La Réunion. Point au 7 décembre 2021. Available online: https://www.santepubliquefrance.fr/regions/ocean-indien/documents/bulletin-regional/2021/surveillance-de-la-dengue-a-la-reunion.-point-au-7-decembre-2021 (accessed on 24 September 2022).
- Renault, P.; Solet, J.-L.; Sissoko, D.; Balleydier, E.; Larrieu, S.; Filleul, L.; Lassalle, C.; Thiria, J.; Rachou, E.; de Valk, H.; et al. A Major Epidemic of Chikungunya Virus Infection on Reunion Island, France, 2005–2006. Am. J. Trop. Med. Hyg. 2007, 77, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Grange, L.; Simon-Loriere, E.; Sakuntabhai, A.; Gresh, L.; Paul, R.; Harris, E. Epidemiological Risk Factors Associated with High Global Frequency of Inapparent Dengue Virus Infections. Front. Immunol. 2014, 5, 280. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Wang, M.; Shu, B.; Chen, X.; Luo, L.; Wang, J.; Cen, Y.; Anderson, B.D.; Merrill, M.M.; Merrill, H.R.; et al. Evaluation of Inapparent Dengue Infections during an Outbreak in Southern China. PLoS Negl. Trop. Dis. 2015, 9, e0003677. [Google Scholar] [CrossRef]
- Chikaki, E.; Ishikawa, H. A Dengue Transmission Model in Thailand Considering Sequential Infections with All Four Serotypes. J. Infect. Dev. Ctries. 2009, 3, 711–722. [Google Scholar] [CrossRef]
- Dengue—Chapter 4—2020 Yellow Book | Travelers’ Health | CDC. Available online: https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/dengue (accessed on 9 August 2021).
- WHO | Dengue. Available online: http://www.who.int/denguecontrol/en/ (accessed on 25 September 2016).
- Dussart, P.; Baril, L.; Petit, L.; Beniguel, L.; Quang, L.C.; Ly, S.; Azevedo, R.; do, S.S.; Meynard, J.-B.; Vong, S.; et al. Clinical and Virological Study of Dengue Cases and the Members of Their Households: The Multinational DENFRAME Project. PLoS Negl. Trop. Dis. 2012, 6, e1482. [Google Scholar] [CrossRef]
- Ly, S.; Fortas, C.; Duong, V.; Benmarhnia, T.; Sakuntabhai, A.; Paul, R.; Huy, R.; Sorn, S.; Nguon, K.; Chan, S.; et al. Asymptomatic Dengue Virus Infections, Cambodia, 2012–2013. Emerg. Infect. Dis. 2019, 25, 1354–1362. [Google Scholar] [CrossRef]
- Duong, V.; Lambrechts, L.; Paul, R.E.; Ly, S.; Lay, R.S.; Long, K.C.; Huy, R.; Tarantola, A.; Scott, T.W.; Sakuntabhai, A.; et al. Asymptomatic Humans Transmit Dengue Virus to Mosquitoes. Proc. Natl. Acad. Sci. USA 2015, 112, 14688–14693. [Google Scholar] [CrossRef] [PubMed]
- PAHO. Tool for the Diagnosis and Care of Patients with Suspected Arboviral Diseases; PAHO: Washington, DC, USA, 2017; ISBN 978-92-75-11936-5. [Google Scholar]
- WHO | Dengue Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition. Available online: http://www.who.int/rpc/guidelines/9789241547871/en/ (accessed on 4 July 2017).
- Guzman, M.G.; Gubler, D.J.; Izquierdo, A.; Martinez, E.; Halstead, S.B. Dengue Infection. Nat. Rev. Dis. Primer 2016, 2, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Chatchen, S.; Sabchareon, A.; Sirivichayakul, C. Serodiagnosis of Asymptomatic Dengue Infection. Asian Pac. J. Trop. Med. 2017, 10, 11–14. [Google Scholar] [CrossRef] [PubMed]
- García, G.; Sierra, B.; Pérez, A.B.; Aguirre, E.; Rosado, I.; Gonzalez, N.; Izquierdo, A.; Pupo, M.; Danay Díaz, D.R.; Sánchez, L.; et al. Asymptomatic Dengue Infection in a Cuban Population Confirms the Protective Role of the RR Variant of the FcγRIIa Polymorphism. Am. J. Trop. Med. Hyg. 2010, 82, 1153–1156. [Google Scholar] [CrossRef]
- Lacroix, R.; Delatte, H.; Hue, T.; Reiter, P. Dispersal and Survival of Male and Female Aedes Albopictus (Diptera: Culicidae) on Réunion Island. J. Med. Entomol. 2009, 46, 1117–1124. [Google Scholar] [CrossRef]
- Giry, C.; Roquebert, B.; Li-Pat-Yuen, G.; Gasque, P.; Jaffar-Bandjee, M.-C. Simultaneous Detection of Chikungunya Virus, Dengue Virus and Human Pathogenic Leptospira Genomes Using a Multiplex TaqMan® Assay. BMC Microbiol. 2017, 17, 105. [Google Scholar] [CrossRef]
- Légifrance—Publications Officielles—Journal Officiel—JORF N° 0277 Du 30/11/2006. Available online: https://www.legifrance.gouv.fr/download/pdf?id=REqL9dEa6zHzO_9B-g8NfXy_5j9RBhfoFzUoFVjb4G4= (accessed on 9 December 2022).
- Chien, Y.-W.; Liu, Z.-H.; Tseng, F.-C.; Ho, T.-C.; Guo, H.-R.; Ko, N.-Y.; Ko, W.-C.; Perng, G.C. Prolonged Persistence of IgM against Dengue Virus Detected by Commonly Used Commercial Assays. BMC Infect. Dis. 2018, 18, 156. [Google Scholar] [CrossRef]
- Burke, D.S.; Nisalak, A.; Johnson, D.E.; Scott, R.M. A Prospective Study of Dengue Infections in Bangkok. Am. J. Trop. Med. Hyg. 1988, 38, 172–180. [Google Scholar] [CrossRef]
- Pengsaa, K.; Limkittikul, K.; Yoksan, S.; Wisetsing, P.; Sabchareon, A. Dengue Antibody in Thai Children From Maternally Transferred Antibody to Acquired Infection. Pediatr. Infect. Dis. J. 2011, 30, 897–900. [Google Scholar] [CrossRef]
- Chau, T.N.B.; Hieu, N.T.; Anders, K.L.; Wolbers, M.; Le Bich, L.; Lu Thi Minh, H.; Hien, T.T.; Hung, N.T.; Farrar, J.; Whitehead, S.; et al. Dengue Virus Infections and Maternal Antibody Decay in a Prospective Birth Cohort Study of Vietnamese Infants. J. Infect. Dis. 2009, 200, 1893–1900. [Google Scholar] [CrossRef]
- da Cunha, R.V.; Dias, M.; Nogueira, R.M.; Chagas, N.; Miagostovich, M.P.; Schatzmayr, H.G. Secondary Dengue Infection in Schoolchildren in a Dengue Endemic Area in the State of Rio de Janeiro, Brazil. Rev. Inst. Med. Trop. Sao Paulo 1995, 37, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Endy, T.P.; Yoon, I.-K.; Mammen, M.P. Prospective Cohort Studies of Dengue Viral Transmission and Severity of Disease. In Dengue Virus; Rothman, A.L., Ed.; Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2010; pp. 1–13. ISBN 978-3-642-02214-2. [Google Scholar]
- Balmaseda, A.; Standish, K.; Mercado, J.C.; Matute, J.C.; Tellez, Y.; Saborío, S.; Hammond, S.N.; Nuñez, A.; Avilés, W.; Henn, M.R.; et al. Trends in Patterns of Dengue Transmission over Four Years of a Pediatric Cohort Study in Nicaragua. J. Infect. Dis. 2010, 201, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Capeding, R.Z.; Brion, J.D.; Caponpon, M.M.; Gibbons, R.V.; Jarman, R.G.; Yoon, I.-K.; Libraty, D.H. The Incidence, Characteristics, and Presentation of Dengue Virus Infections during Infancy. Am. J. Trop. Med. Hyg. 2010, 82, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Lamaurt, F.; De Santis, O.; Ramis, J.; Schultz, C.; Rivadeneyra, A.; Waelli, M.; Flahault, A. Knowledge, Attitudes, Beliefs, and Practices Regarding Dengue in La Réunion Island, France. Int. J. Environ. Res. Public Health 2022, 19, 4390. [Google Scholar] [CrossRef]
- Dossier Complet—Département de La Réunion (974) | Insee. Available online: https://www.insee.fr/fr/statistiques/2011101?geo=DEP-974 (accessed on 9 December 2022).




{kind=link}
{kind=link}
{kind=link}
| Date | Estimated Cases | Confirmed Cases | Death |
|---|---|---|---|
| 2018 | 15,460 | 6770 | 6 |
| 2019 | 42,420 | 18,217 | 14 |
| 2020 | 30,580 | 16,414 | 22 |
| 2021 | 59,230 | 29,577 | 33 |
| Cluster | Season [Month] | Location | Number of Participants | DENV RT-PCR+ | IgM + | IgG + | Serotype |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||||
| 1 | Winter [10] | South | 17 | 0 | 0 | 2 (12%) | DEN-2 |
| 2 | Summer [11] | South | 33 | 0 | 5 (15%) | 14 (42%) | DEN-2 |
| 3 | Summer [11] | South | 43 | 0 | 2 (5%) | 21 (49%) | DEN-1 |
| 4 | Summer [02] | South | 39 | 3 (8%) | 6 (15%) | 19 (49%) | DEN-1 |
| 5 | Summer [02] | South | 39 | 1 (3%) | 1 (3%) | 11 (28%) | DEN-2 |
| 6 | Summer [02] | South | 46 | 0 | 3 (7%) | 19 (41%) | DEN-1 |
| 7 | Summer [03] | East | 33 | 6 (18%) | 5 (15%) | 15 (45%) | DEN-3 |
| 8 | Summer [03] | East | 27 | 0 | 3 (11%) | 7 (26%) | NA |
| 9 | Summer [04] | South | 3 | 0 | 0 | 1 (33%) | DEN-1 |
| 10 | Winter [05] | South | 31 | 2 (6%) | 3 (10%) | 5 (16%) | DEN-1 |
| 11 | Winter [06] | South | 45 | 5 (11%) | 14 (31%) | 32 (71%) | NA |
| 12 | Winter [06] | West | 16 | 2 (12%) | 7 (44%) | 8 (50%) | DEN-1 |
| 13 | Winter [06] | West | 13 | 0 | 0 | 2 (15%) | DEN-1 |
| 14 | Winter [07] | West | 12 | 2 (17%) | 3 (25%) | 6 (50%) | NA |
| 15 | Winter [07] | West | 49 | 1 (2%) | 4 (8%) | 28 (57%) | NA |
| 16 | Winter [07] | West | 56 | 7 (13%) | 6 (11%) | 29 (52%) | DEN-1 |
| 17 | Winter [08] | West | 28 | 0 | 1 (4%) | 6 (21%) | DEN-1 |
| 18 | Winter [08] | West | 12 | 0 | 2 (17%) | 6 (50%) | NA |
| 19 | Winter [08] | West | 63 | 3 (5%) | 1 (2%) | 27 (43%) | NA |
| Total | 605 | 32 (5.3%) | 66 (11%) | 258 (43%) |
| Demographic Characteristics | Index Cases N = 17 | Participants N = 605 |
|---|---|---|
| Sex | ||
| Female | 11 (65%) | 346 (57%) |
| Male | 6 (35%) | 259 (43%) |
| Age mean (SD); median [IQR] | 36 (21); 36 [25] | 46 (20); 48 [30] |
| Age categories (years) | ||
| <5 | 1 (6%) | 5 (1%) |
| 5–11 | 3 (18%) | 36 (6%) |
| 12–17 | 0 | 39 (6%) |
| 18–59 | 11 (65%) | 340 (56%) |
| ≥60 | 2 (12%) | 185 (31%) |
| Activity | ||
| Housewife/husband or unemployed | 1 (6%) | 135 (22%) |
| Retired/Disabled | 1 (6%) | 160 (26%) |
| Student/in training | 4 (24%) | 93 (15%) |
| Worker | 11 (65%) | 205 (34%) |
| NA | 0 | 12 (2%) |
| Cluster no | Time Interval between the Date of Dengue Infection Confirmation and the Date of Inclusion in the Study [days] | Minimum Time Interval between Dengue Infections Dates in Each Cluster [days] | |
|---|---|---|---|
| IC | Participants | ||
| Cluster 01 | 4 | - | - |
| Cluster 02 | 8 | - | - |
| Cluster 03 | 7 | - | - |
| Cluster 04 | 10 | 0, 7, 9 | 0–9 |
| Cluster 05 | 12 | 13 | 0 |
| Cluster 06 | 11 | - | - |
| Cluster 07 | 13 * | 0, 12, 0, 10, 13, 36 | 0–23 |
| Cluster 08 | 14 | - | - |
| Cluster 09 | 0 & | - | - |
| Cluster 10 | 9 | 8, 25 | 4–7 |
| Cluster 11 | 13 | 22, 86, 84, 43, 68 | 3–19 |
| Cluster 12 | 5 | 22, 46 | 14–25 |
| Cluster 13 | 12 | - | - |
| Cluster 14 | 71 | 65 | 6 |
| Cluster 15 | NA µ | 36 | - |
| Cluster 16 | 31 | 57, 54, 54, 44, 45, 73, 64 | 1–14 |
| Cluster 17 | 13 | - | - |
| Cluster 18 | NA # | - | - |
| Cluster 19 | 30 | 81, 105, 9 | 15–29 |
| Explanatory Variables | Outcome | |||||
|---|---|---|---|---|---|---|
| RT-PCR DENV-Positive | IgG-Positive | |||||
| OR # | 95%CI | p-Value | OR # | 95%CI | p-Value | |
| Age categories | 0.3 | >0.9 | ||||
| Sex | >0.9 | 0.7 | ||||
| Body mass index (BMI) categories | 0.3 | 0.3 | ||||
| Duration of stay home ≥ 20 h a day | 0.5 | 2.78 | 1.7-4.7 | <0.001 | ||
| Activity: student/in training | 0.2 | 0.3 | 0.2–0.5 | <0.001 | ||
| History of dengue | 28 | 8.8–144 | <0.001 | 7.5 | 5–11.5 | <0.001 |
| History of chikungunya | 0.8 | 3.7 | 2.6–5.5 | <0.001 | ||
| Level of education | ||||||
| Never attended school | 0.5 | 5.2 | 1.5–23.9 | 0.015 | ||
| Primary school | >0.9 | 2 | 1.2–3.4 | 0.005 | ||
| Secondary school | 0.5 | 1.6 | 1.1–2.5 | 0.031 | ||
| High school | 0.13 | 0.8 | 0.2 | |||
| Yellow fever vaccination | 0.6 | 0.11 | ||||
| Smoking | 0.09 | 0.002–0.6 | 0.001 | 0.8 | ||
| Risky drinking $ | 0.6 | 1.2 | 0.4–4.2 | 0.017 | ||
| Chronic disease | 0.11 | 1.4 | 1–2 | 0.04 | ||
| Chronic medication | 0.7 | 1.5 | 1.1–2.1 | 0.017 | ||
| Sense of severity | 0.2 | 0.7 | ||||
| Sense of risk & | 0.5 | 0.2 | ||||
| Mosquito protection use ¥ | 0.8 | 0.8 | ||||
| Mosquito bites α | 0.4 | 0.11 | ||||
| Mosquito presence | 0.2 | 0.074 | ||||
| Season | 0.2 | 0.2 | ||||
| House with courtyard | 0.2 | 4.6 | 2.4–9.9 | <0.001 | ||
| Type of courtyard | >0.9 | 0.2–0.9 | ||||
| Surface of courtyard | ||||||
| 100–500 square meters | 0.5 | 1.8 | 1.2–2.6 | 0.004 | ||
| >500 square meters | 0.5 | 2 | 1.3–3 | 0.003 | ||
| Earthen courtyard floor | 2.1 | 1–4.4 | 0.032 | 1.8 | 1.2–2.9 | 0.009 |
| Presence of grass | 0.3 | 1.5 | 1–2.1 | 0.04 | ||
| Presence of windows with glasses | 0.5 | 0.2–1 | 0.032 | 0.5 | 0.3–0.9 | 0.007 |
| Presence of air conditioning | 0.6 | 0.6 | 0.5–1 | 0.032 | ||
| Presence of swimming-pool | >0.9 | 0.3 | 0.1–0.8 | 0.007 | ||
| Presence of stagnant water | 0.7 | 0.6 | ||||
| Presence of animals | 0.8 | 1.9 | 1–3.4 | 0.028 | ||
| Presence of poultry | 0.076 | 2 | 1.3–3.2 | 0.001 | ||
| Presence of rubbish in the courtyard | >0.9 | 0.12 | ||||
| Presence of rubbish in the surrounding area | 1.8 | 0.9–3.5 | 0.043 | 1.8 | 1.2–2.6 | 0.002 |
| Orchard in the surrounding area | 0.12 | 0.8 | ||||
| Banana plantation in the surrounding area | >0.9 | 0 | 0–0.4 | 0.002 | ||
| Sugarcane plantation in the surrounding area | 0.4 | 0.14 | ||||
| Other agriculture in the surrounding area | 0.2 | 0.12 | ||||
| Farm in the surrounding area | 5.6 | 1.5–17.9 | 0.006 | 0.051 | ||
| Seaside | 0.6 | 0.2 | ||||
| Industrial area | >0.9 | 0.4 | ||||
| Neighborhood of houses | 0.8 | 1.7 | 1.2–2.6 | 0.003 | ||
| Neighborhood of buildings | 0.6 | 0.5 | 0.3–0.8 | 0.003 | ||
| Explanatory Variables | aOR | 95%CI | p-Value |
|---|---|---|---|
| Outcome: RT-PCR DENV-positive | |||
| Smoking | 0.08 | 0.0–0.4 | 0.02 |
| Earthen courtyard floor | 2.1 | 1–4.3 | 0.046 |
| Farm in the surrounding area | 5.5 | 1.6–16.9 | 0.005 |
| Presence of rubbish in the surrounding area | 1.6 | 0.3–1.12 | 0.20 |
| Presence of windows with glasses | 0.5 | 0.8–3.1 | 0.09 |
| Outcome: IgG anti-dengue-positive | |||
| History of chikungunya | 2.5 | 1.6–3.9 | <0.001 |
| Type of housing: house with courtyard | 5.3 | 2.2–14 | <0.001 |
| Presence of rubbish in the surrounding area | 1.6 | 1.1–2.6 | 0.04 |
| Duration of stay home ≥ 20 h a day | 1.7 | 0.9–3.3 | 0.15 |
| Activity: student/in training | 0.4 | 0.1–1.7 | 0.30 |
| Level of education | 0.07 | ||
| Never attended school | 2.2 | 0.5–15.9 | |
| Primary school | 1.6 | 0.7–3.6 | |
| Secondary school | 0.9 | 0.6–1.8 | |
| High school | 0.6 | 0.3–1.1 | |
| Surface of courtyard | 0.26 | ||
| 100–500 square meters | 1.02 | 0.6–1.8 | |
| >500 square meters | 1.5 | 0.8–2.9 | |
| Earthen courtyard floor | 1.4 | 0.8–2.5 | 0.21 |
| Presence of windows with glasses | 1.04 | 0.6–1.9 | 0.89 |
| Presence of swimming-pool | 0.7 | 0.3–1.7 | 0.44 |
| Presence of poultry | 0.9 | 0.5–1.6 | 0.81 |
| Neighborhood of houses | 0.8 | 0.4–1.3 | 0.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Santis, O.; Pothin, E.; Bouscaren, N.; Irish, S.R.; Jaffar-Bandjee, M.-C.; Menudier, L.; Ramis, J.; Schultz, C.; Lamaurt, F.; Wisniak, A.; et al. Investigation of Dengue Infection in Asymptomatic Individuals during a Recent Outbreak in La Réunion. Viruses 2023, 15, 742. https://doi.org/10.3390/v15030742
De Santis O, Pothin E, Bouscaren N, Irish SR, Jaffar-Bandjee M-C, Menudier L, Ramis J, Schultz C, Lamaurt F, Wisniak A, et al. Investigation of Dengue Infection in Asymptomatic Individuals during a Recent Outbreak in La Réunion. Viruses. 2023; 15(3):742. https://doi.org/10.3390/v15030742
Chicago/Turabian StyleDe Santis, Olga, Emilie Pothin, Nicolas Bouscaren, Seth R. Irish, Marie-Christine Jaffar-Bandjee, Luce Menudier, Julie Ramis, Cédric Schultz, Florence Lamaurt, Ania Wisniak, and et al. 2023. "Investigation of Dengue Infection in Asymptomatic Individuals during a Recent Outbreak in La Réunion" Viruses 15, no. 3: 742. https://doi.org/10.3390/v15030742
APA StyleDe Santis, O., Pothin, E., Bouscaren, N., Irish, S. R., Jaffar-Bandjee, M.-C., Menudier, L., Ramis, J., Schultz, C., Lamaurt, F., Wisniak, A., Bertolotti, A., Hafsia, S., Dussart, P., Baril, L., Mavingui, P., & Flahault, A. (2023). Investigation of Dengue Infection in Asymptomatic Individuals during a Recent Outbreak in La Réunion. Viruses, 15(3), 742. https://doi.org/10.3390/v15030742