
Direct-Acting Antivirals Reduce the De Novo Development of Esophageal Varices in Patients with Hepatitis C Virus Related Liver Cirrhosis
 , , , , , , , ,
, , , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
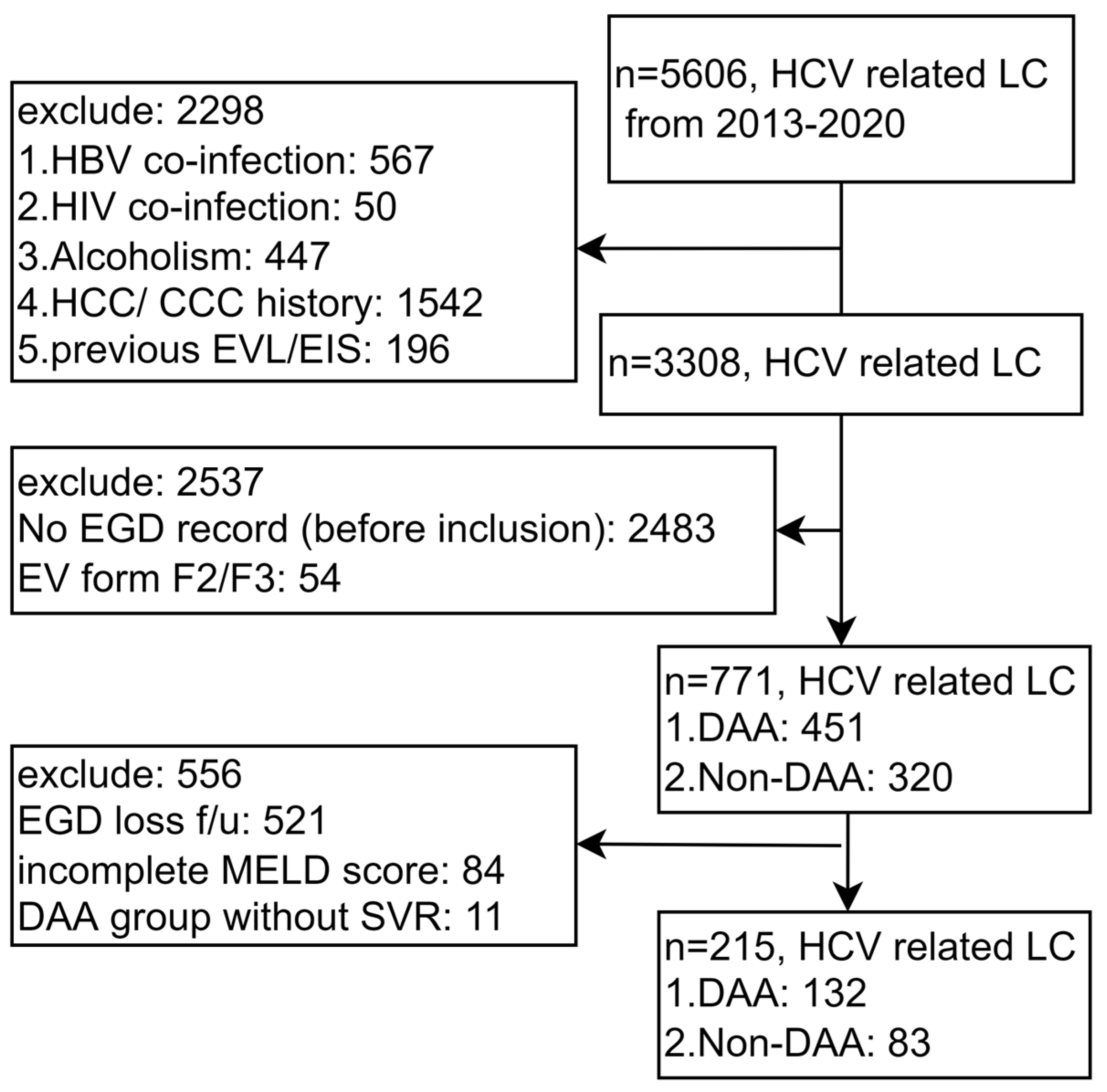
2.1. Case Enrollment and Data Organization
2.2. EV and Endoscopy Criteria
2.3. EV Occurrence/Progression
2.4. SVR in the DAA Group
2.5. Statistical Analysis
3. Results
3.1. Baseline Case Characteristics
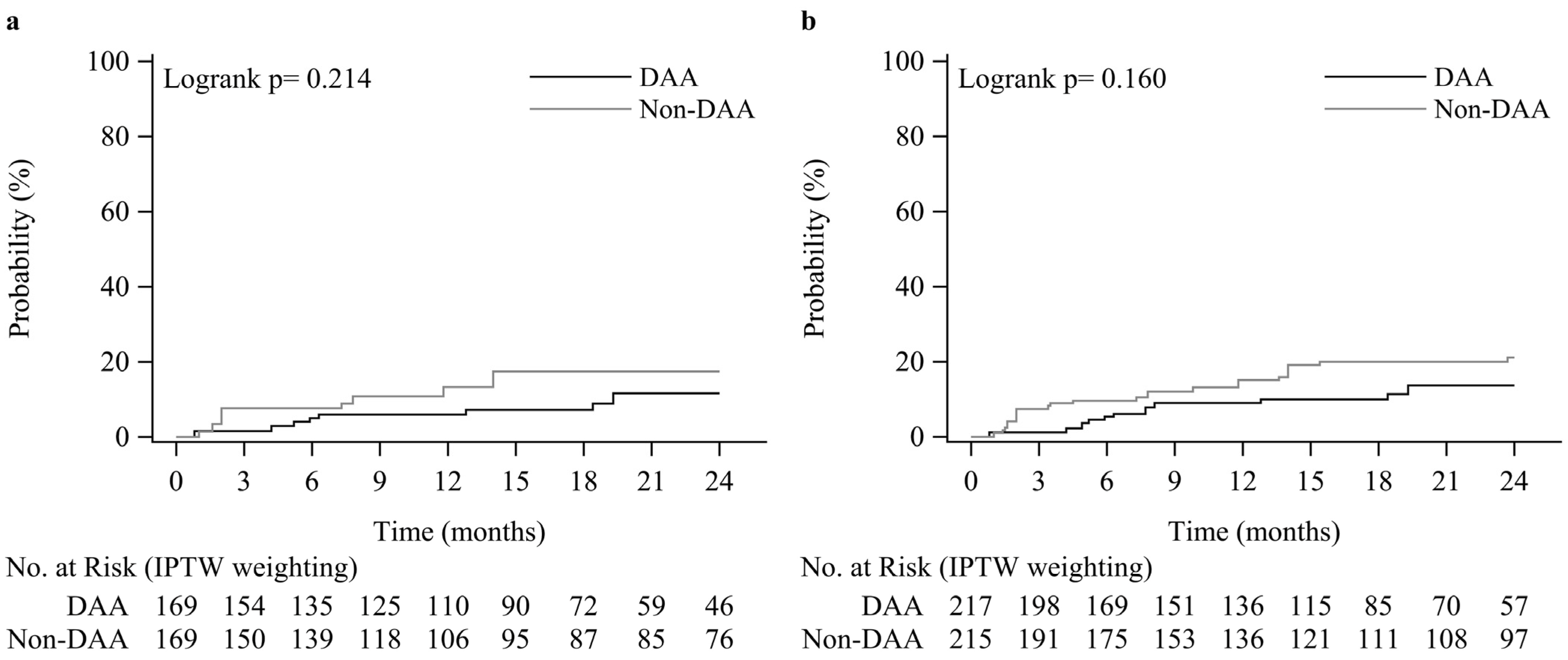
3.2. Association between DAA and EV Occurrence/Progression
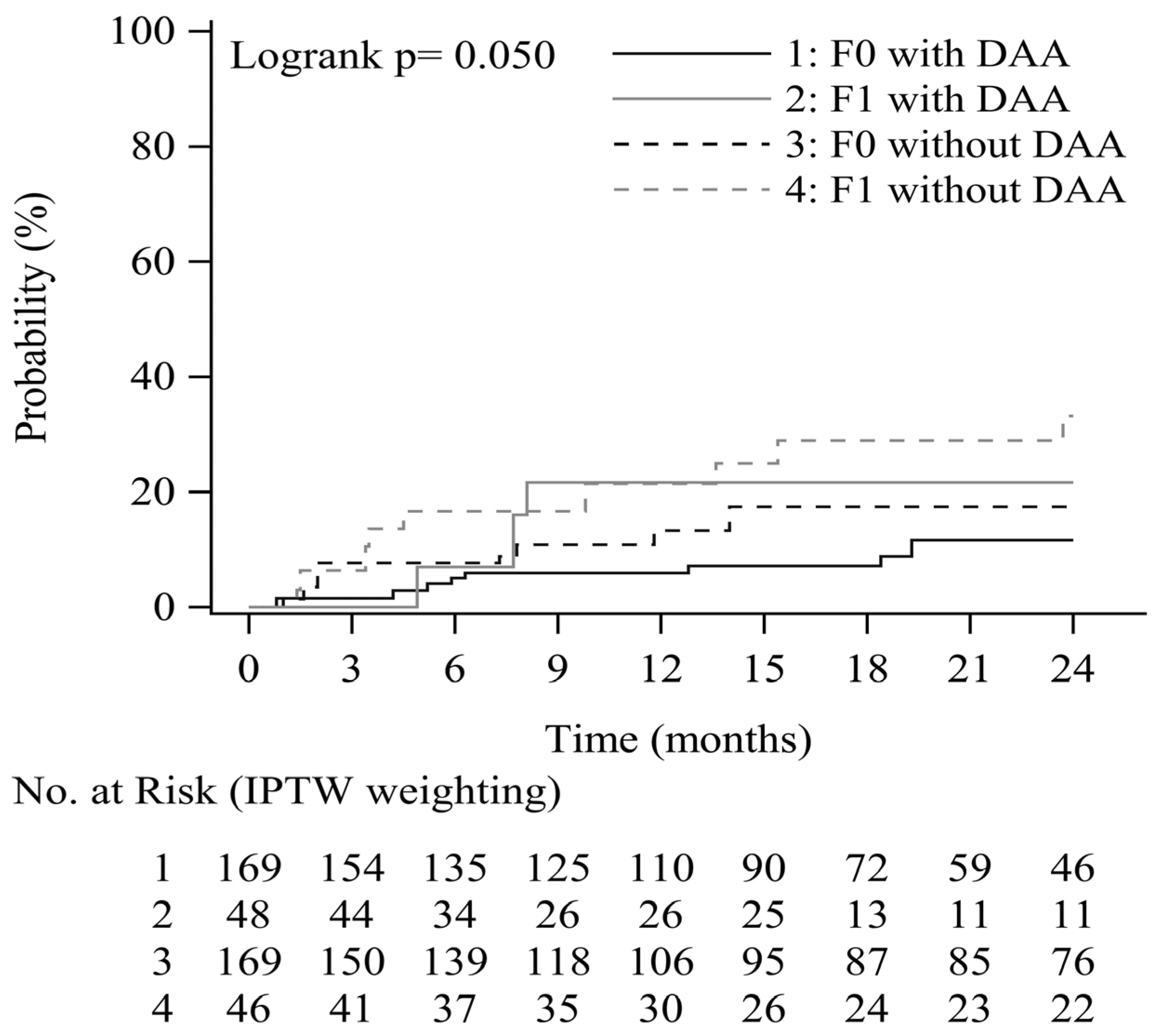
3.3. Progression of EV as a Function of DAA and Baseline EV Form
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruno, S.; Zuin, M.; Crosignani, A.; Rossi, S.; Zadra, F.; Roffi, L.; Borzio, M.; Redaelli, A.; Chiesa, A.; Silini, E.M.; et al. Predicting mortality risk in patients with compensated HCV-induced cirrhosis: A long-term prospective study. Am. J. Gastroenterol. 2009, 104, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Christensen, E.; Fauerholdt, L.; Schlichting, P.; Juhl, E.; Poulsen, H.; Tygstrup, N. Aspects of the natural history of gastrointestinal bleeding in cirrhosis and the effect of prednisone. Gastroenterology 1981, 81, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Bosch, J. Management of varices and variceal hemorrhage in cirrhosis. N. Engl. J. Med. 2010, 362, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Carbonell, N.; Pauwels, A.; Serfaty, L.; Fourdan, O.; Levy, V.G.; Poupon, R. Improved survival after variceal bleeding in patients with cirrhosis over the past two decades. Hepatology 2004, 40, 652–659. [Google Scholar] [CrossRef]
- Bruno, S.; Crosignani, A.; Facciotto, C.; Rossi, S.; Roffi, L.; Redaelli, A.; de Franchis, R.; Almasio, P.L.; Maisonneuve, P. Sustained virologic response prevents the development of esophageal varices in compensated, Child-Pugh class A hepatitis C virus-induced cirrhosis. A 12-year prospective follow-up study. Hepatology 2010, 51, 2069–2076. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.H.; Pwu, R.F.; Chen, S.C. Achieving hepatitis C elimination in Taiwan-Overcoming barriers by setting feasible strategies. J. Formos Med. Assoc. 2018, 117, 1044–1045. [Google Scholar] [CrossRef]
- Huang, Y.T.; Hsieh, Y.Y.; Chen, W.M.; Tung, S.Y.; Wei, K.L.; Shen, C.H.; Chang, K.C.; Lu, C.K.; Yen, C.W.; Lu, S.N.; et al. Sofosbuvir/velpatasvir is an effective treatment for patients with hepatitis C and advanced fibrosis or cirrhosis in a real-world setting in Taiwan. BMC Gastroenterol. 2021, 21, 259. [Google Scholar] [CrossRef]
- Chang, K.C.; Tung, S.Y.; Wei, K.L.; Shen, C.H.; Hsieh, Y.Y.; Chen, W.M.; Chen, Y.H.; Chen, C.H.; Yen, C.W.; Xu, H.W.; et al. Real-world efficacy and safety of pangenotypic direct-acting antivirals against hepatitis C virus infection in Taiwan. Sci. Rep. 2021, 11, 13543. [Google Scholar] [CrossRef]
- Lens, S.; Alvarado-Tapias, E.; Marino, Z.; Londono, M.C.; Enrique, L.L.; Martinez, J.; Fortea, J.I.; Ibanez, L.; Ariza, X.; Baiges, A.; et al. Effects of All-Oral Anti-Viral Therapy on HVPG and Systemic Hemodynamics in Patients with Hepatitis C Virus-Associated Cirrhosis. Gastroenterology 2017, 153, 1273–1283. [Google Scholar] [CrossRef]
- Lens, S.; Baiges, A.; Alvarado-Tapias, E.; Enrique, L.L.; Martinez, J.; Fortea, J.I.; Ibanez-Samaniego, L.; Marino, Z.; Rodriguez-Tajes, S.; Gallego, A.; et al. Clinical outcome and hemodynamic changes following HCV eradication with oral antiviral therapy in patients with clinically significant portal hypertension. J. Hepatol. 2020, 73, 1415–1424. [Google Scholar] [CrossRef]
- Mandorfer, M.; Kozbial, K.; Schwabl, P.; Chromy, D.; Semmler, G.; Stattermayer, A.F.; Pinter, M.; Hernandez-Gea, V.; Fritzer-Szekeres, M.; Steindl-Munda, P.; et al. Changes in Hepatic Venous Pressure Gradient Predict Hepatic Decompensation in Patients Who Achieved Sustained Virologic Response to Interferon-Free Therapy. Hepatology 2020, 71, 1023–1036. [Google Scholar] [CrossRef] [PubMed]
- Moon, A.M.; Green, P.K.; Rockey, D.C.; Berry, K.; Ioannou, G.N. Hepatitis C eradication with direct-acting anti-virals reduces the risk of variceal bleeding. Aliment. Pharmacol. Ther. 2020, 51, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.C.; Chan, Y.Y.; Kao Yang, Y.H.; Lin, S.J.; Hung, M.J.; Chien, R.N.; Lai, C.C.; Lai, E.C. The Chang Gung Research Database-A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Changchien, C.S.; Hung, C.H.; Eng, H.L.; Tung, W.C.; Kee, K.M.; Chen, C.H.; Hu, T.H.; Lee, C.M.; Lu, S.N. FibroScan and ultrasonography in the prediction of hepatic fibrosis in patients with chronic viral hepatitis. J. Gastroenterol. 2009, 44, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Friedrich-Rust, M.; Nierhoff, J.; Lupsor, M.; Sporea, I.; Fierbinteanu-Braticevici, C.; Strobel, D.; Takahashi, H.; Yoneda, M.; Suda, T.; Zeuzem, S.; et al. Performance of Acoustic Radiation Force Impulse imaging for the staging of liver fibrosis: A pooled meta-analysis. J. Viral Hepat. 2012, 19, e212–e219. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.Y.; Sheen, I.S.; Chiu, C.T.; Lin, S.M.; Kuo, Y.C.; Liaw, Y.F. Ultrasonographic changes of early liver cirrhosis in chronic hepatitis B: A longitudinal study. J. Clin. Ultrasound 1993, 21, 303–308. [Google Scholar] [CrossRef]
- Moon, K.M.; Kim, G.; Baik, S.K.; Choi, E.; Kim, M.Y.; Kim, H.A.; Cho, M.Y.; Shin, S.Y.; Kim, J.M.; Park, H.J.; et al. Ultrasonographic scoring system score versus liver stiffness measurement in prediction of cirrhosis. Clin. Mol. Hepatol. 2013, 19, 389–398. [Google Scholar] [CrossRef]
- North Italian Endoscopic Club for the, S.; Treatment of Esophageal, V. Prediction of the first variceal hemorrhage in patients with cirrhosis of the liver and esophageal varices. A prospective multicenter study. N. Engl. J. Med. 1988, 319, 983–989. [Google Scholar] [CrossRef]
- Ghany, M.G.; Morgan, T.R.; AASLD-IDSA Hepatitis C Guidance Panel. Hepatitis C guidance 2019 update: American Association for the Study of Liver Diseases–Infectious Diseases Society of America recommendations for testing, managing, and treating hepatitis C virus infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [PubMed]
- Hernan, M.A.; Robins, J.M. Using Big Data to Emulate a Target Trial When a Randomized Trial Is Not Available. Am. J. Epidemiol. 2016, 183, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Backus, L.I.; Belperio, P.S.; Shahoumian, T.A.; Mole, L.A. Impact of Sustained Virologic Response with Direct-Acting Antiviral Treatment on Mortality in Patients with Advanced Liver Disease. Hepatology 2019, 69, 487–497. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Fontana, R.J.; Di Bisceglie, A.M.; Everhart, J.E.; Doherty, M.C.; Everson, G.T.; Donovan, J.A.; Malet, P.F.; Mehta, S.; Sheikh, M.Y.; et al. The prevalence and risk factors associated with esophageal varices in subjects with hepatitis C and advanced fibrosis. Gastrointest. Endosc. 2006, 64, 855–864. [Google Scholar] [CrossRef]
- Rockey, D.C. Fibrosis reversal after hepatitis C virus elimination. Curr. Opin. Gastroenterol. 2019, 35, 137–144. [Google Scholar] [CrossRef]
- Pawlotsky, J.M.; Germanidis, G.; Neumann, A.U.; Pellerin, M.; Frainais, P.O.; Dhumeaux, D. Interferon resistance of hepatitis C virus genotype 1b: Relationship to nonstructural 5A gene quasispecies mutations. J. Virol. 1998, 72, 2795–2805. [Google Scholar] [CrossRef] [PubMed]
- Qamar, A.A.; Grace, N.D.; Groszmann, R.J.; Garcia-Tsao, G.; Bosch, J.; Burroughs, A.K.; Maurer, R.; Planas, R.; Escorsell, A.; Garcia-Pagan, J.C.; et al. Platelet count is not a predictor of the presence or development of gastroesophageal varices in cirrhosis. Hepatology 2008, 47, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Garcia-Tsao, G.; Bosch, J.; Grace, N.D.; Burroughs, A.K.; Morillas, R.; Escorsell, A.; Garcia-Pagan, J.C.; Patch, D.; Matloff, D.S.; et al. Obesity is an independent risk factor for clinical decompensation in patients with cirrhosis. Hepatology 2011, 54, 555–561. [Google Scholar] [CrossRef]
- Hammerstad, S.S.; Grock, S.F.; Lee, H.J.; Hasham, A.; Sundaram, N.; Tomer, Y. Diabetes and Hepatitis C: A Two-Way Association. Front. Endocrinol. 2015, 6, 134. [Google Scholar] [CrossRef]
- Romero-Gomez, M.; Del Mar Viloria, M.; Andrade, R.J.; Salmeron, J.; Diago, M.; Fernandez-Rodriguez, C.M.; Corpas, R.; Cruz, M.; Grande, L.; Vazquez, L.; et al. Insulin resistance impairs sustained response rate to peginterferon plus ribavirin in chronic hepatitis C patients. Gastroenterology 2005, 128, 636–641. [Google Scholar] [CrossRef]
- Khan, M.S.; Majeed, A.; Ghauri, F. Comparison of carvedilol and esophageal variceal band ligation for prevention of variceal bleed among cirrhotic patients. Age Years 2017, 52, 54.07–54.54. [Google Scholar]
- Kristiansson, P.; Wang, J.X. Reproductive hormones and blood pressure during pregnancy. Hum. Reprod. 2001, 16, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Beebe-Dimmer, J.L.; Pfeifer, J.R.; Engle, J.S.; Schottenfeld, D. The epidemiology of chronic venous insufficiency and varicose veins. Ann. Epidemiol. 2005, 15, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Abraldes, J.G.; Berzigotti, A.; Bosch, J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017, 65, 310–335. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, A.; Kedarisetty, C.K.; Vashishtha, C.; Bhadoria, A.S.; Jindal, A.; Kumar, G.; Choudhary, A.; Shasthry, S.M.; Maiwall, R.; Kumar, M.; et al. Carvedilol delays the progression of small oesophageal varices in patients with cirrhosis: A randomised placebo-controlled trial. Gut 2017, 66, 1838–1843. [Google Scholar] [CrossRef]
- Qi, X.S.; Bao, Y.X.; Bai, M.; Xu, W.D.; Dai, J.N.; Guo, X.Z. Nonselective beta-blockers in cirrhotic patients with no or small varices: A meta-analysis. World J. Gastroenterol. 2015, 21, 3100–3108. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Unweighted Sample, No. | SMD | IPTW † Sample | SMD | ||||
|---|---|---|---|---|---|---|---|---|
| DAA | Non-DAA | DAA | Non-DAA | |||||
| (n = 132) | (n = 83) | (n = 217) | (n = 215) | |||||
| Sex | 0.033 | −0.057 | ||||||
| Female | 69 | (52.3%) | 42 | (50.6%) | 50.7% | 53.5% | ||
| Male | 63 | (47.7%) | 41 | (49.4%) | 49.3% | 46.5% | ||
| Age (years) | ||||||||
| Mean (±SD) | 64.8 | (±10.3) | 61.0 | (±9.7) | 0.378 | 63.2 | 63.5 | −0.026 |
| Comorbidity | ||||||||
| Diabetes | 55 | (41.7%) | 38 | (45.8%) | −0.083 | 43.9% | 43.3% | 0.013 |
| Dyslipidemia | 42 | (31.8%) | 23 | (27.7%) | 0.090 | 32.2% | 29.1% | 0.067 |
| Arterial hypertension | 76 | (57.6%) | 47 | (56.6%) | −0.019 | 58.7% | 57.0% | 0.035 |
| Obesity | 6 | (4.6%) | 7 | (8.4%) | −0.158 | 6.0% | 5.7% | 0.009 |
| Use of non-carvedilol beta blockers | 8 | (6.1%) | 4 | (4.8%) | 0.055 | 6.1% | 6.9% | −0.033 |
| Baseline EV form | 0.509 | −0.002 | ||||||
| F0 | 115 | (87.1%) | 55 | (66.3%) | 78.0% | 78.8% | ||
| F1 | 17 | (12.9%) | 28 | (33.7%) | 22.0% | 21.2% | ||
| Genotype | 0.127 | −0.030 | ||||||
| 1b | 64 | (48.5%) | 35 | (42.2%) | 47.7% | 49.2% | ||
| Non-1b | 68 | (51.5%) | 48 | (57.8%) | 52.3% | 50.8% | ||
| Platelets (1000/mL) | −0.397 | −0.016 | ||||||
| <150 | 54 | (40.9%) | 48 | (57.8%) | 49.3% | 49.3% | ||
| ≥150 | 78 | (59.1%) | 35 | (42.2%) | 50.7% | 50.7% | ||
| MELD score | ||||||||
| Mean (±SD) | 6.8 | (±6.6) | 7.1 | (±6.1) | 0.343 | 7.3 | 7.0 | 0.000 |
| Median (25–75% quartiles) | 5 | (3–7) | 5 | (3–9) | ||||
| Outcomes | ||||||||
| EV occurrence ‡ | 8 | (7.0%) | 7 | (12.7%) | −0.195 | 8.0% | 14.6% | −0.208 |
| EV progression | 11 | (8.3%) | 16 | (19.3%) | −0.321 | 9.7% | 17.7% | −0.233 |
| Variables | Unweighted Sample | IPTW Sample | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude HR | Adjusted HR | Crude HR | Adjusted HR | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Sex | ||||||||
| Female | 5.83 (1.31–25.8) | 0.020 | 7.67 (1.41–41.8) | 0.019 | 11.8 (3.42–40.6) | 0.001 | 22.5 (5.58–91.1) | <0.001 |
| Male | 1 | 1 | 1 | 1 | ||||
| Age (linear) † | 1.55 (0.91–2.65) | 0.108 | 1.51 (0.73–3.14) | 0.268 | 1.83 (1.31–2.56) | <0.001 | 1.35 (0.85–2.15) | 0.205 |
| Comorbidity | ||||||||
| Diabetes | 2.69 (0.92–7.87) | 0.071 | 1.89 (0.51–7.05) | 0.341 | 2.14 (1.12–4.10) | 0.022 | 1.63 (0.67–3.97) | 0.279 |
| Dyslipidemia | 0.75 (0.24–2.36) | 0.623 | 0.63 (0.17–2.34) | 0.488 | 0.88 (0.44–1.77) | 0.726 | 0.61 (0.26–1.44) | 0.262 |
| Arterial hypertension | 1.42 (0.48–4.15) | 0.524 | 0.82 (0.21–3.22) | 0.774 | 2.59 (1.21–5.53) | 0.014 | 2.28 (0.88–5.87) | 0.088 |
| Obesity | 2.43 (0.56–10.8) | 0.242 | 2.03 (0.33–12.7) | 0.448 | 2.05 (0.73–5.79) | 0.176 | 1.32 (0.38–4.52) | 0.661 |
| Use of non-carvedilol beta blockers | 2.28 (0.51–10.1) | 0.279 | 1.34 (0.25–7.03) | 0.732 | 1.74 (0.66–4.59) | 0.262 | 0.95 (0.32–2.78) | 0.920 |
| Genotype | ||||||||
| 1b | 0.77 (0.27–2.15) | 0.612 | 0.64 (0.21–1.95) | 0.429 | 0.82 (0.44–1.56) | 0.554 | 0.73 (0.35–1.52) | 0.402 |
| Non-1b | 1 | 1 | 1 | 1 | ||||
| Platelets (103/μL) | ||||||||
| <150 | 2.44 (0.83–7.15) | 0.104 | 1.33 (0.39–4.55) | 0.655 | 1.35 (0.72–2.55) | 0.355 | 1.76 (0.36–1.64) | 0.489 |
| ≥150 | 1 | 1 | 1 | 1 | ||||
| MELD score (linear) a | 1.03 (0.97–1.10) | 0.322 | 1.08 (0.99–1.17) | 0.053 | 1.01 (0.97–1.06) | 0.569 | 1.08 (1.02–1.14) | 0.006 |
| Treatment | ||||||||
| DAA | 0.58 (0.21–1.60) | 0.294 | 0.57 (0.19–1.73) | 0.324 | 0.56 (0.29–1.09) | 0.089 | 0.47 (0.24–0.93) | 0.030 |
| Non-DAA | 1 | 1 | 1 | 1 | ||||
| Variables | Unweighted Sample | IPTW Sample | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude HR | Adjusted HR | Crude HR | Adjusted HR | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Sex | ||||||||
| Female | 2.85 (1.21–6.74) | 0.017 | 4.35 (1.53–12.4) | 0.006 | 3.83 (2.04–7.22) | <0.001 | 6.53 (2.98–14.3) | <0.001 |
| Male | 1 | 1 | 1 | 1 | ||||
| Age (linear) † | 1.08 (0.74–1.58) | 0.676 | 0.81 (0.49–1.33) | 0.403 | 1.31 (1.01–1.69) | 0.044 | 0.93 (0.67–1.29) | 0.645 |
| Comorbidity | ||||||||
| Diabetes | 1.50 (0.71–3.20) | 0.291 | 1.61 (0.69–3.74) | 0.267 | 1.68 (1.00–2.80) | 0.048 | 2.23 (1.21–4.13) | 0.010 |
| Dyslipidemia | 0.42 (0.14–1.20) | 0.106 | 0.59 (0.18–1.93) | 0.380 | 0.56 (0.30–1.08) | 0.082 | 0.54 (0.26–1.12) | 0.099 |
| Arterial hypertension | 1.17 (0.54–2.53) | 0.687 | 1.62 (0.63–4.21) | 0.319 | 1.80 (1.04–3.13) | 0.037 | 2.48 (1.31–4.71) | 0.006 |
| Obesity | 1.29 (0.31–5.45) | 0.729 | 1.03 (0.20–5.33) | 0.974 | 1.18 (0.43–3.27) | 0.747 | 0.84 (0.27–2.58) | 0.754 |
| Use of non-carvedilol beta blockers | 2.94 (1.02–8.52) | 0.047 | 3.30 (0.95–11.4) | 0.061 | 2.74 (1.37–5.48) | 0.004 | 2.18 (1.00–4.76) | 0.051 |
| Baseline EV form | ||||||||
| F0 | 1 | 1 | 1 | 1 | ||||
| F1 | 3.02 (1.41–6.45) | 0.004 | 3.62 (1.51–8.71) | 0.004 | 2.07 (1.21–3.53) | 0.008 | 3.12 (1.72–5.67) | <0.001 |
| Genotype | ||||||||
| 1b | 0.67 (0.31–1.47) | 0.318 | 0.73 (0.31–1.72) | 0.475 | 0.80 (0.48–1.33) | 0.384 | 1.07 (0.60–1.91) | 0.810 |
| Non-1b | 1 | 1 | 1 | 1 | ||||
| Platelets (103/μL) | ||||||||
| <150 | 2.57 (1.12–5.87) | 0.025 | 1.96 (0.80–4.79) | 0.141 | 1.41 (0.84–2.37) | 0.189 | 0.93 (0.53–1.66) | 0.813 |
| ≥150 | 1 | 1 | 1 | 1 | ||||
| MELD score (linear) a | 1.02 (0.96–1.07) | 0.546 | 1.05 (0.99–1.12) | 0.119 | 1.00 (0.96–1.04) | 0.942 | 1.02 (0.98–1.07) | 0.299 |
| Treatment | ||||||||
| DAA | 0.46 (0.21–0.98) | 0.045 | 0.69 (0.30–1.60) | 0.391 | 0.57 (0.34–0.98) | 0.040 | 0.55 (0.32–0.95) | 0.033 |
| Non-DAA | 1 | 1 | 1 | 1 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, Y.-Y.; Chen, W.-M.; Chang, K.-C.; Chang, T.-S.; Hung, C.-H.; Yang, Y.-H.; Tung, S.-Y.; Wei, K.-L.; Shen, C.-H.; Wu, C.-S.; et al. Direct-Acting Antivirals Reduce the De Novo Development of Esophageal Varices in Patients with Hepatitis C Virus Related Liver Cirrhosis. Viruses 2023, 15, 252. https://doi.org/10.3390/v15010252
Hsieh Y-Y, Chen W-M, Chang K-C, Chang T-S, Hung C-H, Yang Y-H, Tung S-Y, Wei K-L, Shen C-H, Wu C-S, et al. Direct-Acting Antivirals Reduce the De Novo Development of Esophageal Varices in Patients with Hepatitis C Virus Related Liver Cirrhosis. Viruses. 2023; 15(1):252. https://doi.org/10.3390/v15010252
Chicago/Turabian StyleHsieh, Yung-Yu, Wei-Ming Chen, Kao-Chi Chang, Te-Sheng Chang, Chao-Hung Hung, Yao-Hsu Yang, Shui-Yi Tung, Kuo-Liang Wei, Chen-Heng Shen, Cheng-Shyong Wu, and et al. 2023. "Direct-Acting Antivirals Reduce the De Novo Development of Esophageal Varices in Patients with Hepatitis C Virus Related Liver Cirrhosis" Viruses 15, no. 1: 252. https://doi.org/10.3390/v15010252
APA StyleHsieh, Y.-Y., Chen, W.-M., Chang, K.-C., Chang, T.-S., Hung, C.-H., Yang, Y.-H., Tung, S.-Y., Wei, K.-L., Shen, C.-H., Wu, C.-S., Ding, Y.-J., Hu, J.-H., Huang, Y.-T., Lin, M.-H., Lu, C.-K., Lin, Y.-H., & Lin, M.-S. (2023). Direct-Acting Antivirals Reduce the De Novo Development of Esophageal Varices in Patients with Hepatitis C Virus Related Liver Cirrhosis. Viruses, 15(1), 252. https://doi.org/10.3390/v15010252