
Implementation of Novel Quality Assurance Program for Hepatitis C Viral Load Point of Care Testing


Abstract
:1. Introduction
1.1. Laboratory Testing for HCV
1.2. PoCT for HCV
- Sample types—Whereas laboratory-based testing uses serum or plasma, PoCT often use peripheral whole blood for both HCV serology and NAT. QA programs should use the sample matrix similar to the patient’s sample tested by the participant.
- Sample logistics—Sending samples to testing sites poses some difficult barriers. The samples used in laboratory-based QA are often biological materials that require being shipped either chilled or on dry ice that complies with the international air transport association (IATA) standard. An accredited EQAS provider is responsible for the delivery of the samples to the participant and ensures QA samples are received in good condition. Shipping is expensive and access to remote and regional sites are extremely difficult. Servicing numerous PoCT sites with multiple but small sized packages is not cost effective and administratively cumbersome. Therefore, the number of shipments per year should be kept to a minimum.
- Lack of infrastructure—Many PoCT sites lack the infrastructure commonly found in laboratories. Laboratory-based QA samples usually require refrigerated or frozen storage. The addition of samples into the testing devices commonly require pipettes or utilise manufacture-provided applicators. Therefore, the samples provided must be suitable for a range of different test kits. Some sites in very remote geographies or in places experiencing conflict or natural disasters do not have access to electricity and/or pure water.
- Fixed test events—Usually, EQAS providers conduct several test events per year, where the EQAS samples are sent to the test sites just prior to the opening of the test event and the test site has a defined period of time to test and report the results. After the deadline, the EQAS provider analyses the results submitted by all participants and issues a report. This process is partly to reduce collusion (where test sites compare results before submission). Set test events create a barrier to PoCT QA, because the QA samples must be received by the site at a particular time, exacerbating the logistics issues. Additionally, not all PoCT sites perform testing continuously. Some PoCT sites are mobile. Others may have no tests (or expired kits) available at the time of the test event. The test events may also be scheduled during significant festival/holiday time, times of conflict or civil unrest, monsoon, or other extreme weather conditions when delivery of samples is disrupted. The site, therefore, is unable to participate, wasting the cost of the programs and the shipping.
- Cost—Many PoCT sites that are funded to participate in EQAS use international laboratory-based programs, which are costly both in subscription rates and shipping costs. Once the external funding ceases, so does the participation in the QA programs.
- Regulations—Quality control samples are in-vitro diagnostic devices (IVDs) subject to internationally applied conformity assessment. They must be approved for use by the local regulatory authority before they are supplied to the market. This requirement makes international QC samples costly. Often there is no access to locally produced materials. There are few QC samples that have been developed specifically for PoCTs.
- Data collection and management—Even when PoCT sites participate in a QA program, the data are often not collected and stored in a central database, and rarely are the data used to monitor the performance of the test kit, in particular for qualitative tests. Whereas errors in reporting of specific sample testing are investigated, data obtained from many test sites using the same sample set can expose unexpected trends that may indicate poor IVD performance. A lack of centrally stored and analyzed QA data is a lost opportunity to monitor the quality of PoCTs in the field.
- Data analysis—The analysis and reporting of quantitative QA data is well-defined. Traditionally, the quantitative results of QC programs are plotted on a Levey–Jennings chart and acceptance limits are applied. Although there is some debate on how those limits should be calculated, there is a general acceptance that this process should be used. Where possible, it is ideal that test sites using the same assay and QC compare their results by using a peer-to-peer QC monitoring system. National Serology Reference Laboratory, Australia (NRL) provides an international QC program called QConnect™ that allows peer comparison. However, there is a poorer understanding of how to manage qualitative data such as those derived from RDT testing. The use of a rating system to note the intensity of the bands can convert qualitative data from nominal to ordinal, allowing more sophisticated analysis.
1.3. Novel Approach to the Monitoring of HCV Molecular PoCT
2. Materials and Methods
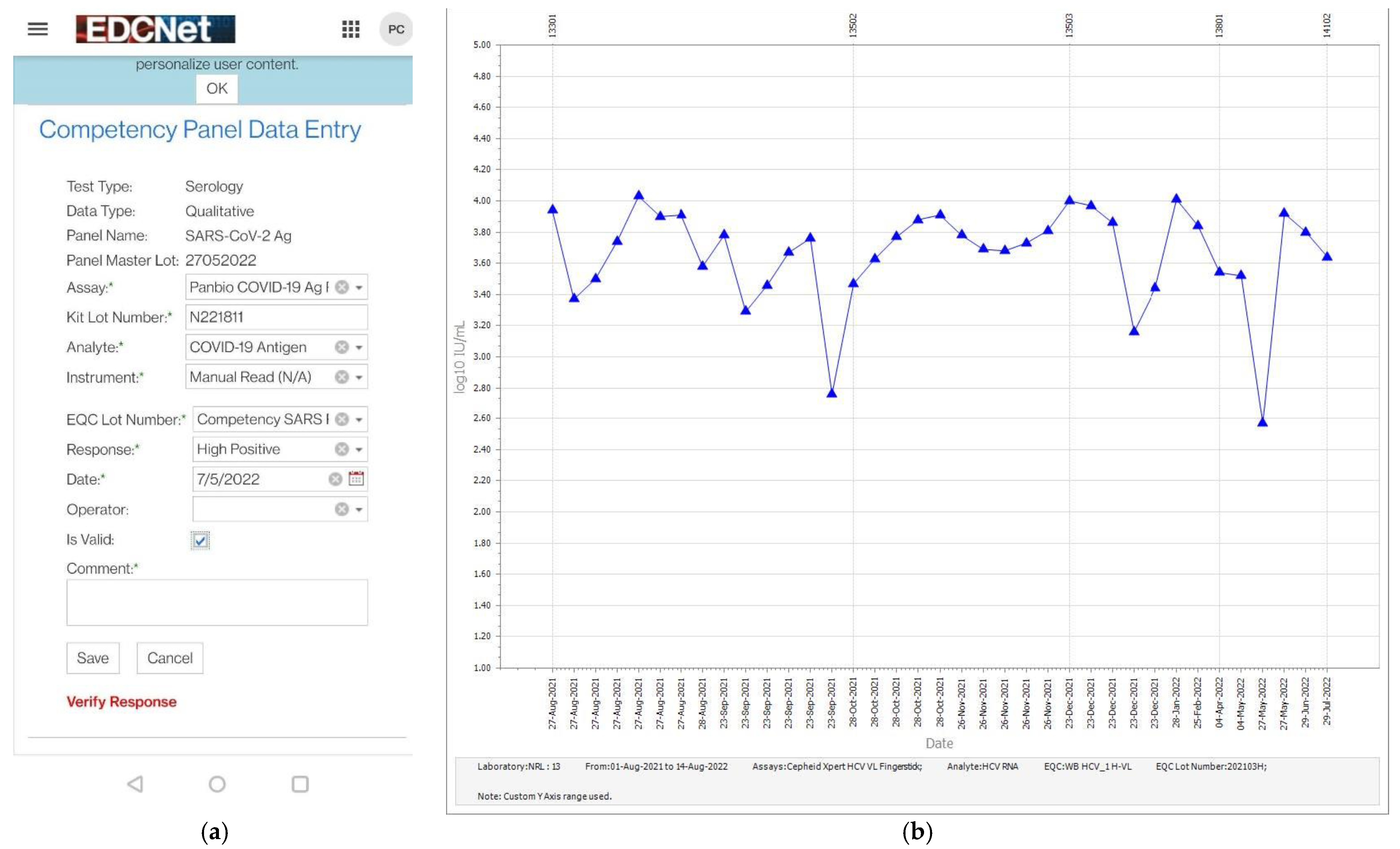
- Competency panel results: The systematic collection of not only QA test results but also associated metadata is critical to a QA program. Metadata include the date of testing, operator identification, test kit name and lot number, sample identification, test result and, where appropriate, any comments relevant to the testing performed. Therefore, the data collected and the mode of submission must be simple.
- EQAS panel results: EQAS are usually organized so that all participants test the same samples at the same time. This is partly due to reduce collusion, where participants discuss the results prior to submission. An EQAS designed to allow participants to test ad hoc must overcome this situation. The samples in the NRL PoCT EQAS have a four-digit, alpha-numeric code. Each EQAS sample type is manufactured in bulk. For example, 1000 vials of HCV genotype 3 high viral load, being the “true result”, will be manufactured. NRL has designed a database whereby the samples within this manufacturing lot are labelled with unique four-digit codes (i.e., 1000 different four-digit codes) but each code is related back to the “true result” of that manufacture lot. The five-member EQAS panels are comprised of different sample types selected randomly. Therefore, on receipt of the EQAS panels, the participant will be unable to identify the true results of the EQAS samples, as the samples within their panels will be different to those received by others. On data entry of the result of an EQAS sample, the four-digit code is compared with the “true result” in the database. The participant will receive notification of the accuracy of the results immediately on submission.
3. Results
3.1. Sample Type
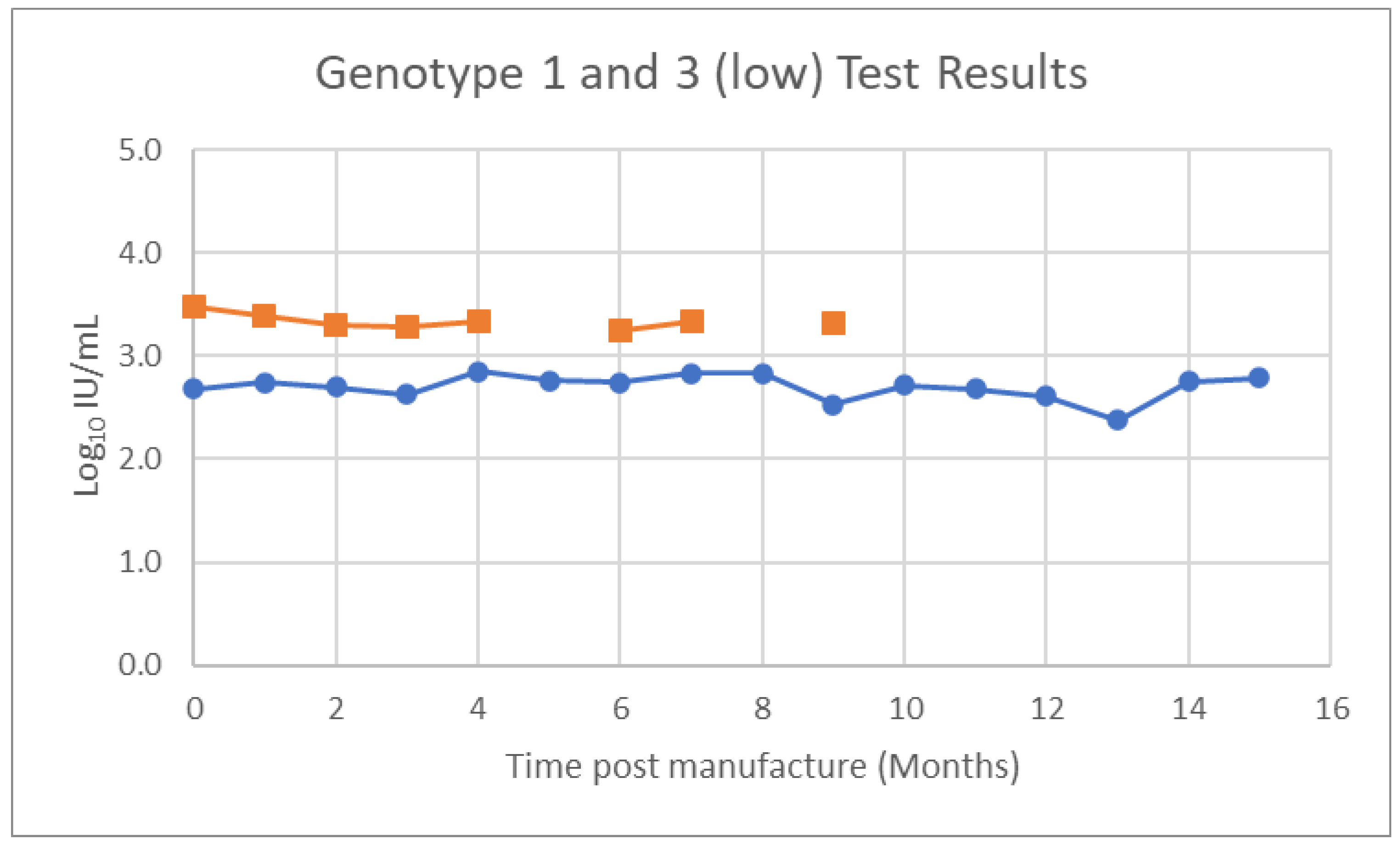
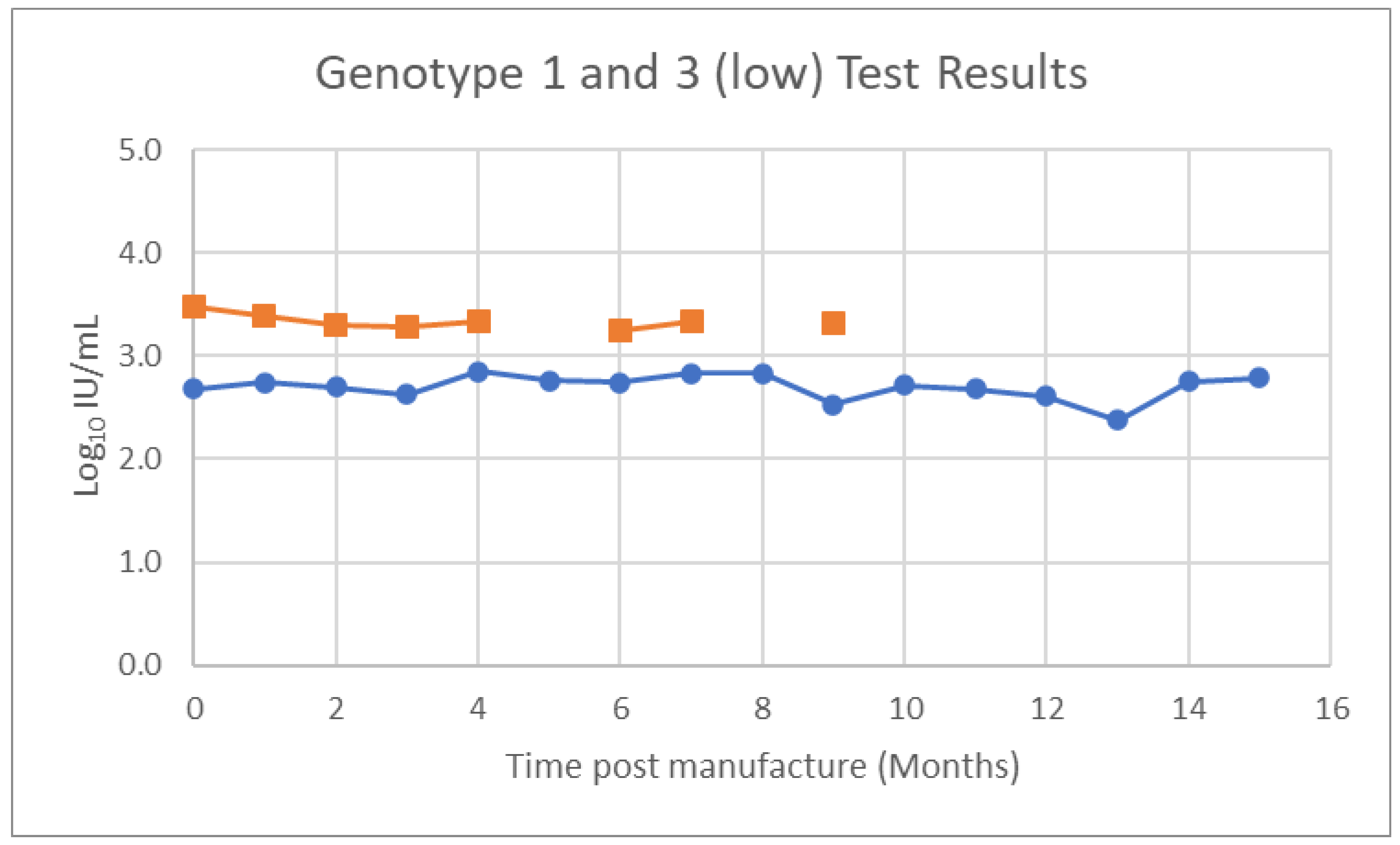
3.1.1. Real-Time Stability Testing
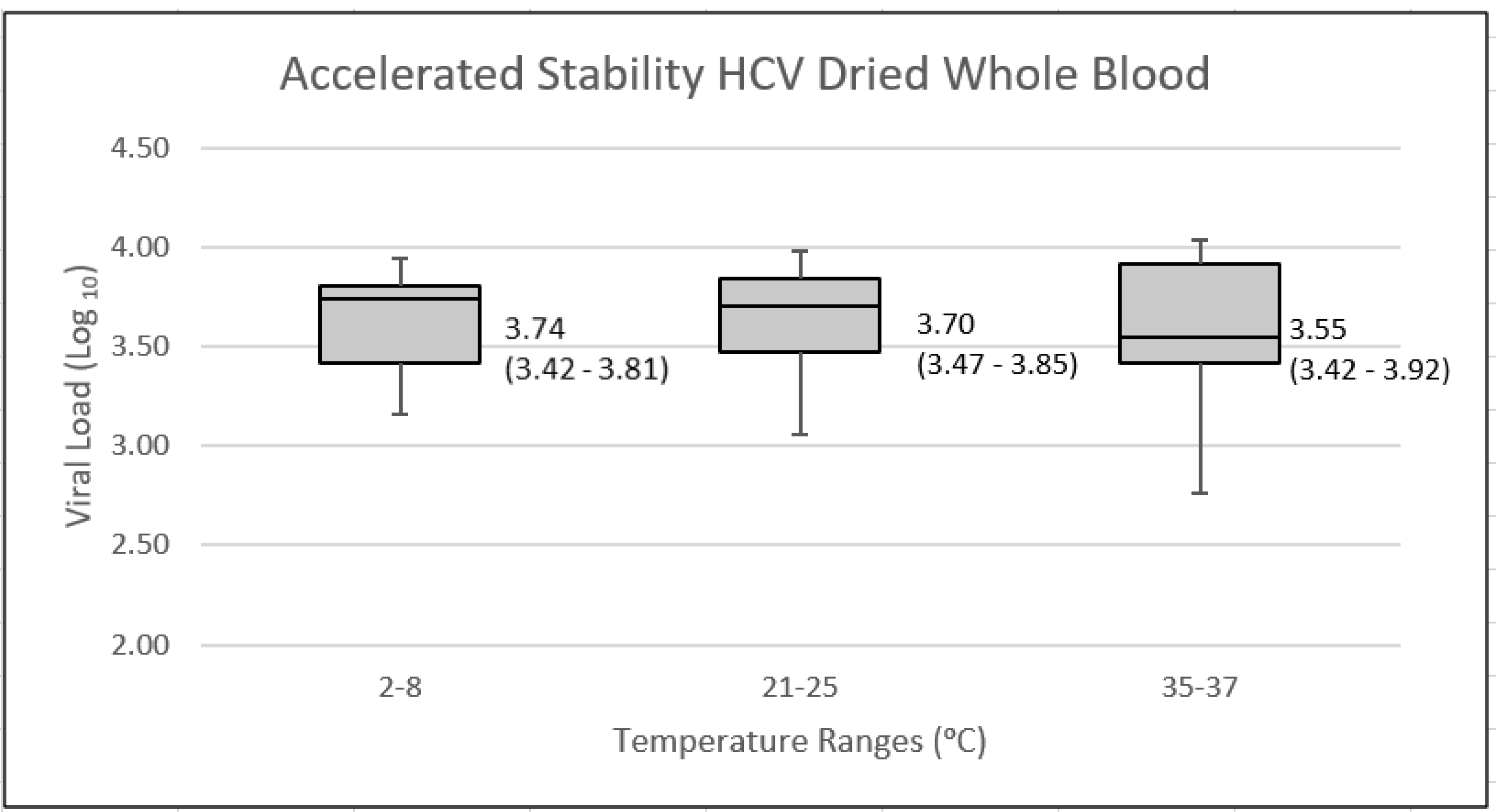
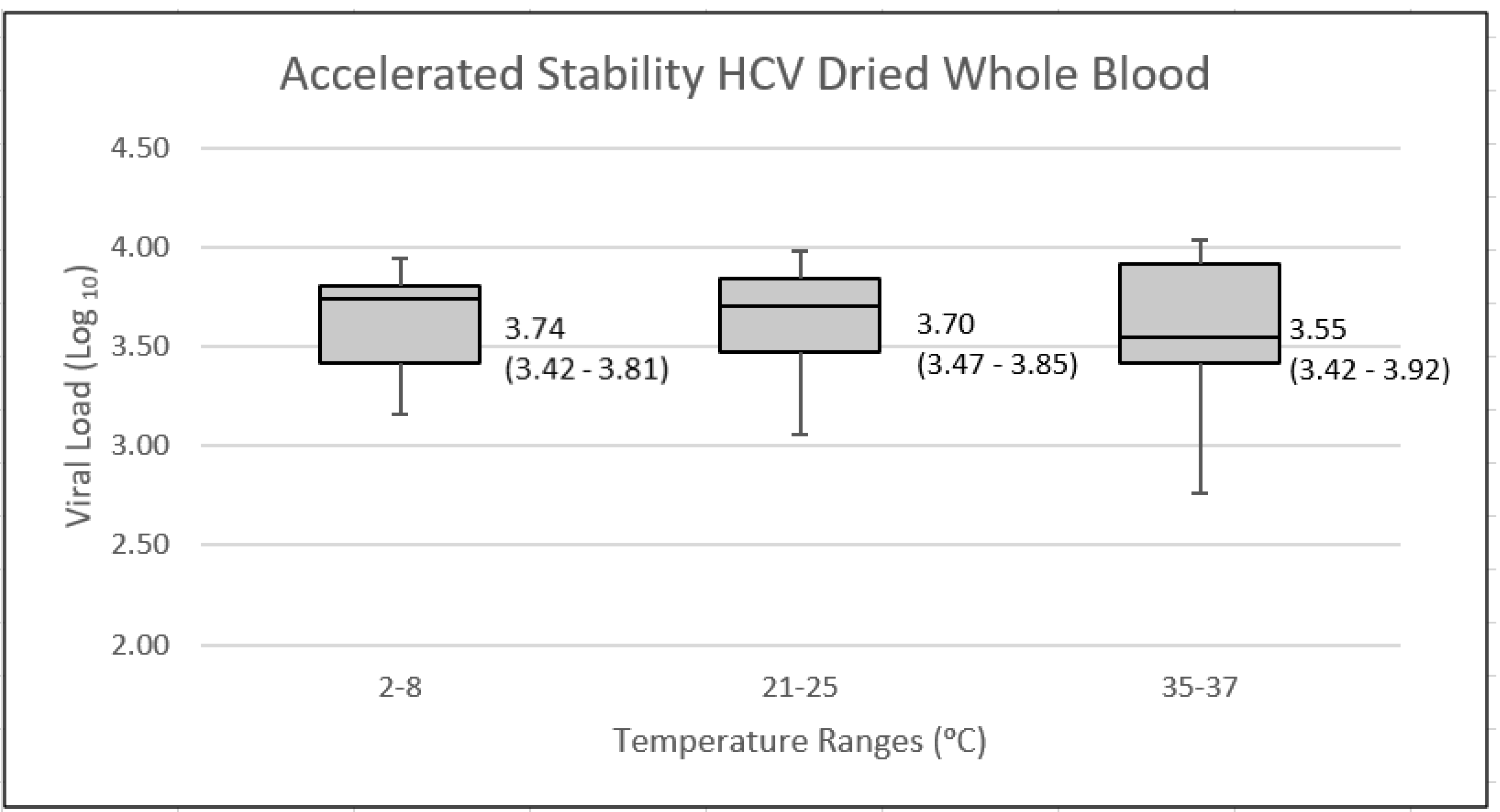
3.1.2. Accelerated Stability Testing
3.2. Data Collection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ISO 13485:2016; Medical Devices—Quality Management Systems—Requirements for Regulatory Purposes. International Organization for Standardization: Geneva, Switzerland, 2016.
- International Medical Device Regulators Forum. Essential Principles of Safety and Performance of Medical Devices and IVD Medical Devices; IMDRF Good Regulatory Review Practices Group, Ed.; International Medical Device Regulators Forum: Canberra, Australia, 2018. [Google Scholar]
- European Parliament and the Council of the European Union. Regulation (EU) 2017/745 of the European Parliament and of the Council on Medical Devices. Off. J. Eur. Union 2017, 60, L117. [Google Scholar]
- European Parliament and of the Council Regulation (EU) 2017/746 of the European Parliament and of the Council. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32017R0746 (accessed on 17 February 2021).
- Australian Government. Classification of IVD Medical Devices; Department of Health Therapeutic Goods Administration, Ed.; Australian Government: Canberra, Australia, 2015; Volume 2.
- National Pathology Accreditation Advisory Council. Requirements for Medical Testing of Microbial Nucleic Acids; Australian Gouvernment: Canberra, Australia, 2013.
- Dimech, W.; Walker, S.; Jardine, D.; Read, S.; Smeh, K.; Karakaltsas, K.; Dent, B.; Dax, E. Comprehensive quality control programme for serology and nucleic acid testing using an Internet-based application. Accred. Qual. Assur. 2004, 8, 148–151. [Google Scholar] [CrossRef]
- Draper, B.L.; Pedrana, A.; Howell, J.; Yee, W.L.; Htay, H.; Aung, K.S.; Shilton, S.; Kyi, K.P.; Naing, W.; Hellard, M. Decentralized, Community-Based Hepatitis C Point-of-Care Testing and Direct-Acting Antiviral Treatment for People Who Inject Drugs and the General Population in Myanmar: Protocol for a Feasibility Study. JMIR Res. Protoc. 2020, 9, e16863. [Google Scholar] [CrossRef] [PubMed]
- Latham, N.H.; Pedrana, A.; Doyle, J.S.; Howell, J.; Williams, B.; Higgs, P.; Thompson, A.J.; Hellard, M.E. Community-based, point-of-care hepatitis C testing: Perspectives and preferences of people who inject drugs. J. Viral Hepat. 2019, 26, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Baveewo, S.; Kamya, M.R.; Mayanja-Kizza, H.; Fatch, R.; Bangsberg, D.R.; Coates, T.; Hahn, J.A.; Wanyenze, R.K. Potential for false positive HIV test results with the serial rapid HIV testing algorithm. BMC Res. Notes 2012, 5, 154. [Google Scholar] [CrossRef] [PubMed]
- Galli, R.A.; Green, K.F.; La Marca, A.; Waldman, L.F.; Powers, R.E.; Daly, A.C.; Shackleton, C.R. Evaluation of the accuracy and ease of use of a rapid HIV-1 Antibody Test performed by untrained operators at the point of care. J. Clin. Virol. 2013, 58 (Suppl. S1), e65–e69. [Google Scholar] [CrossRef] [PubMed]
- Jani, I.V.; Meggi, B.; Mabunda, N.; Vubil, A.; Sitoe, N.E.; Tobaiwa, O.; Quevedo, J.I.; Lehe, J.D.; Loquiha, O.; Vojnov, L.; et al. Accurate early infant HIV diagnosis in primary health clinics using a point-of-care nucleic acid test. J. Acquir. Immune Defic. Syndr. 2014, 67, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.C.; Fonner, V.; Sands, A.; Ford, N.; Obermeyer, C.M.; Tsui, S.; Wong, V.; Baggaley, R. To err is human, to correct is public health: A systematic review examining poor quality testing and misdiagnosis of HIV status. J. Int. AIDS Soc. 2017, 20 (Suppl. S6), 21755. [Google Scholar] [CrossRef] [PubMed]
- Ndase, P.; Celum, C.; Kidoguchi, L.; Ronald, A.; Fife, K.H.; Bukusi, E.; Donnell, D.; Baeten, J.M.; Partners PrEP Study Team. Frequency of false positive rapid HIV serologic tests in African men and women receiving PrEP for HIV prevention: Implications for programmatic roll-out of biomedical interventions. PLoS ONE 2015, 10, e0123005. [Google Scholar]
- Boeke, C.E.; Adesigbin, C.; Agwuocha, C.; Anartati, A.; Aung, H.T.; Aung, K.S.; Grover, G.S.; Ngo, D.; Okamoto, E.; Ngwije, A.; et al. Initial success from a public health approach to hepatitis C testing, treatment and cure in seven countries: The road to elimination. BMJ Glob. Health 2020, 5, e003767. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.; Subbarao, S.; Zhang, G.; Parsons, L.; Nkengasong, J.; Ou, C.Y.; Ellenberger, D. Impact of proficiency testing program for laboratories conducting early diagnosis of HIV-1 infection in infants in low- to middle-income countries. J. Clin. Microbiol. 2014, 52, 773–780. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Laboratory Quality Management System: Handbook; WHO Press: Lyon, France, 2011. [Google Scholar]
- National Pathology Accreditation Advisory Council. Requirements for Laboratory Testing of Human Immunodeficiency Virus (HIV) and Hepatitis C Virus (HCV), 3rd ed.; Department of Health, Ed.; Australian Goverment: Canberra, Australia, 2013.
- National Pathology Accreditation Advisory Council. Requirements for Quality Control, External Quality Assurance & Method Evaluation, 6th ed.; Department of Health, Ed.; Australian Government: Canberra, Australia, 2018.
- World Health Organization Prequalification of In Vitro Diagnostics. Available online: https://extranet.who.int/pqweb/vitro-diagnostics/vitro-diagnostics-lists (accessed on 17 February 2021).
- Shanks, L.; Klarkowski, D.; O’Brien, D.P. False positive HIV diagnoses in resource limited settings: Operational lessons learned for HIV programmes. PLoS ONE 2013, 8, e59906. [Google Scholar]
- Dimech, W.; Lamoury, F.; Ding, X.C.; Lastra, L.M.; Vincini, G.; Sands, A. Policy Analysis: User Monitoring of In-vitro Diagnostic Medical Devices used for Near Patient Testing of Infectious Diseases. IJQHC Commun. 2022, 2, lyac010. [Google Scholar] [CrossRef]
- Parekh, B.S.; Anyanwu, J.; Patel, H.; Downer, M.; Kalou, M.; Gichimu, C.; Keipkerich, B.S.; Clement, N.; Omondi, M.; Mayer, O.; et al. Dried tube specimens: A simple and cost-effective method for preparation of HIV proficiency testing panels and quality control materials for use in resource-limited settings. J. Virol. Methods 2010, 163, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.; Nguyen, S.; Garcia, A.; Subbarao, S.; Nkengasong, J.N.; Ellenberger, D. Generation of dried tube specimen for HIV-1 viral load proficiency test panels: A cost-effective alternative for external quality assessment programs. J. Virol. Methods 2013, 188, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dimech, W.; Vincini, G.; Davies, K.; Karakaltsas, M.; van Cauwalaert, N.D.; Guichet, E.; Koppelman, M.; Cabuang, L. Validation of dried tube sample format quality controls for the monitoring of viral load and blood screening assays. J. Virol. Methods 2020, 285, 113957. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Viral Load Units | HCV Genotype 1 | HCV Genotype 3 | ||
|---|---|---|---|---|
| Low | High | Low | High | |
| Viral load (IU/mL) | 3020 | 11,300 | 476 | 26,900 |
| Viral load (Log10 IU/mL) | 3.48 | 4.05 | 2.68 | 4.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimech, W.; Cabuang, L.; Davies, K.; Vincini, G. Implementation of Novel Quality Assurance Program for Hepatitis C Viral Load Point of Care Testing. Viruses 2022, 14, 1929. https://doi.org/10.3390/v14091929
Dimech W, Cabuang L, Davies K, Vincini G. Implementation of Novel Quality Assurance Program for Hepatitis C Viral Load Point of Care Testing. Viruses. 2022; 14(9):1929. https://doi.org/10.3390/v14091929
Chicago/Turabian StyleDimech, Wayne, Liza Cabuang, Kylie Davies, and Giuseppe Vincini. 2022. "Implementation of Novel Quality Assurance Program for Hepatitis C Viral Load Point of Care Testing" Viruses 14, no. 9: 1929. https://doi.org/10.3390/v14091929
APA StyleDimech, W., Cabuang, L., Davies, K., & Vincini, G. (2022). Implementation of Novel Quality Assurance Program for Hepatitis C Viral Load Point of Care Testing. Viruses, 14(9), 1929. https://doi.org/10.3390/v14091929