
Effect of Casirivimab/Imdevimab Treatment on Serum Type I Interferon Levels in SARS-CoV-2 Infection

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants and Protocol
2.3. Blood Samples
2.4. Cytokine Measurement and Protocol
2.5. Quantitative Reverse Transcription Polymerase Chain Reaction
2.6. Statistical Analysis
3. Results
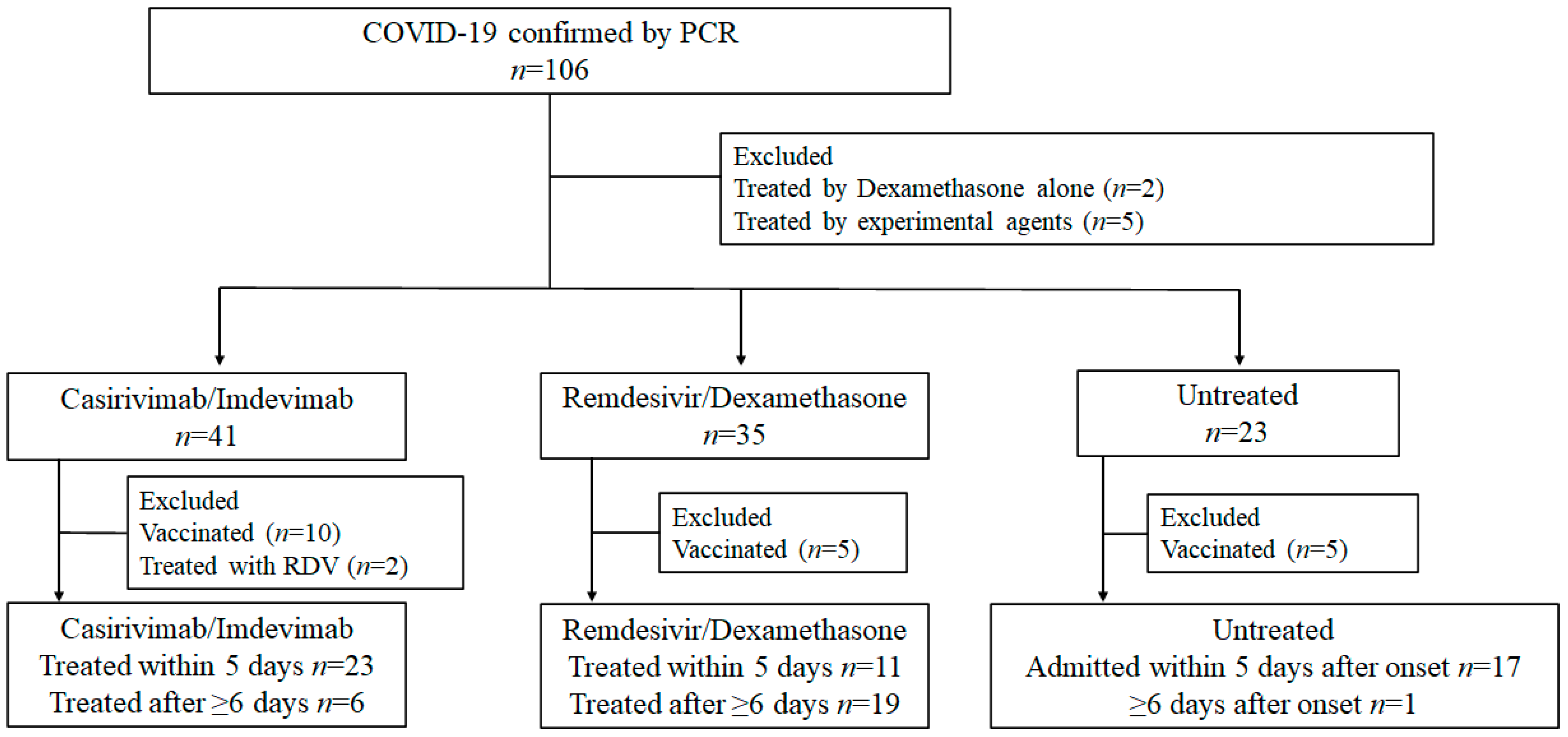
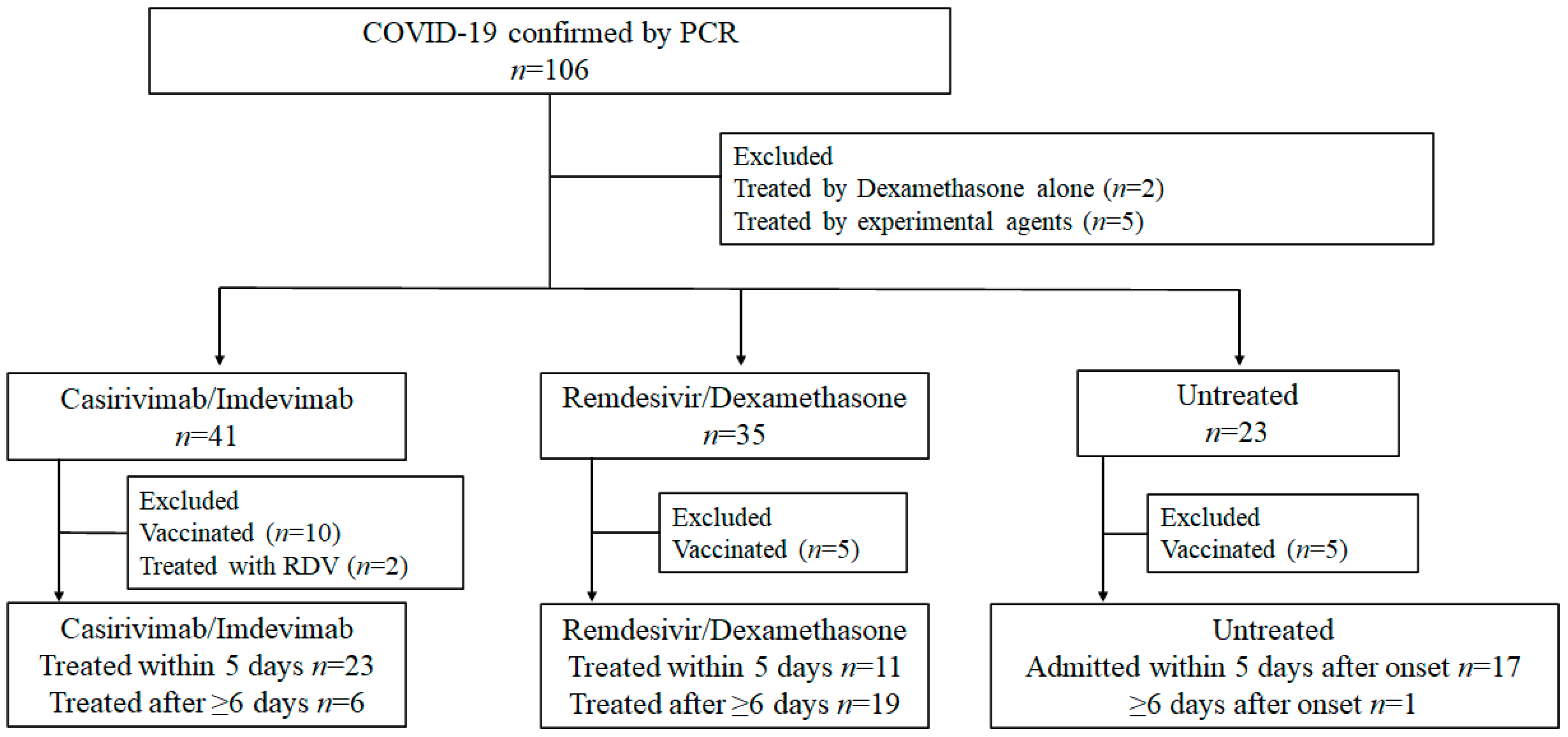
3.1. Study Participants
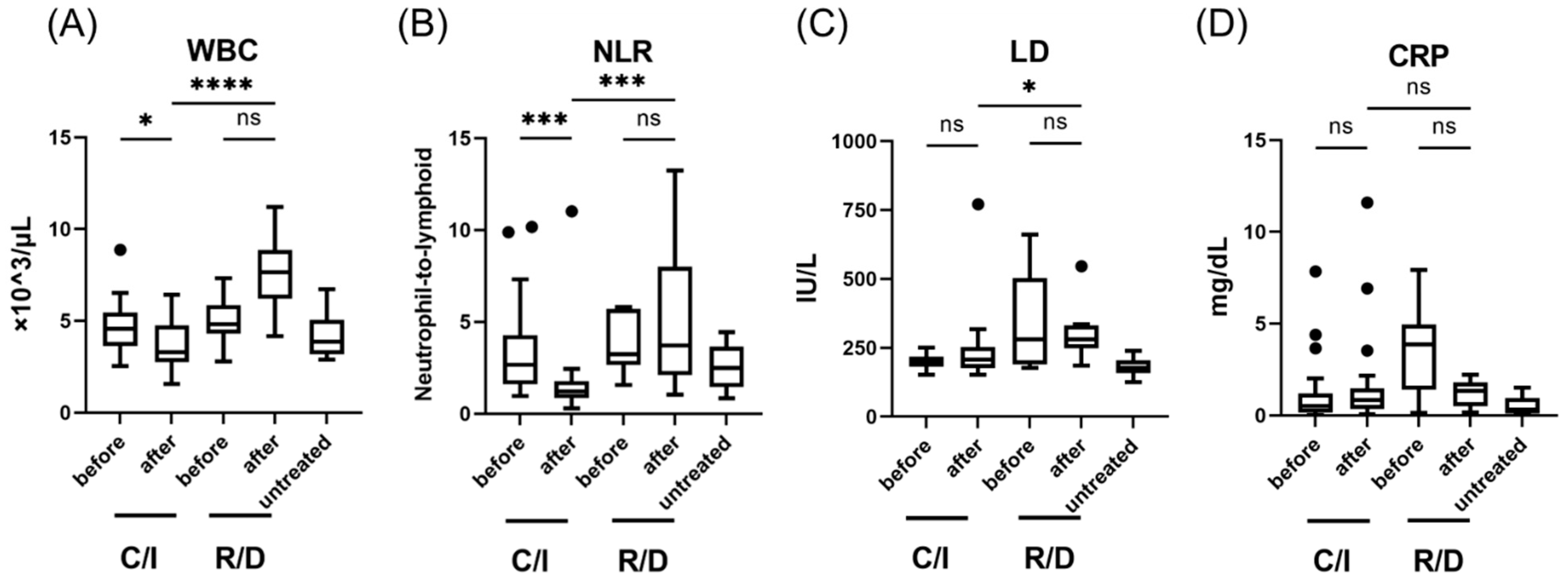
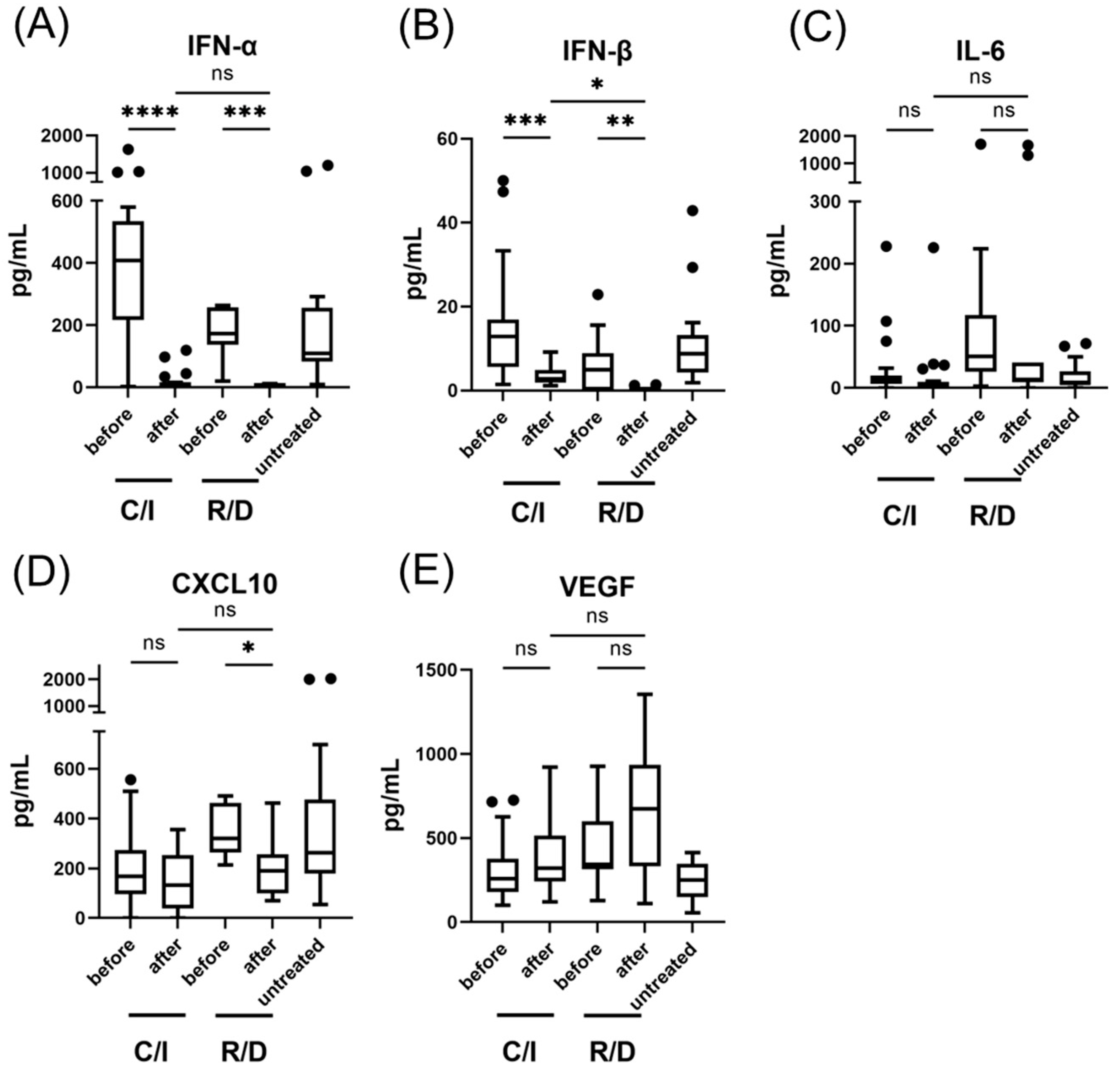
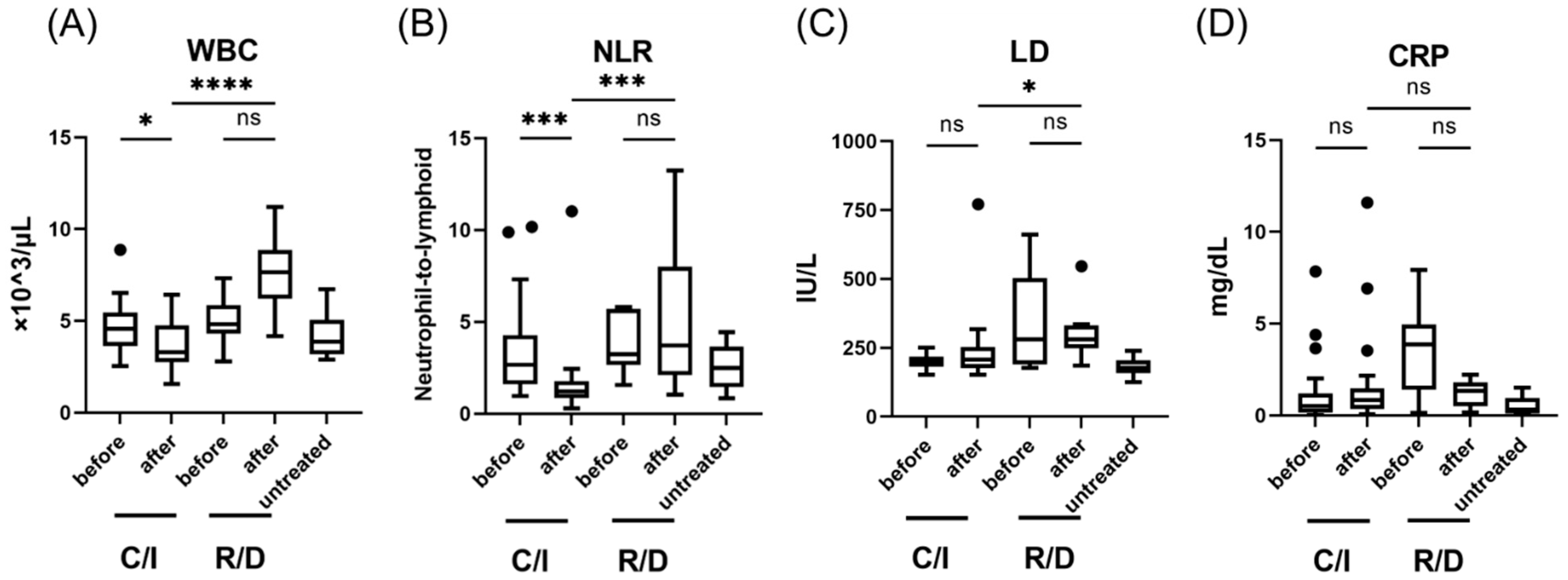
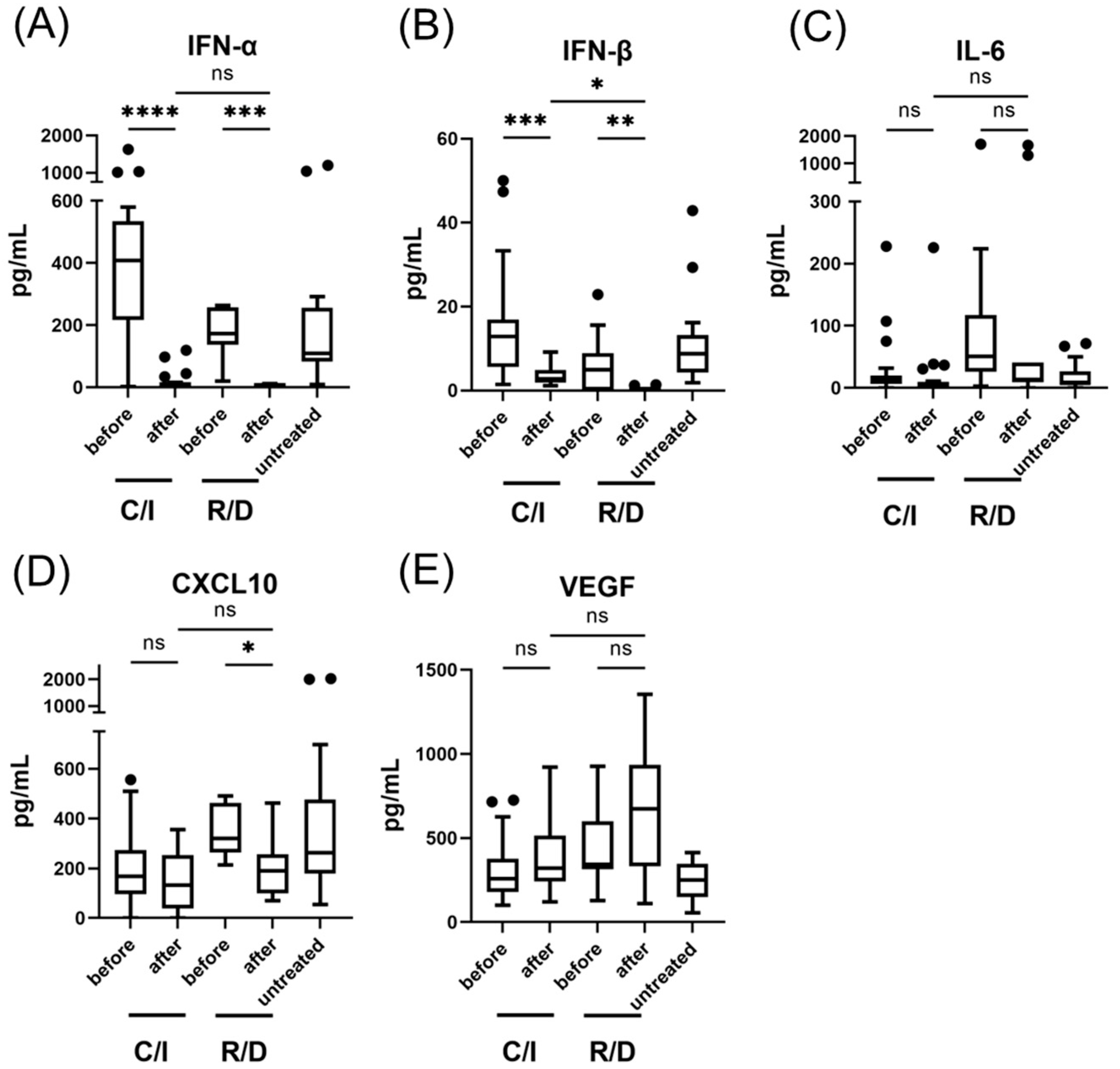
3.2. The Effect of Casirivimab and Imdevimab on the Immune Response in the Early Phase of SARS-CoV-2 Infection
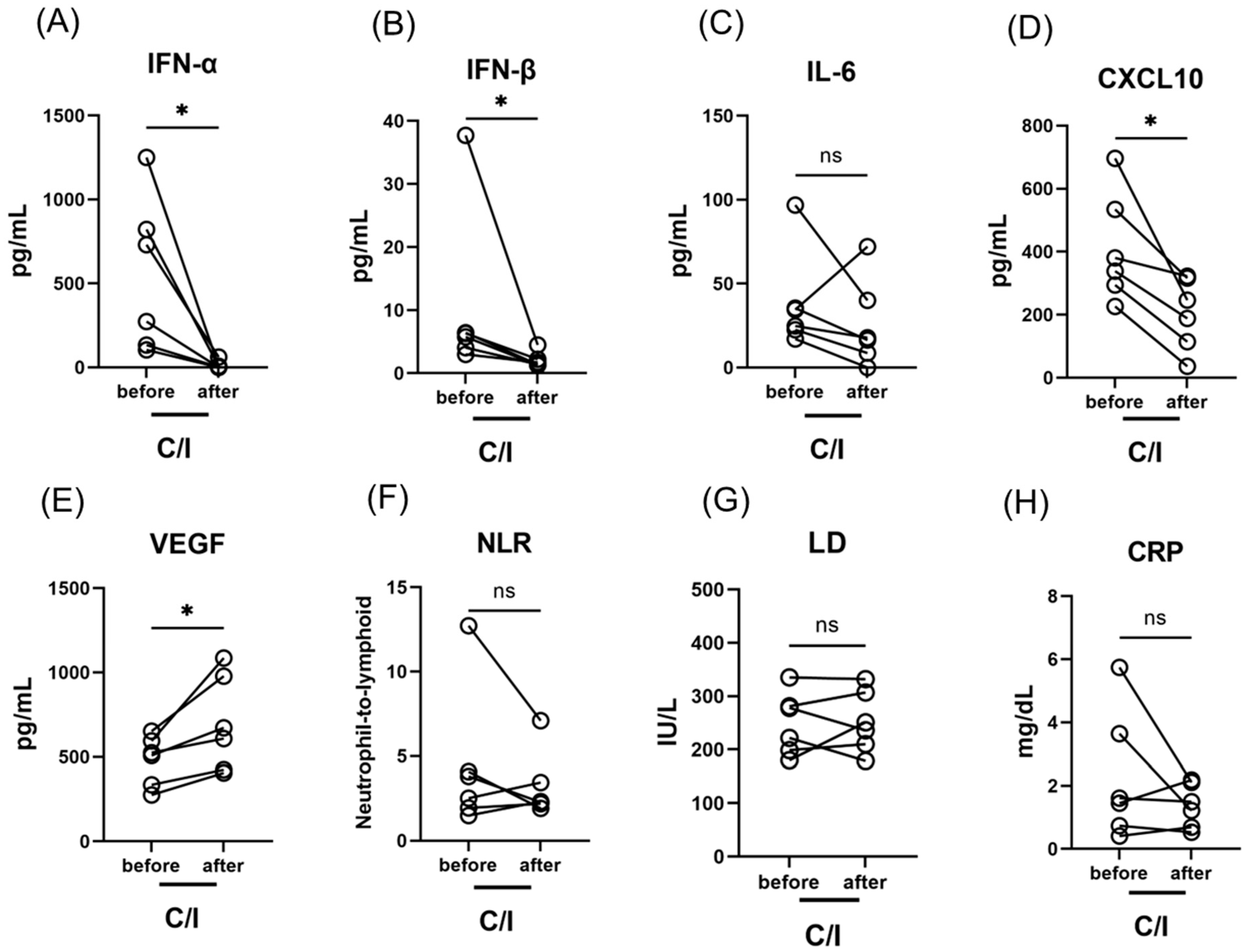
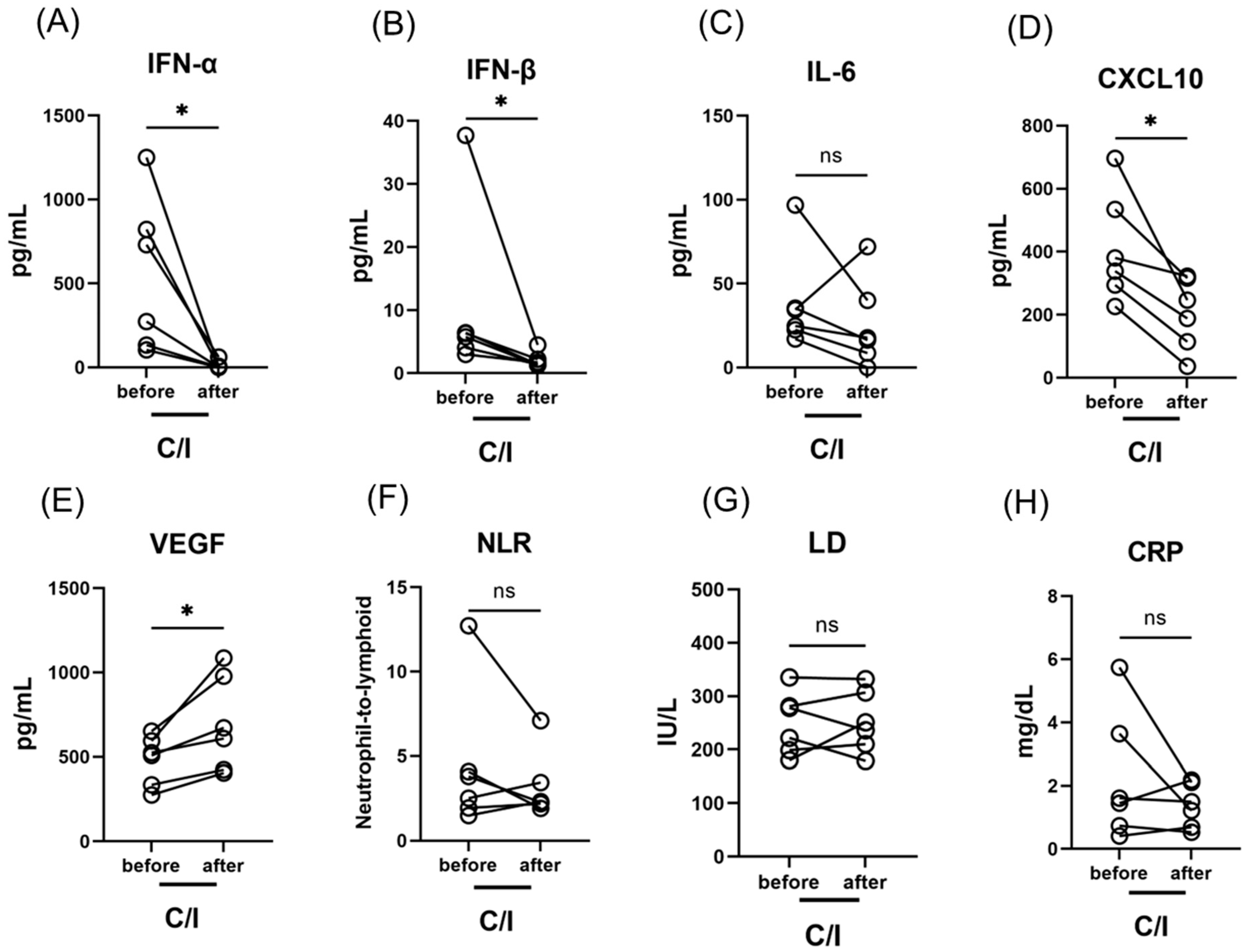
3.3. The Effect of C/I in the Late Phase on the Immune Response against SARS-CoV-2 Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Renn, A.; Fu, Y.; Hu, X.; Hall, M.D.; Simeonov, A. Fruitful neutralizing antibody pipeline brings hope to defeat SARS-CoV-2. Trends Pharmacol. Sci. 2020, 41, 815–829. [Google Scholar] [CrossRef] [PubMed]
- Shanmugaraj, B.; Siriwattananon, K.; Wangkanont, K.; Phoolcharoen, W. Perspectives on monoclonal antibody therapy as potential therapeutic intervention for Coronavirus disease-19 (COVID-19). Asian Pac. J. Allergy Immunol. 2020, 38, 10–18. [Google Scholar] [PubMed]
- Taylor, P.C.; Adams, A.C.; Hufford, M.M.; de la Torre, I.; Winthrop, K.; Gottlieb, R.L. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat. Rev. Immunol. 2021, 21, 382–393. [Google Scholar] [CrossRef]
- Baum, A.; Fulton, B.O.; Wloga, E.; Copin, R.; Pascal, K.E.; Russo, V.; Giordano, S.; Lanza, K.; Negron, N.; Ni, M.; et al. Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies. Science 2020, 369, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Musser, B.J.; Soo, Y.; Rofail, D.; Im, J.; et al. REGN-COV2, a neutralizing antibody cocktail, in outpatients with COVID-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.J.; Banu, S.; Sasikala, M.; Parsa, K.V.L.; Sowpati, D.T.; Yadav, R.; Tallapaka, K.B.; Siva, A.B.; Vishnubhotla, R.; Rao, G.V.; et al. Effectiveness of REGEN-COV antibody cocktail against the B.1.617.2 (delta) variant of SARS-CoV-2: A cohort study. J. Intern. Med. 2022, 291, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Piccicacco, N.; Zeitler, K.; Montero, J.; Kumar, A.; Lakshmi, S.; Kim, K.; Wein, D.; Vasey, T.; Vasey, M.; Oxner, A. Effectiveness of severe acute respiratory syndrome Coronavirus 2 monoclonal antibody infusions in high-risk outpatients. Open Forum Infect. Dis. 2021, 8, ofab292. [Google Scholar] [CrossRef]
- Verderese, J.P.; Stepanova, M.; Lam, B.; Racila, A.; Kolacevski, A.; Allen, D.; Hodson, E.; Aslani-Amoli, B.; Homeyer, M.; Stanmyre, S.; et al. Neutralizing monoclonal antibody treatment reduces hospitalization for mild and moderate Coronavirus disease 2019 (COVID-19): A real-world experience. Clin. Infect. Dis. 2022, 74, 1063–1069. [Google Scholar] [CrossRef]
- Ganesh, R.; Philpot, L.M.; Bierle, D.M.; Anderson, R.J.; Arndt, L.L.; Arndt, R.F.; Culbertson, T.L.; Destro Borgen, M.J.; Hanson, S.N.; Kennedy, B.D.; et al. Real-world clinical outcomes of bamlanivimab and casirivimab-imdevimab among high-risk patients with mild to moderate Coronavirus disease 2019. J. Infect. Dis. 2021, 224, 1278–1286. [Google Scholar] [CrossRef]
- Razonable, R.R.; Pawlowski, C.; O’Horo, J.C.; Arndt, L.L.; Arndt, R.; Bierle, D.M.; Borgen, M.D.; Hanson, S.N.; Hedin, M.C.; Lenehan, P.; et al. Casirivimab-Imdevimab treatment is associated with reduced rates of hospitalization among high-risk patients with mild to moderate coronavirus disease-19. EClinicalMedicine 2021, 40, 101102. [Google Scholar] [CrossRef]
- San Filippo, S.; Crovetto, B.; Bucek, J.; Nahass, R.G.; Milano, M.; Brunetti, L. Comparative Efficacy of Early COVID-19 Monoclonal Antibody Therapies: A Retrospective Analysis. Open Forum Infect. Dis. 2022, 9, ofac080. [Google Scholar] [CrossRef] [PubMed]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Péré, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and infammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hofmann, H.H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef] [PubMed]
- Acharya, D.; Liu, G.; Gack, M.U. Dysregulation of type I interferon responses in COVID-19. Nat. Rev. Immunol. 2020, 20, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Coperchini, F.; Chiovato, L.; Rotondi, M. Interleukin-6, CXCL10 and infiltrating macrophages in COVID-19-related cytokine storm: Not one for all but all for one! Front. Immunol. 2021, 12, 668507. [Google Scholar] [CrossRef]
- Zhou, Q.; Chen, V.; Shannon, C.P.; Wei, X.S.; Xiang, X.; Wang, X.; Wang, Z.H.; Tebbutt, S.J.; Kollmann, T.R.; Fish, E.N. Interferon-α2b treatment for COVID-19. Front. Immunol. 2020, 11, 1061. [Google Scholar] [CrossRef]
- Pereda, R.; González, D.; Rivero, H.B.; Rivero, J.C.; Pérez, A.; Lopez, L.D.R.; Mezquia, N.; Venegas, R.; Betancourt, J.R.; Domínguez, R.E.; et al. Therapeutic effectiveness of interferon alpha 2b treatment for COVID-19 patient recovery. J. Interferon Cytokine Res. 2020, 40, 578–588. [Google Scholar] [CrossRef]
- Rahmani, H.; Davoudi-Monfared, E.; Nourian, A.; Khalili, H.; Hajizadeh, N.; Jalalabadi, N.Z.; Fazeli, M.R.; Ghazaeian, M.; Yekaninejad, M.S. Interferon β-1b in treatment of severe COVID-19: A randomized clinical trial. Int. Immunopharmacol. 2020, 88, 106903. [Google Scholar] [CrossRef]
- Monk, P.D.; Marsden, R.J.; Tear, V.J.; Brookes, J.; Batten, T.N.; Mankowski, M.; Gabbay, F.J.; Davies, D.E.; Holgate, S.T.; Ho, L.P.; et al. Safety and efficacy of inhaled nebulised interferon beta-1a (SNG001) for treatment of SARS-CoV-2 infection: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Respir. Med. 2021, 9, 196–206. [Google Scholar] [CrossRef]
- Chen, C.C.; Yang, Y.P.; Tsai, H.L.; Tung, T.H. Effects of tocilizumab on adults with COVID-19 pneumonia: A meta-analysis. Front. Med. 2022, 9, 838904. [Google Scholar] [CrossRef]
- Wang, Y.C.; Lu, M.C.; Yang, S.F.; Bien, M.Y.; Chen, Y.F.; Li, Y.T. Respiratory care for the critical patients with 2019 novel coronavirus. Respir. Med. 2021, 186, 106516. [Google Scholar] [CrossRef] [PubMed]
- Kawasuji, H.; Takegoshi, Y.; Kaneda, M.; Ueno, A.; Miyajima, Y.; Kawago, K.; Fukui, Y.; Yoshida, Y.; Kimura, M.; Yamada, H.; et al. Transmissibility of COVID-19 depends on the viral load around onset in adult and symptomatic patients. PLoS ONE 2020, 15, e0243597. [Google Scholar] [CrossRef] [PubMed]
- Shirato, K.; Nao, N.; Katano, H.; Takayama, I.; Saito, S.; Kato, F.; Katoh, H.; Sakata, M.; Nakatsu, Y.; Mori, Y.; et al. Development of genetic diagnostic methods for novel Coronavirus 2019 (nCoV-2019) in Japan. Jpn. J. Infect. Dis. 2020, 73, 304–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, J.; Shiraishi, K.; Tamura, T.; Otani, K.; Kikuchi, T.; Mataga, A.; Ueno, T.; Tanaka, M. Casirivimab-imdevimab neutralizing SARS-CoV-2: Post-infusion clinical events and their risk factors. J. Pharm. Health Care. Sci. 2022, 8, 1. [Google Scholar] [CrossRef]
- Cicchitto, G.; Cardillo, L.; de Martinis, C.; Sabatini, P.; Marchitiello, R.; Abate, G.; Rovetti, A.; Cavallera, A.; Apuzzo, C.; Ferrigno, F.; et al. Effects of casirivimab/imdevimab monoclonal antibody treatment among vaccinated patients infected by SARS-CoV-2 delta variant. Viruses 2022, 14, 650. [Google Scholar] [CrossRef]
- Motozono, C.; Toyoda, M.; Zahradnik, J.; Saito, A.; Nasser, H.; Tan, T.S.; Ngare, I.; Kimura, I.; Uriu, K.; Kosugi, Y.; et al. SARS-CoV-2 spike L452R variant evades cellular immunity and increases infectivity. Cell Host Microbe 2021, 29, 1124–1136. [Google Scholar] [CrossRef]
- Ricci, D.; Etna, M.P.; Rizzo, F.; Sandini, S.; Severa, M.; Coccia, E.M. Innate immune response to SARS-CoV-2 infection: From cells to soluble mediators. Int. J. Mol. Sci. 2021, 22, 7017. [Google Scholar] [CrossRef]
- Lowery, S.A.; Sariol, A.; Perlman, S. Innate immune and inflammatory responses to SARS-CoV-2: Implications for COVID-19. Cell Host Microbe 2021, 29, 1052–1062. [Google Scholar] [CrossRef]
- Crouse, J.; Kalinke, U.; Oxenius, A. Regulation of antiviral T cell responses by type I interferons. Nat. Rev. Immunol. 2015, 15, 231–242. [Google Scholar] [CrossRef]
- Nagaoka, K.; Kawasuji, H.; Murai, Y.; Kaneda, M.; Ueno, A.; Miyajima, Y.; Fukui, Y.; Morinaga, Y.; Yamamoto, Y. Circulating type I interferon levels in the early phase of COVID-19 are associated with the development of respiratory failure. Front. Immunol. 2022, 13, 844304. [Google Scholar] [CrossRef]
- Chen, X.; Pan, Z.; Yue, S.; Yu, F.; Zhang, J.; Yang, Y.; Li, R.; Liu, B.; Yang, X.; Gao, L.; et al. Disease severity dictates SARS-CoV-2-specific neutralizing antibody responses in COVID-19. Signal Transduct. Target. Ther. 2020, 5, 180. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Kawasuji, H.; Morinaga, Y.; Tani, H.; Kimura, M.; Yamada, H.; Yoshida, Y.; Takegoshi, Y.; Kaneda, M.; Murai, Y.; Kimoto, K.; et al. Delayed neutralizing antibody response in the acute phase correlates with severe progression of COVID-19. Sci. Rep. 2021, 11, 16535. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Ramanan, A.V.; Kartman, C.E.; de Bono, S.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Saraiva, J.F.K.; Chakladar, S.; Marconi, V.C. Efficacy and safety of baricitinib plus standard of care for the treatment of critically ill hospitalised adults with COVID-19 on invasive mechanical ventilation or extracorporeal membrane oxygenation: An exploratory, randomised, placebo-controlled trial. Lancet Respir. Med. 2022, 10, 327–336. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 51) | C/I (n = 23) | R/D (n = 11) | Untreated (n = 17) | |
|---|---|---|---|---|
| Age, years | 51 (40–55) | 53 (50–56) | 52 (43–57) | 38 (30–50) |
| Sex; male/female | 32/19 | 11/12 ** | 10/1 | 11/6 |
| Underlying disease | ||||
| None | 29 (57) | 15 (65) | 5 (45) | 9 (53) |
| Hypertension | 9 (18) | 4 (17) | 4 (36) | 1 (6) |
| Diabetes mellitus | 2 (4) | 0 (0) | 1 (9) | 1 (6) |
| Body mass index (kg/m2) | 21.7 (20.0–25.0) | 21.7 (19.1–24.8) | 27.0 (24.8–30.9) | 20.8 (19.3–21.5) |
| Initial nasopharyngeal-viral load (log copies/μL) | 5.0 (4.3–5.7) | 5.2 (4.7–5.8) | 4.7 (4.0–5.3) | 5.0 (4.5–5.6) |
| Deterioration of fever after treatment a | - | 14 (61) ** | 0 (0) | - |
| <1.0 °C | - | 7 (30) | 0 (0) | - |
| ≥1.0 °C | - | 7 (30) | 0 (0) | - |
| Oxygen therapy | ||||
| required oxygen therapy | 18 (35) | 8 (35) ** | 10 (91) | - |
| duration period of oxygen therapy (days) | 3 (2–10) | 2 (1.8–2.3) ** | 9 (4.8–12.3) | - |
| invasive positive pressure ventilation | 2/2 | 0 | 2/2 | - |
| The length of hospital stay (days) | 6 (5–8) | 5 (5–7) ** | 11 (11–15) | 4 (4–7) ** |
| Death within 30-days after onset | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Patient | Age | Sex | Underlying Disease | C/I Initiated Timing (Clinical Day) | Deterioration of Fever after C/I (Elevated Temperature) a | Required Oxygen Therapy after C/I (Treated Days) | Length of Hospital Stay after Treatment (Days) |
|---|---|---|---|---|---|---|---|
| A | 50 | F | None | 10 | No | Yes (3) | 6 |
| B | 55 | M | None | 6 | Yes (≥1.0 °C) | Yes (4) | 6 |
| C | 41 | M | None | 7 | No | Yes (3) | 5 |
| D | 46 | M | None | 9 | Yes (<1.0 °C) | Yes (2) | 4 |
| E | 44 | M | None | 7 | Yes (<1.0 °C) | No | 3 |
| F | 49 | M | Allergic rhinitis | 7 | No | No | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagaoka, K.; Kawasuji, H.; Takegoshi, Y.; Murai, Y.; Kaneda, M.; Ueno, A.; Miyajima, Y.; Niimi, H.; Morinaga, Y.; Yamamoto, Y. Effect of Casirivimab/Imdevimab Treatment on Serum Type I Interferon Levels in SARS-CoV-2 Infection. Viruses 2022, 14, 1399. https://doi.org/10.3390/v14071399
Nagaoka K, Kawasuji H, Takegoshi Y, Murai Y, Kaneda M, Ueno A, Miyajima Y, Niimi H, Morinaga Y, Yamamoto Y. Effect of Casirivimab/Imdevimab Treatment on Serum Type I Interferon Levels in SARS-CoV-2 Infection. Viruses. 2022; 14(7):1399. https://doi.org/10.3390/v14071399
Chicago/Turabian StyleNagaoka, Kentaro, Hitoshi Kawasuji, Yusuke Takegoshi, Yushi Murai, Makito Kaneda, Akitoshi Ueno, Yuki Miyajima, Hideki Niimi, Yoshitomo Morinaga, and Yoshihiro Yamamoto. 2022. "Effect of Casirivimab/Imdevimab Treatment on Serum Type I Interferon Levels in SARS-CoV-2 Infection" Viruses 14, no. 7: 1399. https://doi.org/10.3390/v14071399
APA StyleNagaoka, K., Kawasuji, H., Takegoshi, Y., Murai, Y., Kaneda, M., Ueno, A., Miyajima, Y., Niimi, H., Morinaga, Y., & Yamamoto, Y. (2022). Effect of Casirivimab/Imdevimab Treatment on Serum Type I Interferon Levels in SARS-CoV-2 Infection. Viruses, 14(7), 1399. https://doi.org/10.3390/v14071399