
Mortality in SARS-CoV-2 Hospitalized Patients Treated with Remdesivir: A Nationwide, Registry-Based Study in Italy

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
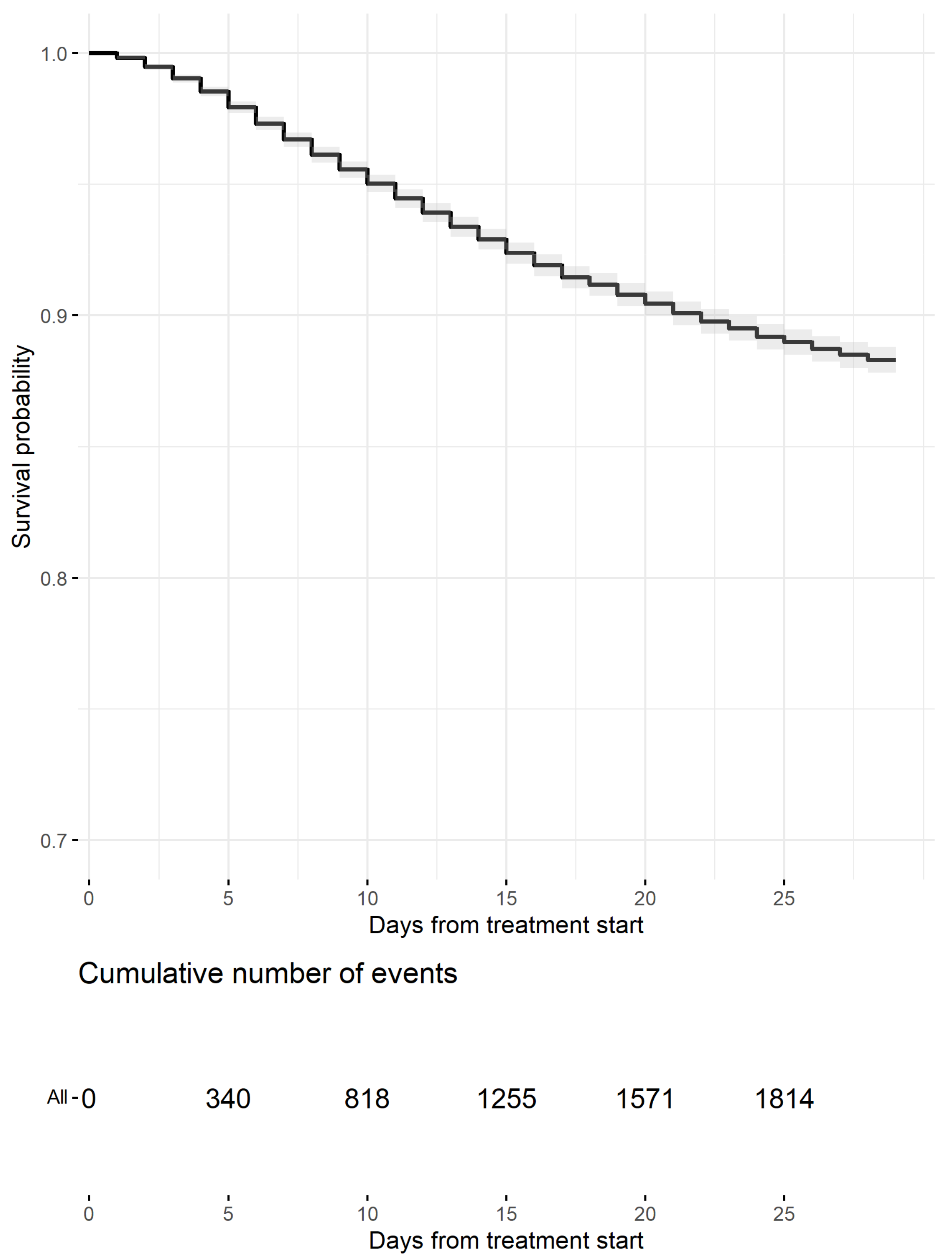
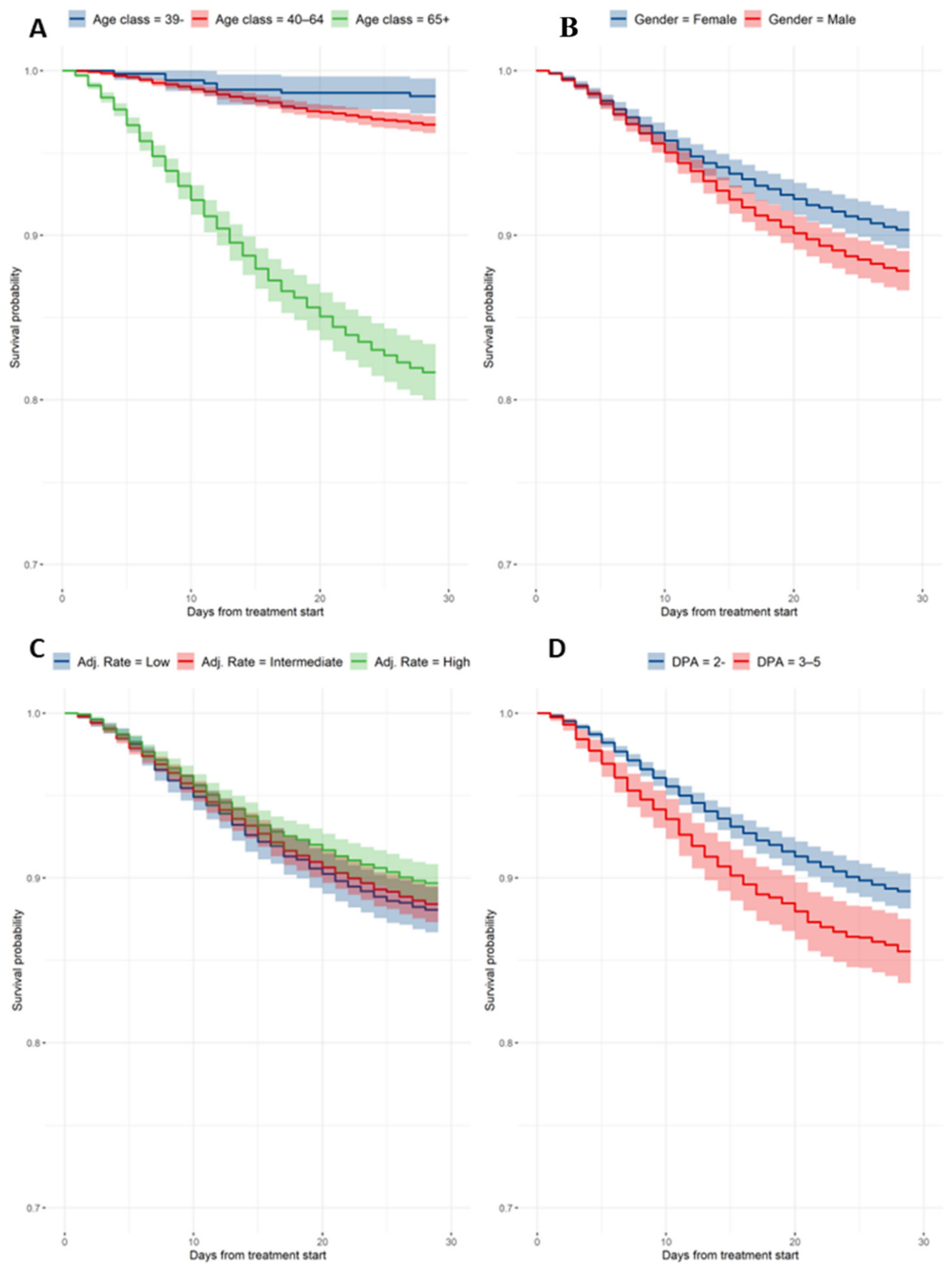
3.1. Crude Mortality and Cox-Adjusted Estimates
3.2. Hospitalization and Need of Mechanical Ventilation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, G.; De Clercq, E. Therapeutic options for the 2019 novel coronavirus (2019-nCoV). Nat. Rev. Drug. Discov. 2020, 19, 149–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheahan, T.P.; Sims, A.C.; Leist, S.R.; Schäfer, A.; Won, J.; Brown, A.J.; Montgomery, S.A.; Hogg, A.; Babusis, D.; Clarke, M.O.; et al. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat. Commun. 2020, 11, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- ACTT-1 Study Group. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- WHO Solidarity Trial Consortium. Repurposed antiviral drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2020, 384, 497–511. [Google Scholar]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Poissy, J.; Belhadi, D.; Diallo, A.; Lê, M.-P.; Peytavin, G.; Staub, T.; et al. DisCoVeRy Study Group. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): A phase 3, randomised, controlled, open-label trial. Lancet Infect. Dis. 2021, 22, 209–221. [Google Scholar] [CrossRef]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Paño-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2021, 28, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Rochwerg, B.; Siemieniuk, R.A.; Agoritsas, T.; Lamontagne, F.; Askie, L.; Lytvyn, L.; Agarwal, A.; Leo, Y.-S.; Macdonald, H.; Zeng, L.; et al. A living WHO guideline on drugs for COVID-19. BMJ 2020, 370, m3379. [Google Scholar]
- Thiruchelvam, K.; Kow, C.S.; Hadi, M.A.; Hasan, S.S. The use of remdesivir for the management of patients with moderate-to-severe COVID-19: A systematic review. Expert. Rev. Anti. Infect. Ther. 2021, 20, 211–229. [Google Scholar] [CrossRef] [PubMed]
- Ohl, M.E.; Miller, D.R.; Lund, B.C.; Kobayashi, T.; Miell, K.R.; Beck, B.F.; Alexander, B.; Crothers, K.; Sarrazin, M.S.V. Association of Remdesivir Treatment With Survival and Length of Hospital Stay Among US Veterans Hospitalized With COVID-19. JAMA Netw. Open 2021, 4, e2114741. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. CHMP Post-Authorisation Summary of Positive Opinion for Veklury (II-16). 2021. Available online: https://www.ema.europa.eu/en/documents/smop/chmp-post-authorisation-summary-positive-opinion-veklury-ii-16_en.pdf (accessed on 16 December 2021).
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. GS-US-540-9012 (PINETREE) Investigators. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2021, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Takashita, E.; Kinoshita, N.; Yamayoshi, S.; Sakai-Tagawa, Y.; Fujisaki, S.; Ito, M.; Iwatsuki-Horimoto, K.; Chiba, S.; Halfmann, P.; Nagai, H.; et al. Efficacy of Antibodies and Antiviral Drugs against COVID-19 Omicron Variant. N. Engl. J. Med. 2022, 386, 995–998. [Google Scholar] [CrossRef]
- Vangeel, L.; Chiu, W.; De Jonghe, S.; Maes, P.; Slechten, B.; Raymenants, J.; André, E.; Leyssen, P.; Neyts, J.; Jochmans, D. Remdesivir, molnupiravir and nirmatrelvir remain active against SARS-CoV-2 Omicron and other variants of concern. Antiviral Res. 2022, 198, 105252. [Google Scholar] [CrossRef]
- Italian Medicines Agency. Remdesivir in the Therapy of Adult Patients with COVID-19. 2020. Available online: https://www.aifa.gov.it/documents/20142/1267737/Remdesivir_EN_24.11.2020.pdf (accessed on 24 November 2020).
- Breccia, M.; Olimpieri, P.P.; Olimpieri, O.; Pane, F.; Iurlo, A.; Foggi, P.; Cirilli, A.; Colatrella, A.; Cuomo, M.; Gozzo, L.; et al. How many chronic myeloid leukemia patients who started a frontline second-generation tyrosine kinase inhibitor have to switch to a second-line treatment? A retrospective analysis from the monitoring registries of the Italian medicines agency (AIFA). Cancer Med. 2020, 9, 4160–4165. [Google Scholar] [CrossRef] [Green Version]
- Onder, G.; Olimpieri, P.P.; Celant, S.; Di Lenarda, A.; Ambrosio, G.; Reboldi, G.; Gensini, G.; Colatrella, A.; Palmer, K.; Gabrielli, D.; et al. AIFA Monitoring Registries Group. Under-prescription of direct oral anticoagulants for treatment of non-valvular atrial fibrillation and venous thromboembolism in the COVID-19 lockdown period. Eur. J. Prev. Cardiol. 2021, 29, e149–e152. [Google Scholar] [CrossRef]
- Riccardo, F.; Ajelli, M.; Andrianou, X.D.; Bella, A.; Del Manso, M.; Fabiani, M.; Bellino, S.; Boros, S.; Urdiales, A.M.; Marziano, V.; et al. Epidemiological characteristics of COVID-19 cases and estimates of the reproductive numbers 1 month into the epidemic, Italy, 28 January to 31 March 2020. Eurosurveillance 2020, 25, 2000790. [Google Scholar] [CrossRef]
- Therneau, T.M.; Crowson, C.S.; Atkinson, E.J. Adjusted Survival Curves. 2015. Available online: https://cran.r-project.org/web/packages/survival/vignettes/adjcurve.pdf (accessed on 8 September 2021).
- Frost, M.T.; Jimenez-Solem, E.; Ankarfeldt, M.Z.; Nyeland, M.E.; Andreasen, A.H.; Petersen, T.S. The Adaptive COVID-19 Treatment Trial-1 (ACTT-1) in a real-world population: A comparative observational study. Crit. Care 2020, 24, 677. [Google Scholar] [CrossRef]
- Ferroni, E.; Rossi, P.G.; Alegiani, S.S.; Trifirò, G.; Pitter, G.; Leoni, O.; Cereda, D.; Marino, M.; Pellizzari, M.; Fabiani, M.; et al. Survival of hospitalized COVID-19 patients in Northern Italy: A population-based cohort study by the ITA-COVID-19 Network. Clin. Epidemiol. 2020, 12, 1337–1346. [Google Scholar] [CrossRef]
- Kumar, A.; Narayan, R.K.; Kulandhasamy, M.; Prasoon, P.; Kumari, C.; Kumar, S.; Pareek, V.; Sesham, K.; Shekhawat, P.S.; Kant, K.; et al. COVID-19 pandemic: Insights into molecular mechanisms leading to sex-based differences in patient outcomes. Expert. Rev. Mol. Med. 2021, 23, e7. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Azoulay, E.; Al-Dorzi, H.M.; Phua, J.; Salluh, J.; Binnie, A.; Hodgson, C.; Angus, D.C.; Cecconi, M.; Du, B.; et al. How the COVID-19 pandemic will change the future of critical care. Intensive Care Med. 2021, 47, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, L.; Vanacore, N.; Donfrancesco, C.; Noce, C.L.; Canevelli, M.; Punzo, O.; Raparelli, V.; Pezzotti, P.; Riccardo, F.; Bella, A.; et al. Clinical characteristics of hospitalized individuals dying with COVID-19 by age group in Italy. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1796–1800. [Google Scholar] [CrossRef] [PubMed]
- Italian Medicine Agency. Corticosteroids in the Therapy of Adult Patients with COVID-19. 2020. Available online: https://www.aifa.gov.it/documents/20142/1267737/Corticosteroids_EN_06.10.2020.pdf/ (accessed on 6 October 2020).



{kind=link}
{kind=link}
| Characteristics | n (%) 16,462 |
|---|---|
| Gender, female | 5430 (32.99%) |
| Gender, male | 11,032 (67.01%) |
| Age, median (1st–3rd q) | 66.87 (56.78–76.81) |
| Age, mean (sd) | 66.34 (13.70) |
| Age, 39− | 541 (3.29%) |
| Age, 40–64 | 6925 (42.07%) |
| Age, 65+ | 8996 (54.65%) |
| DAP, 0–2 | 13,791 (83.77%) |
| DAP, 3–5 | 1886 (11.46%) |
| DAP, 6–9 | 497 (3.02%) |
| DAP, 10+ | 288 (1.75%) |
| AAR High | 4904 (29.79%) |
| AAR Intermediate | 7467 (45.36%) |
| AAR Low | 4091 (24.85%) |
| Baseline Characteristics | HR | Low 95% CI | High 95% CI |
| Gender, M vs. F | 1.28 | 1.16 | 1.42 |
| Age, 40–64 vs. <40 years | 2.14 | 1.06 | 4.33 |
| Age, ≥65 vs. <40 years | 13.05 | 6.52 | 26.16 |
| AAR Intermediate vs. Low | 0.97 | 0.86 | 1.09 |
| AAR High vs. Low | 0.85 | 0.75 | 0.97 |
| DAP 3–5 vs. 0–2 | 1.39 | 1.22 | 1.58 |
| Cox-adjusted mortality by day-15 estimates | % | Low 95% CI | High 95% CI |
| <40 | 1.16 | 0.23 | 2.08 |
| 40–65 | 1.83 | 1.47 | 2.19 |
| ≥65 | 12.03 | 10.79 | 13.26 |
| Sex, F | 6.26 | 5.41 | 7.09 |
| Sex, M | 7.83 | 6.97 | 8.68 |
| DAP, 0–2 | 6.89 | 6.14 | 7.62 |
| DAP, 3–5 | 9.85 | 8.29 | 11.38 |
| AAR Low | 7.82 | 6.75 | 8.87 |
| AAR Intermediate | 7.32 | 6.5 | 8.12 |
| AAR High | 6.8 | 5.91 | 7.67 |
| Cox-adjusted mortality by day-29 estimates | % | Low 95% CI | High 95% CI |
| <40 | 1.54 | 0.47 | 2.61 |
| 40–65 | 3.28 | 2.76 | 3.79 |
| ≥65 | 18.32 | 16.61 | 20.00 |
| Sex, F | 9.67 | 8.53 | 10.79 |
| Sex, M | 12.16 | 10.96 | 13.34 |
| DAP, 0–2 | 10.80 | 9.73 | 11.86 |
| DAP, 3–5 | 14.46 | 12.50 | 16.37 |
| AAR Low | 11.94 | 10.55 | 13.29 |
| AAR Intermediate | 11.59 | 10.47 | 12.68 |
| AAR High | 10.32 | 9.17 | 11.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, P.; Tacconelli, E.; Olimpieri, P.P.; Celant, S.; Colatrella, A.; Tomassini, L.; Palù, G. Mortality in SARS-CoV-2 Hospitalized Patients Treated with Remdesivir: A Nationwide, Registry-Based Study in Italy. Viruses 2022, 14, 1197. https://doi.org/10.3390/v14061197
Russo P, Tacconelli E, Olimpieri PP, Celant S, Colatrella A, Tomassini L, Palù G. Mortality in SARS-CoV-2 Hospitalized Patients Treated with Remdesivir: A Nationwide, Registry-Based Study in Italy. Viruses. 2022; 14(6):1197. https://doi.org/10.3390/v14061197
Chicago/Turabian StyleRusso, Pierluigi, Evelina Tacconelli, Pier Paolo Olimpieri, Simone Celant, Antonietta Colatrella, Luca Tomassini, and Giorgio Palù. 2022. "Mortality in SARS-CoV-2 Hospitalized Patients Treated with Remdesivir: A Nationwide, Registry-Based Study in Italy" Viruses 14, no. 6: 1197. https://doi.org/10.3390/v14061197
APA StyleRusso, P., Tacconelli, E., Olimpieri, P. P., Celant, S., Colatrella, A., Tomassini, L., & Palù, G. (2022). Mortality in SARS-CoV-2 Hospitalized Patients Treated with Remdesivir: A Nationwide, Registry-Based Study in Italy. Viruses, 14(6), 1197. https://doi.org/10.3390/v14061197