
Antiviral Efficacy of Molnupiravir for COVID-19 Treatment

Abstract
:1. Introduction
2. Methods
3. Parameter Calibration of Within-Host Modeling
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oliver, N.; Lepri, B.; Sterly, H.; Lambiotte, R.; Deletaille, S.; De Nadai, M.; Letouzé, E.; Salah, A.A.; Benjamins, R.; Cattuto, C.; et al. Mobile Phone Data for Informing Public Health Actions across the COVID-19 Pandemic Life Cycle. Sci. Adv. 2020, 6, eabc0764. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, D.; Markard, J. A COVID-19 Recovery for Climate. Science 2020, 368, 447. [Google Scholar] [CrossRef] [PubMed]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, C.; Wu, K.J.; Corum, J.; Kristoffersen, M. Coronavirus Drug and Treatment Tracker. The New York Times, 23 October 2020; 10–27. [Google Scholar]
- Kozlov, M. Merck’s COVID Pill Loses Its Lustre: What That Means for the Pandemic. Nature 2021. [Google Scholar] [CrossRef]
- Fatehi, F.; Bingham, R.J.; Dykeman, E.C.; Stockley, P.G.; Twarock, R. Comparing Antiviral Strategies against COVID-19 via Multiscale within-Host Modelling. R. Soc. Open Sci. 2021, 8, 210082. [Google Scholar] [CrossRef]
- Gonçalves, A.; Bertrand, J.; Ke, R.; Comets, E.; de Lamballerie, X.; Malvy, D.; Pizzorno, A.; Terrier, O.; Rosa Calatrava, M.; Mentré, F.; et al. Timing of Antiviral Treatment Initiation Is Critical to Reduce SARS-CoV-2 Viral Load. CPT Pharm. Syst. Pharmacol. 2020, 9, 509–514. [Google Scholar] [CrossRef]
- Hernandez Vargas, E.A.; Velasco-Hernandez, J.X. In-Host Modelling of COVID-19 Kinetics in Humans. Infect. Dis. (Except HIV/AIDS) 2020. [Google Scholar] [CrossRef] [Green Version]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation Period of 2019 Novel Coronavirus (2019-nCoV) Infections among Travellers from Wuhan, China, 20–28 January 2020. Euro. Surveill. 2020, 25, 2000062. [Google Scholar] [CrossRef] [Green Version]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological Assessment of Hospitalized Patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Traynard, P.; Ayral, G.; Twarogowska, M.; Chauvin, J. Efficient Pharmacokinetic Modeling Workflow with the MonolixSuite: A Case Study of Remifentanil. CPT Pharm. Syst. Pharmacol. 2020, 9, 198–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, Y.D.; Ejima, K.; Kim, K.S.; Iwanami, S.; Bento, A.I.; Fujita, Y.; Jung, I.H.; Aihara, K.; Watashi, K.; Miyazaki, T.; et al. Revisiting the Guidelines for Ending Isolation for COVID-19 Patients. Elife 2021, 10, e69340. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, I. Within Host Dynamics of SARS-CoV-2 in Humans: Modeling Immune Responses and Antiviral Treatments. SN Comp. Sci. 2021, 2, 482. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Vargas, E.A.; Velasco-Hernandez, J.X. In-Host Mathematical Modelling of COVID-19 in Humans. Annu. Rev. Control 2020, 50, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Jenner, A.L.; Aogo, R.A.; Alfonso, S.; Crowe, V.; Deng, X.; Smith, A.P.; Morel, P.A.; Davis, C.L.; Smith, A.M.; Craig, M. COVID-19 Virtual Patient Cohort Suggests Immune Mechanisms Driving Disease Outcomes. PLoS Pathog. 2021, 17, e1009753. [Google Scholar] [CrossRef]
- Fischer, W.A., 2nd; Eron, J.J., Jr.; Holman, W.; Cohen, M.S.; Fang, L.; Szewczyk, L.J.; Sheahan, T.P.; Baric, R.; Mollan, K.R.; Wolfe, C.R.; et al. A Phase 2a Clinical Trial of Molnupiravir in Patients with COVID-19 Shows Accelerated SARS-CoV-2 RNA Clearance and Elimination of Infectious Virus. Sci. Transl. Med. 2022, 14, eabl7430. [Google Scholar] [CrossRef]
- Du, Z.; Nugent, C.; Galvani, A.P.; Krug, R.M.; Meyers, L.A. Modeling Mitigation of Influenza Epidemics by Baloxavir. Nat. Commun. 2020, 11, 2750. [Google Scholar] [CrossRef]
- Vegvari, C.; Hadjichrysanthou, C.; Cauët, E.; Lawrence, E.; Cori, A.; de Wolf, F.; Anderson, R.M. How Can Viral Dynamics Models Inform Endpoint Measures in Clinical Trials of Therapies for Acute Viral Infections? PLoS ONE 2016, 11, e0158237. [Google Scholar] [CrossRef] [Green Version]
- Benlloch, J.-M.; Cortés, J.-C.; Martínez-Rodríguez, D.; Julián, R.-S.; Villanueva, R.-J. Effect of the Early Use of Antivirals on the COVID-19 Pandemic. A Computational Network Modeling Approach. Chaos Solitons Fractals 2020, 140, 110168. [Google Scholar] [CrossRef]
- Office of the Commissioner. Coronavirus (COVID-19) Update: FDA Issues Emergency Use Authorization for Potential COVID-19 Treatment. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-issues-emergency-use-authorization-potential-covid-19-treatment (accessed on 17 July 2020).
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.-Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe COVID-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Preliminary Report. N. Engl. J. Med. 2020, 383, 1813–1836. [Google Scholar] [CrossRef] [PubMed]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.-X.; et al. Compassionate Use of Remdesivir for Patients with Severe COVID-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study. Engineering 2020, 6, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19—Preliminary Report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameter | Estimation | Similar Estimates |
|---|---|---|
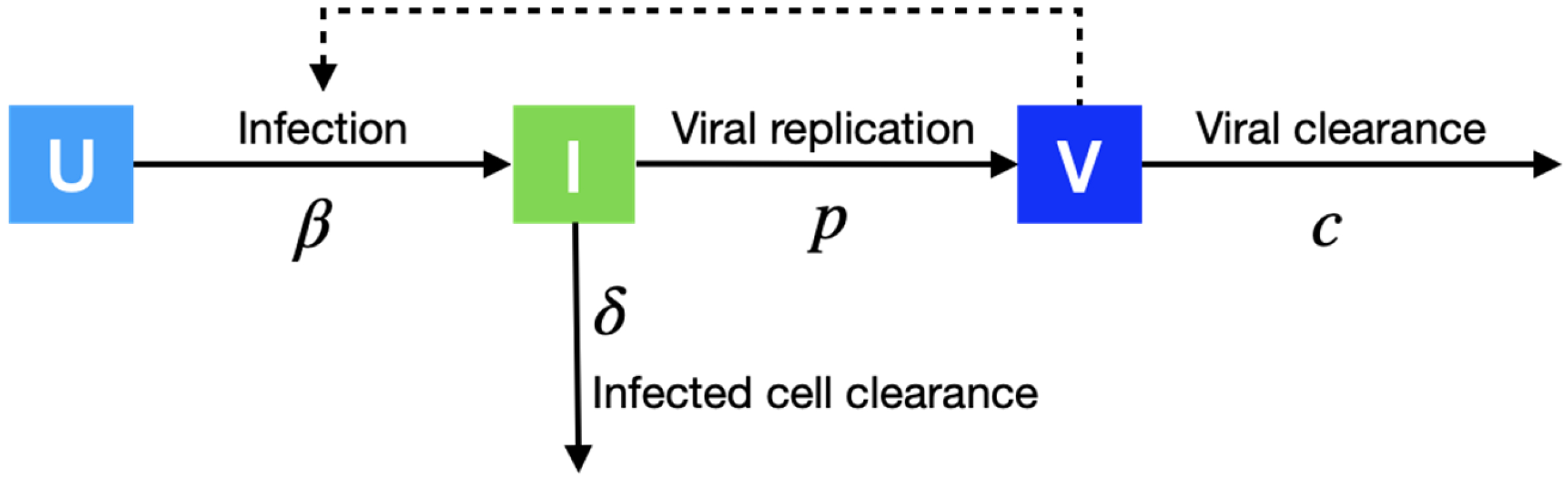
| Cell infection rate in 10−6 days−1 (β) | 2.8 (95% CI: 2.16, 3.69) | 1.6 [12] |
| Infected cell death rate in days−1 (δ) | 0.53 (95% CI: 0.52, 0.54) | 0.65 [13] |
| Virus production rate in Copies/mL in days−1 (p) | 10.96 (95% CI: 9.65, 12.40) | 8.57 (95% CI: 5.01, 12.58) [14] |
| Virus death rate in days−1 (c) | 1.33 (95% CI: 1.26, 1.41) | 1.75 (95% CI: 0, 3.55) [6] |
| Antiviral efficacy (ϵ) | 0.56 (95% CI: 0.49, 0.64) | Not appliable |
| Parameter | Scenario V1 | Scenario V2 | Scenario V3 | Scenario V4 |
|---|---|---|---|---|
| Initial number of viruses in copies/mL (V0), assumed | 1 | 10 | 100 | 1000 |
| Cell infection rate in 10−6 days−1 (), calibrated | 1.74 (95% CI:1.27, 2.42) | 0.87 (95% CI:0.73, 1.03) | 1.36 (95% CI:0.94, 1.97) | 1.15 (95% CI:0.74, 1.8) |
| Infected cell death rate in days−1 (), calibrated | 0.54 (95% CI:0.53, 0.55) | 0.53 (95% CI:0.52, 0.54) | 0.53 (95% CI:0.52, 0.54) | 0.53 (95% CI:0.52, 0.53) |
| Virus production rate in Copies/mL in days−1 (p), calibrated | 12.01 (95% CI:9.97, 14.52) | 10.55 (95% CI:8.38, 13.34) | 11.29 (95% CI:9.93, 13.03) | 12.26 (95% CI:10.88, 13.9) |
| Virus death rate in days−1 (c), calibrated | 1.35 (95% CI:1.27, 1.43) | 1.51 (95% CI:1.43, 1.6) | 1.29 (95% CI:1.17, 1.43) | 1.36 (95% CI:1.28, 1.45) |
| Antiviral efficacy (), calibrated | 0.55 (95% CI:0.45, 0.65) | 0.55 (95% CI:0.47, 0.63) | 0.62 (95% CI:0.54, 0.69) | 0.53 (95% CI:0.45, 0.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, Y.; Shen, M.; Zhang, L. Antiviral Efficacy of Molnupiravir for COVID-19 Treatment. Viruses 2022, 14, 763. https://doi.org/10.3390/v14040763
Bai Y, Shen M, Zhang L. Antiviral Efficacy of Molnupiravir for COVID-19 Treatment. Viruses. 2022; 14(4):763. https://doi.org/10.3390/v14040763
Chicago/Turabian StyleBai, Yuan, Mingwang Shen, and Lei Zhang. 2022. "Antiviral Efficacy of Molnupiravir for COVID-19 Treatment" Viruses 14, no. 4: 763. https://doi.org/10.3390/v14040763
APA StyleBai, Y., Shen, M., & Zhang, L. (2022). Antiviral Efficacy of Molnupiravir for COVID-19 Treatment. Viruses, 14(4), 763. https://doi.org/10.3390/v14040763