
Multisystem Inflammatory Syndrome in Neonates Born to Mothers with SARS-CoV-2 Infection (MIS-N) and in Neonates and Infants Younger Than 6 Months with Acquired COVID-19 (MIS-C): A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
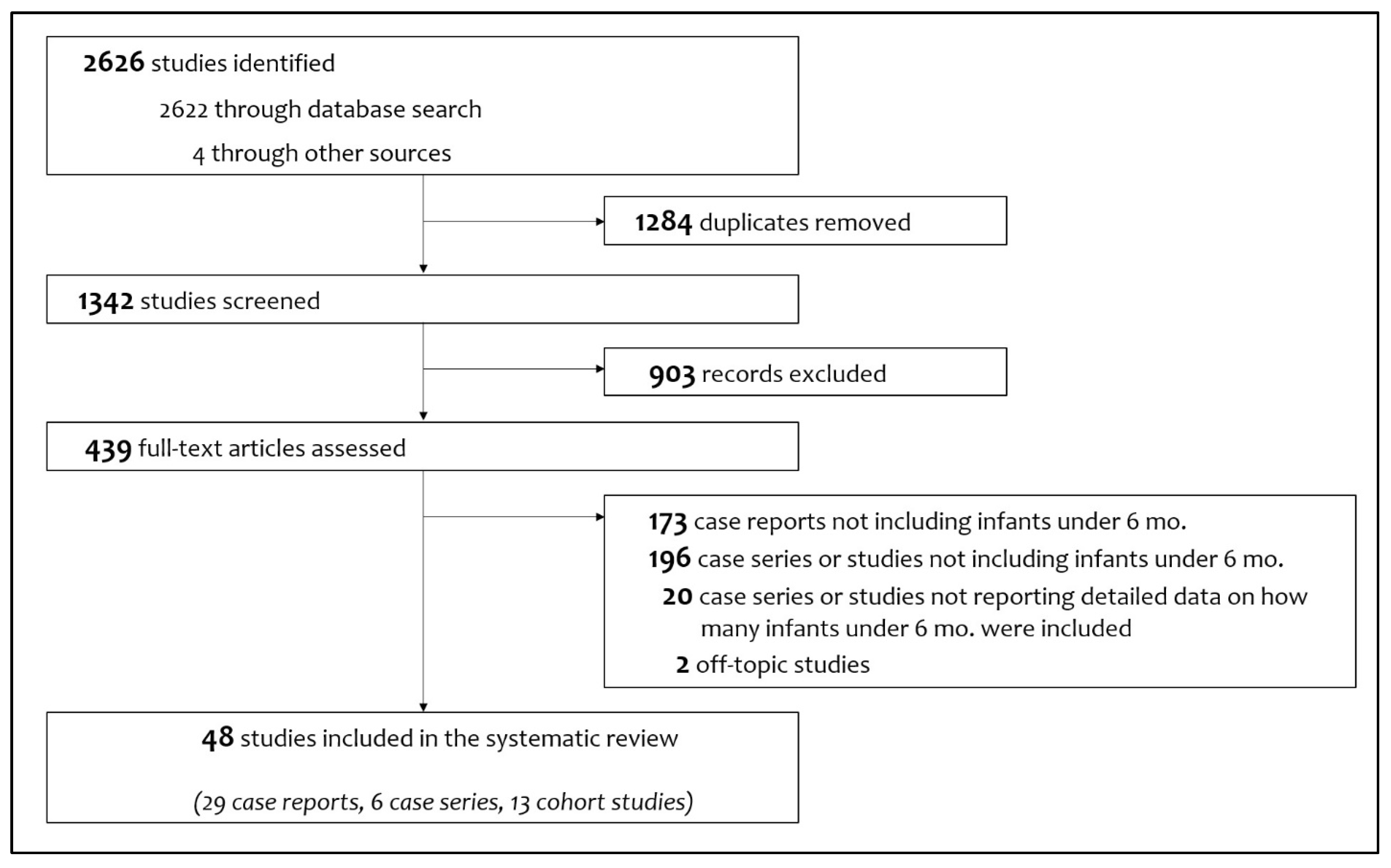
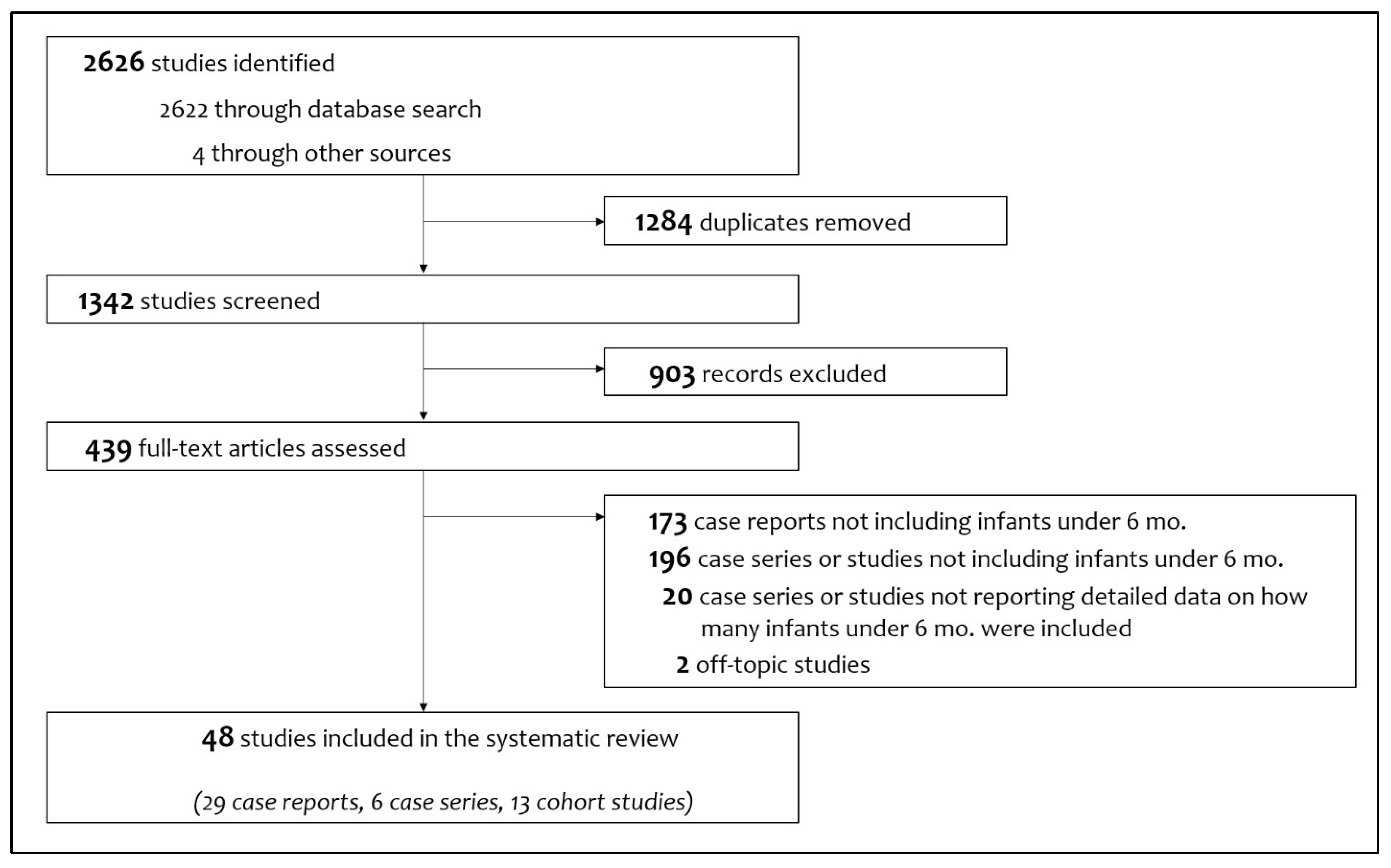
3.1. Workflow of Review and Synthesis
3.2. Neonates with MIS-N
3.3. Neonates and Infants with MIS-C
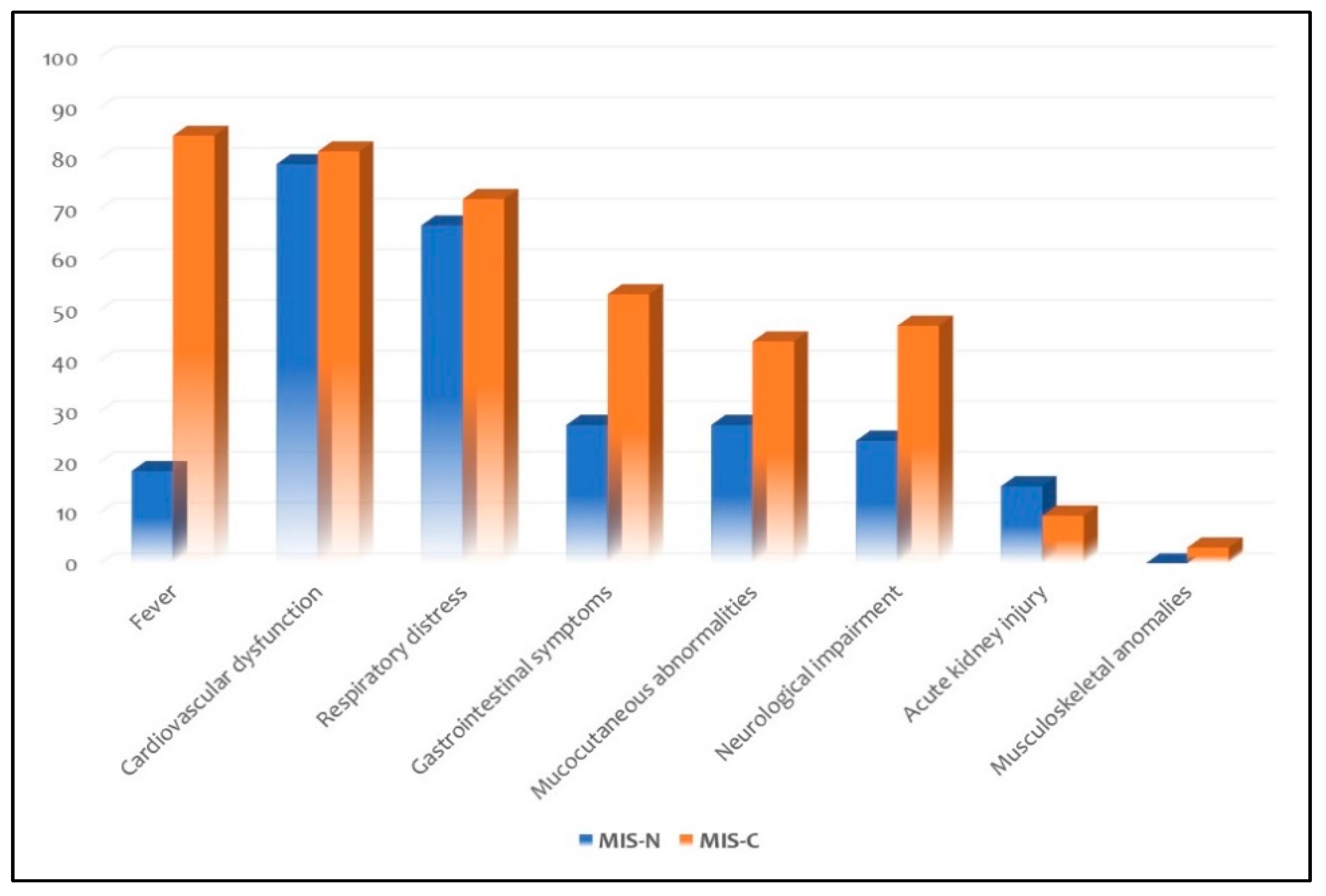
3.4. Differences between Neonates with MIS-N and Neonates with MIS-C
3.5. Incidence of Multisystem Inflammatory Syndrome within Six Months of Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection among Children and Adolescents Compared with Adults: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Auriti, C.; De Rose, D.U.; Mondì, V.; Stolfi, I.; Tzialla, C. Neonatal SARS-CoV-2 Infection: Practical Tips. Pathogens 2021, 10, 611. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, S.; Helve, O.; Andersson, S.; Janér, C.; Süvari, L.; Kaskinen, A. Nasal expression of SARS-CoV-2 entry receptors in newborns. Arch. Dis. Child Fetal Neonatal. Ed. 2022, 107, F95–F97. [Google Scholar] [CrossRef] [PubMed]
- Olivini, N.; Calò Carducci, F.I.; Santilli, V.; De Ioris, M.A.; Scarselli, A.; Alario, D.; Geremia, C.; Lombardi, M.H.; Marabotto, C.; Mariani, R.; et al. A neonatal cluster of novel coronavirus disease 2019: Clinical management and considerations. Ital. J. Ped. 2020, 46, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.; Radia, T.; Harman, K.; Agrawal, P.; Cook, J.; Gupta, A. COVID-19 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: A systematic review of critically unwell children and the association with underlying comorbidities. Eur. J. Ped. 2021, 180, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Tang, K.; Levin, M.; Irfan, O.; Morris, S.K.; Wilson, K.; Klein, J.D.; Bhutta, Z.A. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect. Dis. 2020, 20, e276–e288. [Google Scholar] [CrossRef]
- Soma, V.L.; Shust, G.F.; Ratner, A.J. Multisystem inflammatory syndrome in children. Curr. Opin. Ped. 2021, 33, 152–158. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N. Multisystem Inflammatory Syndrome in Children Related to SARS CoV 2. Pediatr. Drugs. 2021, 23, 1–11. [Google Scholar] [CrossRef]
- Morris, S.B.; Schwartz, N.G.; Patel, P.; Abbo, L.; Beauchamps, L.; Balan, S.; Lee, E.H.; Paneth-Pollak, R.; Geevarughese, A.; Lash, M.K.; et al. Case Series of Multisystem Inflammatory Syndrome in Adults Associated with SARS-CoV-2 Infection—United Kingdom and United States, March–August 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1450–1456. [Google Scholar] [CrossRef]
- Pawar, R.; Gavade, V.; Patil, N.; Mali, V.; Girwalkar, A.; Tarkasband, V.; Loya, S.; Chavan, A.; Nanivadekar, N.; Shinde, R.; et al. Neonatal multisystem inflammatory syndrome (MIS-N) associated with prenatal maternal SARS-CoV-2: A case series. Children 2021, 8, 572. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acharyya, B.C.; Acharyya, S.; Das, D. Novel Coronavirus Mimicking Kawasaki Disease in an Infant. Indian Pediatr. 2020, 57, 753–754. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, G.; Wazir, S.; Arora, A.; Sethi, S.K. Multisystem inflammatory syndrome in a neonate masquerading as surgical abdomen. BMJ Case Rep. 2021, 14, e246579. [Google Scholar] [CrossRef]
- Amonkar, P.S.; Gavhane, J.B.; Kharche, S.N.; Kadam, S.S.; Bhusare, D.B. Aortic thrombosis in a neonate with COVID-19-related fetal inflammatory response syndrome requiring amputation of the leg: A case report. Paediatr. Int. Child Health 2021, 41, 211–216. [Google Scholar] [CrossRef]
- Cui, Y.; Tian, M.; Huang, D.; Wang, X.; Huang, Y.; Fan, L.; Wang, L.; Chen, Y.; Liu, W.; Zhang, K.; et al. A 55-day-old female infant infected with 2019 novel coronavirus disease: Presenting with pneumonia, liver injury, and heart damage. J. Infect. Dis. 2020, 221, 1775–1780. [Google Scholar] [CrossRef]
- Del Barba, P.; Canarutto, D.; Sala, E.; Frontino, G.; Guarneri, M.P.; Camesasca, C.; Baldoli, C.; Esposito, A.; Barera, G. COVID-19 cardiac involvement in a 38-day old infant. Pediatr. Pulmonol. 2020, 55, 1879–1881. [Google Scholar] [CrossRef]
- Diggikar, S.; Nanjegowda, R.; Kumar, A.; Kumar, V.; Kulkarni, S.; Venkatagiri, P. Neonatal Multisystem Inflammatory Syndrome secondary to SARS-CoV-2 infection. J. Paediatr. Child Health 2021, 2–4. [Google Scholar] [CrossRef]
- Divekar, A.A.; Patamasucon, P.; Benjamin, J.S. Presumptive Neonatal Multisystem Inflammatory Syndrome in Children Associated with Coronavirus Disease 2019. Am. J. Perinatol. 2021, 38, 632–636. [Google Scholar] [CrossRef]
- Diwakar, K.; Gupta, B.K.; Uddin, M.W.; Sharma, A.; Jhajra, S. Multisystem inflammatory syndrome with persistent neutropenia in neonate exposed to SARS-CoV-2 virus: A case report and review of literature. J. Neonatal. Perinatal. Med. 2021, 1–5. [Google Scholar] [CrossRef]
- Dugue, R.; Cay-Martínez, K.C.; Thakur, K.T.; Garcia, J.A.; Chauhan, L.V.; Williams, S.H.; Briese, T.; Jain, K.; Foca, M.; McBrian, D.K.; et al. Neurologic manifestations in an infant with COVID-19. Neurology 2020, 94, 1100–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frauenfelder, C.; Brierley, J.; Whittaker, E.; Perucca, G.; Bamford, A. Infant with SARS-CoV-2 infection causing severe lung disease treated with remdesivir. Pediatrics 2020, 146, e20201701. [Google Scholar] [CrossRef] [PubMed]
- García-Howard, M.; Herranz-Aguirre, M.; Moreno-Galarraga, L.; Urretavizcaya-Martínez, M.; Alegría-Echauri, J.; Gorría-Redondo, N.; Planas-Serra, L.; Schlüter, A.; Gut, M.; Pujol, A.; et al. Case Report: Benign Infantile Seizures Temporally Associated With COVID-19. Front. Pediatr. 2020, 8, 507. [Google Scholar] [CrossRef]
- Giacomet, V.; Manfredini, V.A.; Meraviglia, G.; Peri, C.F.; Sala, A.; Longoni, E.; Gasperetti, A.; Stracuzzi, M.; Mannarino, S.; Zuccotti, G.V. Acute inflammation and elevated cardiac markers in a two-month-old infant with severe acute respiratory syndrome coronavirus 2 infection presenting with cardiac symptoms. Pediatr. Infect. Dis. J. 2020, 39, e149–e151. [Google Scholar] [CrossRef] [PubMed]
- Kappanayil, M.; Balan, S.; Alawani, S.; Mohanty, S.; Leeladharan, S.P.; Gangadharan, S.; Jayashankar, J.P.; Jagadeesan, S.; Kumar, A.; Gupta, A.; et al. Multisystem inflammatory syndrome in a neonate, temporally associated with prenatal exposure to SARS-CoV-2: A case report. Lancet Child Adolesc. Health 2021, 5, 304–308. [Google Scholar] [CrossRef]
- Khaund Borkotoky, R.; Banerjee Barua, P.; Paul, S.P.; Heaton, P.A. COVID-19-Related Potential Multisystem Inflammatory Syndrome in Childhood in a Neonate Presenting as Persistent Pulmonary Hypertension of the Newborn. Pediatr. Infect. Dis. J. 2021, 40, e162–e164. [Google Scholar] [CrossRef] [PubMed]
- Jones, V.G.; Mills, M.; Suarez, D.; Hogan, C.A.; Yeh, D.; Segal, J.B.; Nguyen, E.L.; Barsh, G.R.; Maskatia, S.; Mathew, R. COVID-19 and Kawasaki Disease: Novel Virus and Novel Case. Hosp. Pediatr. 2020, 10, 537–540. [Google Scholar] [CrossRef]
- Lad, S.S.; Suryawanshi, P.B.; Jadhav, P.; Kait, S.P.; Lad, P.; Mujawar, J.; Khetre, R.; Kataria, P.; Balte, P.; Neela, A.; et al. Fresh Per Rectal Bleeding in Pediatric Inflammatory Multisystem Syndrome Temporally Associated with SARS-CoV-2 (PIMS-TS). Indian J. Pediatr. 2021, 88, 607. [Google Scholar] [CrossRef]
- Lima, A.; Cardoso, C.C.; Bentim, P.; Voloch, C.M.; Rossi, Á.D.; da Costa, R.; da Paz, J.; Agostinho, R.F.; Figueiredo, V.; Júnior, J.; et al. Maternal SARS-CoV-2 Infection Associated to Systemic Inflammatory Response and Pericardial Effusion in the Newborn: A Case Report. J. Pediatr. Infect. Dis. Soc. 2021, 10, 536–539. [Google Scholar] [CrossRef]
- Lorenz, N.; Treptow, A.; Schmidt, S.; Hofmann, R.; Raumer-Engler, M.; Heubner, G.; Gröber, K. Neonatal Early-Onset infection with SARS-CoV-2 in a newborn presenting with encephalitic symptoms. Pediatr. Infect. Dis. J. 2020, 39, e212. [Google Scholar] [CrossRef]
- Luna Santiago, L.; Aguilar-Martinez, N.; Cabanas-Espinosa, B.; Ramirez-Machuca, X. SARS-CoV-2-related multisystem inflammatory syndrome in familial refractory hemophagocytic lymphohistiocytosis: A case report. Pediatr. Crit. Care Med. 2021, 22, 352. [Google Scholar] [CrossRef]
- Mariani, R.; Liu, H. Severe transient pancytopenia with dyserythropoiesis and dysmegakaryopoiesis in COVID-19–associated MIS-C. Blood 2020, 136, 2964. [Google Scholar] [CrossRef] [PubMed]
- McCarty, K.L.; Tucker, M.; Lee, G.; Pandey, V. Fetal inflammatory response syndrome associated with maternal SARS-CoV-2 infection. Pediatrics 2021, 147, e2020010132. [Google Scholar] [CrossRef] [PubMed]
- Orlanski-Meyer, E.; Yogev, D.; Auerbach, A.; Megged, O.; Glikman, D.; Hashkes, P.J.; Bar-Meir, M. Multisystem Inflammatory syndrome in children associated with SARS-CoV-2 in an 8-week old infant. J. Pediatr. Infect. Dis. Soc. 2020, 9, 781–784. [Google Scholar] [CrossRef]
- Raut, S.; Roychowdhoury, S.; Bhakta, S.; Sarkar, M.; Nandi, M. Incomplete Kawasaki Disease as Presentation of COVID-19 Infection in an Infant: A Case Report. J. Trop. Pediatr. 2021, 67, 1–4. [Google Scholar] [CrossRef]
- Rodriguez-Gonzalez, M.; Rodríguez-Campoy, P.; Sánchez-Códez, M.; Gutiérrez-Rosa, I.; Castellano-Martinez, A.; Rodríguez-Benítez, A. New onset severe right ventricular failure associated with COVID-19 in a young infant without previous heart disease. Cardiol. Young. 2020, 30, 1346–1349. [Google Scholar] [CrossRef]
- Saha, S.; Pal, P.; Mukherjee, D. Neonatal MIS-C: Managing the Cytokine Storm. Pediatrics 2021, 148, e2020042093. [Google Scholar] [CrossRef]
- Schoenmakers, S.; Snijder, P.; Verdijk, R.M.; Kuiken, T.; Kamphuis, S.; Koopman, L.P.; Krasemann, T.B.; Rousian, M.; Broekhuizen, M.; Steegers, E.; et al. Severe acute respiratory syndrome coronavirus 2 placental infection and inflammation leading to fetal distress and neonatal multi-organ failure in an asymptomatic woman. J. Pediatr. Infect. Dis. Soc. 2021, 10, 556–561. [Google Scholar] [CrossRef]
- Shaiba, L.A.; Hadid, A.; Altirkawi, K.A.; Bakheet, H.M.; Alherz, A.M.; Hussain, S.A.; Sobaih, B.H.; Alnemri, A.M.; Almaghrabi, R.; Ahmed, M.; et al. Case Report: Neonatal Multi-System Inflammatory Syndrome Associated With SARS-CoV-2 Exposure in Two Cases from Saudi Arabia. Front. Pediatr. 2021, 6, 652857. [Google Scholar] [CrossRef]
- Richardson, K.L.; Jain, A.; Evans, J.; Uzun, O. Giant coronary artery aneurysm as a feature of coronavirus-related inflammatory syndrome. BMJ Case Rep. 2021, 14, 1–6. [Google Scholar] [CrossRef]
- Malle, L.; Bastard, P.; Martin-Nalda, A.; Carpenter, T.; Bush, D.; Patel, R.; Colobran, R.; Soler-Palacin, P.; Casanova, J.L.; Gans, M.; et al. Atypical Inflammatory Syndrome Triggered by SARS-CoV-2 in Infants with Down Syndrome. J. Clin. Immunol. 2021, 41, 1457–1462. [Google Scholar] [CrossRef] [PubMed]
- Marino, A.; Varisco, T.; Quattrocchi, G.; Amoroso, A.; Beltrami, D.; Venturiello, S.; Ripamonti, A.; Villa, A.; Andreotti, M.; Ciuffreda, M.; et al. Children with Kawasaki disease or Kawasaki-like syndrome (MIS-C/PIMS) at the time of COVID-19: Are they all the same? Case series and literature review. Reumatismo 2021, 73, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Rakha, S.; Sobh, A.; Hager, A.H.; Hafez, M.; Alsawah, G.A.; Abuelkheir, M.M.; Zeid, M.S.; Nahas, M.; Elmarsafawy, H. Cardiac Implications of Multisystem Inflammatory Syndrome Associated with COVID-19 in Children under the age of Five Years. Cardiol. Young. 2021, 1–6. [Google Scholar] [CrossRef]
- Shaiba, L.A.; Altirkawi, K.; Hadid, A.; Alsubaie, S.; Alharbi, O.; Alkhalaf, H.; Alharbi, M.; Alruqaie, N.; Alzomor, O.; Almughaileth, F.; et al. COVID-19 Disease in Infants Less Than 90 Days: Case Series. Front. Pediatr. 2021, 9, 1–8. [Google Scholar] [CrossRef]
- Villacis-Nunez, D.S.; Hashemi, S.; Nelson, M.C.; Flanagan, E.; Thakral, A.; Rodriguez, F., 3rd; Jaggi, P.; Oster, M.E.; Prahalad, S.; Rouster-Stevens, K.A. Giant Coronary Aneurysms in Multisystem Inflammatory Syndrome in Children Associated with SARS-CoV-2 Infection. JACC Case Rep. 2021, 3, 1499–1508. [Google Scholar] [CrossRef]
- Abdel-Haq, N.; Asmar, B.I.; Deza Leon, M.P.; McGrath, E.J.; Arora, H.S.; Cashen, K.; Tilford, B.; Charaf Eddine, A.; Sethuraman, U.; Ang, J.Y. SARS-CoV-2-associated multisystem inflammatory syndrome in children: Clinical manifestations and the role of infliximab treatment. Eur. J. Pediatr. 2021, 180, 1581–1591. [Google Scholar] [CrossRef]
- Alharbi, M.; Kazzaz, Y.M.; Hameed, T.; Alqanatish, J.; Alkhalaf, H.; Alsadoon, A.; Alayed, M.; Hussien, S.A.; Shaalan, M.A.; Al Johani, S.M. SARS-CoV-2 infection in children, clinical characteristics, diagnostic findings and therapeutic interventions at a tertiary care center in Riyadh, Saudi Arabia. J. Infect. Public Health 2021, 14, 446–453. [Google Scholar] [CrossRef]
- Antúnez-Montes, O.Y.; Escamilla, M.I.; Figueroa-Uribe, A.F.; Arteaga-Menchaca, E.; Lavariega-Saráchaga, M.; Salcedo-Lozada, P.; Melchior, P.; de Oliveira, R.B.; Tirado Caballero, J.C.; Redondo, H.P.; et al. COVID-19 and Multisystem Inflammatory Syndrome in Latin American Children: A Multinational Study. Pediatr. Infect. Dis. J. 2020, 40, e1–e6. [Google Scholar] [CrossRef]
- Caro-Domínguez, P.; Navallas, M.; Riaza-Martin, L.; Ghadimi Mahani, M.; Ugas Charcape, C.F.; Valverde, I.; D’Arco, F.; Toso, S.; Shelmerdine, S.C.; van Schuppen, J.; et al. Imaging findings of multisystem inflammatory syndrome in children associated with COVID-19. Pediatr. Radiol. 2021, 51, 1608–1620. [Google Scholar] [CrossRef]
- Chandran, J.; James, E.J.; Verghese, V.P.; Kumar, T.S.; Sundaravalli, E.; Vyasam, S. Clinical Spectrum of Children with Multisystem Inflammatory Syndrome Associated With SARS-CoV-2 Infection. Indian Pediatr. 2021, 58, 955–958. [Google Scholar] [CrossRef]
- Dufort, E.M.; Koumans, E.H.; Chow, E.J.; Rosenthal, E.M.; Muse, A.; Rowlands, J.; Barranco, M.A.; Maxted, A.M.; Rosenberg, E.S.; Easton, D.; et al. New York State and Centers for Disease Control and Prevention Multisystem Inflammatory Syndrome in Children Investigation Team. Multisystem Inflammatory Syndrome in Children in New York State. N. Engl. J. Med. 2020, 383, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Esteve-Sole, A.; Anton, J.; Pino-Ramirez, R.M.; Sanchez-Manubens, J.; Fumadó, V.; Fortuny, C.; Rios-Barnes, M.; Sanchez-de-Toledo, J.; Girona-Alarcón, M.; Mosquera, J.M.; et al. Similarities and differences between the immunopathogenesis of COVID-19-related pediatric multisystem inflammatory syndrome and Kawasaki disease. J. Clin. Investig. 2021, 131, e144554. [Google Scholar] [CrossRef] [PubMed]
- Falah, N.U.; Hashmi, S.; Ahmed, Z.; Jaan, A.; Akhtar, A.; Khalid, F.; Farooque, U.; Shera, M.T.; Ali, S.; Javed, A. Kawasaki Disease-Like Features in 10 Pediatric COVID-19 Cases: A Retrospective Study. Cureus 2020, 12, e11035. [Google Scholar] [CrossRef] [PubMed]
- Godfred-Cato, S.; Tsang, C.A.; Giovanni, J.; Abrams, J.; Oster, M.E.; Lee, E.H.; Lash, M.K.; Le Marchand, C.; Liu, C.Y.; Newhouse, C.N.; et al. Multisystem Inflammatory Syndrome in Infants <12 months of Age, United States, May 2020–January 2021. Pediatr. Infect. Dis. J. 2021, 40, 601–605. [Google Scholar] [CrossRef]
- Grewal, M.K.; Gregory, M.J.; Jain, A.; Mohammad, D.; Cashen, K.; Ang, J.Y.; Thomas, R.L.; Valentini, R.P. Acute Kidney Injury in Pediatric Acute SARS-CoV-2 Infection and Multisystem Inflammatory Syndrome in Children (MIS-C): Is There a Difference? Front. Pediatr. 2021, 9, 692256. [Google Scholar] [CrossRef] [PubMed]
- Güllü, U.U.; Güngör, Ş.; İpek, S.; Yurttutan, S.; Dilber, C. Predictive value of cardiac markers in the prognosis of COVID-19 in children. Am. J. Emerg. Med. 2021, 48, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Mehra, B.; Pandey, M.; Gupta, D.; Oberoi, T.; Jerath, N.; Sharma, R.; Lal, N.; Singha, C.; Malhotra, B.; Manocha, V.; et al. COVID-19 associated multisystem inflammatory syndrome in children: A multicentric retrospective cohort study. Indian J. Crit. Care Med. 2021, 25, 1174–1180. [Google Scholar]
- Niño-Taravilla, C.; Otaola-Arca, H.; Lara-Aguilera, N.; Zuleta-Morales, Y.; Ortiz-Fritz, P. Multisystem inflammatory syndrome in children, Chile, May-August 2020. Emerg. Infect. Dis. 2021, 27, 1457–1461. [Google Scholar] [CrossRef]
- Yasuhara, J.; Watanabe, K.; Takagi, H.; Sumitomo, N.; Kuno, T. COVID-19 and multisystem inflammatory syndrome in children: A systematic review and meta-analysis. Pediatr. Pulmonol. 2021, 56, 837–848. [Google Scholar] [CrossRef]
- De Rose, D.U.; Coppola, M.; Gallini, F.; Maggio, L.; Vento, G.; Rigante, D. Overview of the rarest causes of fever in newborns: Handy hints for the neonatologist. J. Perinatol. 2021, 41, 372–382. [Google Scholar] [CrossRef]
- Hofer, N.; Müller, W.; Resch, B. Neonates presenting with temperature symptoms: Role in the diagnosis of early onset sepsis. Pediatr. Int. 2012, 54, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Lakshminrusimha, S.; Hudak, M.L.; Dimitriades, V.R.; Higgins, R.D. Multisystem Inflammatory Syndrome in Neonates following Maternal SARS-CoV-2 COVID-19 Infection. Am. J. Perinatol. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hiles, M.; Culpan, A.M.; Watts, C.; Munyombwe, T.; Wolstenhulme, S. Neonatal respiratory distress syndrome: Chest X-ray or lung ultrasound? A systematic review. Ultrasound 2017, 25, 80–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musolino, A.M.; Boccuzzi, E.; Buonsenso, D.; Supino, M.C.; Mesturino, M.A.; Pitaro, E.; Ferro, V.; Nacca, R.; Sinibaldi, S.; Palma, P.; et al. The Role of Lung Ultrasound in Diagnosing COVID-19-Related Multisystemic Inflammatory Disease: A Preliminary Experience. J. Clin. Med. 2022, 11, 234. [Google Scholar] [CrossRef] [PubMed]
- Tissot, C.; Singh, Y. Neonatal functional echocardiography. Curr. Opin. Pediatr. 2020, 32, 235–244. [Google Scholar] [CrossRef]
- Giesinger, R.E.; McNamara, P.J. Hemodynamic instability in the critically ill neonate: An approach to cardiovascular support based on disease pathophysiology. Semin. Perinatol. 2016, 40, 174–188. [Google Scholar] [CrossRef]
- Haghighi Aski, B.; Manafi Anari, A.; Abolhasan Choobdar, F.; Zareh Mahmoudabadi, R.; Sakhaei, M. Cardiac abnormalities due to multisystem inflammatory syndrome temporally associated with COVID-19 among children: A systematic review and meta-analysis. Int. J. Cardiol. Heart Vasc. 2021, 33, 100764. [Google Scholar] [CrossRef]
- Bottari, G.; Damiani, E.; Confalone, V.; Scorcella, C.; Casarotta, E.; Gandolfo, C.; Stoppa, F.; Cecchetti, C.; Donati, A. Microvascular dysfunction in pediatric patients with SARS-COV-2 pneumonia: Report of three severe cases. Microvasc. Res. 2022, 141, 104312. [Google Scholar] [CrossRef]
- Zhao, Y.; Yin, L.; Patel, J.; Tang, L.; Huang, Y. The inflammatory markers of multisystem inflammatory syndrome in children (MIS-C) and adolescents associated with COVID-19: A meta-analysis. J. Med. Virol. 2021, 93, 4358–4369. [Google Scholar] [CrossRef]
- McArdle, A.J.; Vito, O.; Patel, H.; Seaby, E.G.; Shah, P.; Wilson, C.; Broderick, C.; Nijman, R.; Tremoulet, A.H.; Munblit, D.; et al. BATS Consortium. Treatment of Multisystem Inflammatory Syndrome in Children. N. Engl. J. Med. 2021, 385, 1–12. [Google Scholar] [CrossRef]
- Cattalini, M.; Taddio, A.; Bracaglia, C.; Cimaz, R.; Paolera, S.D.; Filocamo, G.; La Torre, F.; Lattanzi, B.; Marchesi, A.; Simonini, G.; et al. Rheumatology Study Group of the Italian Society of Pediatrics. Childhood multisystem inflammatory syndrome associated with COVID-19 (MIS-C): A diagnostic and treatment guidance from the Rheumatology Study Group of the Italian Society of Pediatrics. Ital. J. Pediatr. 2021, 47, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gruber, C.N.; Patel, R.S.; Trachtman, R.; Lepow, L.; Amanat, F.; Krammer, F.; Wilson, K.M.; Onel, K.; Geanon, D.; Tuballes, K.; et al. Mapping systemic inflammation and antibody responses in multisystem inflammatory syndrome in children (MIS-C). Cell 2020, 183, 982–995. [Google Scholar] [CrossRef] [PubMed]
- Kazatchkine, M.D.; Kaveri, S.V. Immunomodulation of autoimmune and inflammatory diseases with Intravenous Immune Globulin. N. Engl. J. Med. 2001, 345, 747–755. [Google Scholar] [CrossRef]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The immunology of multisystem inflammatory syndrome in children with COVID-19. Cell 2020, 183, 968–981.e7. [Google Scholar] [CrossRef]
- Ouldali, N.; Toubiana, J.; Antona, D.; Javouhey, E.; Madhi, F.; Lorrot, M.; Léger, P.L.; Galeotti, C.; Claude, C.; Wiedemann, A.; et al. French COVID-19 Paediatric Inflammation Consortium. Association of Intravenous Immunoglobulins Plus Methylprednisolone vs Immunoglobulins Alone with course of fever in Multisystem Inflammatory Syndrome in Children. JAMA 2021, 325, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Yock-Corrales, A.; Lenzi, J.; Ulloa-Gutiérrez, R.; Gómez-Vargas, J.; Antúnez-Montes, O.Y.; Rios Aida, J.A.; Del Aguila, O.; Arteaga-Menchaca, E.; Campos, F.; Uribe, F.; et al. High rates of antibiotic prescriptions in children with COVID-19 or multisystem inflammatory syndrome: A multinational experience in 990 cases from Latin America. Acta. Paediatr. 2021, 110, 1902–1910. [Google Scholar] [CrossRef]
- Branstetter, J.W.; Barker, L.; Yarbrough, A.; Ross, S.; Stultz, J.S. Challenges of antibiotic stewardship in the pediatric and neonatal intensive care units. J. Pediatr. Pharmacol. Ther. 2021, 26, 659–668. [Google Scholar] [CrossRef]
- De Rose, D.U.; Perri, A.; Auriti, C.; Gallini, F.; Maggio, L.; Fiori, B.; D’Inzeo, T.; Spans, T.; Vento, G. Time to positivity of blood cultures could inform decisions on antibiotics administration in neonatal early-onset sepsis. Antibiotics 2021, 10, 123. [Google Scholar] [CrossRef]
- Kuzniewicz, M.W.; Mukhopadhyay, S.; Li, S.; Walsh, E.M.; Puopolo, K.M. Time to Positivity of Neonatal Blood Cultures for Early-onset Sepsis. Pediatr. Infect. Dis. J. 2020, 39, 634–640. [Google Scholar] [CrossRef]
- Rahmani, S.; Rezaei, N. Omicron (B.1.1.529) variant: Development, dissemination, and dominance. J. Med. Virol. 2022, 94, 1787–1788. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Article Type | Country | Quality Score | Overall Quality | Neonates and Infants < 6 Months with MIS (n) |
|---|---|---|---|---|---|
| Abdel-Haq [46] | Cohort study | United States | N.A. | N.A. | 1 |
| Acharyya [13] | Case report | India | 4 | Intermediate | 1 |
| Agrawal [14] | Case report | India | 6 | Good | 1 |
| Alharbi [47] | Cohort study | Saudi Arabia | 5 | Intermediate | 2 |
| Amonkar [15] | Case report | India | 5 | Intermediate | 1 |
| Antúnez-Montes [48] | Cohort study | Mexico | N.A. | N.A. | 3 |
| Caro-Dominguez [49] | Cohort study | Spain | N.A. | N.A. | 1 |
| Chandran [50] | Cohort study | India | N.A. | N.A. | 3 |
| Cui [16] | Case report | China | 6 | Good | 1 |
| Del Barba [17] | Case report | Italy | 5 | Intermediate | 1 |
| Diggikar [18] | Case report | India | 5 | Intermediate | 1 |
| Divekar [19] | Case report | United States | 5 | Intermediate | 1 |
| Diwakar [20] | Case report | India | 5 | Intermediate | 1 |
| Dugue [21] | Case report | United States | 3 | Intermediate | 1 |
| Dufort [51] | Cohort study | United States | N.A. | N.A. | 1 |
| Esteve-Sole [52] | Cohort study | Spain | 3 | Intermediate | 1 |
| Falah [53] | Cohort study | Pakistan | 3 | Intermediate | 2 |
| Frauenfelder [22] | Case report | United Kingdom | 6 | Good | 1 |
| García-Howard [23] | Case report | Spain | 5 | Intermediate | 1 |
| Giacomet [24] | Case report | Italy | 5 | Intermediate | 1 |
| Godfred-Cato [54] | Cohort study | United States | N.A. | N.A. | 1 |
| Grewal [55] | Cohort study | United States | N.A. | N.A. | 9 |
| Güllü [56] | Cohort study | Turkey | N.A. | N.A. | 3 |
| Kappanyil [25] | Case report | India | 6 | Good | 1 |
| Khaund Borkotoky [26] | Case report | India | 5 | Intermediate | 1 |
| Jones [27] | Case report | United States | 5 | Intermediate | 1 |
| Lad [28] | Case report | India | 2 | Low | 1 |
| Lima [29] | Case report | Brazil | 6 | Good | 1 |
| Lorenz [30] | Case report | Germany | 3 | Intermediate | 1 |
| Luna Santiago [31] | Case report | Mexico | 3 | Intermediate | 1 |
| Malle [41] | Case series | United States | 6 | Good | 1 |
| Mariani [32] | Case report | United States | 3 | Intermediate | 1 |
| Marino [42] | Case series | Italy | 4 | Intermediate | 1 |
| McCarty [33] | Case report | United States | 5 | Intermediate | 1 |
| Mehra [57] | Cohort study | India | N.A. | N.A. | 1 |
| Niño-Taravilla [58] | Cohort study | Chile | 2 | N.A. | 2 |
| Orlanski-Meyer [34] | Case report | Israel | 5 | Intermediate | 1 |
| Pawar [11] | Case series | India | 6 | Good | 20 |
| Rakha [43] | Case series | Egypt | 5 | Intermediate | 5 |
| Raut [35] | Case report | India | 5 | Intermediate | 1 |
| Richardson [40] | Case report | United Kingdom | 6 | Good | 1 |
| Rodriguez-Gonzalez [36] | Case report | Spain | 5 | Intermediate | 1 |
| Saha [37] | Case report | India | 6 | Good | 1 |
| Schoenmakers [38] | Case report | Netherlands | 6 | Good | 1 |
| Shaiba [39] | Case report | Saudi Arabia | 6 | Good | 2 |
| Shaiba [44] | Case series | Saudi Arabia | 5 | Intermediate | 2 |
| Villacis-Nunez [45] | Case series | United States | 6 | Good | 1 |
| Vivanti [5] | Case report | France | 6 | Good | 1 |
| Total of included infants | 90 | ||||
| Subject Number | First Author | Age/ Sex/ Birthweight/GA | Neonatal RT-PCR and Serology for SARS-CoV-2 | Prior Maternal SARS-CoV-2 Exposure | Fever | Organ Involvement | Laboratory Work-Up | Imaging | Treatment | NICU Admission/Need for MV/Length of Hospital Stay | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Agrawal [14] | 44 h/M/3300 g/39 w | RT-PCR neg/IgG pos/IgM neg | YES—positive maternal IgG (without vaccination): she had a history of contact with COVID-19 4 weeks before delivery but remained asymptomatic. | Yes | Hypotension; respiratory distress requiring MV; indurated ulcer with erythema noted on the occiput; non-bilious vomiting and abdominal distension—surgical abdomen | Leukocytosis (23,940), metabolic acidosis (pH 7.18), PCT 10.76, NT-proBNP 4297, D-dimer 1331 | Normal inflation with minimal pulmonary infiltrates bilaterally (CXR); normal echocardiogram; dilated small and large intestines with absence of rectal gas and no radiological evidence of intestinal atresia or NEC (AXR) | IVIG, steroids, inotropes (dopamine), enoxaparin, aspirin | Yes/Yes/16 days | Favorable |
| 2 | Amonkar [15] | 6 days/M/2400 g/full-term | RT-PCR neg/IgG pos/IgM pos | YES—maternal asymptomatic infection with positive IgG and IgM on day 11 of life in both mother and neonate | No | Respiratory distress requiring ventilatory support (not specified); progressive blackish discoloration of the toes of the right lower limb; irritability | Leukocytosis (17,100), CRP 18.6, PCT 1.28, albumin 3, NT-proBNP 12,194, ferritin 515, D-dimer 4110, IL-6 20.29 | Acute thrombosis of abdominal aorta below renal arteries (80–90% occlusion at echocardiogram) | Steroids, r-TPA and surgical embolectomy, aspirin after limb amputation, unfractionated heparin | Yes/No/28 days | Favorable but he required amputation of the leg |
| 3 | Divekar [19] | At birth/F/1300 g/30 w | RT-PCR neg/IgG pos/IgM neg | YES—positive maternal RT-PCR prior to delivery | No | Hypotension and inadequate urine output; hypoxic respiratory failure requiring surfactant and HFOV; generalized anasarca; oliguric renal failure | Tn 189, NT-proBNP >5000, IL-6 21.9 | Cardiomegaly and pulmonary edema (CXR); small pericardial effusion without tamponade, pathological coronary artery dilation and ventricular systolic dysfunction (echocardiogram) | IVIG | Yes/Yes/2 months | Favorable |
| 4 | Diwakar [20] | 19 days/M/3910 g/39 w | RT-PCR neg/Positive IgG | YES—maternal fever a week before delivery; she resulted positive when the baby was admitted | Yes | Rash over forehead and cheeks on day 2; diarrhea | Thrombocytopenia (97 × 109/L), transient neutropenia, CRP 12.13, hyponatremia (127), albumin 2.92, D-dimer 710, IL-6 1624 | Clear lung fields (CXR); normal structure and function with normal coronary arteries (echocardiogram) | IVIG, aspirin | Yes/No/6 days | Favorable |
| 5 | Kappanayil [25] | 24 days/F/3750 g/term | RT-PCR neg/IgG pos/IgM neg | YES—mother with a history of positive RT-PCR, with mild COVID-19 at 31 weeks GA, which was managed with symptomatic and supportive measures. | No | Hypotension and tachycardia; hypoxic respiratory failure; cool peripheries with erythema over the occiput and at bilateral gluteal regions; drowsiness | CRP 0.65, hyper-transamin-asemia (ALT 866 U/L and AST 2240 U/L), metabolic acidosis (pH 7.13), Tn 123, NT-proBNP 157,000, ferritin 56,400, D-dimer 20,000 | Cardiomegaly (CXR); severe biventricular dysfunction; coronary arteries with normal luminal dimensions, but appeared prominent and hyper-choic (echocardiogram) | IVIG, steroids, inotropes (epinephrine and milrinone), furosemide, vitamin C and D, zinc, heparin | Yes/Yes/29 days | Favorable |
| 6 | Khaund Borkotoky [26] | 4 h/M/4840 g/38 w | RT-PCR neg/IgG pos/IgM neg | YES—maternal fever and cough 3 weeks before delivery. On the day of delivery, her throat and nasal swab for COVID-19 PCR were negative. Anti-SARS-CoV-2 IgG were positive. | Yes | PPHN; hypoxic respiratory failure at 4 h of life and again on day 7; vasculitic rash on day 14; features suggestive of early NEC on day 14 | Leukocytosis (19,800), thrombocytopenia (70 × 109/L), CRP 3.91, albumin 2.2, Tn 171.2, NT-proBNP 6125, ferritin 1432, D-dimer >10,000, IL-6 43.49 | Bilateral haze (CXR) and bilateral ground opacities considered consistent with COVID-19 (chest CD); PPHN (echocardiogram) | Steroids, sildenafil, inotropes (dopamine), furosemide | Yes/Yes/34 days | Favorable |
| 7 | Lima [29] | 3 days/F/2400 g/33 w | RT-PCR pos/IgG pos/IgM neg | YES—flu-like symptoms at 29 weeks GA. At 32 weeks, the fetal echocardiogram revealed significant pericardial effusion with dilation of the vena cava and an overload in the cardiovascular system | No | Pericardial effusion; hemodynamic instability or bradycardia; respiratory distress and apnea requiring mechanical ventilation | CRP 1.1, metabolic acidosis (pH 7.12), Tn 38,000, ferritin 358, INR 1.4, D-dimer 2200, IL-6 56.4 in serum and 202.9 in pericardial fluid | Inflammatory ground glass pattern affecting less than 25% of the lung parenchyma (chest CT); pericardial effusion (echocardiogram) | Pericardiocentesis; red blood cell concentrate transfusion, inotropes (not specified amine) | Yes/Yes/23 days | Favorable |
| 8 | Lorenz [30] | 24 h/F/NA/40 w | RT-PCR pos/NA | YES—mother with mild respiratory infection and loss of smell and taste, and fever during delivery (38 °C) | No | Respiratory distress at about 80 h of life, requiring CPAP and oxygen therapy until day 6 of life; encephalitic symptoms (lethargic but severely hyperexcitable, high pitched crying) at 54 h of life | NA | Bilateral viral pneumonia (CXR) | Paracetamol and caffeine | Yes/No/NA | Favorable |
| 9 | McCarty [33] | 1st day/M/NA/34 w | RT-PCR neg/Serology NA | YES—mother with COVID-19 symptoms and positive RT-PCR | Yes | Severe pulmonary hypertension; respiratory distress requiring surfactant, mechanical ventilation and inhaled nitric oxide | Lymphopenia (230 at 48 h of life), thrombocytopenia (25 × 109/L), CRP 6.78, metabolic acidosis (pH 7.00) | Diffuse bilateral granular opacities (CXR); severe PPHN (echocardiogram) | None | Yes/Yes/22 days | Favorable |
| 10 | Pawar [11] | 1st day/F/4000 g/38 w | RT-PCR NA/IgG pos on day 1/IgM neg | YES—maternal RT-PCR positive 3 weeks before delivery | Yes | Hypotension | CRP 1.4, PCT 1.3, ferritin 1500, D-dimer 5088 | LV dysfunction (echocardiogram) | IVIG, steroids, inotropes (not specified) | Yes/No/13 days | Favorable |
| 11 | Pawar [11] | 1st day/M/2020 g/35 w | RT-PCR NA/IgG pos on day 2/IgM neg | YES—asymptomatic, COVID-19 contact 8 weeks before delivery | No | Shock | NT-proBNP >30,000, ferritin 393, D-dimer 5100 | Bilateral effusions (CXR); LV dysfunction (echocardiogram) | IVIG, steroids, LMWH | Yes/No/14 days | Favorable |
| 12 | Pawar [11] | 4 days/F/2000 g/33 w | RT-PCR NA/IgG pos on day 6/IgM neg | YES—asymptomatic, COVID-19 contact 6 weeks before delivery, with positive IgG | No | Severe bradycardia, prolonged QTc and 2:1 AVB; respiratory distress requiring surfactant and MV | ferritin 407, D-dimer 3020 | NA | IVIG, steroids | Yes/Yes/16 days | Favorable |
| 13 | Pawar [11] | 1st day/M/2000 g/36 w | RT-PCR NA/IgG pos on day 1/IgM neg | YES—asymptomatic, COVID-19 contact 6 weeks before delivery | No | Dilated RA/RV, pericardial effusion, RV dysfunction; shock; respiratory distress | CRP 1.2, NT-proBNP >25,000, D-dimer 6848 | Pleural effusions (CXR); dilated hypertrophied RV with dysfunction, moderate TR, large thrombus at LPA origin on day 3 | IVIG, steroids, inotropes (not specified), alteplase, LMWH | Yes/Yes/19 days | Favorable |
| 14 | Pawar [11] | 3 days/M/3500 g/38 w | RT-PCR NA/IgG pos on day 5/IgM neg | YES—Febrile illness at 7 months of gestation | No | Hypotension and intermittent bradycardia; respiratory distress requiring MV; feeding intolerance; lethargy | Leukocytosis (18,600), CRP 6.0, PCT 2.1, ferritin 878, D-dimer 6483 | NA | IVIG, steroids, inotropes (not specified) | Yes/Yes/13 days | Favorable |
| 15 | Pawar [11] | 2 days/M/2300 g/34 w | RT-PCR NA/IgG pos on day 12/IgM neg | YES—Febrile illness 2 weeks before delivery | No | Hypotension and intermittent bradycardia; respiratory distress requiring CPAP; rash, pedal edema, oral and skin lesions, skin peeling; feeding intolerance, brown gastric aspirates on day 4, treated like NEC, bleeding; decreased activity on day 2 | Thrombocytopenia (39 × 109/L), CRP 2.4, D-dimer 4200 | NA | IVIG, steroids, inotropes (not specified), LMWH | Yes/No/38 days | Favorable |
| 16 | Pawar [11] | 3 days/F/1400 g/34 w | RT-PCR NA/IgG pos on day 1/IgM neg | YES—Asymptomatic, positive RT-PCR at 5th month of gestation | No | Supraventricular tachycardia from day 8; brown gastric aspirates from day 3, frank melena from day 6 | CRP 5.0, D-dimer 5100 | Bilateral pleural effusions (CXR and echocardiogram) | IVIG, steroids, beta-blockers, LMWH | Yes/No/20 days | Favorable |
| 17 | Pawar [11] | 2 days/M/1900 g/32 w | RT-PCR NA/IgG pos on day 1/IgM neg | YES—Asymptomatic, positive RT-PCR at 3rd month of gestation | No | Bradycardia with prolonged QTc and 2:1 AVB on day 2; respiratory distress requiring MV | CRP 4.3, D-dimer 6600, IL-6 116 | NA | IVIG, steroids, inotropes (not specified), LMWH | Yes/Yes/23 days | Favorable |
| 18 | Pawar [11] | 2 days/F/1900 g/33 w | RT-PCR NA/IgG pos on day 4/IgM neg | YES—Asymptomatic, COVID-19 contact 8 weeks before delivery | No | Bradycardia with prolonged QTc and 2:1 AVB on day 2 | CRP 3.5, D-dimer 10,000 | NA | IVIG, steroids, LMWH | Yes/No/18 days | Favorable |
| 19 | Pawar [11] | 2 days/M/1600 g/33 w | RT-PCR NA/IgG pos on day 5/IgM neg | YES—Asymptomatic, COVID-19 contact 8 weeks before delivery | No | Bradycardia with prolonged QTc and 2:1 AVB on day 4 | D-dimer 10,000 | NA | IVIG, steroids, LMWH | Yes/No/18 days | Favorable |
| 20 | Pawar [11] | 4 days/F/2050 g/34 w | RT-PCR NA/IgG pos on day 4/IgM neg | YES—Febrile illness 3 weeks before delivery, with IgG level below cut-off | No | Bradycardia with prolonged QTc and 2:1 AVB on day 4 | PCT 1.8, NT-proBNP >25,000, D-dimer 4840 | NA | IVIG, steroids, inotropes (not specified), LMWH | Yes/No/11 days | Favorable |
| 21 | Pawar [11] | 4 days/M/2100 g/34 w | RT-PCR NA/IgG pos on day 4/IgM neg | YES—Febrile illness 3 weeks before delivery, with IgG level below cut-off | No | Bradycardia with prolonged QTc and 2:1 AVB on day 4 | PCT 1.4, D-dimer 5932 | NA | IVIG, steroids, inotropes (not specified), LMWH | Yes/No/11 days | Favorable |
| 22 | Pawar [11] | 3 days/F/1000 g/27 w | RT-PCR NA/IgG pos on day 4/IgM neg | YES—Asymptomatic, COVID-19 contact 8 weeks before delivery | No | Bradycardia with prolonged QTc and 2:1 AVB on day 4 | PCT 51, NT-proBNP 25,000, D-dimer 10,000 | NA | IVIG, steroids, LMWH | Yes/Yes/death on day 11 due to NEC | Death on day 11 (NEC) |
| 23 | Pawar [11] | 2 days/M/2400 g/36 w | RT-PCR NA/IgG pos on day 6/IgM neg | YES—Asymptomatic, COVID-19 contact 10 weeks before delivery, with positive IgG | No | Cardiogenic shock on day 5; echo-dilated coronaries severe TR, mild MR, ASD, PDA, Severe pulmonary hypertension; refusing feed on day 2 | CRP 1.1, D-dimer 4700 | Cardiomegaly (CXR); dilated coronaries, severe TR, mild MR, ASD, PDA, PPHN (echocardiogram) | IVIG, steroids, inotropes (not specified), aspirin, LMWH | Yes/Yes/14 days | Favorable |
| 24 | Pawar [11] | 4 days/M/2000 g/36 w | RT-PCR NA/IgG pos on day 4/IgM neg | YES—Asymptomatic, COVID-19 contact 4 weeks before delivery | No | Shock, bradycardia, mild LV dysfunction; acute renal failure, hyperkalemia; seizures | CRP 1.8, Cr 1.9, K+ 6.9, NT-proBNP 14,500, D-dimer 4700 | Small ASD, dilated all four chambers, mild LV dysfunction (echocardiogram) | IVIG, steroids, inotropes (not specified), peritoneal dialysis | Yes/Yes/death on day 8 due to MIS-C | Death on day 8 (multi-organ dysfunction) |
| 25 | Pawar [11] | 1st day/F/2000 g/36 w | RT-PCR NA/IgG pos on day 6/IgM neg | YES—Asymptomatic, COVID-19 contact 4 weeks before delivery, with positive IgG | Yes on day 1 | Tachypnea, desaturation; feeding intolerance, vomiting | CRP 6.2, PCT 2.4, NT-proBNP 7361, D-dimer 9734 | NA | IVIG, steroids | Yes/No/10 days | Favorable |
| 26 | Pawar [11] | 2 days/F/1500 g/32 w | RT-PCR NA/IgG neg/IgM neg | YES—Asymptomatic, COVID-19 contact 10 weeks before delivery | No | Bradycardia with prolonged QTc and 2:1 AVB on day 3; respiratory distress | CRP 1.8, D-dimer 12,000 | NA | IVIG, steroids, inotropes (not specified) | Yes/No/13 days | Favorable |
| 27 | Pawar [11] | 2 days/F/1500 g/32 w | RT-PCR NA/IgG below cut-off level/IgM negative | YES—Febrile illness 8 weeks before delivery | No | Bradycardia with prolonged QTc and 2:1 AVB on day 3; respiratory distress | CRP 2.5, NT-proBNP 23,700, D-dimer 10,000 | NA | IVIG, steroids | Yes/No/14 days | Favorable |
| 28 | Pawar [11] | 1st day/M/1900 g/34 w | IgG below cut-off level/IgM negative | YES—Febrile illness 6 weeks before delivery; IgG below cut-off levels, negative IgM | No | Dilated coronaries; not cried after birth; tachypnea, crepitations; pitting edema over chest wall; hepatomegaly | Thrombocytopenia (93 × 109/L), NT-proBNP >25,000, D-dimer 2820 | Pleural effusion (CXR); pericardial effusion, dilated coronaries, large PDA, mild TR, normal function on inotropes (echocardiogram); ascites and hepatomegaly (abdomen US) | IVIG, steroids, inotropes (not specified), aspirin, LMWH | Yes/Yes/NA | Favorable |
| 29 | Pawar [11] | 1st day/F/2700 g/38 w | RT-PCR NA/IgG pos on day 2/IgM neg | YES—Febrile illness 6 weeks before delivery; positive IgG | No | Poor peripheral pulsation and hypotension; not cried after birth; respiratory distress requiring surfactant; mottling | CRP 5.3, NT-proBNP 17,018, D-dimer 3942 | Intracardiac thrombus in RA on day 4, normal LV function (echocardiogram) | IVIG, steroids, inotropes (not specified), LMWH | Yes/Yes/NA | Favorable |
| 30 | Schoenmakers [38] | At birth/F/1800 g/31 w | RT-PCR neg/Serology neg | YES—maternal SARS-CoV-2 infection during the third trimester associated with a placental inflammatory reaction and subsequent placental dysfunction | No | PPHN; hypoxic respiratory failure managed with surfactant, HFOV and inhaled nitric oxide; elevated creatinine; intraventricular hemorrhage | Leukopenia, thrombocytopenia, elevated liver function tests, elevated Cr, Tn and NT-proBNP, ferritin 14,272, elevated D-dimer | Bilateral opacities (CXR), significantly enlarged LMCA, flattened IVS, mild-to-moderate TR, small PDA with right-to-left shunt (echocardiogram) | IVIG, steroids, inotropes (not specified), aspirin | Yes/Yes/NA | Favorable |
| 31 | Shaiba [39] | At birth/F/3004 g/36 w | RT-PCR neg/IgG pos/IgM not tested | YES—The mother tested positive for the SARS-CoV-2 virus in the second trimester, and then again positive 19 days prior to delivery | No | Poor systolic function and hypotension; respiratory distress requiring MV and inhaled nitric oxide; elevated creatinine | CRP 15, PCT 73 (day 1) and 1.22 (day 4), ALT 119 and AST 71, GGT 378, Cr 1, metabolic acidosis, Tn 130, NT-proBNP 3433, ferritin 384, INR 2.59 | Moderately dilated LV with poor systolic function, echogenic papillary muscles (could be secondary to ischemia vs. acidosis), wide PDA with a bidirectional shunt and myocarditis (echocardiogram) | IVIG, steroids, plasma transfusion, PGE1, inotropes (dobutamine) | Yes/Yes/12 days | Favorable |
| 32 | Shaiba [39] | At birth/F/1700 g/32 w | RT-PCR pos/Serology neg | YES—Ten hours after delivery the mother’s swab result turned out to be positive for SARS-CoV-2 | No | Myocarditis, grunting and tachypnea, requiring CPAP; elevated creatinine | CRP 2.02, GGT 141, Tn 51.9, NT-proBNP 5610, ferritin 567, INR 1.06, D-dimer 1060 | Bilateral ground glass appearance with bilateral haziness and good lung volume (CXR); myocarditis (echocardiogram) | IVIG, steroids, | Yes/Yes/30 days | Favorable |
| 33 | Vivanti [5] | 3 days/M/2540 g/35 w | RT-PCR pos/Serology NA | YES—Severe cough since 2 days before hospitalization; positive RT-PCR in blood, amniotic fluid, nasopharyngeal and vaginal swabs | No | Respiratory distress requiring mechanical ventilation; poor feeding on day 3; irritability, axial hypertonia and opisthotonos on day 3 | GGT 290, Tn 43 | Brain MRI on day 11 showed bilateral gliosis on the deep white periventricular and subcortical matter, with slightly left predominance | None | Yes/Yes/18 days | Favorable |
| Subject Number | First Author | Age/Sex/Comorbidities | RT-PCR and Serology for SARS-CoV-2 | Parental SARS-CoV-2 Exposure | Fever | Organ Involvement | Laboratory Work-Up | Imaging | Treatment | ICU Admission/Need for MV/Length of Hospital Stay | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Acharyya [13] | 4 months/M/NA | RT-PCR pos/NA | YES—his mother was also subsequently found positive for SARS-CoV-2. | Yes | Diffuse ectasia of coronary arteries; Erythematous macular rash over the trunk, palm and sole on day 2; Red lips, congested throat and small cervical lymphadenopathy; Irritability | CRP 11.56, Albumin 3, Anemia | Perivascular brightness and diffuse ectasia of coronary arteries (echocardiogram) | IVIG, aspirin | No/No/NA | Favorable |
| 2 | Alharbi [47] | 1 month/F/No | RT-PCR pos/NA | NA | No | Hypotension, increase in troponin; respiratory distress requiring MV for 12 days | Tn 2410, NT-proBNP 1127, ferritin 6130, IL-6 9.1 | Ejection fraction 60%, normal coronary arteries (echocardiogram) | IVIG, Anakinra, inotropes (not specified) | Yes/Yes/13 days | Death |
| 3 | Alharbi [47] | 3 months/M/No | RT-PCR pos/NA | NA | No | Hypotension, increase in troponin; respiratory distress requiring MV for 15 days | Tn 1294, NT-proBNP 2241, ferritin 813, IL-6 9.3 | Ejection fraction 80,5%, normal coronary arteries (echocardiogram) | IVIG, Anakinra | Yes/Yes/73 days | Favorable |
| 4 | Cui [16] | 55 days/F/No | RT-PCR pos/IgM pos | YES—a week earlier (parents) | No | Tachycardia; productive cough and hypoxic respiratory failure requiring oxygen supplementation through a nasal cannula (day 7 of illness) | CRP 5.6, Tn 25,000, D-dimer 54,000 | Ground-glass opacity (CXR); Patchy shadows and ground-glass opacity in the right lung (day 4 of illness), pneumonia (day 9) at chest CT | Inhaled interferon α-1b, reduced glutathione, urso-deoxycholic acid, and traditional Chinese medicine lotus qingwen | No/No/20 days | Favorable |
| 5 | Del Barba [17] | 38 days/M/No | RT-PCR pos/NA | YES—Both parents diagnosed with COVID-19 | Yes | Increase in troponin; rhinitis; modest hypo-reactivity | Thrombocytosis (525 × 109/L), PCT 3.28, Tn 82, NT-proBNP 208, D-dimer 133,000, fibrinogen 128 | Mild thickening of broncho-vascular markings, but no pulmonary parenchymal opacities (CXR); minimal pericardial effusion (cardiac MRI) | None | No/No/14 days | Favorable |
| 6 | Diggikar [18] | 7 days/NA/No | RT-PCR pos/IgG neg/IgM neg | YES—the mother tested positive for SARS-CoV-2 infection one day before the presentation | Yes | Small coronary artery aneurysm; apnoea and respiratory distress requiring MV; reduced tone, sluggish reflexes and seizures | CRP 60, D-dimer 5000 | Small coronary artery aneurysm (echocardiogram); diffuse changes involving the periventricular white matter, external capsule and internal capsule, while peripheral bilateral thalami show T2 fluid-attenuated inversion recovery hyperintensity with diffusion restriction (brain MRI) | Steroids, remdesivir, enoxaparin, levetiracetam and phenobarbitone | Yes/Yes/NA | Favorable |
| 7 | Dugue [21] | 6 weeks/M/No | RT-PCR positive for SARS-CoV-2 and Rhinovirus/NA | NA | Yes | Cough; mottled appearance; brief episodes of upward gaze associated with bilateral leg stiffening and altered responsiveness | Leukopenia (5070) | Excess of temporal sharp transients for age and intermittent vertex delta slowing with normal sleep-wake cycling (long-term EEG) | None | No/No/1 day | Favorable |
| 8 | Esteve-Sole [52] | 3 months/M/NA | RT-PCR neg/serology neg | YES | Yes | Peripheral extremity changes; gastrointestinal symptoms (not specified); irritability | Leukopenia (4000), CRP 12.8, Albumin 2.3, NT-proBNP 3628, D-dimer 2000 | Coronary abnormalities (not specified at echocardiogram) | IVIG, steroids, aspirin, clopidogrel | No/No/NA | Favorable |
| 9 | Falah [53] | 4 months/M/No | RT-PCR pos/NA | NA | Yes | Isolated coronary artery disease; Rash, conjunctival injection, lips and oral cavity changes; Irritability, neurological symptoms (not specified) | Leukocytosis, CRP 11.56, Albumin 3 | Coronary artery dilation (echocardiogram) | IVIG, aspirin | No/No/NA | Favorable |
| 10 | Falah [53] | 6 months/F/No | RT-PCR pos/NA | NA | Yes | Rash, conjunctival injection, lips and oral cavity changes; Not specified GI symptoms, poor feeding; Irritability, neurological symptoms (not specified) | Leukocytosis, CRP 13.3, Albumin 2.8 | Faint opacity in the left mid-lung zone (CXR) | IVIG, aspirin | No/No/NA | Favorable |
| 11 | Frauenfelder [22] | 32 days (corrected age 37 + 3 weeks)/M/Prematurity | RT-PCR pos/NA | YES—recent contact with family members and asymptomatic healthcare workers | No | Need for inotropes, mildly elevated troponin; significant glottic swelling and copious airway secretions; hypoxic respiratory failure requiring HFOV and inhaled nitric oxide | Lymphopenia (1.45 × 109/L), CRP 4.2, Albumin 2, Tn 138, Ferritin 138, D-dimer 1143 | Mild bilateral ground-glass opacities (CXR); Small patent foramen ovale with left-to-right shunt, mild dilation left side structures, and mild MR (echocardiogram) | Steroids, remdesivir, not specified anticoagulation (not specified, because of a line-associated femoral arterial thrombus), inotropes (noradrenaline and adrenaline) | Yes/Yes/18 days | Favorable |
| 12 | García-Howard [23] | 3 months/F/No | RT-PCR pos/NA | YES | Yes | Rhinorrhea and cough; Diarrhea; Mild hypotonia, staring gaze, clonic movements of the face and right extremities, and repeating sucking movements of the mouth, lasting <5 min | CRP 0.67, Ferritin 385, Increased D-dimer, negative CSF culture | Normal interictal EEG, Normal cerebral MRI | Levetiracetam, Hydroxychloroquine | No/No/9 days | Favorable |
| 13 | Giacomet [24] | 2 months/F/No | RT-PCR pos/NA | YES— Father and older brother tested positive | Yes | Intermittent tachycardia; mottled skin; non-bloody diarrhea and vomiting | Anemia (Hb 7.9), Tn 103, NT-proBNP 12,507, D-dimer 1918, IL-6 236 | Hypokinesia of the inferior left ventricular wall and the inferior interventricular septum, with a mild decrease in the left ventricular ejection fraction | IVIG, Packed red blood cells transfusion | Yes/No/NA | NA |
| 14 | Jones [27] | 6 months/F/No | RT-PCR pos/NA | YES—her 9-year-old sibling had upper respiratory symptoms 3 weeks before | Yes | Sinus tachycardia during fever; mild congestion and subcostal retractions; Prominent tongue papilla; a blanching, polymorphous, maculopapular rash, limbic sparing conjunctivitis, and dry cracked lips; Irritability | Left-shifted white blood cell count with bandemia, normocytic anemia, CRP 13.3, Albumin 2.8 | Faint opacity in the left midlung zone (CXR) | IVIG, aspirin | No/No/NA | Favorable |
| 15 | Lad [28] | 4 months/F/NA | RT-PCR neg/IgG pos | YES—Father with COVID-19 a month before | Yes | Compensated shock; Vomiting and fresh blood in stool; Lethargy | Neutrophilic leukocytosis; Anemia (Hb 8) | Both coronaries dilated with high z-score > 2.5; Abdominal CT showed dilated jejunum and proximal ileum suggestive of obstruction. | IVIG, steroids, exploratory laparotomy (showing extensively congested ileum and tiny fibrous band about 2.5 cm crossing from antimesenteric border to mesentery in proximal ileum, without any obvious volvulus), packed red blood cells transfusion | No/No/NA | Favorable |
| 16 | Luna Santiago [31] | 2 months/M/Griscelli syndrome type 2 | RT-PCR pos/NA | NA | Yes | Shock; respiratory distress; Hepatosplenomegaly | Pancytopenia (in the context of a familial hemophagocytic lympho-histiocytosis triggered by SARS-CoV-2 at bone marrow aspiration), with increased CRP, D-dimer, triglycerides and IL-6 | NA | Steroids, anticoagulation therapy (not specified); inotropes (not specified), multiple transfusions, cyclosporine, cytarabine and inhibitor of JAK signaling | Yes/Yes/NA | Death |
| 17 | Malle [41] | 6 months/F/Down syndrome and CHD | RT-PCR pos/serology neg | YES—her father had contracted COVID-19 | Yes | Heart dysfunction and distributive shock; cough; Maculopapular erythematous rash with peripheral desquamation, edematous hands; Vomiting; Fatigue | Lymphopenia and neutrophilic leukocytosis, increased CRP and PCT, Hypoalbuminemia, Increased Tn, ferritin, D-dimer, fibrinogen and IL-6; Increased STAT3 phosphorylation and increased FcɣRI and ICAM1 on neutrophils and monocytes | Myocarditis and coronary dilatation (echocardiogram) | IVIG, steroids, lopinavir/ritonavir and hydroxychloroquine | Yes/No/4 months | Favorable |
| 18 | Mariani [32] | 5 months/F/NA | RT-PCR pos/IgG pos | YES—five weeks earlier, her father had tested positive | Yes | Intermittent tachycardia | Thrombocytopenia (36 × 109/L) in the context of a Severe transient pancytopenia with dys-erythropoiesis and dys-megakaryopoiesis; hypoalbuminemia, NT-proBNP 3617, D-dimer 8060 | Mild to moderate TR with small pericardial effusion (echocardiogram) | Steroids | No/No/NA | Favorable |
| 19 | Marino [42] | 5 months/F/No | RT-PCR neg/NA | No | Yes | Isolated coronary artery disease; Erythematous rash at the trunk; Sterile pyuria; Diarrhea; Irritability | CRP 6.4 and PCT 0.96, Tn 13, NT-proBNP 1019, Ferritin 259, D-dimer 1053 | Dilatation of both right coronary artery (RCA) and left main coronary artery (LMCA); dim opacity of the left lung base (CXR); gallbladder hydrops (abdominal US); | IVIG, steroids, aspirin | No/No/NA | Favorable |
| 20 | Orlanski-Meyer [34] | 8 weeks/F/No | RT-PCR neg/IgG pos | YES—both parents tested positive at 2 weeks of age. The positive serology was unlikely to represent the passive transfer of maternal antibodies. | No | Tachycardia; Cracked lips; Profuse watery diarrhea, transient bloody stool, vomiting | Thrombocytosis (958 × 109/L), ALT 173 and AST 140, GGT 274, Albumin 1.4, NT-proBNP 1011, Ferritin 385, Fibrinogen 393, IL-6 37.5 | Mild-moderate MR with normal coronary arteries and systolic function (echocardiogram); nonspecific intestinal wall changes and mucosal flattening and splenomegaly (abdominal US); patchy erythema and scattered pinpoint (colonoscopy) | IVIG, steroids, anakinra | No/No/NA | Favorable |
| 21 | Rakha [43] | 5 months/NA/No | NA/IgG and IgM pos | NA | Yes | Isolated coronary artery disease; not specified respiratory and GI symptoms | Leukocytosis, increased CRP and ferritin | Diffuse ectasia of RCA and LCMA; initial fractional shortening 35% (echocardiogram) | IVIG, aspirin | NA/NA/from 6 to 14 days | Favorable |
| 22 | Rakha [43] | 5 months/NA/No | NA/IgG and IgM pos | NA | Yes | Isolated coronary artery disease; not specified respiratory and GI symptoms | Leukocytosis, increased CRP and ferritin | Medium aneurysm LMCA, ectasia of LAD and diffuse ectasia of RCA; initial fractional shortening 29% (echocardiogram) | IVIG, aspirin | NA/NA/from 6 to 14 days | Favorable |
| 23 | Rakha [43] | 3 months/NA/No | NA/IgG and IgM pos | NA | Yes | Isolated coronary artery disease; not specified respiratory and GI symptoms | Leukocytosis, increased CRP and ferritin | Multiple medium and giant aneurysms in left circumflex, and LAD; initial fractional shortening 28% (echocardiogram) | IVIG, aspirin | NA/NA/2 days | Death on second day of admission |
| 24 | Rakha [43] | 6 months/NA/No | NA/IgG and IgM pos | NA | Yes | Coronary artery disease with myopericarditis; not specified respiratory and GI symptoms | Leukocytosis, increased CRP and ferritin | Ectasia of RCA, LCA, and LAD with decreased contractility; initial fractional shortening 22% (vomiting) | IVIG, aspirin | NA/NA/from 6 to 14 days | Favorable |
| 25 | Rakha [43] | 36 days/NA/No | NA/IgG and IgM pos | NA | Yes | Supraventricular tachycardia; not specified respiratory and GI symptoms | Leukocytosis, increased CRP and ferritin | Initial fractional shortening 28% (echocardiogram) | None | NA/NA/from 6 to 14 days | Favorable |
| 26 | Raut [35] | 5 months/M/No | RT-PCR pos/NA | NA | Yes | Isolated coronary artery disease; Skin rash and bilateral non-purulent conjunctivitis; Irritability | CRP 21.5, PCT 8.6, Albumin 2.4, NT-proBNP 2025, Ferritin 975 | Normal left ventricular function, with coronary dilatation in LMCA and LAD (echocardiogram) | IVIG, aspirin | No/No/22 days | Favorable |
| 27 | Richardson [40] | 5 months/F/No | RT-PCR neg/IgG pos a week after hospitalization | NA | Yes | Isolated coronary artery disease; respiratory distress requiring high-flow oxygen on day 5 of illness; Erythematous rash on trunk and extremities (at presentation) with peeling skin on her hands and feet and cracked lips (day 10) | CRP 50, Albumin 2.2, Ferritin 937, D-dimer 6692, Fibrinogen 4700 | Coronary artery aneurysm (echocardiogram) | IVIG, steroids, Anakinra then Infliximab, aspirin | Yes/No/NA | Favorable |
| 28 | Rodriguez-Gonzalez [36] | 6 months/M/short bowel syndrome (secondary to multiple intestinal resections during the neonatal period), antithrombotic prophylaxis due to previous local thrombotic obstructions of the central line | RT-PCR neg/IgG pos on day 21 of illness | NA | Yes | Cardiogenic shock secondary to severe pulmonary hypertension and new onset right ventricular failure; respiratory distress requiring MV | Thrombocytopenia (98 × 109/L), PCT 3.46, Tn 90, NT-proBNP 26,000, Ferritin 7634, Fibrinogen 179, IL-6 198 | Massive pulmonary thromboembolism, with a pattern of ground glass and numerous consolidations of predominance in the posterior-basal segments of both lungs (chest CT); Severely dilated right chambers, severe right ventricular systolic dysfunction, and supra-systemic pulmonary hypertension (echocardiogram); irregular pleural line, B-lines, some coalescent, with bilateral patchy distribution, and small peripheral consolidations, which were larger in posterior-basal areas (lung US) | Steroids, Tocilizumab, previous antithrombotic prophylaxis, hydroxychloroquine and inotropic support (milrinone and norepinephrine) | Yes/Yes/21 days | Favorable |
| 29 | Saha [37] | 25 days/F/Previous hospitalization due to bacterial late-onset sepsis | RT-PCR pos/NA | NO—No family members had signs and symptoms suggestive of SARS-CoV-2. She was in 2 different hospitals previously and may have contracted the virus there. | Yes | Cardiogenic shock; respiratory distress requiring MV; disseminated maculopapular rash; acute kidney injury post-resuscitation; hepatosplenomegaly and greenish watery stool; short-duration seizures | Thrombocytopenia (100 × 109/L), PCR 2.9, Metabolic acidosis, increased NT-proBNP, Ferritin 16,000, D-dimer 16,500 | Atelectasis of both lower lobes of lung (chest CT); Significant systolic dysfunction, with ejection fraction of 40% and mild pericardial infusion (echocardiogram) | IVIG, steroids, enoxaparin, inotropes (adrenaline and milrinone), phenobarbitone, furosemide, packed red blood cells transfusion | Yes/Yes/50 days | Favorable |
| 30 | Shaiba [44] | 30 days/F/NA | RT-PCR pos/NA | NA | Yes | Increased cardiac enzymes; respiratory distress requiring MV; impaired renal function; not specified GI symptoms | Thrombocytopenia (43 × 109/L), CRP 1.1 and PCT 1.7, Hyponatremia (123), Cr 2.44, Tn 684, NT-proBNP 971, Ferritin 2316, D-dimer 5500, Fibrinogen 225, | NA | IVIG, steroids, anakinra, heparin, hydralazine, amlodipine | Yes/Yes/15 days | Death |
| 31 | Shaiba [44] | 90 days/M/NA | RT-PCR pos/NA | NA | Yes | Increased cardiac enzymes; respiratory distress requiring MV | CRP 5.6, ALT 1070 and 1178, Cr 0.89, Tn 108, NT-proBNP 1370, Ferritin 813, INR 1.49, D-dimer 1320 | NA | IVIG, steroids, anakinra, aspirin, enoxaparin, hydralazine, amlodipine, sildenafil | Yes/Yes/75 days | Favorable |
| 32 | Villacis-Nunez [45] | 4 months/M/Prematurity, twin | RT-PCR pos/IgG pos on day 19 of illness | NA | Yes | Isolated coronary artery disease; respiratory distress requiring non-invasive positive-pressure ventilation; rash, hand and foot swelling, conjunctivitis; diarrhea | Increased CRP (>3) | Giant LAD and RCA aneurysms identified on day 21 of illness (echocardiogram); coronary involvement with possible LAD artery mural thrombus (cardiac CT) | IVIG, steroids, infliximab, remdesivir, aspirin, enoxaparin, clopidogrel | Yes/No/ 26 days | Favorable |
| First Author | Total Number of Children with MIS-C | Number of Infants under Six Months of Age | Available Description |
|---|---|---|---|
| Abdel-Haq [46] | 13 | 1 | A 3-months-old girl with a positive RT-PCR for SARS-CoV-2 and dilated coronary arteries, successfully treated with IVIG and infliximab |
| Alharbi [47] | 5 | 2 | Full description in Table 3 (Case 2 and Case 3) |
| Antúnez-Montes [48] | 95 | 3 | 3 infants under the age of a month, but their specific clinical characteristics were not described |
| Caro-Domínguez [49] | 37 | 1 | A 6-months-old boy with cardiac failure and positive RT-PCR for SARS-CoV-2 |
| Chandran [50] | 17 | 3 | Two infants survived (a 1-month-old infant who had prematurity as comorbidity and a 6-months-old infant who had previously undergone Kasai procedure at 2 months of age for biliary atresia). A 1-month-old infant with refractory thrombocytopenia and multiorgan involvement, treated with IVIG, methylprednisolone and cyclosporine, died. |
| Dufort [51] | 191 | 1 | A neonate with MIS-N, born to a positive mother (asymptomatic at delivery) who presented with fever and left breast cellulitis between 14 and 28 days of age. Laboratory work-up showed increasing troponin levels; echocardiogram showed good ventricular function and unremarkable coronary arteries. Two molecular tests for SARS-CoV-2 were negative. The discharge diagnoses were cellulitis, myocarditis, and shock. |
| Godfred-Cato [54] | 85 | 1 | The specific clinical characteristics of infants < 6 months of age are not described. |
| Grewal [55] | 92 | 9 | Nine infants under the age of 6 months, none with acute kidney injury. |
| Güllü [56] | 320 | 3 | A 1-month-old girl, followed up with aortic coarctation, resulted to be positive for SARS-CoV-2 and had fever and poor feeding. A 3-months-old boy, followed up with ventricular septal defect and pulmonary hypertension, had fever, diarrhoea (leading to a severe dehydration and lack of urine). A 6-days-old boy, who applied with fever, vomiting, decreased feeding and respiratory distress for 2 days. It was learned that his aunt and grandfather had been diagnosed with COVID-19 and they had loved and cared for the baby. |
| Mehra [57] | 120 | 1 | Among four deaths, one was a 3-month-old infant with acute COVID-19 related severe acute respiratory distress syndrome and shock |
| Niño-Taravilla [58] | 26 | 2 | Two neonates with MIS-C (the specific clinical characteristics are not described) |
| Shaiba LA [44] | 36 | 2 | Full description in Table 3 (Case 30 and Case 31) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Rose, D.U.; Pugnaloni, F.; Calì, M.; Ronci, S.; Caoci, S.; Maddaloni, C.; Martini, L.; Santisi, A.; Dotta, A.; Auriti, C. Multisystem Inflammatory Syndrome in Neonates Born to Mothers with SARS-CoV-2 Infection (MIS-N) and in Neonates and Infants Younger Than 6 Months with Acquired COVID-19 (MIS-C): A Systematic Review. Viruses 2022, 14, 750. https://doi.org/10.3390/v14040750
De Rose DU, Pugnaloni F, Calì M, Ronci S, Caoci S, Maddaloni C, Martini L, Santisi A, Dotta A, Auriti C. Multisystem Inflammatory Syndrome in Neonates Born to Mothers with SARS-CoV-2 Infection (MIS-N) and in Neonates and Infants Younger Than 6 Months with Acquired COVID-19 (MIS-C): A Systematic Review. Viruses. 2022; 14(4):750. https://doi.org/10.3390/v14040750
Chicago/Turabian StyleDe Rose, Domenico Umberto, Flaminia Pugnaloni, Monica Calì, Sara Ronci, Stefano Caoci, Chiara Maddaloni, Ludovica Martini, Alessandra Santisi, Andrea Dotta, and Cinzia Auriti. 2022. "Multisystem Inflammatory Syndrome in Neonates Born to Mothers with SARS-CoV-2 Infection (MIS-N) and in Neonates and Infants Younger Than 6 Months with Acquired COVID-19 (MIS-C): A Systematic Review" Viruses 14, no. 4: 750. https://doi.org/10.3390/v14040750
APA StyleDe Rose, D. U., Pugnaloni, F., Calì, M., Ronci, S., Caoci, S., Maddaloni, C., Martini, L., Santisi, A., Dotta, A., & Auriti, C. (2022). Multisystem Inflammatory Syndrome in Neonates Born to Mothers with SARS-CoV-2 Infection (MIS-N) and in Neonates and Infants Younger Than 6 Months with Acquired COVID-19 (MIS-C): A Systematic Review. Viruses, 14(4), 750. https://doi.org/10.3390/v14040750