
SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Existing Laboratory Surveillance Network in India
2.2. Selection of Laboratories for the ILI/SARI Surveillance Network
2.3. Tiered Structure of the ILI/SARI Surveillance Laboratory Network
2.4. Diagnostic Multiplex rRTPCR (Real Time Reverse Transcriptase PCR) Kit Used by Laboratories in the Network
2.5. Case Definition for COVID-19/Influenza Co-Infection and Influenza A/B Dual Infection Cases
2.6. Data Entry and Analysis
2.7. Retrieval of Demographic and Clinical Data
2.8. Period of Reporting
3. Results
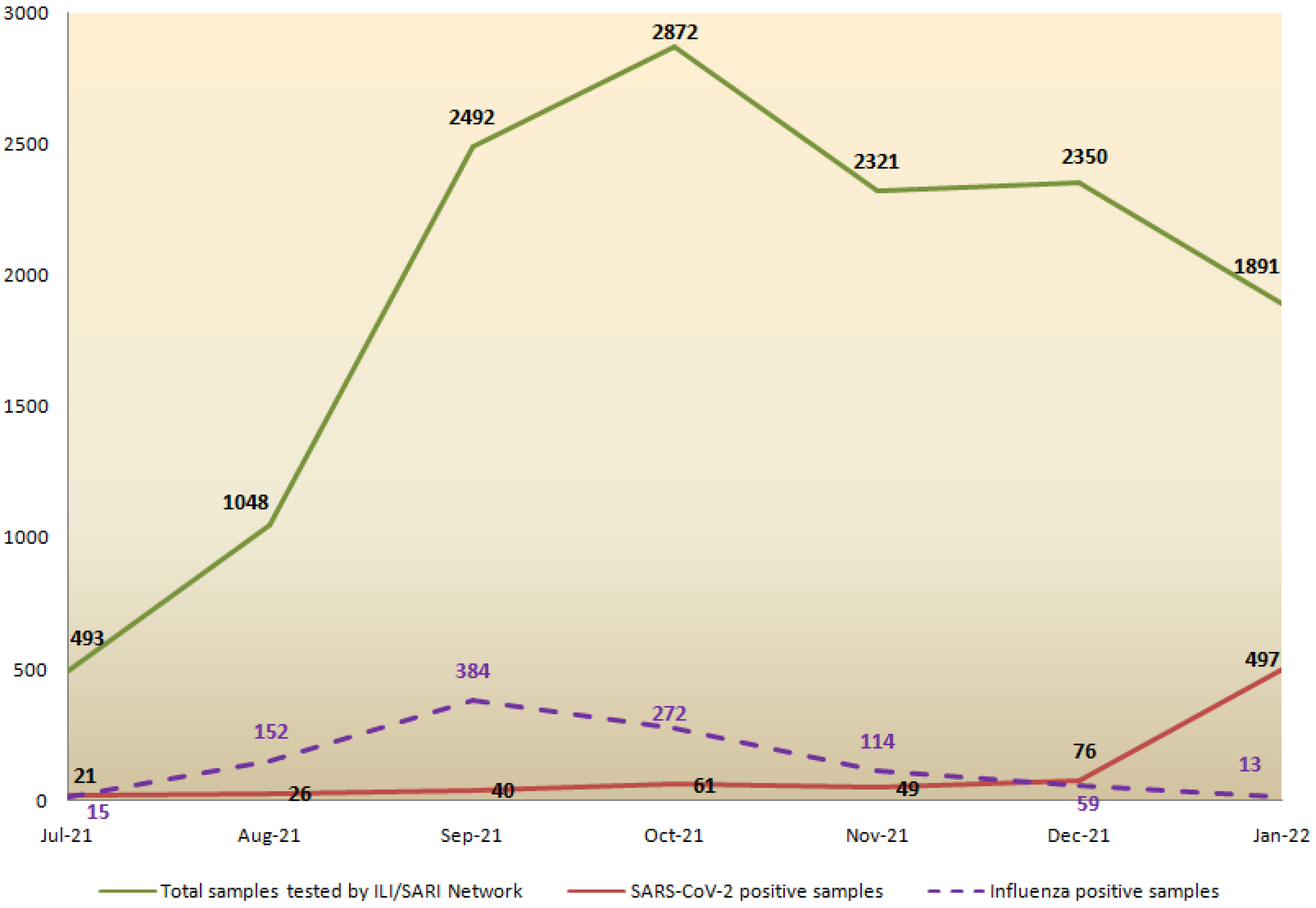
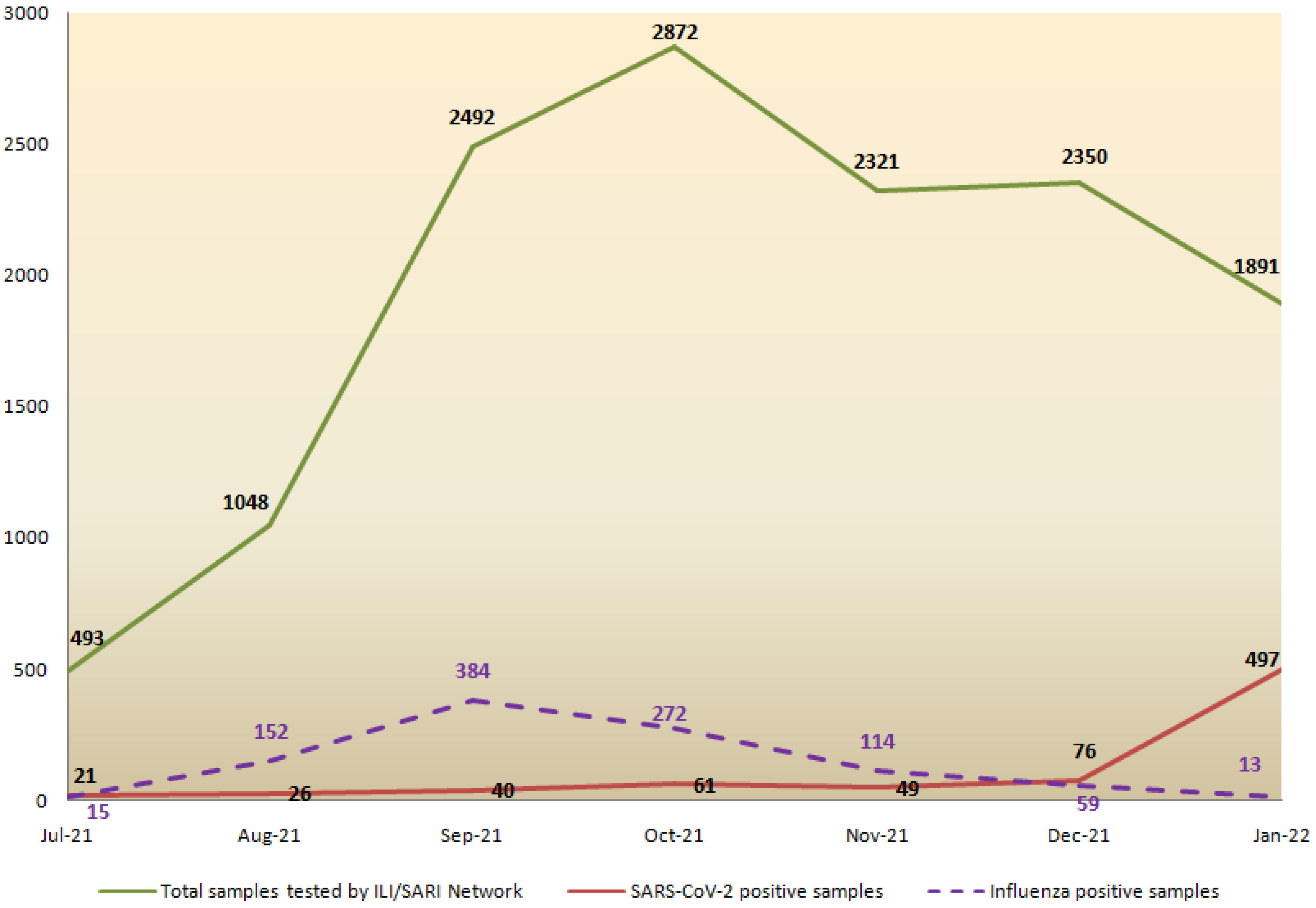
3.1. Samples Tested and Respiratory Pathogens Detected through the ILI/SARI Surveillance Network
3.2. Cases of Co-Infections
- i.
- Infecting virus type: Two cases had infections with SARS-CoV-2 and influenza A H3N2, while three cases were co-infected with SARS-CoV-2 and influenza B Victoria virus.
- ii.
- Demographic details including co-morbidity: Three of the co-infection cases were children with ages ranging from 1–8 years, while there were 2 adults aged 18 and 74 years. The elderly patient was a known case of COPD (Chronic Obstructive Pulmonary Disease) and CKD (Chronic Kidney Disease) and was on dialysis. The other patients did not have any co-morbidity. Two cases each were reported from the western state of Maharashtra and the northeastern state of Assam, whereas the remaining case was from the southern state of Kerala.
- iii.
- Symptoms, severity, and hospitalization: The symptoms reported by these patients were fever, cough, running nose, and shortness of breath. Two patients were managed at home, and three patients had to be hospitalized.
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Wang, Q.; Gao, Y.; Zhang, J.; Cheng, S.; Chen, H.; Zeng, Z.; Wang, Z. The global burden and trends of maternal sepsis and other maternal infections in 204 countries and territories from 1990 to 2019. BMC Infect. Dis. 2021, 21, 100986. [Google Scholar] [CrossRef] [PubMed]
- Caballero, M.T.; Bianchi, A.M.; Nuño, A.; Ferretti, A.J.P.; Polack, L.M.; Remondino, I.; Rodriguez, M.G.; Orizzonte, L.; Vallone, F.; Bergel, E.; et al. Mortality Associated With Acute Respiratory Infections Among Children at Home. J. Infect. Dis. 2019, 219, 358–364. [Google Scholar] [CrossRef]
- Atamna, A.; Babich, T.; Froimovici, D.; Yahav, D.; Sorek, N.; Ben-Zvi, H.; Leibovici, L.; Bishara, J.; Avni, T. Morbidity and mortality of respiratory syncytial virus infection in hospitalized adults: Comparison with seasonal influenza. Int. J. Infect. Dis. 2021, 103, 489–493. [Google Scholar] [CrossRef]
- Chadha, M.S.; Potdar, V.A.; Saha, S.; Koul, P.A.; Broor, S.; Dar, L.; Chawla-Sarkar, M.; Biswas, D.; Gunasekaran, P.; Abraham, A.M.; et al. Dynamics of influenza seasonality at sub-regional levels in India and implications for vaccination timing. PLoS ONE 2015, 10, e0124122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsen, S.J.; Azziz-Baumgartner, E.; Budd, A.P.; Brammer, L.; Sullivan, S.; Pineda, R.F.; Cohen, C.; Fry, A.M. Decreased Influenza Activity During the COVID-19 Pandemic—United States, Australia, Chile, and South Africa, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1305–1309. [Google Scholar] [CrossRef]
- Tang, J.W.; Bialasiewicz, S.; Dwyer, D.E.; Dilcher, M.; Tellier, R.; Taylor, J.; Hua, H.; Jennings, L.; Kok, J.; Levy, A.; et al. Where have all the viruses gone? Disappearance of seasonal respiratory viruses during the COVID-19 pandemic. J. Med. Virol. 2021, 93, 4099–4101. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, B.; Swamy, M.A.; Reddy, P.V.J.; Kumar, N.; Tiwari, J.K. Evaluation of custom multiplex real—Time RT—PCR in comparison to fast—Track diagnostics respiratory 21 pathogens kit for detection of multiple respiratory viruses. Virol. J. 2016, 13, 91. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.; Zhang, T.; Wang, Q.; Xie, Y.; Peng, Z.; Zheng, J.; Qin, Y.; Zhang, M.; Lai, S.; Wang, D.; et al. Impact of COVID-19 outbreaks and interventions on influenza in China and the United States. Nat. Commun. 2021, 12, 121. [Google Scholar] [CrossRef]
- Soo, R.J.J.; Chiew, C.J.; Ma, S.; Pung, R.; Lee, V.; Lee, V.J. Decreased influenza incidence under COVID-19 control measures, Singapore. Emerg. Infect. Dis. 2020, 26, 1933–1935. [Google Scholar] [CrossRef] [PubMed]
- Jones, N. How COVID-19 is changing the cold and flu season. Nature 2020, 588, 388–390. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, Z.; Islam, M.A.; Aleem, M.A.; Mah-E-Muneer, S.; Ahmmed, M.K.; Ghosh, P.K.; Rahman, M.; Rahman, M.Z.; Sumiya, M.K.; Rahman, M.M.; et al. SARS-CoV-2 and influenza virus coinfection among patients with severe acute respiratory infection during the first wave of COVID-19 pandemic in Bangladesh: A hospital-based descriptive study. BMJ Open 2021, 11, e053768. [Google Scholar] [CrossRef]
- Ali, R.; Patel, A.; Chan, K.H.; Veeraballi, S.; Slim, J. A Case Series of SARS-CoV-2 and Influenza Co-infection. Cureus 2021, 13, e17597. [Google Scholar] [CrossRef] [PubMed]
- Ozaras, R.; Cirpin, R.; Duran, A.; Duman, H.; Arslan, O.; Bakcan, Y.; Kaya, M.; Mutlu, H.; Isayeva, L.; Kebanlı, F.; et al. Influenza and COVID-19 coinfection: Report of six cases and review of the literature. J. Med. Virol. 2020, 92, 2657–2665. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Liu, P.; Xiong, G.; Yang, Z.; Wang, M.; Li, Y.; Yu, X.J. Coinfection of SARS-CoV-2 and multiple respiratory pathogens in children. Clin. Chem. Lab. Med. 2020, 58, 1160–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Wang, W.; Le Grange, J.M.; Wang, X.; Du, S.; Li, C.; Wei, J.; Zhang, J.N. Coinfection of SARS-CoV-2 and other respiratory pathogens. Infect. Drug Resist. 2020, 13, 3045–3053. [Google Scholar] [CrossRef] [PubMed]
- Stowe, J.; Tessier, E.; Zhao, H.; Guy, R.; Muller-Pebody, B.; Zambon, M.; Andrews, N.; Ramsay, M.; Lopez Bernal, J. Interactions between SARS-CoV-2 and influenza, and the impact of coinfection on disease severity: A test-negative design. Int. J. Epidemiol. 2021, 50, 1124–1133. [Google Scholar] [CrossRef]
- Alosaimi, B.; Naeem, A.; Hamed, M.E.; Alkadi, H.S.; Alanazi, T.; Al Rehily, S.S.; Almutairi, A.Z.; Zafar, A. Influenza co-infection associated with severity and mortality in COVID-19 patients. Virol. J. 2021, 18, 127. [Google Scholar] [CrossRef]
- Duployez, C.; Le Guern, R.; Tinez, C.; Lejeune, A.L.; Robriquet, L.; Six, S.; Loez, C.; Wallet, F.; Duployez, C.; Le Guern, R.; et al. Panton-valentine leukocidin secreting staphylococcus aureus pneumonia complicating COVID-19. Emerg. Infect. Dis. 2020, 26, 1939–1941. [Google Scholar] [CrossRef]
- Blaize, M.; Mayaux, J.; Nabet, C.; Nabet, C.; Lampros, A.; Marcelin, A.G.; Marcelin, A.G.; Thellier, M.; Thellier, M.; Piarroux, R.; et al. Fatal Invasive Aspergillosis and Coronavirus Disease in an Immunocompetent Patient. Emerg. Infect. Dis. 2020, 26, 1636–1637. [Google Scholar] [CrossRef]
- Vargas Ponce, K.G.; Salas López, A.; Llanos Tejada, F.; Morales Avalos, A. COVID-19 and Influenza: Report of five cases in a peruvian hospital. Rev. Fac. Med. Hum. 2020, 20, 738–742. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Chadha, M.S.; Broor, S.; Gunasekaran, P.; Potdar, V.A.; Krishnan, A.; Chawla-Sarkar, M.; Biswas, D.; Abraham, A.M.; Jalgaonkar, S.V.; Kaur, H.; et al. Multisite virological influenza surveillance in India: 2004–2008. Influenza Other Respir. Viruses 2012, 6, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Potdar, V.; Praharaj, I.; Giri, S.; Sapkal, G.; Yadav, P.; Choudhary, M.; Dar, L.; Sugunan, A.; Kaur, H.; et al. Laboratory preparedness for SARS-CoV-2 testing in India: Harnessing a network of Virus Research & Diagnostic Laboratories. Indian J. Med. Res. 2020, 151, 216–225. [Google Scholar] [CrossRef]
- WHO. Operational Considerations for COVID-19 Surveillance Using GISRS. In WHO—Interim Guidance; WHO: Geneva, Switzerland, 2020; pp. 1–6. [Google Scholar]
- World Health Organization. Maintaining Surveillance of Influenza and Monitoring SARS-CoV-2—Adapting Global Influenza Surveillance and Response System (GISRS) and Sentinel Systems during the COVID-19 Pandemic—Interim Guidance; WHO/2019-nCoV/Adapting_GISRS/2020.1; WHO: Geneva, Switzerland, 2020; p. 53. [Google Scholar]
- Agarwal, A.; Sharma, A.; Agarwal, M.; Jakhar, R. The Clinical Characteristics of Coinfection of COVID19 and Influenza A Viruses—A Case Series. J. Assoc. Physicians India 2021, 69, 33–37. [Google Scholar] [PubMed]
- Sreenath, K.; Batra, P.; Vinayaraj, E.V.; Bhatia, R.; SaiKiran, K.; Singh, V.; Singh, S.; Verma, N.; Singh, U.B.; Mohan, A.; et al. Coinfections with Other Respiratory Pathogens among Patients with COVID-19. Microbiol. Spectr. 2021, 9, e00163-21. [Google Scholar] [CrossRef] [PubMed]
- Influenza-SARS-CoV-2. Available online: https://influenza.icmr.org.in/login/?next=/info/ (accessed on 14 February 2022).
- Dadashi, M.; Khaleghnejad, S.; Abedi Elkhichi, P.; Goudarzi, M.; Goudarzi, H.; Taghavi, A.; Vaezjalali, M.; Hajikhani, B. COVID-19 and Influenza Co-infection: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 681469. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and metaanalysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef]
- Cuadrado-Payán, E.; Montagud-Marrahi, E.; Torres-Elorza, M.; Bodro, M.; Blasco, M.; Poch, E.; Soriano, A.; Piñeiro, G.J. SARS-CoV-2 and influenza virus co-infection. Lancet 2020, 395, e84. [Google Scholar] [CrossRef]
- CDC. Sentinel Surveillance Laboratory Testing and WHO Global Influenza Surveillance and Response System Reporting. COVID-19 Surveillance Webinar; CDC: Singapore, 2020. [Google Scholar]
- World Health Organization. End-to-End Integration of SARS-CoV-2 and Influenza Sentinel Surveillance—Revised Interim Guidance; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Mir, H.; Koul, P.A. Negligible circulation of influenza in COVID times in Northern India. Lung India 2021, 38, 401–402. [Google Scholar] [PubMed]
- Bai, L.; Zhao, Y.; Dong, J.; Liang, S.; Guo, M.; Liu, X.; Wang, X.; Huang, Z.; Sun, X.; Zhang, Z.; et al. Coinfection with influenza A virus enhances SARS-CoV-2 infectivity. Cell Res. 2021, 31, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Watanabe, K.; Sakurai, Y.; Nishi, K.; Yoshikawa, R.; Yasuda, J. Co-infection of SARS-CoV-2 and influenza virus causes more severe and prolonged pneumonia in hamsters. Sci. Rep. 2021, 11, 21259. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus (COVID-19) Cases—Our World in Data. Available online: https://ourworldindata.org/covid-cases (accessed on 14 February 2022).

{kind=link}
| Case No. | Region | Age/Gender | Setting | Signs and Symptoms | ILI/SARI | Pathogens | Managed at Home/Hospital | Duration between Onset of Symptom and Hospital Admission | Duration of Hospital Admission | ICU/HDU/CCU Admission | Need of O2/Ventilator | Chest CT Scan Findings | Final Outcome | Co-Morbidities | Influenza Vaccination History |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Western India | 8Y/M | Community | Fever, dry cough | ILI | H3N2+SARS-CoV-2 | Home | - | - | - | No | NA | Resolved in 2 days | None | Not vaccinated |
| 2 | Western India | 18m/F | Hospital | Fever | SARI | Victoria+SARS-CoV-2 | Hospital | Few hours | 3 days | No | No | NA | Discharged in 3 days | None | Not vaccinated |
| 3 | North-Eastern India | 1Y/M | Hospital | Fever, cough, runny nose, shortness of breath, stridor in calm patient | SARI | Victoria+SARS-CoV-2 | Hospital | Few hours | 12 days | No | Yes (O2) | NA | Discharged after 12 days | None | Not vaccinated |
| 4 | North-Eastern India | 18Y/F | Community | Fever, cough, runny nose | ILI | Victoria+SARS-CoV-2 | Home | - | - | - | No | NA | Resolved in 10 days | None | Not vaccinated |
| 5 | Southern India | 74Y/M | Hospital | Fever, shortness of breath, runny nose | SARI | H3N2+SARS-CoV-2 | Hospital | 2 days | 18 days | No | No | Few atelectatic bands in lower lobes of both lungs. Fibroatelectatic changes in right lower lobe suggestive of bronchiectasis; mild pulmonary hypertension | Discharged after 18 days | CKD (on dialysis), COPD | Not vaccinated |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aggarwal, N.; Potdar, V.; Vijay, N.; Mukhopadhyay, L.; Borkakoty, B.; Manjusree, S.; Choudhary, M.L.; Chowdhury, D.; Verma, R.; Bhardwaj, S.D.; et al. SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report. Viruses 2022, 14, 627. https://doi.org/10.3390/v14030627
Aggarwal N, Potdar V, Vijay N, Mukhopadhyay L, Borkakoty B, Manjusree S, Choudhary ML, Chowdhury D, Verma R, Bhardwaj SD, et al. SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report. Viruses. 2022; 14(3):627. https://doi.org/10.3390/v14030627
Chicago/Turabian StyleAggarwal, Neeraj, Varsha Potdar, Neetu Vijay, Labanya Mukhopadhyay, Biswajyoti Borkakoty, S. Manjusree, Manohar Lal Choudhary, Deepika Chowdhury, Riya Verma, Sumit Dutt Bhardwaj, and et al. 2022. "SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report" Viruses 14, no. 3: 627. https://doi.org/10.3390/v14030627
APA StyleAggarwal, N., Potdar, V., Vijay, N., Mukhopadhyay, L., Borkakoty, B., Manjusree, S., Choudhary, M. L., Chowdhury, D., Verma, R., Bhardwaj, S. D., Sarmah, N., H., S. K., Kumar, P., & Gupta, N. (2022). SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report. Viruses, 14(3), 627. https://doi.org/10.3390/v14030627