
SARS-CoV-2 Vaccines during Pregnancy and Breastfeeding: A Systematic Review of Maternal and Neonatal Outcomes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
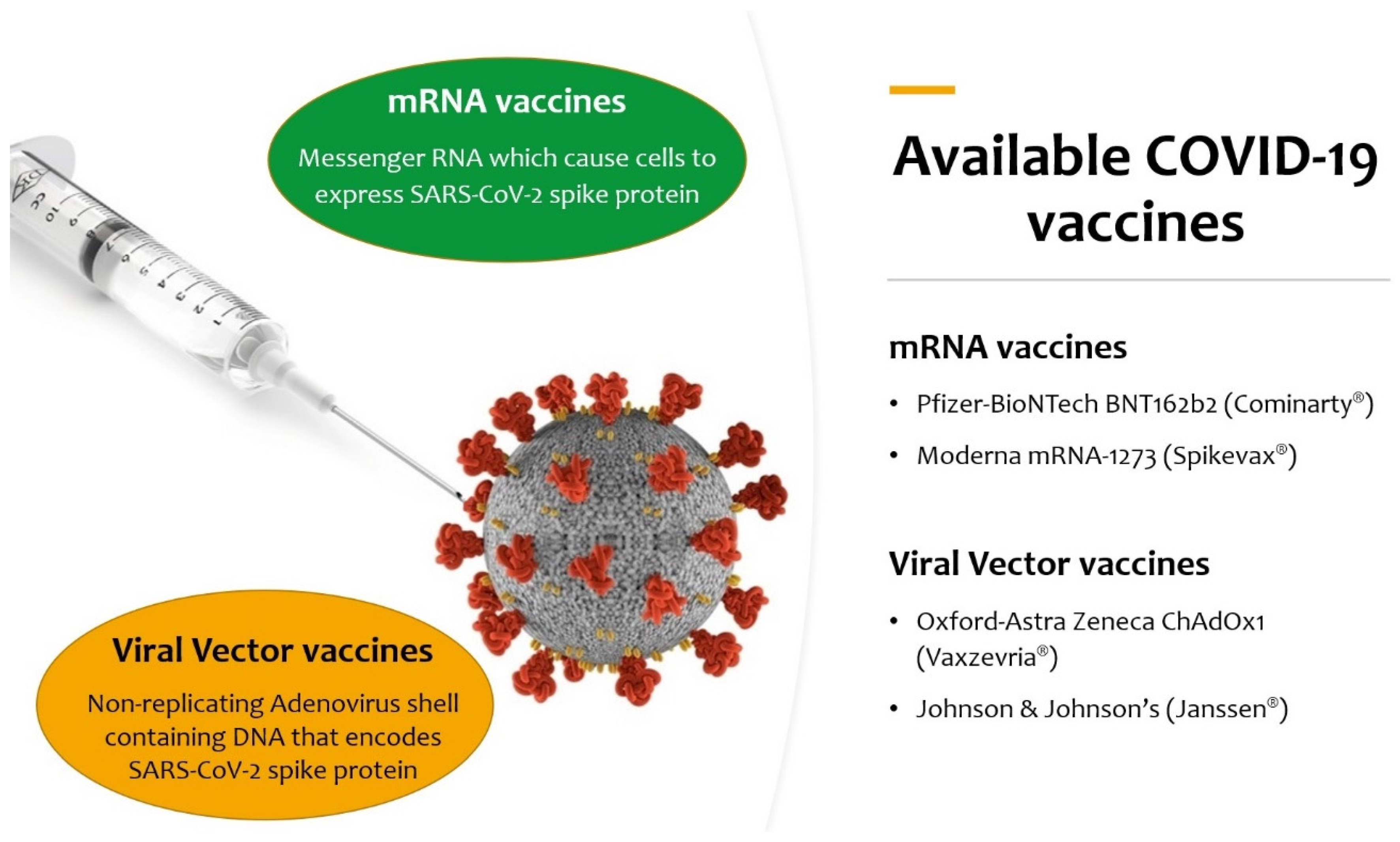
- mRNA vaccines: based on messenger RNA (mRNA) or a self-replicating RNA that provides the genetic information required to produce the spike protein: Pfizer–BioNTech BNT162b2 (Comirnaty®) and Moderna mRNA-1273 (Spikevax®);
- Viral-vector vaccines: an existing virus that is incompetent for replication but contains DNA that encodes for the spike protein. In the case of ChAdOx-1S, developed by the University of Oxford and AstraZeneca (Vaxzevria®), the vector is a modified chimpanzee adenovirus; in the case of Johnson & Johnson’s Ad26.COV2.S (Janssen®), the vector is a recombinant human adenovirus (Ad 26–serotype 26); in the case of the Russian Gam-COVID-Vac (Sputnik V®), two recombinant replication-defective human adenoviruses were used (Ad26 and Ad5–serotype 5); in the case of Ad5-nCov (Convidecia®), the vector is similarly the human adenovirus serotype 5 (Ad5);
- Recombinant protein vaccines: based on the laboratory synthesis of the spike protein, the receptor-binding domain (RBD), or virus-like particles. This category includes the American Nuvaxovid®/Indian Covovax ®, the Russian EpiVacCorona®, the Chinese ZF2001 (Zifivax®), the Cuban Soberana-2®, and the Sanofi-GSK VAT00008;
- Inactivated viral vaccines: the SARS-CoV-2 virus has been cultivated in cell cultures and chemically inactivated. This category includes the Chinese CoronaVac® and the Indian Covaxin®;
- Live-attenuated virus vaccines: a genetically weakened variant of the virus that replicates to a limited amount but does not cause illness while eliciting an immune response, as for measles, mumps, and rubella (MMR) vaccine;
- DNA vaccines: modified plasmids that carry genes that typically code for the spike protein, which is then produced in the vaccinated individual, as in Indian ZyCoV-D® COVID vaccine.
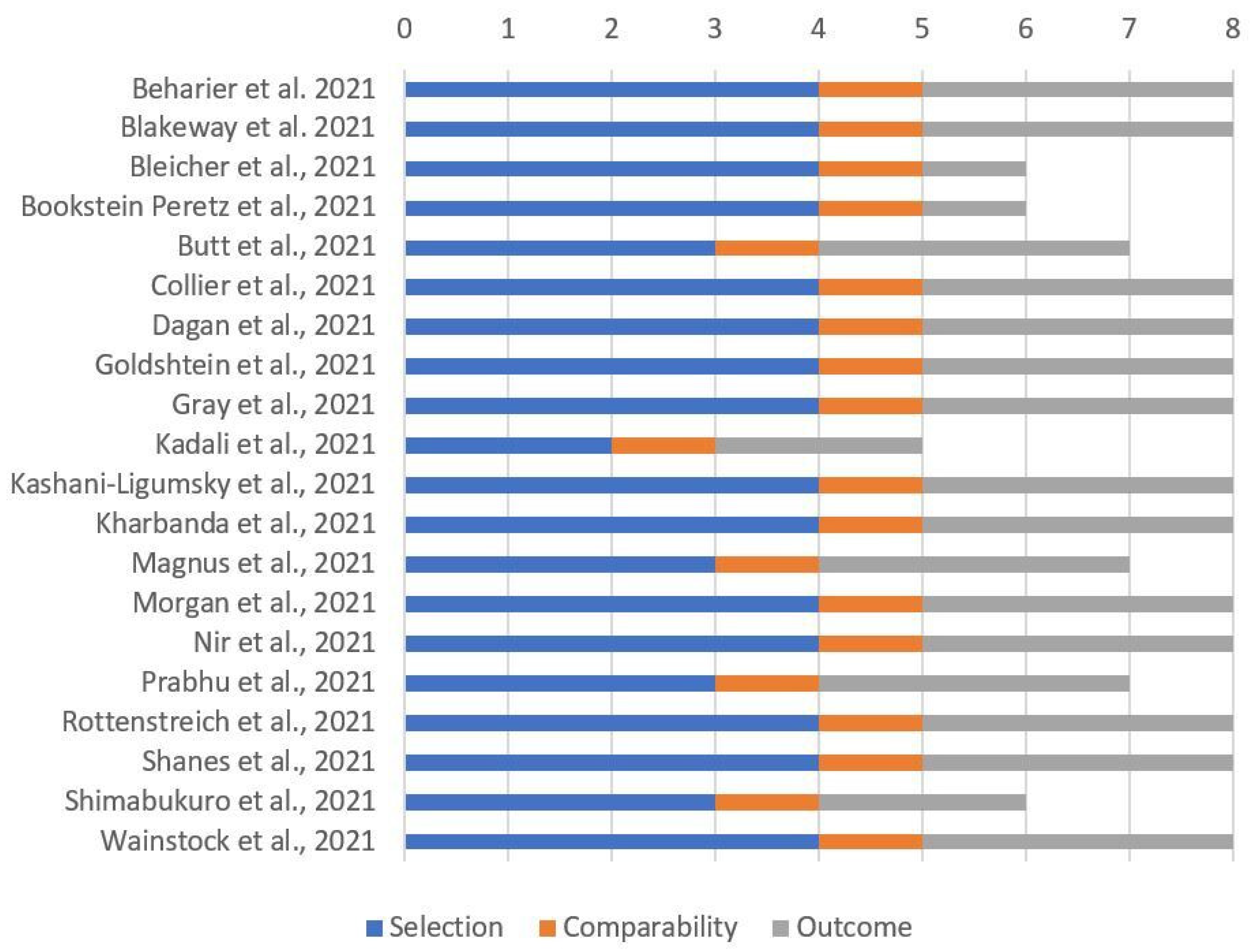
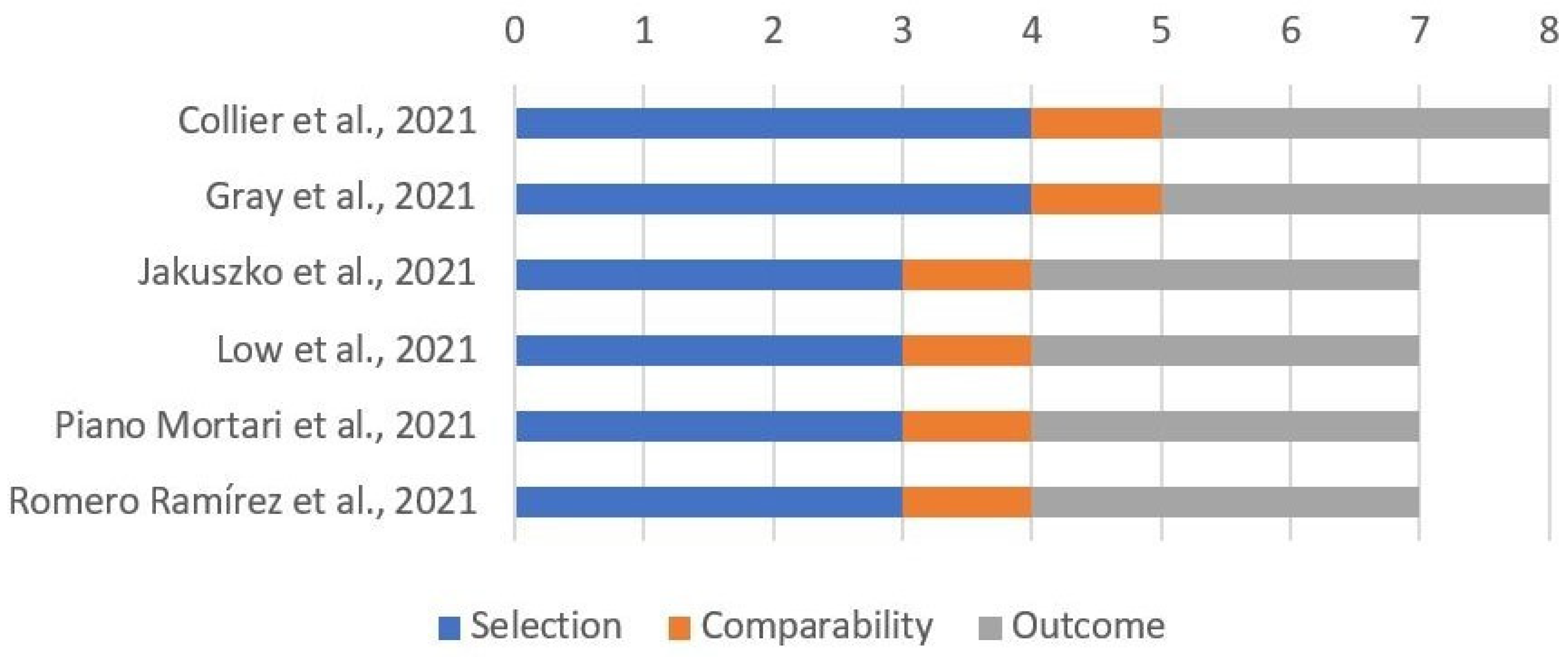
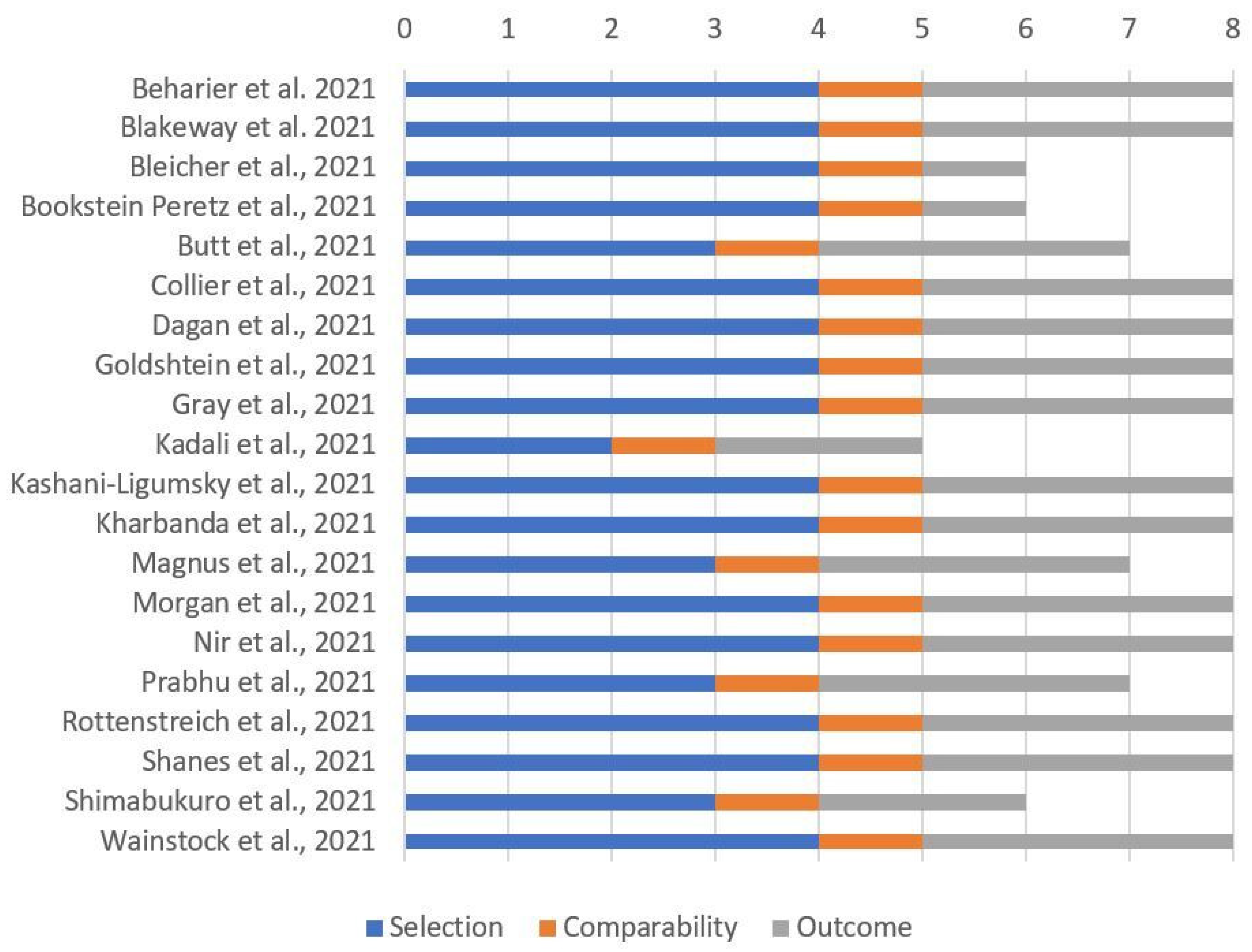
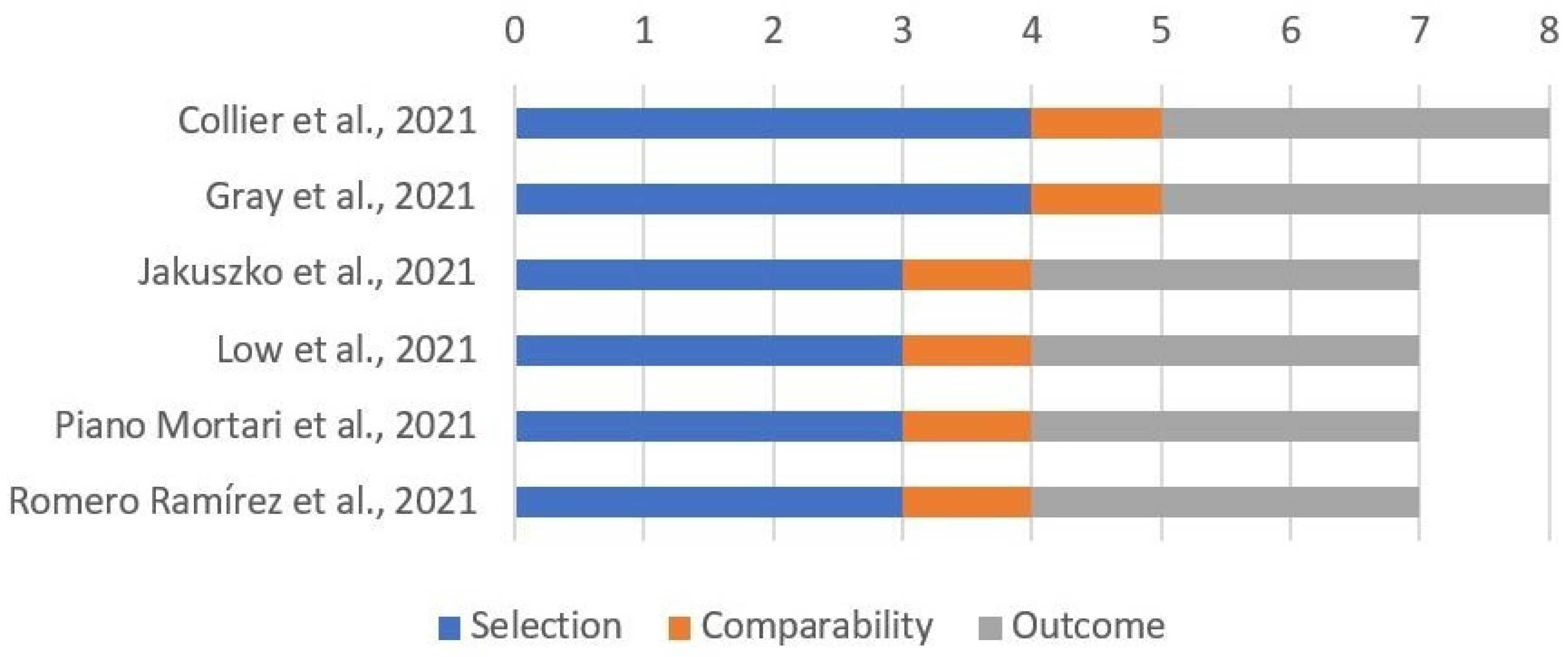
2.2. Assessment of Risk of Bias
3. Results
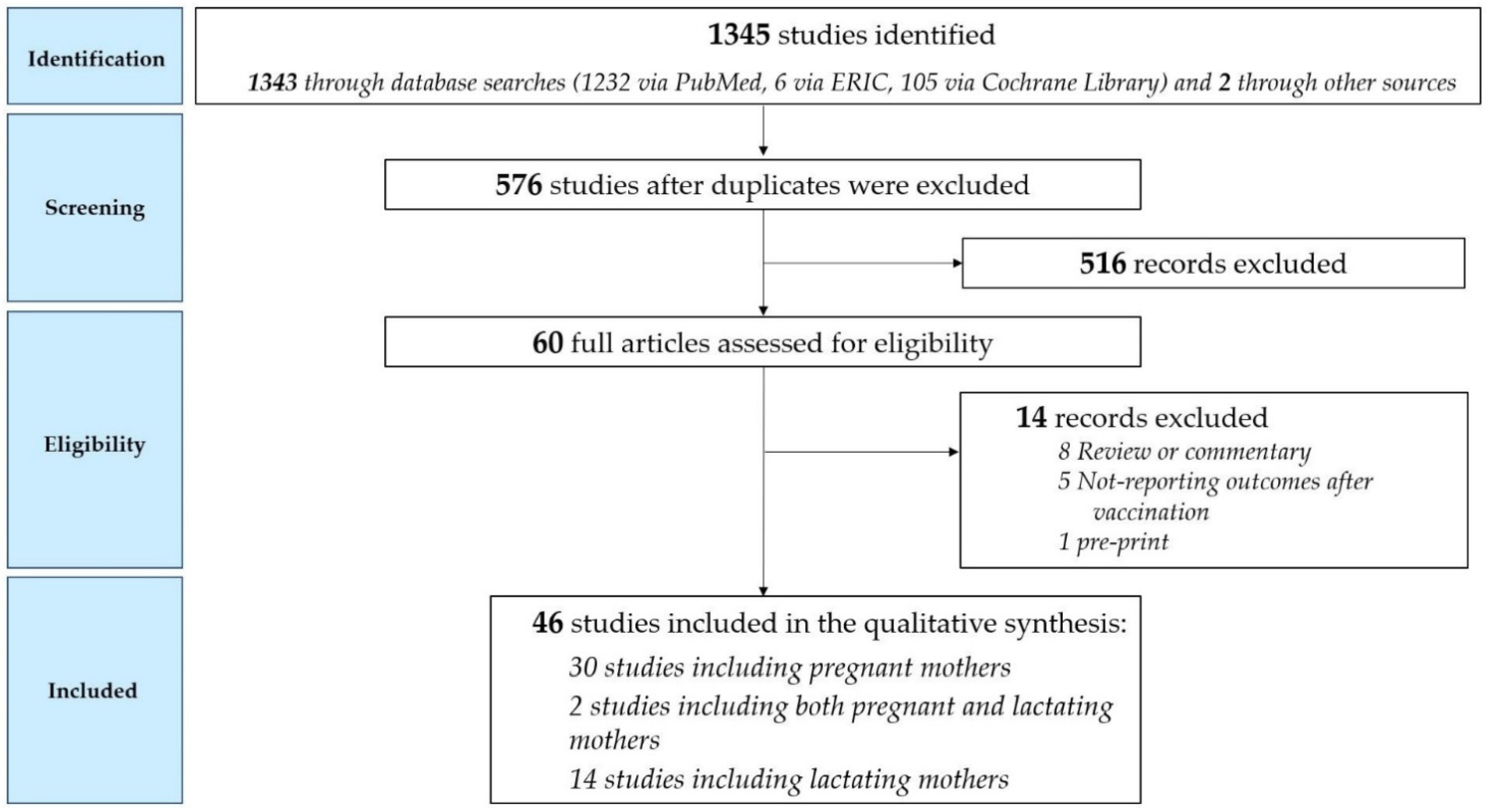
3.1. Study Selection Process
3.2. Synthesis of Results in Pregnant Women
3.3. Synthesis of Results in Lactating Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jamieson, D.J.; Rasmussen, S.A. An update on COVID-19 and pregnancy. Am. J. Obstet. Gynecol. 2021, 226, 177–186. [Google Scholar] [CrossRef]
- Arthurs, A.L.; Jankovic-Karasoulos, T.; Roberts, C.T. COVID-19 in pregnancy: What we know from the first year of the pandemic. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2021, 1867, 166248. [Google Scholar] [CrossRef]
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status-United States, 22 January–7 June 2020. MMWR Morb. Mortal. Wkly Rep. 2020, 69, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Principi, N.; Esposito, S. Is the immunization of pregnant women against covid-19 justified? Vaccines 2021, 9, 970. [Google Scholar] [CrossRef] [PubMed]
- Shook, L.L.; Fallah, P.N.; Silberman, J.N.; Edlow, A.G. COVID-19 Vaccination in Pregnancy and Lactation: Current Research and Gaps in Understanding. Front. Cell. Infect. Microbiol. 2021, 11, 899. [Google Scholar] [CrossRef]
- Martins, I.; Louwen, F.; Ayres-de-Campos, D.; Mahmood, T. EBCOG position statement on COVID-19 vaccination for pregnant and breastfeeding women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 262, 256–258. [Google Scholar] [CrossRef]
- Schaler, L.; Wingfield, M. COVID-19 vaccine—Can it affect fertility? Ir. J. Med. Sci. 2021, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Beharier, O.; Plitman Mayo, R.; Raz, T.; Nahum Sacks, K.; Schreiber, L.; Suissa-Cohen, Y.; Chen, R.; Gomez-Tolub, R.; Hadar, E.; Gabbay-Benziv, R.; et al. Efficient maternal to neonatal transfer of antibodies against SARS-CoV-2 and BNT162b2 mRNA COVID-19 vaccine. J Clin. Investig. 2021, 131, e150319. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am. J. Obstet. Gynecol. 2021, 226, 236.e1–236.e14. [Google Scholar] [CrossRef]
- Bleicher, I.; Kadour-Peero, E.; Sagi-Dain, L.; Sagi, S. Early exploration of COVID-19 vaccination safety and effectiveness during pregnancy: Interim descriptive data from a prospective observational study. Vaccine 2021, 39, 6535–6538. [Google Scholar] [CrossRef] [PubMed]
- Bookstein Peretz, S.; Regev, N.; Novick, L.; Nachshol, M.; Goffer, E.; Ben-David, A.; Asraf, K.; Doolman, R.; Levin, E.G.; Regev Yochay, G.; et al. Short-term outcome of pregnant women vaccinated with BNT162b2 mRNA COVID-19 vaccine. Ultrasound Obstet. Gynecol. 2021, 58, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.A.; Chemaitelly, H.; al Khal, A.; Coyle, P.V.; Saleh, H.; Kaleeckal, A.; Latif, A.N.; Bertollini, R.; Abou-Samra, A.B.; Abu-Raddad, L.J. SARS-CoV-2 vaccine effectiveness in preventing confirmed infection in pregnant women. J. Clin. Investig. 2021, 131, e153662. [Google Scholar] [CrossRef] [PubMed]
- Cassaniti, I.; Percivalle, E.; Zelini, P.; Nanhorngue, K.N.; Parolo, A.; Bernardi, V.; Jorizzo, G.; Santer, P.; Perotti, F.; Spinillo, A.; et al. Both SARS-CoV-2 infection and vaccination in pregnancy elicited neutralizing antibodies in pregnant women and newborns. Clin. Microbiol. Infect. 2021, 27, 1708–1709. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Biron-Shental, T.; Makov-Assif, M.; Key, C.; Kohane, I.S.; Hernán, M.A.; Lipsitch, M.; Hernandez-Diaz, S.; Reis, B.Y.; et al. Effectiveness of the BNT162b2 mRNA COVID-19 vaccine in pregnancy. Nat. Med. 2021, 27, 1693–1695. [Google Scholar] [CrossRef]
- Douxfils, J.; Gillot, C.; de Gottal, É.; Vandervinne, S.; Bayart, J.L.; Dogné, J.M.; Favresse, J. Efficient Maternal to Neonate Transfer of Neutralizing Antibodies after SARS-CoV-2 Vaccination with BNT162b2: A Case-Report and Discussion of the Literature. Vaccines 2021, 9, 907. [Google Scholar] [CrossRef]
- Gill, L.; Jones, C.W. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibodies in Neonatal Cord Blood After Vaccination in Pregnancy. Obstet. Gynecol. 2021, 137, 894–896. [Google Scholar] [CrossRef]
- Gloeckner, S.; Hornung, F.; Heimann, Y.; Schleussner, E.; Deinhardt-Emmer, S.; Loeffler, B.; Zoellkau, J. Newborns’ passive humoral SARS-CoV-2 immunity following heterologous vaccination of the mother during pregnancy. Am. J. Obstet. Gynecol. 2021, 226, 261–262. [Google Scholar] [CrossRef]
- Goldshtein, I.; Nevo, D.; Steinberg, D.M.; Rotem, R.S.; Gorfine, M.; Chodick, G.; Segal, Y. Association Between BNT162b2 Vaccination and Incidence of SARS-CoV-2 Infection in Pregnant Women. JAMA 2021, 326, 728–735. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.R.; Racherla, S.; Tirumala, R.; Madathala, R.R.; Gajula, V. Adverse effects of COVID-19 messenger RNA vaccines among pregnant women: A cross-sectional study on healthcare workers with detailed self-reported symptoms. Am. J. Obstet. Gynecol. 2021, 225, 458–460. [Google Scholar] [CrossRef]
- Kashani-Ligumsky, L.; Lopian, M.; Cohen, R.; Senderovich, H.; Czeiger, S.; Halperin, A.; Chaim, A.B.; Kremer, I.; Lessing, J.B.; Somekh, E.; et al. Titers of SARS-CoV-2 antibodies in cord blood of neonates whose mothers contracted SARS CoV-2 (COVID-19) during pregnancy and in those whose mothers were vaccinated with mRNA to SARS CoV-2 during pregnancy. J. Perinatol. 2021, 41, 2621–2624. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, E.O.; Haapala, J.; DeSilva, M.; Vazquez-Benitez, G.; Vesco, K.K.; Naleway, A.L.; Lipkind, H.S. Spontaneous Abortion Following COVID-19 Vaccination During Pregnancy. JAMA 2021, 326, 1629–1631. [Google Scholar] [CrossRef] [PubMed]
- Magnus, M.C.; Gjessing, H.K.; Eide, H.N.; Wilcox, A.J.; Fell, D.B.; Håberg, S.E. Covid-19 Vaccination during Pregnancy and First-Trimester Miscarriage. N. Engl. J. Med. 2021, 385, 2008–2010. [Google Scholar] [CrossRef] [PubMed]
- Mangat, C.; Milosavljevic, N. BNT162b2 Vaccination during Pregnancy Protects Both the Mother and Infant: Anti-SARS-CoV-2 S Antibodies Persistently Positive in an Infant at 6 Months of Age. Case Rep. Pediatr. 2021, 2021, 6901131. [Google Scholar] [CrossRef]
- Mehaffey, J.H.; Arnold, M.; Huffstetler, E.; Mehaffey, R.L.; Quillian, H.; Mehaffey, J.H. Successful vertical transmission of SARS-CoV-2 antibodies after maternal vaccination. Birth 2021, 48, 451–452. [Google Scholar] [CrossRef]
- Mithal, L.B.; Otero, S.; Shanes, E.D.; Goldstein, J.A.; Miller, E.S. Cord blood antibodies following maternal coronavirus disease 2019 vaccination during pregnancy. Am. J. Obstet. Gynecol. 2021, 225, 192–194. [Google Scholar] [CrossRef]
- Morgan, J.A.; Biggio, J.R.; Martin, J.K.; Mussarat, N.; Chawla, H.K.; Puri, P.; Williams, F.B. Maternal Outcomes After Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Vaccinated Compared With Unvaccinated Pregnant Patients. Obstet. Gynecol. 2022, 139, 107–109. [Google Scholar] [CrossRef]
- Nir, O.; Schwartz, A.; Toussia-Cohen, S.; Leibovitch, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Lustig, Y.; et al. Maternal-neonatal transfer of SARS-CoV-2 immunoglobulin G antibodies among parturient women treated with BNT162b2 messenger RNA vaccine during pregnancy. Am. J. Obstet. Gynecol. MFM 2021, 4, 100492. [Google Scholar] [CrossRef]
- Paul, G.; Chad, R. Newborn antibodies to SARS-CoV-2 detected in cord blood after maternal vaccination—A case report. BMC Pediatr. 2021, 21, 138. [Google Scholar] [CrossRef]
- Prabhu, M.; Murphy, E.A.; Sukhu, A.C.; Yee, J.; Singh, S.; Eng, D.; Zhao, Z.; Riley, L.E.; Yang, Y.J. Antibody Response to Coronavirus Disease 2019 (COVID-19) Messenger RNA Vaccination in Pregnant Women and Transplacental Passage Into Cord Blood. Obstet. Gynecol. 2021, 138, 278–280. [Google Scholar] [CrossRef]
- Rottenstreich, A.; Zarbiv, G.; Oiknine-Djian, E.; Zigron, R.; Wolf, D.G.; Porat, S. Efficient maternofetal transplacental transfer of anti-SARS-CoV-2 spike antibodies after antenatal SARS-CoV-2 BNT162b2 mRNA vaccination. Clin. Infect. Dis. 2021, 73, 1909–1912. [Google Scholar] [CrossRef] [PubMed]
- Rottenstreich, M.; Sela, H.Y.; Rotem, R.; Kadish, E.; Wiener-Well, Y.; Grisaru-Granovsky, S. Covid-19 vaccination during the third trimester of pregnancy: Rate of vaccination and maternal and neonatal outcomes, a multicentre retrospective cohort study. BJOG 2022, 129, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Shanes, E.D.; Otero, S.; Mithal, L.B.; Mupanomunda, C.A.; Miller, E.S.; Goldstein, J.A. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccination in Pregnancy: Measures of Immunity and Placental Histopathology. Obstet. Gynecol. 2021, 138, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef]
- Trostle, M.E.; Aguero-Rosenfeld, M.E.; Roman, A.S.; Lighter, J.L. High antibody levels in cord blood from pregnant women vaccinated against COVID-19. Am. J. Obstet. Gynecol. MFM 2021, 3, 100481. [Google Scholar] [CrossRef]
- Wainstock, T.; Yoles, I.; Sergienko, R.; Sheiner, E. Prenatal maternal COVID-19 vaccination and pregnancy outcomes. Vaccine 2021, 39, 6037–6040. [Google Scholar] [CrossRef]
- Zauche, L.H.; Wallace, B.; Smoots, A.N.; Olson, C.K.; Oduyebo, T.; Kim, S.Y.; Petersen, E.E.; Ju, J.; Beauregard, J.; Wilcox, A.J.; et al. Receipt of mRNA Covid-19 Vaccines and Risk of Spontaneous Abortion. N. Engl. J. Med. 2021, 385, 1533–1535. [Google Scholar] [CrossRef]
- Zdanowski, W.; Waśniewski, T. Evaluation of SARS-CoV-2 Spike Protein Antibody Titers in cord blood after COVID-19 vaccination during pregnancy in Polish healthcare workers: Preliminary results. Vaccines 2021, 9, 675. [Google Scholar] [CrossRef]
- Collier, A.R.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Apraku Bondzie, E.; Sellers, D.; et al. Immunogenicity of COVID-19 mRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370–2380. [Google Scholar] [CrossRef]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. Coronavirus disease 2019 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, 303.e1–303.e17. [Google Scholar] [CrossRef]
- Baird, J.K.; Jensen, S.M.; Urba, W.J.; Fox, B.A.; Baird, J.R. SARS-CoV-2 Antibodies Detected in Mother’s Milk Post-Vaccination. J. Hum. Lact. 2021, 37, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, K.; Honerkamp-Smith, G.; Chambers, C.D. Maternal and Child Outcomes Reported by Breastfeeding Women following Messenger RNA COVID-19 Vaccination. Breastfeed. Med. 2021, 16, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Charepe, N.; Gonçalves, J.; Juliano, A.M.; Lopes, D.G.; Canhão, H.; Soares, H.; Serrano, E.F. COVID-19 mRNA vaccine and antibody response in lactating women: A prospective cohort study. BMC Pregnancy Childbirth 2021, 21, 632. [Google Scholar] [CrossRef] [PubMed]
- Golan, Y.; Prahl, M.; Cassidy, A.; Lin, C.Y.; Ahituv, N.; Flaherman, V.J.; Gaw, S.L. Evaluation of Messenger RNA From COVID-19 BTN162b2 and mRNA-1273 Vaccines in Human Milk. JAMA Pediatr 2021, 175, 1069–1071. [Google Scholar] [CrossRef]
- Guida, M.; Terracciano, D.; Cennamo, M.; Aiello, F.; la Civita, E.; Esposito, G.; Gargiulo, V.; Maruotti, G.M.; Portella, G.; Sarno, L. COVID-19 Vaccine mRNABNT162b2 Elicits Human Antibody Response in Milk of Breastfeeding Women. Vaccines 2021, 9, 785. [Google Scholar] [CrossRef]
- Jakuszko, K.; Kościelska-Kasprzak, K.; Żabińska, M.; Bartoszek, D.; Poznański, P.; Rukasz, D.; Rukasz, D.; Kłak, R.; Królak-Olejnik, B.; Krajewska, M. Immune response to vaccination against covid-19 in breastfeeding health workers. Vaccines 2021, 9, 663. [Google Scholar] [CrossRef]
- Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. The Levels of SARS-CoV-2 Specific Antibodies in Human Milk Following Vaccination. J. Hum. Lact. 2021, 37, 477–484. [Google Scholar] [CrossRef]
- Kelly, J.C.; Carter, E.B.; Raghuraman, N.; Nolan, L.S.; Gong, Q.; Lewis, A.N.; Good, M. Anti-severe acute respiratory syndrome coronavirus 2 antibodies induced in breast milk after Pfizer-BioNTech/BNT162b2 vaccination. Am. J. Obstet. Gynecol. 2021, 225, 101–103. [Google Scholar] [CrossRef]
- Lechosa-Muñiz, C.; Paz-Zulueta, M.; Mendez-Legaza, J.M.; Irure-Ventura, J.; Cuesta González, R.; Calvo Montes, J.; López-Hoyos, M.; Llorca, J.; Cabero-Pérez, M.J. Induction of SARS-CoV-2-Specific IgG and IgA in Serum and Milk with Different SARS-CoV-2 Vaccines in Breastfeeding Women: A Cross-Sectional Study in Northern Spain. Int. J. Environ. Res. Public Health 2021, 18, 8831. [Google Scholar] [CrossRef]
- Low, J.M.; Gu, Y.; Ng, M.S.F.; Amin, Z.; Lee, L.Y.; Ng, Y.P.M.; Shunmuganathan, B.D.; Niu, Y.; Gupta, R.; Tambyah, P.A.; et al. Codominant IgG and IgA expression with minimal vaccine mRNA in milk of BNT162b2 vaccinees. NPJ Vaccines 2021, 6, 105. [Google Scholar] [CrossRef]
- McLaurin-Jiang, S.; Garner, C.D.; Krutsch, K.; Hale, T.W. Maternal and Child Symptoms following COVID-19 Vaccination among Breastfeeding Mothers. Breastfeed. Med. 2021, 16, 702–709. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2-Specific Antibodies in Breast Milk After COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef] [PubMed]
- Piano Mortari, E.; Russo, C.; Vinci, M.R.; Terreri, S.; Fernandez Salinas, A.; Piccioni, L.; Alteri, C.; Colagrossi, L.; Coltella, L.; Ranno, S.; et al. Highly Specific Memory B Cells Generation after the 2nd Dose of BNT162b2 Vaccine Compensate for the Decline of Serum Antibodies and Absence of Mucosal IgA. Cells 2021, 10, 2541. [Google Scholar] [CrossRef] [PubMed]
- Romero Ramirez, D.S.; Lara Pérez, M.M.; Carretero Pérez, M.; Suarez Hernandez, M.I.; Martin Pulido, S.; Pera Villacampa, L.; Fernández Vilar, A.M.; Rivero Falero, M.; González Carretero, P.; Reyes Millán, B.; et al. SARS-CoV-2 Antibodies in Breast Milk After Vaccination. Pediatrics 2021, 148, e2021052286. [Google Scholar] [CrossRef] [PubMed]
- Golan, Y.; Prahl, M.; Cassidy, A.G.; Gay, C.; Wu, A.H.B.; Jigmeddagva, U.; Lin, C.Y.; Gonzalez, V.J.; Basilio, E.; Chidboy, M.A.; et al. COVID-19 mRNA Vaccination in Lactation: Assessment of Adverse Events and Vaccine Related Antibodies in Mother-Infant Dyads. Front. Immunol. 2021, 12, 777103. [Google Scholar] [CrossRef] [PubMed]
- Mackin, D.W.; Walker, S.P. The historical aspects of vaccination in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 76, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Shamshirsaz, A.A.; Hessami, K.; Morain, S.; Afshar, Y.; Nassr, A.A.; Arian, S.E.; Asl, N.M.; Aagaard, K. Intention to Receive COVID-19 Vaccine during Pregnancy: A Systematic Review and Meta-analysis. Am. J. Perinatol. 2021. [Google Scholar] [CrossRef]
- Ciapponi, A.; Bardach, A.; Comandé, D.; Berrueta, M.; Argento, F.J.; Rodriguez Cairoli, F.; Zamora, N.; Santa María, V.; Xiong, X.; Zaraa, S.; et al. COVID-19 and pregnancy: An umbrella review of clinical presentation, vertical transmission, and maternal and perinatal outcomes. PLoS ONE 2021, 16, e0253974. [Google Scholar] [CrossRef]
- Kazemi, S.N.; Hajikhani, B.; Didar, H.; Hosseini, S.S.; Haddadi, S.; Khalili, F.; Mirsaeidi, M.; Nasiri, M.J. COVID-19 and cause of pregnancy loss during the pandemic: A systematic review. PLoS ONE 2021, 16, e0255994. [Google Scholar] [CrossRef]
- Olivini, N.; Calò Carducci, F.I.; Santilli, V.; de Ioris, M.A.; Scarselli, A.; Alario, D.; Geremia, C.; Lombardi, M.H.; Marabotto, C.; Mariani, R.; et al. A neonatal cluster of novel coronavirus disease 2019: Clinical management and considerations. Ital. J. Pediatr. 2020, 46, 180. [Google Scholar] [CrossRef]
- Garazzino, S.; Montagnani, C.; Donà, D.; Meini, A.; Felici, E.; Vergine, G.; Bernardi, S.; Giacchero, R.; Lo Vecchio, A.; Marchisio, P.; et al. Multicentre Italian study of SARS-CoV-2 infection in children and adolescents, preliminary data as at 10 April 2020. Eurosurveillance 2020, 25, 2000600. [Google Scholar] [CrossRef] [PubMed]
- Lakshminrusimha, S.; Hudak, M.; Dimitriades, V.; Higgins, R. Multisystem Inflammatory Syndrome (MIS-C) in Neonates (MIS-N) Following Maternal SARS CoV-2 COVID-19 Infection. Am. J. Perinatol. 2021. [Google Scholar] [CrossRef]
- Lumbreras-Marquez, M.I.; Fields, K.G.; Campos-Zamora, M.; Rodriguez-Bosch, M.R.; Rodriguez-Sibaja, M.J.; Copado-Mendoza, D.Y.; Acevedo-Gallegos, S.; Farber, M.K. A forecast of maternal deaths with and without vaccination of pregnant women against COVID-19 in Mexico. Int. J. Gynaecol. Obstet. 2021, 154, 566–567. [Google Scholar] [CrossRef]
- COVID-19 Vaccines International Pregnancy Exposure Registry (C-VIPER)—ClinicalTrials.gov—Identifier: NCT04705116. 2021. Available online: https://clinicaltrials.gov/ct2/show/study/NCT04705116 (accessed on 22 November 2021).
- The American College of Obstetricians and Gynecologists (ACOG). COVID-19 Vaccination Considerations for Obstetric-Gynecologic Care. 2021. Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2020/12/covid-19-vaccination-considerations-for-obstetric-gynecologic-care (accessed on 22 November 2021).
- Italian National Institute of Health and Italian Obstetric Surveillance System, Rome (Italy). Ad Interim Indications on “COVID-19 Vaccination during Pregnancy and Breastfeeding” (Update of 2021, September 22). Available online: https://www.epicentro.iss.it/en/vaccines/covid-19-pregnancy-breastfeeding (accessed on 22 November 2021).
- Graham, J.M., Jr. Update on the gestational effects of maternal hyperthermia. Birth Defects Res. 2020, 112, 943–952. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Country, Design | Type of Vaccine (Doses Given) | Vaccinated Pregnant Women (n) | First Vaccine Dose GA* | Outcome | Conclusions |
|---|---|---|---|---|---|---|
| Beharier, 2021 [9] | Israel, prospective, multicenter | Pfizer–BioNTech BNT162b2 (2 doses) | 86 | Mean ± SD: 34.5 ± 7.5 | Antibodies in maternal blood and in umbilical cord blood | Strong maternal humoral IgG response (anti-S and RBD) that crosses the placenta barrier and approaches maternal titers in the fetus within 15 days following the first dose. |
| Blakeway, 2021 [10] | United Kingdom, retrospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 or Oxford–AstraZeneca ChAdOx1 (at least one dose) | 140 | Second or third trimester | Uptake of COVID-19 vaccination and perinatal safety outcomes | Lower uptake among younger women, non-White ethnicity, and lower socioeconomic background. In a propensity score-matched cohort, the rates of adverse pregnancy outcomes were similar to that of unvaccinated pregnant women: stillbirth, fetal abnormalities, postpartum hemorrhage, cesarean delivery, small for gestational age, maternal high-dependency unit or ICU admission, or NICU admission. |
| Bleicher, 2021 [11] | Israel, an interim analysis of a prospective study | Pfizer–BioNTech BNT162b2 (at least one dose) | 80 | 1st trimester (17.8%), 2nd trimester (54.5%), 3rd trimester (27.7%) | Complications in vaccinated and nonvaccinated pregnant women considered any of the following: vaginal bleeding, pregnancy loss, hypertension, gestational diabetes, and preterm birth | mRNA vaccine during pregnancy seems not to increase the rate of pregnancy complications and is effective in prevention of COVID-19 infection. |
| Bookstein Peretz, 2021 [12] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 57 | Median 32.4 (IQR 31.2–33.6) | Vaccine-induced immunity and adverse events associated with the BNT162b2 vaccine among pregnant women | Favorable short-term obstetric and neonatal outcomes. The vaccine is effective in inducing humoral immunity in pregnant women, although SARS-CoV-2 IgG levels were lower when compared with those in nonpregnant vaccinated women. None of the pregnancies were complicated by fetal or neonatal death, and two (3.5%) neonates required NICU admission for respiratory support. |
| Butt, 2021 [13] | Qatar, retrospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 407 | 1st trimester (79.4%) or 2nd trimester (20.6%) | Vaccine effectiveness of mRNA vaccines in preventing confirmed SARS-CoV-2 infection during pregnancy >14 days after the second dose of the vaccine | Vaccine effectiveness was 86.8% (95% CI: 47.5–98.5) ≥14 days after the second dose. In the test-negative analysis, vaccine effectiveness >14 days after the first dose but before the second dose was 40.8% (95% CI: 0.0–80.4). |
| Cassaniti, 2021 [14] | Italy, retrospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 2 | 31+4 and 27+6 | Neutralizing antibodies in pregnant women and newborns | Antibody transfer occurred efficiently from mothers showing anti-SARS-CoV-2 IgG at delivery (elicited either by infection or by vaccination). However, the median neutralizing titer was twofold reduced in newborns with respect to mothers. This may be due to the contributions to neutralization in maternal serum of spike-specific IgA levels, which are not transmitted to the fetus. |
| Collier, 2021 [39] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 30 | 1st trimester (17%), 2nd trimester (50%), 3rd trimester (33%) | Immunogenicity of the current COVID-19 mRNA vaccines in pregnant and lactating women against both the original SARS-CoV-2 USA-WA1/2020 strain and the B.1.1.7 and B.1.351 variants of concern | Binding, neutralizing, and functional non-neutralizing antibody responses, as well as CD4 and CD8 T-cell responses, were present in pregnant, lactating, and nonpregnant women following vaccination. Binding and neutralizing antibodies were also observed in infant cord blood and breast milk. Binding and neutralizing antibody titers against the SARS-CoV-2 B.1.1.7 and B.1.351 variants of concern were reduced, but T-cell responses were preserved against viral variants. |
| Dagan, 2021 [15] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 10,861 | NA | Documented infection with SARS-CoV-2, symptomatic COVID-19, COVID-19-related hospitalization, severe illness, and death | High vaccine effectiveness of BNT162b2 was documented in pregnant women: estimated vaccine effectiveness from 7 through to 56 days after the second dose was 96% (95% CI: 89–100%) for any documented infection, 97% (91–100%) for infections with documented symptoms and 89% (43–100%) for COVID-19-related hospitalization. No deaths were observed. |
| Douxfils, 2021 [16] | Belgium, case report | Pfizer–BioNTech BNT162b2 (2 doses) | 1 | 25 | Neutralizing capacity of umbilical cord blood compared to maternal blood | Successful maternal to fetal transfer of neutralizing antibodies after vaccination with BNT162b2 in a pregnant woman at 25 weeks of gestation. The levels of neutralizing antibodies were approximately fivefold higher in the umbilical cord than in the maternal blood, while the level of total antibodies showed only a twofold increase. |
| Gill and Jones, 2021 [17] | United States, case report | Pfizer–BioNTech BNT162b2 (2 doses) | 1 | 32+6 | Antibodies in maternal blood and in umbilical cord blood | Vaccination in pregnancy produced a robust immune response for the patient, with subsequent transplacental transfer of neutralizing antibodies |
| Gloeckner, 2021 [18] | Germany, retrospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 after a prime vaccination with Oxford–AstraZeneca ChAdOx1 (boost vaccination with a dose of mRNA vaccine after a prime vaccination with a vector-based vaccine) | 3 | NA | Antibody kinetics following heterologous vaccination in pregnant women in comparison to their newborns, as well as to a healthy nonpregnant control group | Vaccine induced SARS-CoV-2 spike IgG antibodies after vector-based prime vaccination in pregnancy, with an average increase of more than one log10 level after an mRNA-based boost. No significant differences were found compared with nonpregnant controls. They found similar levels of anti-spike IgG antibodies with a high neutralization capacity in the cord serum, indicating a strong passive humoral immunity in the newborns. |
| Goldshtein, 2021 [19] | Israel, retrospective, multi-center | Pfizer–BioNTech BNT162b2 (at least one dose) | 7530 | 2nd and 3rd trimester | Documented SARS-CoV-2 infection 28 days or more after the first vaccine dose | BNT162b2 mRNA vaccination compared with no vaccination was associated with a significantly lower risk of SARS-CoV-2 infection. For 28 days or more postvaccination, a statistically significant hazard reduction was observed among the vaccinated group compared with the unvaccinated group (aHR = 0.22; 95%CI: 0.11–0.43; robust p < 0.001) |
| Gray, 2021 [40] | United States, retrospective, multi-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 84 | 23.2 (IQR 16.3–32.1) | Vaccine-induced immunity in vaccinated pregnant and lactating women | Robust and comparable IgG titers were observed across pregnant, lactating, and nonpregnant controls, all of which were significantly higher than those observed in pregnant women with previous SARS-CoV-2 infection. Boosting resulted in augmented IgG levels in the blood, translating to transfer of IgG to the neonate through the placenta and breast milk. |
| Kadali, 2021 [20] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose) | 38 | NA | Side-effect profile of the mRNA vaccines among pregnant healthcare workers (HCWs) with that of nonpregnant HCWs | No significant statistical differences were found between the groups for all of the symptoms reported for both groups (however, the participant with a report of seizure had a known history of seizure disorder and borderline low anticonvulsant blood levels). |
| Kashani-Ligumsky, 2021 [21] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 29 | 3rd trimester | Titers of IgG antibodies to SARS-CoV-2 in umbilical cord blood in vaccinated pregnant women | Neonates born to mothers vaccinated during pregnancy had higher antibody titers and may, therefore, have more prolonged protection compared to those born to women infected during pregnancy. |
| Kharbanda, 2021 [22] | United States, retrospective case-control surveillance analysis of CDC Vaccine Safety Datalink | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 or Janssen vaccine (at least one dose) | 21,267 | 6–19 | Case–control surveillance of COVID-19 vaccination during pregnancy and spontaneous abortion | Spontaneous abortions did not have an increased odds of exposure to a COVID-19 vaccination in the prior 28 days compared with ongoing pregnancies (adjusted odds ratio, 1.02; 95% CI: 0.96–1.08). Results were consistent for mRNA-1273 and BNT162b2 and by gestational age group. |
| Magnus, 2021 [23] | Norway, case-control, multi-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 or Oxford–AstraZeneca ChAdOx1 (at least one dose) | 772 | NA | Previous COVID-19 vaccination and first-trimester miscarriage risk among women who had a miscarriage before 14 weeks of GA | No evidence of an increased risk for early pregnancy loss after COVID-19 vaccination. |
| Mangat, 2021 [24] | United States, case report | Pfizer–BioNTech BNT162b2 (2 doses) | 1 | 22 | Antibodies in neonatal blood | Persistence of anti-SARS-CoV-2 S antibodies was noted in a preterm infant at 6 months of age, which correlates with the prevention of COVID-19 and its complications in early infancy. |
| Mehaffey, 2021 [25] | United States, case report | Pfizer–BioNTech BNT162b2 (2 doses) | 1 | 29 | Antibodies in maternal and umbilical cord blood | Vertical transmission of IgG SARS-CoV-2 specific antibodies from a vaccinated mother to her son with no evidence of prior infection. |
| Mithal, 2021 [26] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose) | 27 | 33 ± 2 | Transfer of SARS-CoV-2 IgG to infants following maternal vaccination during pregnancy | Most pregnant women who received a mRNA vaccine during the third trimester had transplacental transfer of IgG to the infant. The observed mean IgG transfer ratio demonstrated that infant antibody levels are about equal to the maternal levels. |
| Morgan, 2021 [27] | United Sates, retrospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 or Janssen vaccine (at least one dose) | 1332 | NA | Incidence of severe or critical COVID-19 in vaccinated compared with unvaccinated pregnant patients in the context of Delta variant Predominance | Association between SARS-CoV-2 vaccination and lower odds of severe or critical COVID-19 and COVID-19 of any severity in pregnant patients during the Delta variant–predominant fourth surge of SARS-CoV-2. |
| Nir, 2021 [28] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 64 | Mean ± SD: 33.5 ± 3.2 weeks at second dosage | Antibodies in maternal blood and in umbilical cord blood | SARS-CoV-2 IgG antibodies were detected in cord blood, newborn dried blood spot, and breast milk samples. Neonatal and breast milk antibody levels were positively correlated with maternal serum antibody levels. Higher levels of cord blood antibodies were detected in vaccinated women than in COVID-19-recovered women. |
| Paul, 2021 [29] | United States, case report | Moderna mRNA-1273 (one dose) | 1 | 26 | Antibodies in umbilical cord blood after maternal vaccination | SARS-CoV-2 IgG antibodies were detectable in a newborn’s cord blood sample after only a single dose of the Moderna COVID-19 vaccine. |
| Prabhu, 2021 [30] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose) | 122 | NA | Antibodies in maternal blood and in umbilical cord blood | All women and cord blood samples, except for one, had detectable IgG antibodies by 4 weeks after vaccine dose 1. The increasing levels of maternal IgG over time and the increasing placental IgG transfer ratio over time suggest that timing between vaccination and birth may be an important factor to consider in vaccination strategies of pregnant women. |
| Rottenstreich, 2021 [31] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 (at least one dose) | 20 | 3rd trimester | Antibodies in maternal blood and in umbilical cord blood | They demonstrated an efficient placental transfer of IgG antibodies following maternal SARS-CoV-2 vaccination, and a positive correlation between maternal and cord blood antibody concentrations. Nevertheless, while neonatal antibody levels were satisfactory, placental transfer ratios were relatively lower (0.44 for anti-S and 0.34 for anti-RBD IgG) as compared to prior studies of vaccine-elicited antibodies to influenza, pertussis, measles, rubella, and hepatitis B, in which transfer ratios ranging from 0.8 to 1.7 have been reported. |
| Rottenstreich, 2021 [32] | Israel, retrospective, multi-center | Pfizer–BioNTech BNT162b2 (at least one dose) | 712 | 3rd trimester | Vaccination impact on adverse maternal and neonatal outcomes | The uptake of COVID-19 vaccination during the 3rd trimester of pregnancy was not associated with an increased risk of adverse maternal outcomes and lowered the risk for adverse neonatal outcomes |
| Shanes, 2021 [33] | United States, prospective, single-center | mRNA vaccine (not specified which, at least one dose) | 84 | NA | Frequency of placental lesions in patients who received SARS-CoV-2 vaccination in pregnancy | There was no observed increase in the incidence of findings characteristic of SARS-CoV-2 infection in pregnancy and no evidence of vaccine-triggered breakdown in maternal immunologic tolerance of the fetus. |
| Shimabukuro, 2021 [34] | United States, cross-sectional survey | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose) | 35,691 women | Periconception period (2.3%, 1st trimester (28.6%), 2nd trimester (43.3%), 3rd trimester (25.7%) | Participant-reported local and systemic reactogenicity to mRNA vaccines and pregnancy outcomes | Injection-site pain was reported more frequently among pregnant persons than among nonpregnant women, whereas headache, myalgia, chills, and fever were reported less frequently. Adverse neonatal outcomes included preterm birth (in 9.4%) and small size for gestational age (in 3.2%); no neonatal deaths were reported. Most abortions (92.3%) occurred before 13 weeks of gestation. |
| Trostle, 2021 [35] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose) | 36 | 1st trimester (6%), 2nd trimester (83%), 3rd trimester (11%) | Antibodies in maternal blood and in umbilical cord blood | Transplacental antibody transfer following mRNA COVID-19 vaccination during pregnancy, with 100% of cord blood specimens having high levels of anti-S antibodies. |
| Wainstock, 2021 [36] | Israel, retrospective, single-center | Pfizer–BioNTech BNT162b2 (at least one dose) | 913 | 2nd or 3rd trimester | Associations among prenatal Pfizer–BioNTech COVID-19 vaccination, pregnancy Course, and outcomes | Prenatal maternal COVID-19 vaccine had no adverse effects on pregnancy course and outcomes. |
| Zauche, 2021 [37] | United States, retrospective analysis of CDC v-safe COVID-19 vaccine pregnancy registry | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose either before conception or before 20 weeks of gestation) | 2022 | 20 | Cumulative risk of spontaneous abortion from 6 to less than 20 weeks of gestation | The cumulative risk of spontaneous abortion from 6 to less than 20 weeks of gestation was 14.1% (95% CI: 12.1–16.1) in the primary analysis and 12.8% (95% CI: 10.8–14.8) in an analysis using direct maternal age standardization to the reference population. As compared with data from two historical cohorts that represent the lower and upper ranges of spontaneous abortion risk, the risk of spontaneous abortion after mRNA COVID-19 vaccination either before conception or during pregnancy was consistent with the expected risk of spontaneous abortion; these findings add to the accumulating evidence about the safety of mRNA COVID-19 vaccination in pregnancy. |
| Zdanowski, 2021 [38] | Poland, retrospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 16 | 31.8 ± 2.1 | Antibodies in maternal blood and in umbilical cord blood | High titers of anti-S antibodies in cord blood after birth, suggesting that maternal immunization may provide protection to newborns through the transplacental transfer of antibodies. The trend in the correlation coefficients of the number of weeks from the first vaccine dose to delivery is worth noting. |
| First Author, Year | Country, Design | Type of Vaccine (Doses Given) | Vaccinated Lactating Women (n) | Outcome | Conclusions |
|---|---|---|---|---|---|
| Baird, 2021 [41] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 7 | Antibodies in human milk | Significantly elevated levels of SARS-CoV-2-specific IgG and IgA antibodies in human milk beginning approximately 7 days after the initial vaccine dose, with an IgG-dominant response. |
| Bertrand, 2021 [42] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 180 | Safety of vaccination in breastfeeding women and their breastfed children | More than 85% of 180 breastfeeding women who received an mRNA COVID-19 vaccine reported local or systemic symptoms, with higher frequency following the second dose, but no serious adverse events were noted. Some women reported a temporary reduction in milk supply, but the milk supply returned to normal within 3 days. Moreover, few women reported an increase in milk supply after each dose. |
| Charepe, 2021 [43] | Portugal, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 14 | Serological profile of lactating women compared to nonlactating women, after immunization with the BNT162b2 Pfizer vaccine, in a cohort of healthcare workers, and antibody transfer via breast milk | All women showed immunity after vaccination with positive antibodies for IgM, IgA, and IgG antibodies. The dominant serum antibody response was IgG. Modest levels of antibodies in the breast milk of lactating mothers were observed in this study, especially IgG in 42.9%. |
| Collier, 2021 [39] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 16 | Immunogenicity of the current COVID-19 mRNA vaccines in pregnant and lactating women against both the original SARS-CoV-2 USA-WA1/2020 strain and the B.1.1.7 and B.1.351 variants of concern | Binding, neutralizing, and functional non-neutralizing antibody responses, as well as CD4 and CD8 T-cell responses, were present in pregnant, lactating, and nonpregnant women following vaccination. Binding and neutralizing antibodies were also observed in infant cord blood and breast milk. Binding and neutralizing antibody titers against the SARS-CoV-2 B.1.1.7 and B.1.351 variants of concern were reduced, but T-cell responses were preserved against viral variants. |
| Golan, 2021 [44] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose) | 7 | Detection of vaccine-related mRNA in human milk after vaccination | Vaccine-associated mRNA was not detected in 13 milk samples collected 4 to 48 h after vaccination from 7 breastfeeding individuals. |
| Gray, 2021 [40] | United States, prospective, multi-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 31 | Vaccine-induced immunity in vaccinated pregnant and lactating women | Robust and comparable IgG titers were observed across pregnant, lactating, and nonpregnant controls, all of which were significantly higher than those observed in pregnant women with previous SARS-CoV-2 infection. Boosting resulted in augmented IgG levels in the blood, translating to transfer of IgG to the neonate through the placenta and breast milk. |
| Guida, 2021 [45] | Italy, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 10 | Release of SARS-CoV-2 Spike (S) antibodies in human milk samples obtained by patients vaccinated with the mRNA BNT162b2 vaccine | Seven days after the 2nd dose, anti-SARS-CoV-2 S antibodies were detected in all sera and in all milk samples. The milk antibodies/serum antibodies ratio was on average 2%. |
| Jakuszko, 2021 [46] | Poland, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 32 | Immune response to vaccination against COVID-19 in breastfeeding women and possible benefits for both mother and child | As there were no serious side-effects in the children after the mothers’ vaccinations, and the presence of IgG and IgA antibodies in the breast milk was confirmed, the study gives further evidence on the importance of vaccination against COVID-19 in breastfeeding women. |
| Juncker, 2021 [47] | The Netherlands, prospective, single-center | Pfizer–BioNTech BNT162b2 (at least one dose) | 26 | Levels of specific IgA antibodies in human milk following the first and second dose of BNT162b2 | In human milk, a biphasic response was observed, with SARS-CoV-2 specific IgA starting to increase between days 5 –7 after the first dose and declining after day 15, on average. After the second dose, an accelerated immune reaction was observed. |
| Kelly, 2021 [48] | United States, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 5 | Antibodies in human milk | They characterized longitudinal breast milk levels of anti-spike IgG/A following BNT162b2 vaccination, demonstrating sustained elevation of IgG/IgA levels. However, individual-level data suggest a possible gradual decline in anti-spike IgA in human milk over time after the second dose. |
| Lechosa-Muñiz, 2021 [49] | Spain, prospective, single-center | Pfizer–BioNTech BNT162b2, Moderna mRNA-1273, or Oxford–AstraZeneca ChAdOx1 (2 doses of mRNA vaccines or just 1 dose of vector-based vaccine) | 110 | Presence of IgG and IgA antibodies directed against SARS-CoV-2 protein S in blood from breastfeeding women and to detect the presence of IgA and IgG isotype antibodies directed against SARS-CoV-2 protein S in breast milk | The anti-SARS-CoV-2 vaccines used were well tolerated by mothers and breastfed infants. Breastfeeding must not be interrupted after vaccination. They showed a positive correlation between antibody levels in serum and breast milk samples (lower in who received AstraZeneca). As an added value, breastfeeding mothers offer their infants IgA and IgG isotype antibodies directed against SARS-CoV-2 protein S in breast milk. |
| Low, 2021 [50] | Singapore, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 14 | Production and secretion of spike- and receptor-binding domain (RBD)-specific IgA and IgG into human milk | Lactating mothers secreted specific IgA and IgG antibodies into milk, with the most significant increase at 3–7 days post dose 2. Virus-specific IgG titers were stable out to 4–6 weeks after dose 2. In contrast, SARS-CoV-2-specific IgA levels showed substantial decay. Infants who consumed post-vaccination human milk had no reported adverse effects up to 28 days post ingestion. |
| McLaurin-Jiang, 2021 [51] | United States, cross-sectional survey through social networks | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (at least one dose) | 4455 | Impact on breastfeeding of vaccine-related side-effects following COVID-19 vaccination | Minimal disruption of lactation or adverse impact on the breastfed child, more after the 2nd dose: 94% of women reported no changes in milk production or described an increase |
| Perl, 2021 [52] | Israel, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 84 | Antibodies in human milk and any potential adverse events among women and their infants | Specific IgA and IgG antibodies were found in human milk for 6 weeks after vaccination. IgA secretion was evident as early as 2 weeks after vaccination followed by a spike in IgG after 4 weeks (1 week after the second vaccine). |
| Piano Mortari, 2021 [53] | Italy, prospective, single-center | Pfizer–BioNTech BNT162b2 (2 doses) | 16 | Measurement of memory B cells (MBCs) and antibodies in human milk | Completing the vaccination cycle is necessary to generate high levels of specific serum antibodies and MBCs. Seven days after the second vaccine dose, all lactating mothers had detectable spike-specific IgA in human milk, confirming the ability of vaccine-induced MBCs to be home to the inflammatory environment of the lactating mammary gland and locally produce IgA. |
| Romero Ramírez, 2021 [54] | Spain, prospective, single-center | Pfizer–BioNTech BNT162b2 or Moderna mRNA-1273 (2 doses) | 98 | Antibodies in human milk | BNT162b2 and mRNA-1273 COVID-19 vaccines generate immunity in vaccinated mothers and are associated with vaccine-specific immunoglobulin concentrations in human milk. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Rose, D.U.; Salvatori, G.; Dotta, A.; Auriti, C. SARS-CoV-2 Vaccines during Pregnancy and Breastfeeding: A Systematic Review of Maternal and Neonatal Outcomes. Viruses 2022, 14, 539. https://doi.org/10.3390/v14030539
De Rose DU, Salvatori G, Dotta A, Auriti C. SARS-CoV-2 Vaccines during Pregnancy and Breastfeeding: A Systematic Review of Maternal and Neonatal Outcomes. Viruses. 2022; 14(3):539. https://doi.org/10.3390/v14030539
Chicago/Turabian StyleDe Rose, Domenico Umberto, Guglielmo Salvatori, Andrea Dotta, and Cinzia Auriti. 2022. "SARS-CoV-2 Vaccines during Pregnancy and Breastfeeding: A Systematic Review of Maternal and Neonatal Outcomes" Viruses 14, no. 3: 539. https://doi.org/10.3390/v14030539
APA StyleDe Rose, D. U., Salvatori, G., Dotta, A., & Auriti, C. (2022). SARS-CoV-2 Vaccines during Pregnancy and Breastfeeding: A Systematic Review of Maternal and Neonatal Outcomes. Viruses, 14(3), 539. https://doi.org/10.3390/v14030539