
Severity of COVID-19 among Hospitalized Patients: Omicron Remains a Severe Threat for Immunocompromised Hosts
 , , , , , , , , , ,
, , , , , , , , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Demographics
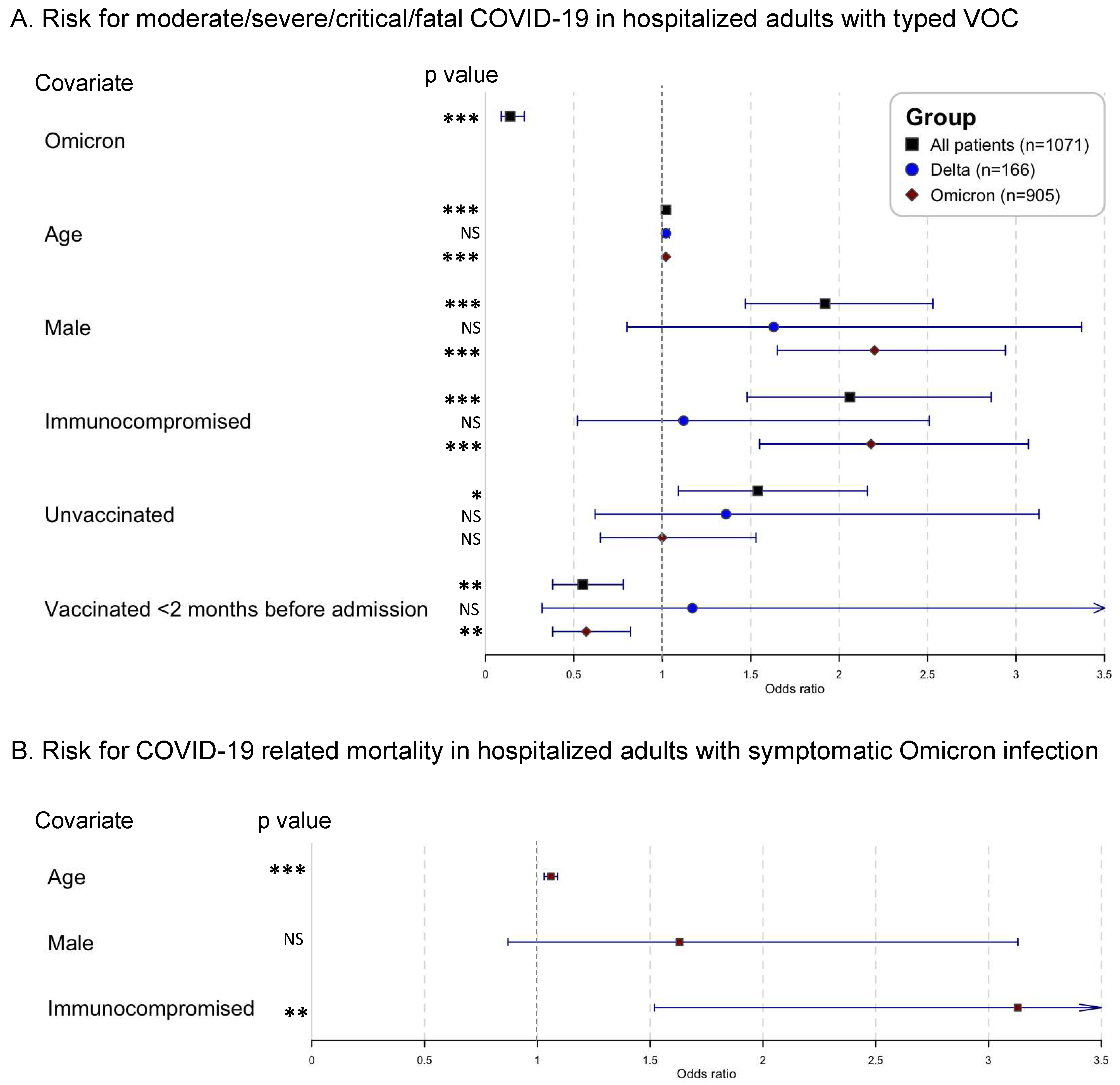
3.2. Hospitalized Adults Infected with Omicron Showed a Reduced Intrinsic COVID-19 Severity Compared to Those Infected with Delta
3.3. Immunocompromised Adults HOSPITALIZED with Omicron Infections Had an Increased Risk of Severe COVID-19 Outcomes
3.4. Neither Vaccination Status Nor Immune Status Determine Total Hospital Length-of-Stay in Omicron-Infected Adults
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, S.; Thambiraja, T.S.; Karuppanan, K.; Subramaniam, G. Omicron and Delta variant of SARS-CoV-2: A comparative computational study of spike protein. J. Med. Virol. 2021, 94, 1641–1649. [Google Scholar] [CrossRef]
- Viana, R.; Moyo, S.; Amoako, D.G.; Tegally, H.; Scheepers, C.; Althaus, C.L.; Anyaneji, U.J.; Bester, P.A.; Boni, M.F.; Chand, M.; et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature 2022, 603, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Gavrilov, D.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; et al. ‘Coronavirus Pandemic (COVID-19)’—Published Online at OurWorldInData.org. Available online: https://ourworldindata.org/coronavirus (accessed on 1 June 2022).
- Tegally, H.; Moir, M.; Everatt, J.; Giovanetti, M.; Scheepers, C.; Wilkinson, E.; Subramoney, K.; Makatini, Z.; Moyo, S.; Amoako, D.G.; et al. Emergence of SARS-CoV-2 Omicron lineages BA.4 and BA.5 in South Africa. Nat. Med. 2022, 28, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Snell, L.B.; Wang, W.; Alcolea-Medina, A.; Charalampous, T.; Batra, R.; de Jongh, L.; Higgins, F.; Nebbia, G.; Wang, Y.; Edgeworth, J.; et al. Descriptive comparison of admission characteristics between pandemic waves and multivariable analysis of the association of the Alpha variant (B.1.1.7 lineage) of SARS-CoV-2 with disease severity in inner London. BMJ Open 2022, 12, e055474. [Google Scholar] [CrossRef]
- Davies, N.G.; Jarvis, C.I.; Edmunds, W.J.; Jewell, N.P.; Diaz-Ordaz, K.; Keogh, R.H. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature 2021, 593, 270–274. [Google Scholar] [CrossRef]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef]
- Bhattacharyya, R.P.; Hanage, W.P. Challenges in Inferring Intrinsic Severity of the SARS-CoV-2 Omicron Variant. N. Engl. J. Med. 2022, 386, e14. [Google Scholar] [CrossRef]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; de Villiers, T.; Van der Walt, Z.; et al. Decreased severity of disease during the first global omicron variant covid-19 outbreak in a large hospital in tshwane, south africa. Int. J. Infect. Dis. 2021, 116, 38–42. [Google Scholar] [CrossRef]
- Jassat, W.; Karim, S.S.A.; Mudara, C.; Welch, R.; Ozougwu, L.; Groome, M.J.; Govender, N.; von Gottberg, A.; Wolter, N.; Wolmarans, M.; et al. Clinical severity of COVID-19 in patients admitted to hospital during the omicron wave in South Africa: A retrospective observational study. Lancet Glob. Health 2022, 10, e961–e969. [Google Scholar] [CrossRef]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and Covid-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.-A.; Kassanjee, R.; Rousseau, P.; Morden, E.; Johnson, L.; Solomon, W.; Hsiao, N.-Y.; Hussey, H.; Meintjes, G.; Paleker, M.; et al. Outcomes of laboratory-confirmed SARS-CoV-2 infection in the Omicron-driven fourth wave compared with previous waves in the Western Cape Province, South Africa. Trop. Med. Int. Health 2022, 27, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Veneti, L.; Bøås, H.; Kristoffersen, A.B.; Stålcrantz, J.; Bragstad, K.; Hungnes, O.; Storm, M.L.; Aasand, N.; Rø, G.; Starrfelt, J.; et al. Reduced risk of hospitalisation among reported COVID-19 cases infected with the SARS-CoV-2 Omicron BA.1 variant compared with the Delta variant, Norway, December 2021 to January 2022. Eurosurveillance 2022, 27, 2200077. [Google Scholar] [CrossRef] [PubMed]
- Dinh, A.; Dahmane, L.; Dahoumane, M.; Masingue, X.; Jourdain, P.; Lescure, F.-X. Impact of Omicron surge in community setting in greater Paris area. Clin. Microbiol. Infect. 2022, 28, 897–899. [Google Scholar] [CrossRef]
- Ferguson, N.; Ghani, A.; Hinsley, W.; Volz, E. Report 50: Hospitalisation Risk for Omicron Cases in England; Imperial College London: London, UK, 2021. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA-J. Am. Med. Assoc. 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Christensen, P.A.; Olsen, R.J.; Long, S.W.; Snehal, R.; Davis, J.J.; Saavedra, M.O.; Reppond, K.; Shyer, M.N.; Cambric, J.; Gadd, R.; et al. Signals of Significantly Increased Vaccine Breakthrough, Decreased Hospitalization Rates, and Less Severe Disease in Patients with Coronavirus Disease 2019 Caused by the Omicron Variant of Severe Acute Respiratory Syndrome Coronavirus 2 in Houston, Texas. Am. J. Pathol. 2022, 192, 642–652. [Google Scholar] [CrossRef]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA-J. Am. Med. Assoc. 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Hong, V.X.; Patel, M.M.; Kahn, R.; Lipsitch, M.; Tartof, S.Y. Clinical Outcomes among Patients Infected with Omicron (B.1.1.529) SARS-CoV-2 Variant in Southern California. MedRxiv 2022. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. COVID-19—Risk Factors and Risk Groups. 2022. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/risk-factors-risk-groups (accessed on 6 August 2022).
- Vaesen, J. Covid Vaccinaties België. 2021. Available online: https://covid-vaccinatie.be/nl (accessed on 6 August 2022).
- Cuypers, L.; Baele, G.; Dellicour, S.; Maes, P.; André, E. Genomic Surveillance of SARS-CoV-2 in Belgium; UZ Leuven: Leuven, Belgium, 2022. [Google Scholar]
- NIH. Clinical Spectrum of SARS-CoV-2 Infection. 2020. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 28 January 2021).
- CDC. COVID-19 Vaccines for Moderately or Severely Immunocompromised People. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html (accessed on 9 February 2022).
- Rstudio Team. RStudio: Integrated Development for R. 2020. Available online: https://www.rstudio.com/ (accessed on 9 February 2022).
- Bager, P.; Wohlfahrt, J.; Bhatt, S.; Stegger, M.; Legarth, R.; Møller, C.H.; Skov, R.L.; Valentiner-Branth, P.; Voldstedlund, M.; Fischer, T.K.; et al. Risk of hospitalisation associated with infection with SARS-CoV-2 omicron variant versus delta variant in Denmark: An observational cohort study. Lancet Infect. Dis. 2022, 22, 967–976. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Van Goethem, N.; Chung, P.Y.J.; Meurisse, M.; Vandromme, M.; De Mot, L.; Brondeel, R.; Stouten, V.; Klamer, S.; Cuypers, L.; Braeye, T.; et al. Clinical Severity of SARS-CoV-2 Omicron Variant Compared with Delta among Hospitalized COVID-19 Patients in Belgium during Autumn and Winter Season 2021–2022. Viruses 2022, 14, 1297. [Google Scholar] [CrossRef] [PubMed]
- Malahe, S.R.K.; Hoek, R.A.S.; Dalm, V.A.S.H.; Broers, A.E.C.; Hoed, C.M.D.; Manintveld, O.C.; Baan, C.C.; van Deuzen, C.M.; Papageorgiou, G.; Bax, H.I.; et al. Clinical Characteristics and Outcomes of Immunocompromised Patients With Coronavirus Disease 2019 Caused by the Omicron Variant: A Prospective, Observational Study. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Han, J.; Zhang, Y.; He, J.; Yu, W.; Zhang, X.; Wu, J.; Zhang, S.; Kong, Y.; Guo, Y.; et al. SARS-CoV-2 Omicron Variant: Epidemiological Features, Biological Characteristics, and Clinical Significance. Front. Immunol. 2022, 13, 877101. [Google Scholar] [CrossRef]
- Focosi, D.; McConnell, S.; Casadevall, A.; Cappello, E.; Valdiserra, G.; Tuccori, M. Monoclonal antibody therapies against SARS-CoV-2. Lancet Infect. Dis. 2022, 22, e311–e326. [Google Scholar] [CrossRef]
- Van Goethem, N.; Vilain, A.; Wyndham-Thomas, C.; Deblonde, J.; Bossuyt, N.; Lernout, T.; Gonzalez, J.R.; Quoilin, S.; Melis, V.; Van Beckhoven, D. Rapid establishment of a national surveillance of COVID-19 hospitalizations in Belgium. Arch. Public Health 2020, 78, 121. [Google Scholar] [CrossRef]
- Pulliam, J.R.C.; van Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022, 376, eabn4947. [Google Scholar] [CrossRef]
- Al Hajji, Y.; Taylor, H.; Starkey, T.; Lee, L.Y.W.; Tilby, M. Antibody response to a third booster dose of SARS-CoV-2 vaccination in adults with haematological and solid cancer: A systematic review. Br. J. Cancer 2022, 127, 1827–1836. [Google Scholar] [CrossRef]
- CDC Health Alert Network. MIS-C associated with COVID-19. Available online: https://emergency.cdc.gov/han/2020/han00432.asp (accessed on 10 February 2022).
- Sullivan, K.E.; Jyonouchi, S.C. Inborn errors of immunity (primary immunodeficiencies): Classification. Available online: https://www.uptodate.com/contents/inborn-errors-of-immunity-primary-immunodeficiencies- (accessed on 15 December 2021).
- Shroff, A.; Mertz, D. Infectious Diseases Risk Whole in Chronic, High-Dose Corticosteroids. Can. J. Gen. Internal Med. 2017, 12, 10–13. [Google Scholar] [CrossRef]

{kind=link}
| Crude OR | 95% CI | p value | Adjusted OR | 95% CI | p Value | |
|---|---|---|---|---|---|---|
| Outcome 1—disease severity: odds of moderate/severe/critical/fatal COVID-19 (n = 449/1071, 41.9%) | ||||||
| Omicron 1 | 0.17 | 0.11–0.26 | <0.001 | 0.14 | 0.09–0.22 | <0.001 |
| Age at admission 2 | 1.01 | 1.01–1.02 | <0.001 | 1.02 | 1.01–1.03 | <0.001 |
| Male 3 | 2.07 | 1.60–2.67 | <0.001 | 1.92 | 1.47–2.53 | <0.001 |
| Immunocompromised 4 | 2.12 | 1.57–2.88 | <0.001 | 2.06 | 1.48–2.86 | <0.001 |
| Unvaccinated 5 | 1.54 | 1.09–2.16 | 0.01 | - | - | - |
| Vaccinated <2 months before admission 6 | 0.55 | 0.38–0.78 | 0.001 | - | - | - |
| Boosted 7 | 0.82 | 0.64–1.07 | 0.14 | - | - | - |
| Viral vector vaccination 8 | 1.35 | 0.99–1.85 | 0.06 | - | - | - |
| Outcome 2—ICU admission: admission or transferred to ICU due to COVID-19 (n = 112/1071, 10.5%) | ||||||
| Omicron 1 | 0.22 | 0.14–0.34 | <0.001 | 0.26 | 0.17–0.40 | <0.001 |
| Age at admission 2 | 0.99 | 0.98–1.00 | 0.01 | 0.99 | 0.98–1.00 | 0.02 |
| Male 3 | 1.97 | 1.32–2.98 | 0.001 | 1.99 | 1.31–3.05 | 0.001 |
| Immunocompromised 4 | 2.59 | 1.68–3.89 | <0.01 | 2.34 | 1.50–3.56 | <0.001 |
| Unvaccinated 5 | 1.80 | 1.10–2.87 | 0.02 | - | - | - |
| Vaccinated <2 months before admission 6 | 0.75 | 0.38–1.36 | 0.36 | - | - | - |
| Outcome 3—mortality: odds of in-hospital mortality related to COVID-19 (n = 89/1071, 8.3%) | ||||||
| Omicron 1 | 0.30 | 0.19–0.48 | <0.001 | 0.24 | 0.14–0.40 | <0.001 |
| Age at admission 2 | 1.03 | 1.02–1.04 | <0.001 | 1.05 | 1.03–1.07 | <0.001 |
| Male 3 | 2.02 | 1.30–3.20 | 0.002 | 1.85 | 1.16–2.99 | 0.01 |
| Immunocompromised 4 | 2.80 | 1.75–4.47 | <0.001 | 3.02 | 1.82–5.05 | <0.001 |
| Unvaccinated 5 | 1.15 | 0.56–2.19 | 0.68 | - | - | - |
| Vaccinated <2 months before admission 6 | 0.51 | 0.15–1.34 | 0.22 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nevejan, L.; Ombelet, S.; Laenen, L.; Keyaerts, E.; Demuyser, T.; Seyler, L.; Soetens, O.; Van Nedervelde, E.; Naesens, R.; Geysels, D.; et al. Severity of COVID-19 among Hospitalized Patients: Omicron Remains a Severe Threat for Immunocompromised Hosts. Viruses 2022, 14, 2736. https://doi.org/10.3390/v14122736
Nevejan L, Ombelet S, Laenen L, Keyaerts E, Demuyser T, Seyler L, Soetens O, Van Nedervelde E, Naesens R, Geysels D, et al. Severity of COVID-19 among Hospitalized Patients: Omicron Remains a Severe Threat for Immunocompromised Hosts. Viruses. 2022; 14(12):2736. https://doi.org/10.3390/v14122736
Chicago/Turabian StyleNevejan, Louis, Sien Ombelet, Lies Laenen, Els Keyaerts, Thomas Demuyser, Lucie Seyler, Oriane Soetens, Els Van Nedervelde, Reinout Naesens, Dieter Geysels, and et al. 2022. "Severity of COVID-19 among Hospitalized Patients: Omicron Remains a Severe Threat for Immunocompromised Hosts" Viruses 14, no. 12: 2736. https://doi.org/10.3390/v14122736
APA StyleNevejan, L., Ombelet, S., Laenen, L., Keyaerts, E., Demuyser, T., Seyler, L., Soetens, O., Van Nedervelde, E., Naesens, R., Geysels, D., Verstrepen, W., Cattoir, L., Martens, S., Michel, C., Mathieu, E., Reynders, M., Evenepoel, A., Hellemans, J., Vanhee, M., ... André, E. (2022). Severity of COVID-19 among Hospitalized Patients: Omicron Remains a Severe Threat for Immunocompromised Hosts. Viruses, 14(12), 2736. https://doi.org/10.3390/v14122736