
Primary SARS-CoV-2 Infections, Re-infections and Vaccine Effectiveness during the Omicron Transmission Period in Healthcare Workers of Trieste and Gorizia (Northeast Italy), 1 December 2021–31 May 2022

 ,
,  on behalf of ORCHESTRA working group
on behalf of ORCHESTRA working group
Abstract
:1. Background
2. Aims
3. Methods
3.1. Ethical Considerations
3.2. Study Population
3.3. Data Collection
3.4. Study Endpoints
3.5. Statistical Analysis
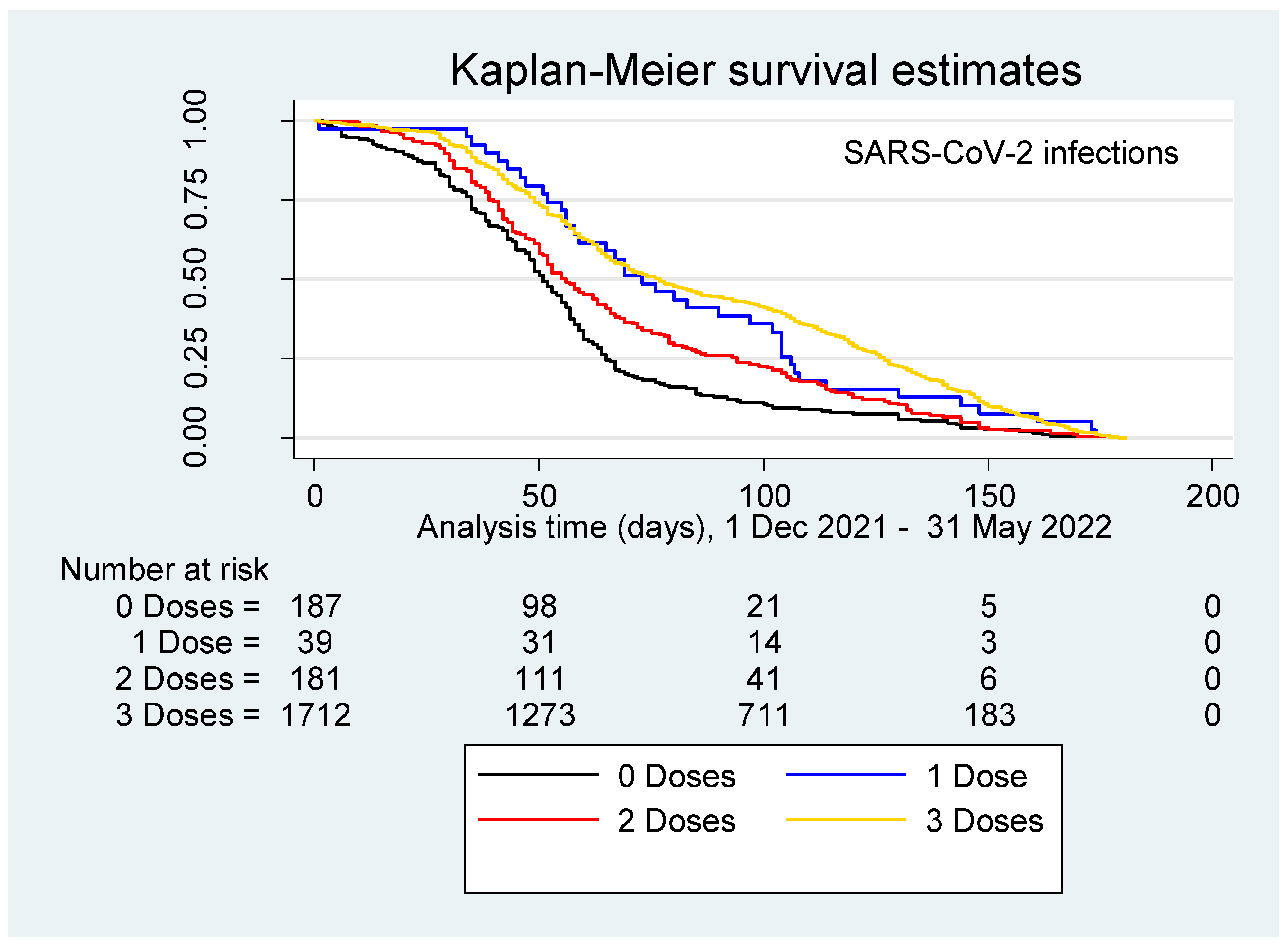
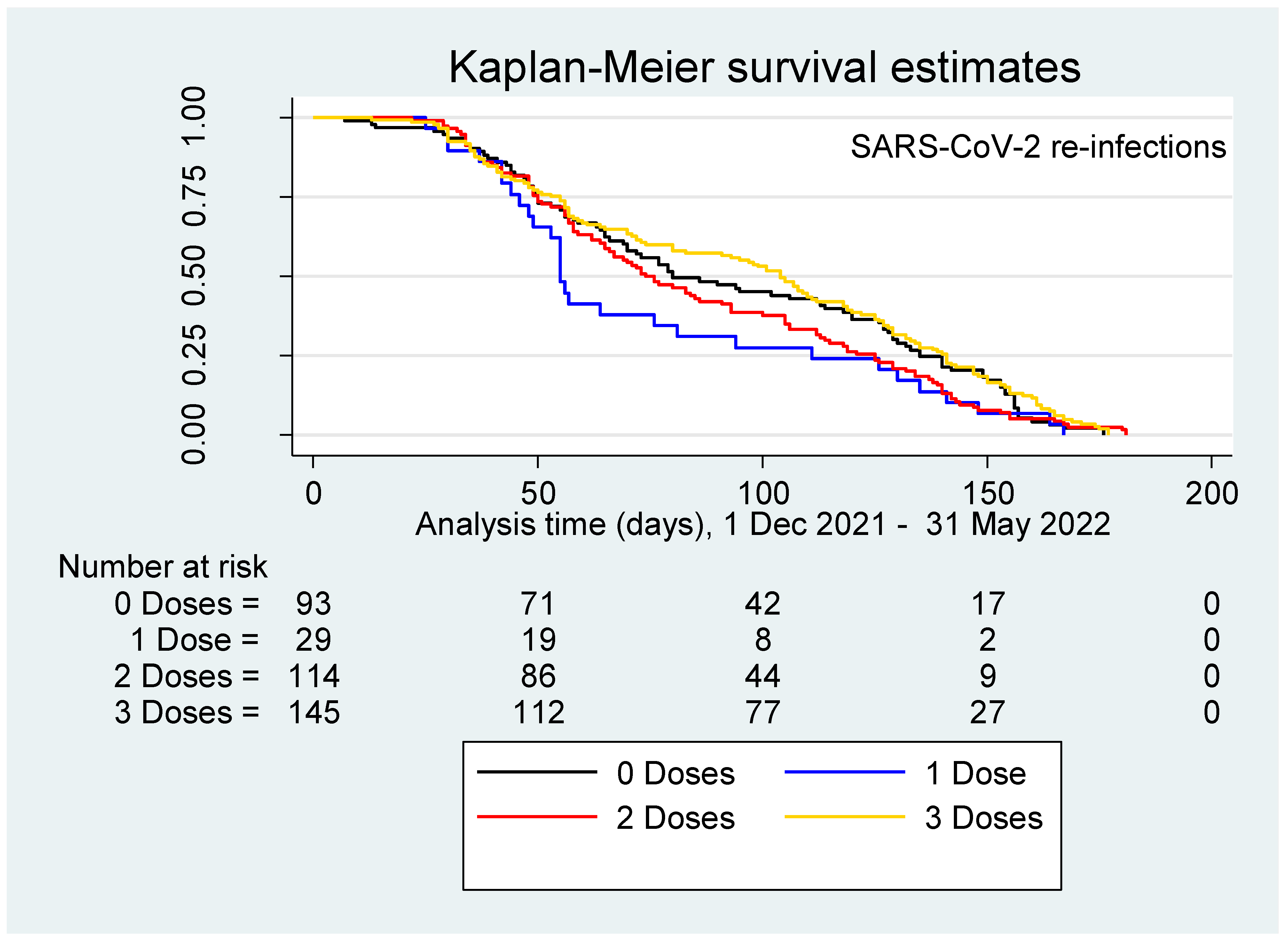
4. Results
- • 14.2 × 1000 p-d among unvaccinated HCWs;
- • 6.2 × 1000 p-d among HCWs immunized with only one dose;
- • 12.5 × 1000 p-d in those vaccinated with 2 doses;
- • 9.1 × 1000 p-d with 3 doses.
- • 12.2 × 1000 p-d among unvaccinated;
- • 11.4 × 1000 p-d in HCWs immunized with one dose;
- • 8.0 × 1000 p-d in HCWs immunized with two doses;
- • 7.5 × 1000 p-d in HCWs immunized with three doses.
- • 3.2 × 1000 p-d among unvaccinated,
- • 0 × 1000 p-d in HCWs vaccinated with one dose,
- • 0.6 × 1000 p-d in HCWs immunized with two doses, and
- • 0.2 × 1000 p-d in HCWs vaccinated with three doses.
5. Discussion
5.1. Main Findings
5.2. Interpretation of Findings
5.3. Generalizability
5.4. Recurrent Infections
5.5. Strengths and Weaknesses
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Islam, M.R.; Hoque, M.N.; Rahman, M.S.; Alam, A.S.M.; Akther, M.; Puspo, J.A.; Akter, S.; Sultana, M.; Crandall, K.A.; Hossain, M.A. Genome-wide analysis of SARS-CoV-2 virus strains circulating worldwide implicates heterogeneity. Sci. Rep. 2020, 10, 14004. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L.; Ronchese, F.; Ricci, F.; Negro, C.; Laese-Filon, F. SARS-CoV-2 Infection in Health Care Workers of Trieste (North-Eastern Italy), 1 October 2020–7 February 2022: Occupational Risk and the Impact of the Omicron Variant. Viruses 2022, 14, 1663. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Wang, W.; Ma, J.; Wu, S.; Sun, F. Reinfection rates among patients previously infected by SARS-CoV-2: Systematic review and meta-analysis. Chin. Med. J. 2022, 135, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Galanti, M.; Shaman, J. Direct observation of repeated infections with endemic coronaviruses. J. Infect. Dis 2021, 223, 409–415. [Google Scholar] [CrossRef]
- Cegolon, L.; Pichierri, J.; Mastrangelo, G.; Cinquetti, S.; Sotgiu, G.; Bellizzi, S.; Pichierri, G. Hypothesis to explain the severe form of COVID-19 in Northern Italy. BMJ Glob. Health 2020, 5, e002564. [Google Scholar] [CrossRef]
- Yang, S.L.; Teha, H.S.; Lian, J.; Suah, J.L.; Husin, M.; Hwong, W.Y. SARS-CoV-2 in Malaysia: A surge of reinfection during the predominantly Omicron period. Lancet Reg. Health West. Pac. 2022, 26, 100572. [Google Scholar] [CrossRef]
- Tillett, R.L.; Sevinsky, J.R.; Hartley, P.D.; Kerwin, H.; Crawford, N.; Gorzalski, A.; Laverdure, C.; Verma, S.C.; Rossetto, C.C.; Jackson, D.; et al. Genomic evidence for reinfection with SARS-CoV-2: A case study. Lancet Infect. Dis. 2021, 21, 52–58. [Google Scholar] [CrossRef]
- Wang, J.; Kaperak, C.; Sato, T.; Sakuraba, A. COVID-19 reinfection: A rapid systematic review of case reports and case series. J. Investig. Med. 2021, 69, 1253–1255. [Google Scholar] [CrossRef]
- Piapan, L.; De Michieli, P.; Ronchese, F.; Rui, F.; Peresson, M.; Segat, L.; D’Agaro, P.; Negro, C.; Bovenzi, M.; Larese Filon, F. COVID-19 outbreaks in hospital workers during the first COVID-19 wave. Occup. Med. 2022, 72, 110–117. [Google Scholar] [CrossRef]
- Piapan, L.; De Michieli, P.; Ronchese, F.; Rui, F.; Mauro, M.; Peresson, M.; Segat, L.; D’Agaro, P.; Negro, C.; Bovenzi, M.; et al. COVID-19 outbreak in healthcare workers in hospitals in Trieste, North-east Italy. J. Hosp. Infect. 2020, 106, 626–628. [Google Scholar] [CrossRef]
- Basso, P.; Negro, C.; Cegolon, L.; Larese Filon, F. Risk of Vaccine Breakthrough SARS-CoV-2 Infection and Associated Factors in Healthcare Workers of Trieste Teaching Hospitals (North-Eastern Italy). Viruses 2022, 14, 336. [Google Scholar] [CrossRef] [PubMed]
- Larese Filon, F.; Rui, F.; Ronchese, F.; De Michieli, P.; Negro, C. Incidence of COVID-19 infection in hospital workers from March 1, 2020 to May 31, 2021 routinely tested, before and after vaccination with BNT162B2. Sci. Rep. 2022, 12, 2533. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 vaccine booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Yelin, D.; Eckerle, I.; Eberhardt, C.S.; Wang, J.; Cao, B.; Kaiser, L. Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin. Microbiol. Infect. 2021, 27, 315–331. [Google Scholar] [CrossRef]
- Center for Disease Prevention and Control. Overview of Testing for SARS-CoV-2, the Virus that Causes COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html (accessed on 25 November 2022).
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef]
- Sheward, D.J.; Kim, C.; Ehling, R.A.; Pankow, A.; Dopico, X.C.; Dyrdak, R.; Martin, D.P.; Reddy, S.T.; Dillner, J.; Hedestam, G.B.K.; et al. Neutralisation sensitivity of the SARS-CoV-2 omicron (B.1.1.529) variant: A cross-sectional study. Lancet Infect. Dis. 2022, 22, 813–820. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination with BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections Among Health Care Workers. JAMA 2021, 325, 2457–2465. [Google Scholar] [CrossRef]
- Canaday, D.H.; Oyebanji, O.A.; White, E.; Keresztesy, D.; Payne, M.; Wilk, D.; Carias, L.; Aung, H.; Denis, K.S.; Sheehan, M.L.; et al. COVID-19 vaccine booster dose needed to achieve Omicron-specific neutralisation in nursing home residents. eBioMedicine 2022, 80, 104066. [Google Scholar] [CrossRef]
- Malhotra, S.; Mani, K.; Lodha, R. COVID-19 infection, and reinfection, and vaccine effectiveness against symptomatic infection among health care workers in the setting of omicron variant transmission in New Delhi, India. Lancet Reg. Health Southeast Asia 2022, 3, 100023. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N. Engl. J. Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L.; Mastrangelo, G.; Emanuelli, E.; Camerotto, R.; Spinato, G.; Frezza, D. Early Negativization of SARS-CoV-2 Infection by Nasal Spra of Seawater plus Additives: The RENAISSANCE Open-Label Controlled Clinical Trial. Pharmaceuticals 2022, 14, 2502. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L.; Mirandola, M.; Salaris, C.; Salvati, M.V.; Mastrangelo, G.; Salata, C. Hypothiocyanite and Hypothiocyanite/Lactoferrin Mixture Exhibit Virucidal Activity In Vitro against SARS-CoV-2. Pathogens 2021, 10, 233. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L. Investigating hypothiocyanite against SARS-CoV-2. Int. J. Hyg. Environ Health 2020, 227, 113520. [Google Scholar] [CrossRef] [PubMed]
- Cegolon, L.; Javanbakht, M.; Mastrangelo, G. Nasal disinfection for the prevention and control of COVID-19: A scoping review on potential chemo-preventive agents. Int. J. Hyg. Environ. Health 2020, 230, 113605. [Google Scholar] [CrossRef]
- Cegolon, L.; Salata, C.; Piccoli, E.; Juarez, V.; Palu, G.; Mastrangelo, G.; Calistri, A. In vitro antiviral activity of hypothiocyanite against A/H1N1/2009 pandemic influenza virus. Int. J. Hyg. Environ. Health 2014, 217, 17–22. [Google Scholar] [CrossRef]
- Rovida, F.; Esposito, G.L.; Rissone, M.; Novelli, V.; Cutti, S.; Muzzi, A.; Rona, C.; Bertoli, E.; Daglio, M.; Piralla, A.; et al. Characteristics and outcomes of vaccinated and nonvaccinated patients hospitalized in a single Italian hub for COVID-19 during the Delta and Omicron waves in Northern Italy. Int. J. Infect. Dis. 2022, 122, 420–426. [Google Scholar] [CrossRef]
- Robilotti, E.V.; Whiting, K.; Lucca, A.; Poon, C.; Jani, K.; McMillen, T.; Freeswick, S.; Korenstein, D.; Babady, N.E.; Seshan, V.E.; et al. Effectiveness of mRNA booster vaccine among health Care workers in New York City during the omicron surge, December 2021–January 2022. Clin. Microbiol. Infect. 2022, 28, 1624–1628. [Google Scholar] [CrossRef]
- Ochoa-Hein, E.; ELeal-Morán, P.; Nava-Guzmán, K.A. Significant Rise in SARS-CoV-2 Reinfection Rate in Vaccinated Hospital Workers during the Omicron Wave: A Prospective Cohort Study. Rev. Investig. Clin. 2022, 74, 175–180. [Google Scholar] [CrossRef]
- Hammerman, A.; Sergienko, R.; Friger, M.; Beckenstein, T.; Peretz, A.; Netzer, D.; Yaron, S.; Arbel, R. Effectiveness of the BNT162b2 vaccine after recovery from COVID-19. N. Engl. J. Med. 2022, 386, 1221–1229. [Google Scholar] [CrossRef]
- Malhotra, S.; Mani, K.; Lodha, R.; Bakhshi, S.; Mathur, V.P.; Gupta, P.; Kedia, S.; Sankar, J.; Kumar, P.; Kumar, A.; et al. SARS-CoV-2 reinfection rate and estimated effectiveness of the inactivated whole virion vaccine BBV152 against reinfection among health care workers in New Delhi, India. JAMA Netw. Open 2022, 5, e2142210. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FACTOR | STRATA | NUMBER | Col % |
|---|---|---|---|
| Sex | Female | 5308 | 68.7 |
| Male | 2415 | 31.3 | |
| Age (years) | Mean ± SD | 46.6 ± 12.0 | |
| Median (IQR) | 48.6 (36.2; 56.7) | ||
| <41 | 2468 | 32.0 | |
| 41–50 | 1751 | 22.7 | |
| 51–60 | 2453 | 31.8 | |
| 61+ | 1051 | 13.6 | |
| ASUGI Site | Gorizia-Monfalcone | 2589 | 33.5 |
| Trieste | 5134 | 66.5 | |
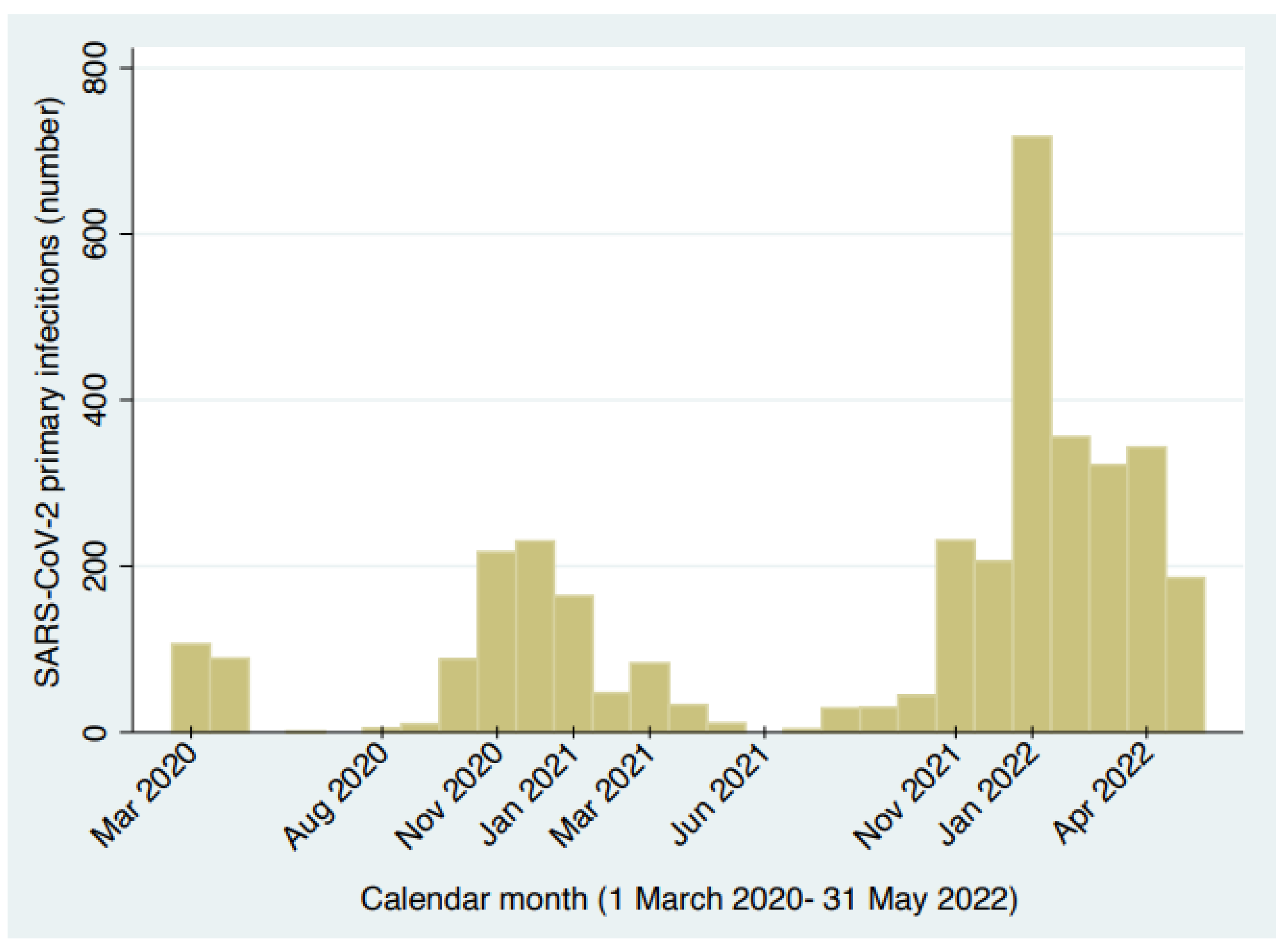
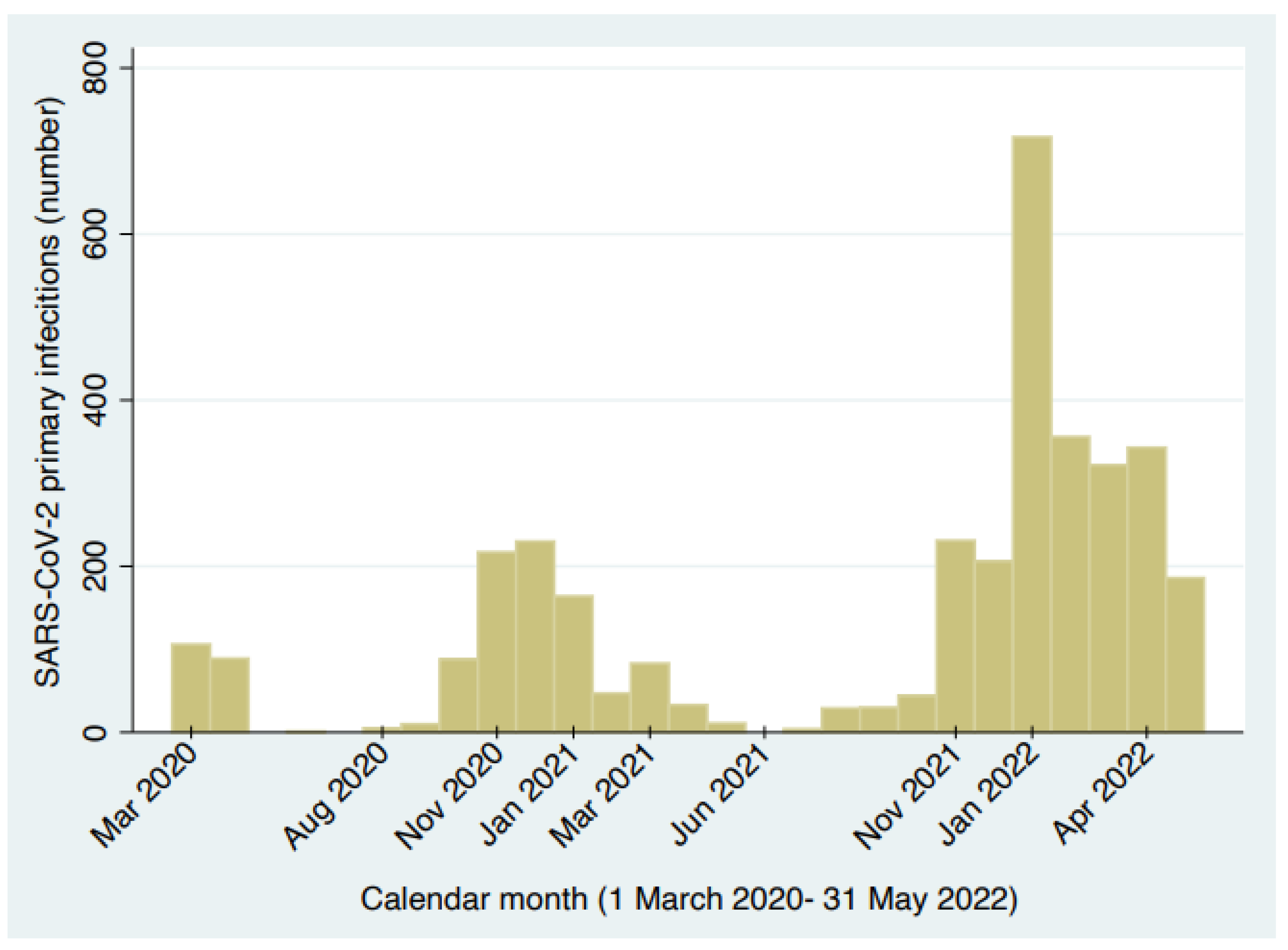
| Incident SARS-CoV-2 infections (Total = 3541) | TOTAL (1 Mar 2020–31 May 2022) | 3571 | 100 |
| I (1 Mar 2020–31 May 2020) | 214 | 6.0 | |
| II (1 Jun 2020–30 Sep 2020) | 16 | 0.5 | |
| III (1 Oct 2020–31 Dec 2020) | 535 | 15.0 | |
| IVa (1 Jan 2021–31 Mar 2021) | 294 | 8.2 | |
| IVb (1 Apr 2021–30 Sep 2021) | 107 | 3.0 | |
| V (1 Oct 2021–30 Nov 2021) | 275 | 7.7 | |
| VI (1 Dec 2021–31 May 2022) | 2130 | 59.7 | |
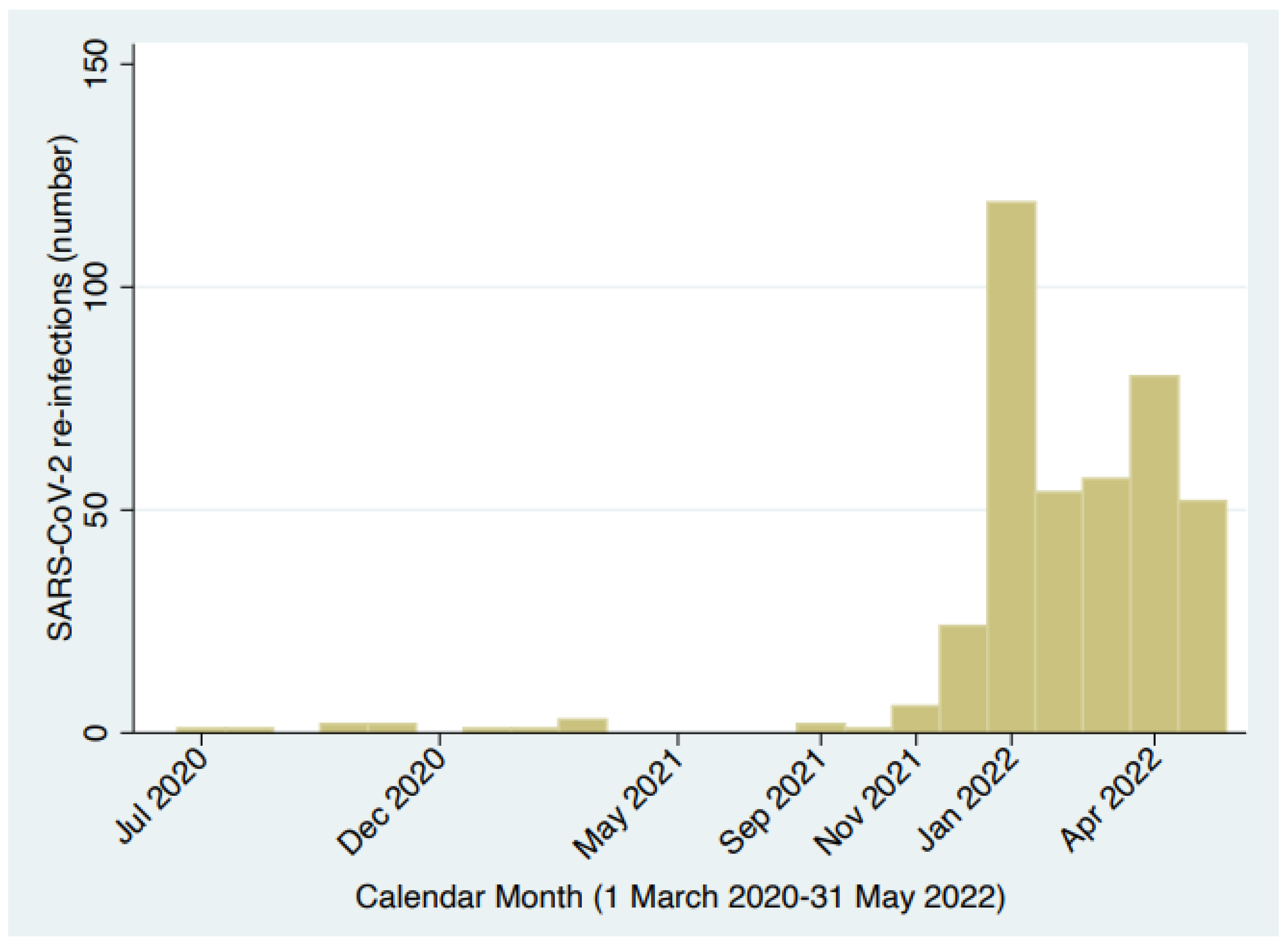
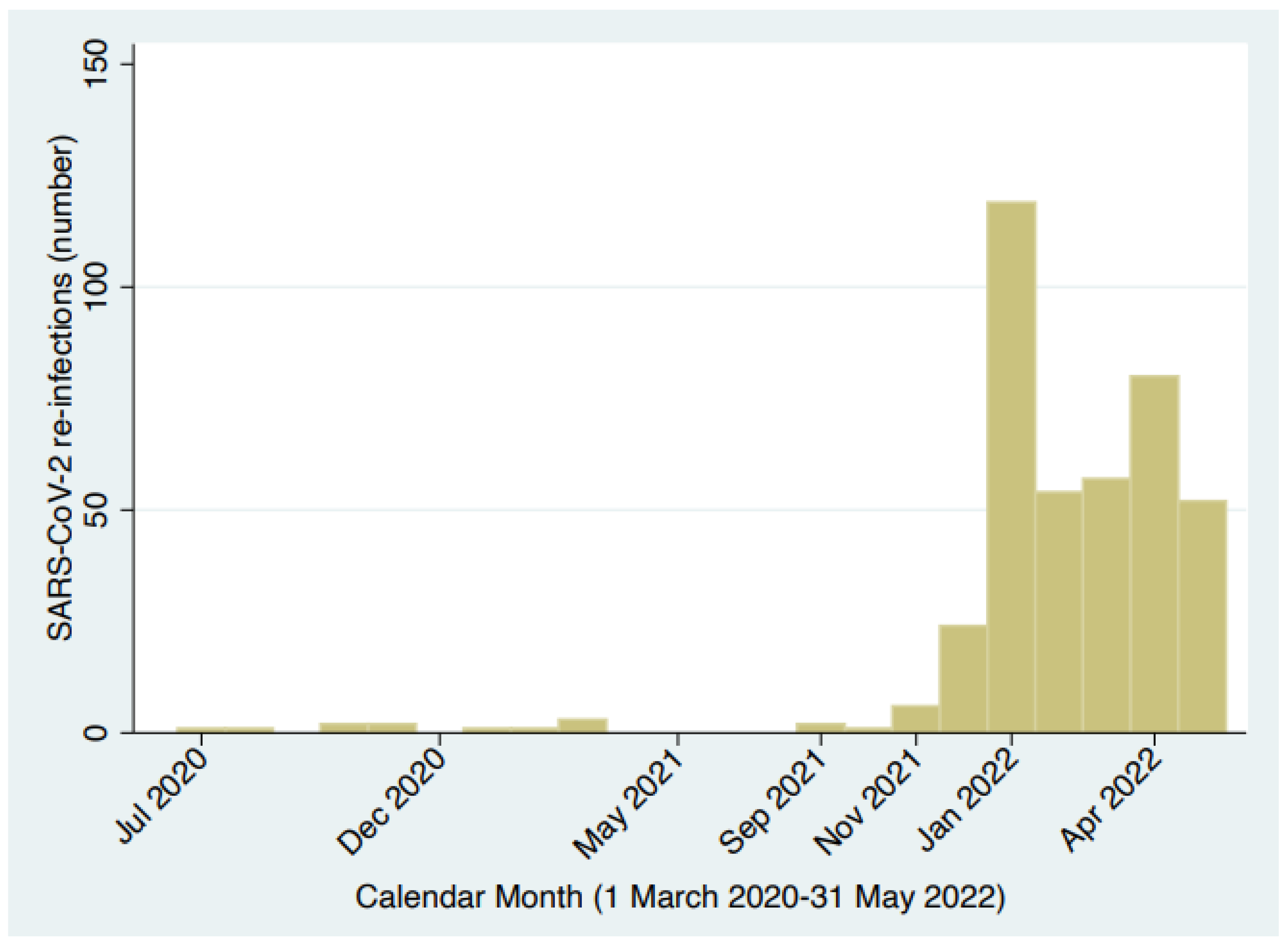
| SARS-CoV-2 re-infections (Tot = 406) | TOTAL (1 Mar 2020–31 May 2022) | 406 | 100 |
| I (1 Mar 2020–31 May 2020) | 0 | 0 | |
| II (1 Jun 2020–30 Sep 2020) | 2 | 0.5 | |
| III (1 Oct 2020–31 Dec 2020) | 4 | 1.0 | |
| IVa (1 Jan 2021–31 Mar 2021) | 2 | 0.5 | |
| IVb (1 Apr 2021–30 Sep 2021) | 5 | 1.2 | |
| V (1 Oct 2021–30 Nov 2021) | 7 | 1.7 | |
| VI (1 Dec 2021–31 May 2022) | 386 | 95.1 | |
| Number of swab tests (1 December 2021– 31 May 2022) | 0 | 602 | 7.8 |
| 1–3 | 754 | 10.6 | |
| 4–6 | 1189 | 16.7 | |
| 7–10 | 1759 | 24.7 | |
| 11+ | 3419 | 48.0 | |
| Number of doses of COVID-19 Vaccine (by 31 May 2022) | TOTAL | 7723 | 100 |
| 0 | 608 | 7.9 | |
| 1 | 186 | 2.4 | |
| 2 | 868 | 11.2 | |
| 3 | 6047 | 78.3 | |
| 4 | 14 | 0.2 | |
| Vaccine type | Comirnaty (Pfitzer/BioNTech) | 7388 | 95.7 |
| Spikevax (Moderna) | 306 | 4.0 | |
| Vaxzevria (Oxford-Astra Zeneca; N = 21) | 29 | 0.4 | |
| Janssen (Johnson & Johnson; N = 7) | |||
| Nuvaxovid (Novavax; N = 1) | |||
| Job task | TOTAL | 7723 | 100 |
| Administrative | 628 | 8.1 | |
| Doctor | 1567 | 20.3 | |
| Nurses | 2733 | 35.4 | |
| Other HCWs | 1642 | 21.3 | |
| Technician | 1153 | 14.9 | |
| Educational level (Missing: 1880) | TOTAL | 5843 | 100 |
| Junior secondary | 2733 | 46.8 | |
| Secondary | 380 | 6.5 | |
| Bachelor’s degree | 1085 | 18.6 | |
| Postgraduate diploma | 1645 | 28.2 | |
| Workplace | TOTAL | 7723 | 100 |
| Administrative services | 935 | 12.1 | |
| Community services | 2339 | 30.3 | |
| Radiology services (technician) | 562 | 7.3 | |
| Surgical ward | 1167 | 15.1 | |
| Medical and geriatric ward | 1449 | 18.8 | |
| COVID-19 area | 245 | 3.2 | |
| Accident and emergency (A&E) | 757 | 9.8 | |
| Non-clinical workers and other | 269 | 3.5 |
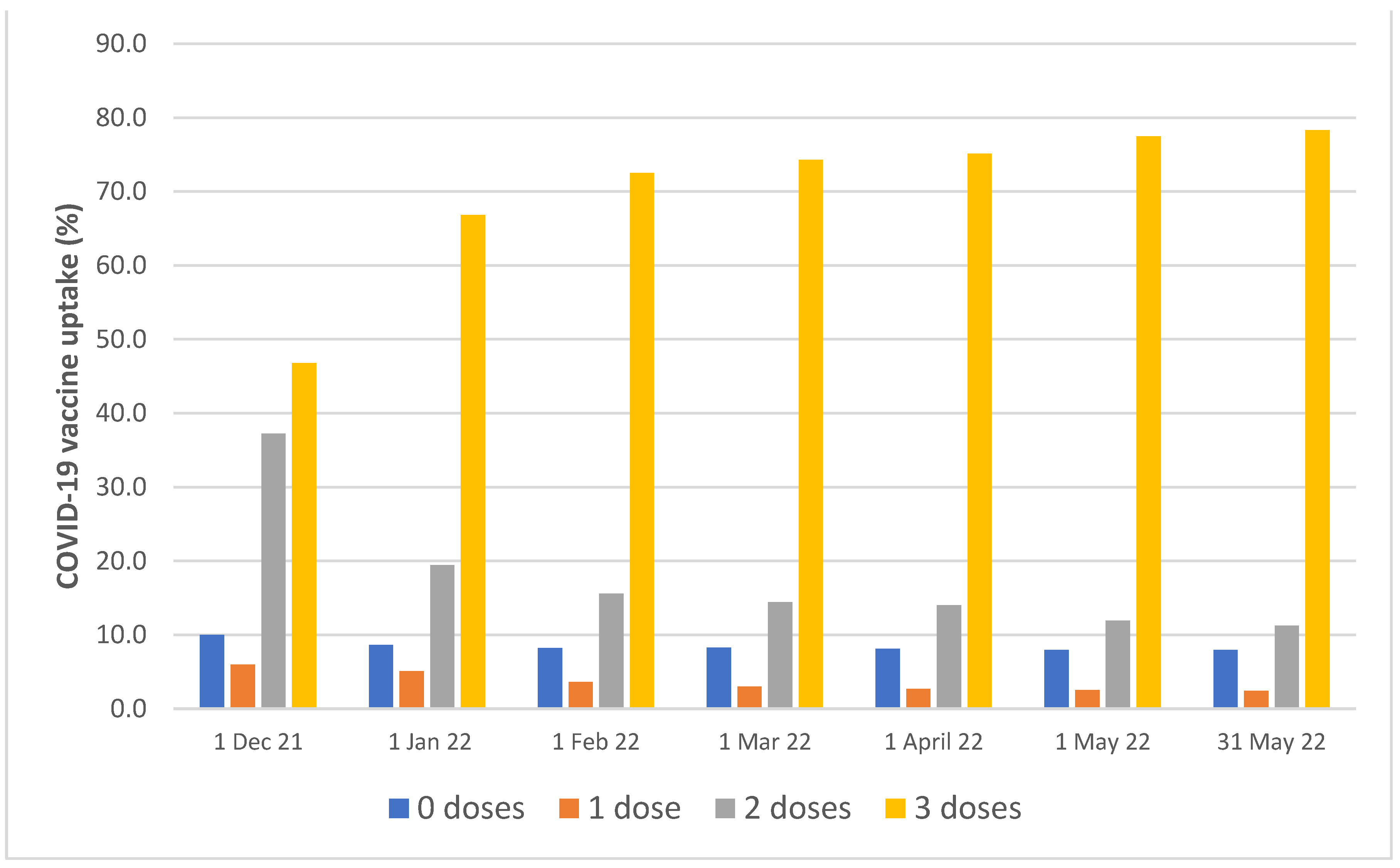
| DATE | Total HCWs | 0 Doses | 1 Dose | 2 Doses | 3 Doses | 4 Doses |
|---|---|---|---|---|---|---|
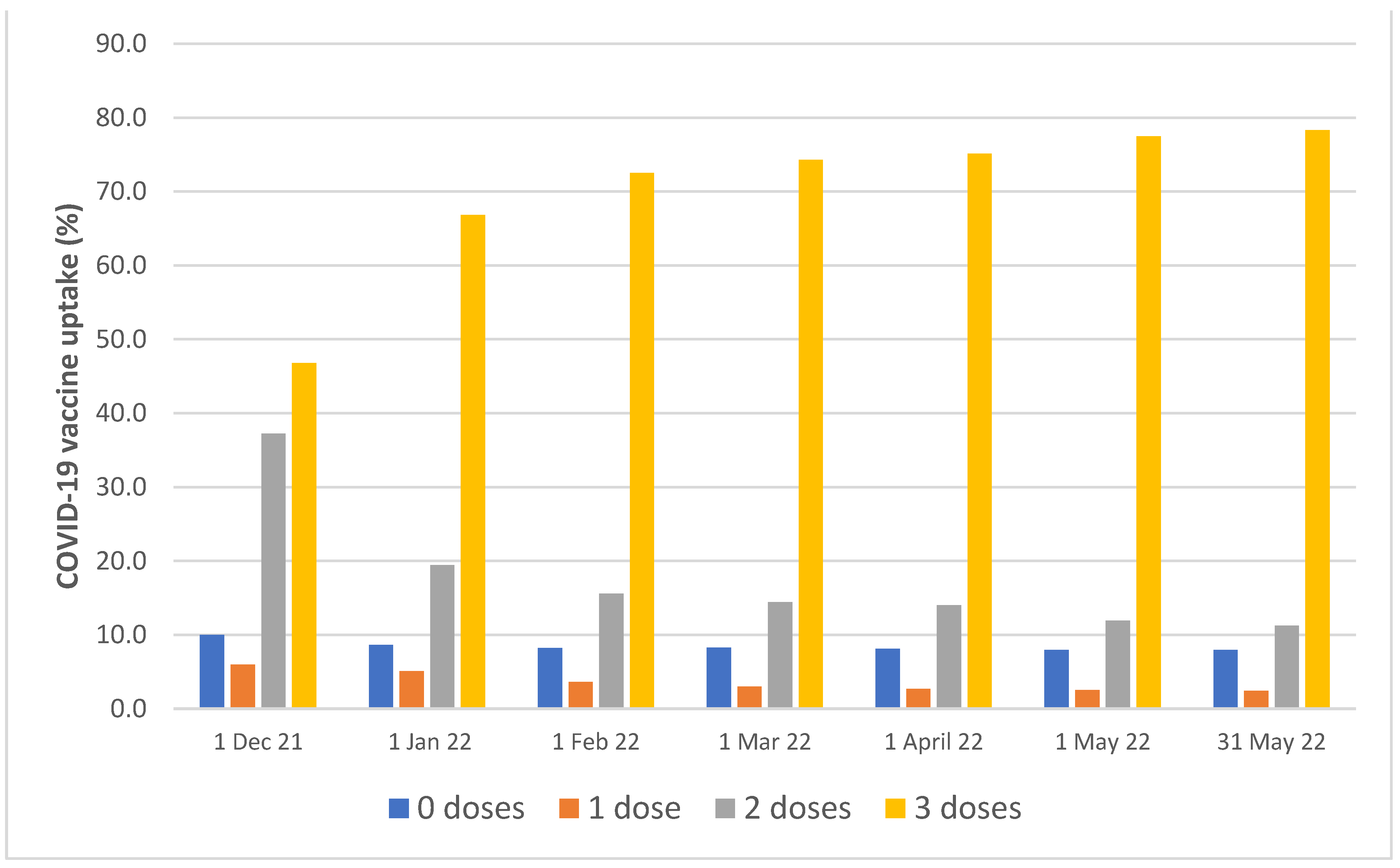
| 1 December 2021 | 7662 | 767 (10.0) | 458 (6.0) | 2850 (37.2) | 3613 (46.8) | 0 |
| 1 January 2022 | 7475 | 651 (8.6) | 384 (5.1) | 1500 (19.4) | 5161 (66.8) | 0 |
| 1 February 2022 | 7448 | 619 (8.30) | 274 (3.7) | 1156 (15.6) | 5399 (72.5) | 0 |
| 1 March 2022 | 7436 | 614 (8.3) | 223 (3.0) | 1068 (14.4) | 5531 (74.4) | 0 |
| 1 April 2022 | 7400 | 611 (8.3) | 198 (2.7) | 1031 (13.9) | 5560 (75.1) | 6 |
| 1 May 2022 | 7364 | 603 (8.2) | 181 (2.5) | 877 (11.5) | 5703 (77.4) | 9 |
| 31 May 2022 | 7345 | 595 (8.1) | 171 (2.3) | 822 (11.2) | 6052 (78.4) | 9 |
| Factors | Type of SARS-CoV-2 Infection (01/12/2021–31/05/2022) | Analysis Time | ||||
|---|---|---|---|---|---|---|
| Cases | Person-Days (p-d) at Risk | Raw Incidence (×1000 p-d) | ||||
| Total SARS-CoV-2 infections | Primary | 2130 | 219781 | 9.7 × 1000 | ||
| Recurrent | Total | 386 | 107,939 | 3.6 × 1000 | ||
| Primary infection before 01/12/2021 | 354 | 39,761 | 8.9 × 1000 | |||
| Primary infection after 30/11/2021 | 32 | 68,178 | 0.5 × 1000 | |||
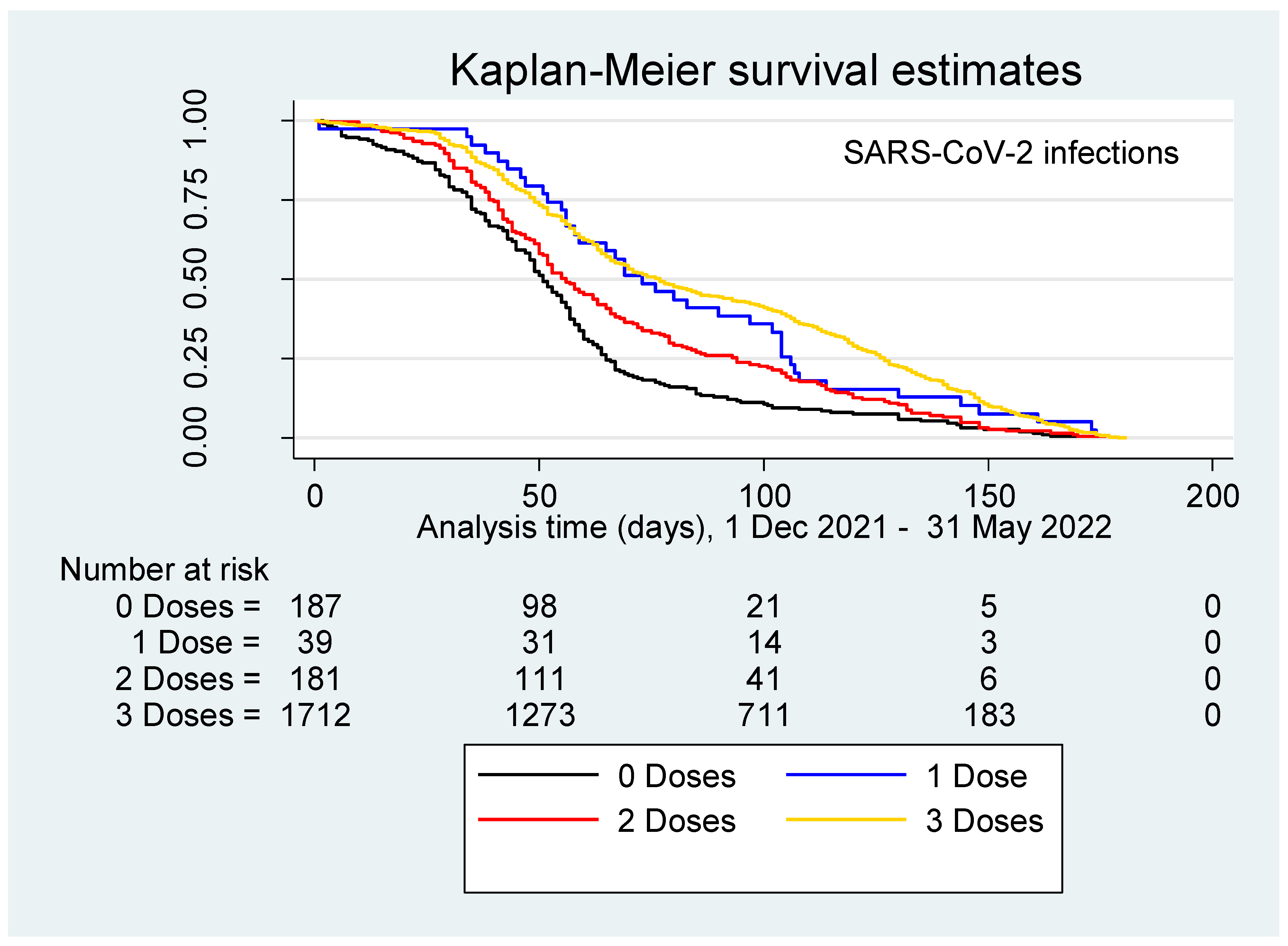
| Doses of COVID-19 vaccines | 0 | Primary | 187 | 13,183 | 14.2 × 1000 | |
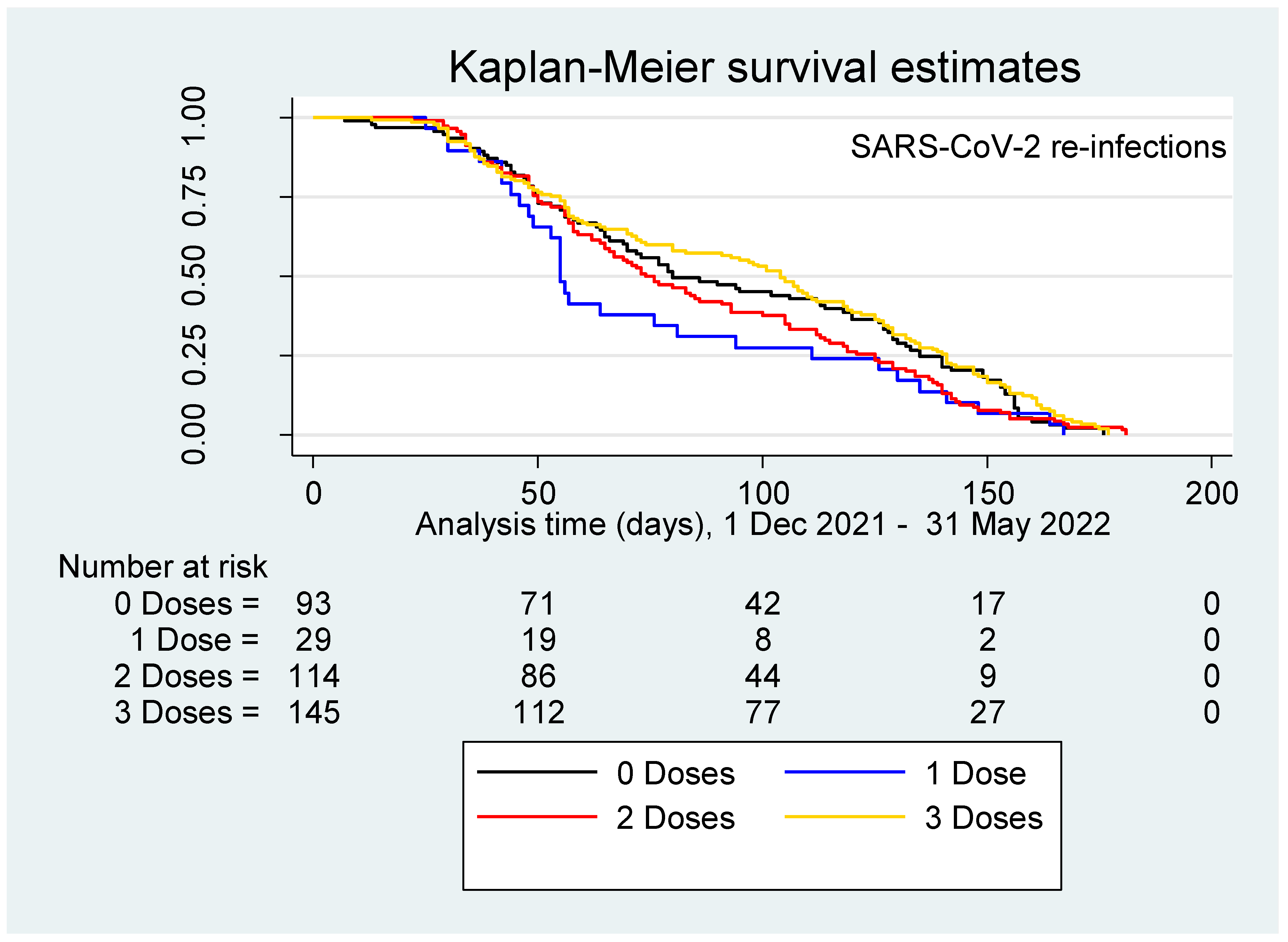
| Recurrent | Total | 93 | 12,199 | 7.6 × 1000 | ||
| Primary infection before 01/12/2021 | 73 | 5973 | 12.2 × 1000 | |||
| Primary infection after 30/11/2021 | 20 | 6226 | 3.2 × 1000 | |||
| 1 | Primary | 39 | 6268 | 6.2 × 1000 | ||
| Recurrent | Total | 29 | 6803 | 4.3 × 1000 | ||
| Primary infection before 01/12/2021 | 29 | 2544 | 11.4 × 1000 | |||
| Primary infection after 30/11/2021 | 0 | 3993 | 0 | |||
| 2 | Primary | 177 | 14,207 | 12.5 × 1000 | ||
| Recurrent | Total | 106 | 19,694 | 5.4 × 1000 | ||
| Primary infection before 01/12/2021 | 102 | 12,726 | 8.0 × 1000 | |||
| Primary infection after 30/11/2021 | 4 | 6968 | 0.6 × 1000 | |||
| 3 | Primary | 1680 | 184,719 | 9.1 × 1000 | ||
| Recurrent | Total | 141 | 68,558 | 2.1 × 1000 | ||
| Primary infection before 01/12/2021 | 133 | 17,833 | 7.5 × 1000 | |||
| Primary infection after 30/11/2021 | 8 | 50,725 | 0.2 × 1000 | |||
| Factor | Strata | Cox Regression Analysis | |||
|---|---|---|---|---|---|
| Univariable HR (95%CI) | Multivariable aHR (95%CI) | ||||
| Sex | Female | Reference | Reference | ||
| Male | 0.87 (0.80; 0.96) | 0.93 (0.83; 1.04) | |||
| Age (years) | <41 | Reference | |||
| 41–50 | 1.27 (1.14; 1.42) | ||||
| 51–60 | 1.11 (1.00; 1.24) | ||||
| 61+ | 0.84 (0.72; 0.97) | ||||
| ASUGI site | Gorizia-Monfalcone | Reference | |||
| Trieste | 0.92 (0.84; 1.00) | ||||
| Vaccine type | Comirnaty (Pfitzer/BioNTech) | Reference | |||
| Spikevax (Moderna) | 0.92 (0.73; 1.16) | ||||
| Other * | 0.68 (0.30; 1.51) | ||||
| N. Doses of COVID-19 vaccines | 0 | Reference | |||
| 1 | 0.41 (0.29; 0.58) | ||||
| 2 | 0.85 (0.69; 1.04) | ||||
| 3 | 0.58 (0.50; 0.67) | ||||
| N. Swab tests (1 Dec 2021– 31 May 2022) | 1–3 | Reference | COVID-19 vaccine doses | 0 | Reference |
| 1 | 4.15 −10 (1.57−10; 1.09−9) | ||||
| 2 | 0.59 (0.23; 1.49) | ||||
| 3 | 0.47 (0.21; 1.08) | ||||
| 4–6 | 1.27 (1.03; 1.56) | COVID-19 vaccine doses | 0 | 0.87 (0.37; 2.04) | |
| 1 | 0.36 (0.11; 1.16) | ||||
| 2 | 0.74 (0.32; 1.73) | ||||
| 3 | 0.65 (0.30; 1.42) | ||||
| 7–10 | 1.40 (1.16; 1.69) | COVID-19 vaccine doses | 0 | 1.16 (0.51; 2.64) | |
| 1 | 0.30 (0.09; 0.96) | ||||
| 2 | 0.85 (0.38; 1.93) | ||||
| 3 | 0.58 (0.27; 1.24) | ||||
| 10+ | 0.96 (0.80; 1.15) | COVID-19 vaccine doses | 0 | 0.88 (0.40; 1.95) | |
| 1 | 0.34 (0.14; 0.84) | ||||
| 2 | 0.65 (0.29; 1.47) | ||||
| 3 | 0.41 (0.15; 1.11) | ||||
| Job task | Administrative clerks | Reference | Years of age | <41 | Reference |
| 41–50 | 2.55 (1.45; 4.49) | ||||
| 51–60 | 2.28 (1.41; 3.67) | ||||
| 61+ | 1.07 (0.61; 1.89) | ||||
| Doctor | 1.16 (0.97; 1.38) | Years of age | <41 | 1.29 (0.84; 1.99) | |
| 41–50 | 2.46 (1.62; 3.73) | ||||
| 51–60 | 2.31 (1.45; 3.68) | ||||
| 61+ | 1.70 (1.02; 2.84) | ||||
| Nurses | 1.39 (1.18; 1.64) | Years of age | <41 | 3.12 (2.11; 4.61) | |
| 41–50 | 3.01 (2.00; 4.52) | ||||
| 51–60 | 2.21 (1.46; 3.37) | ||||
| 61+ | 2.08 (1.22; 3.53) | ||||
| Other HCWs | 1.39 (1.16; 1.65) | Years of age | <41 | 2.70 (1.74; 4.20) | |
| 41–50 | 2.84 (1.87; 4.33) | ||||
| 51–60 | 2.30 (1.51; 3.49) | ||||
| 61+ | 2.52 (1.55; 4.10) | ||||
| Health technicians | 1.20 (0.99; 1.44) | Years of age | <41 | 2.38 (1.59; 3.56) | |
| 41–50 | 2.78 (1.80; 4.30) | ||||
| 51–60 | 1.97 (1.26; 3.09) | ||||
| 61+ | 1.66 (0.96; 2.87) | ||||
| Workplace | Administrative services | Reference | Reference | ||
| Community health services | 1.42 (1.22; 1.65) | 1.18 (0.98; 1.43) | |||
| Radiology services (technicians) | 1.48 (1.21; 1.82) | 1.58 (1.26; 1.97) | |||
| Surgical wards | 1.34 (1.13; 1.59) | 1.43 (1.17; 1.76) | |||
| Medical and geriatric wards | 1.28 (1.09; 1.50) | 1.34 (1.11; 1.63) | |||
| COVID-19 areas | 1.04 (0.78; 1.40) | 1.07 (0.78; 1.47) | |||
| Accident and emergency (A&E) | 1.25 (1.04 1.50) | 1.28 (1.03; 1.59) | |||
| Non-clinical and other | 1.32 (1.01; 1.71) | 1.12 (0.79; 1.59) | |||
| Years of employment (linear term) | 1.01 (1.01; 1.01) | 1.01 (1.01; 1.02) | |||
| Educational level | Junior secondary | Reference | |||
| Secondary | 0.77 (0.62; 0.95) | ||||
| Bachelor’s degree | 1.01 (0.88; 1.15) | ||||
| Postgraduate diploma | 0.85 (0.75; 0.95) | ||||
| Factor | Strata | Cox Regression Analysis | |||
|---|---|---|---|---|---|
| Univariable HR (95%CI) | Multivariable aHR (95%CI) | ||||
| Sex | Female | Reference | Reference | ||
| Male | 0.71 (0.57; 0.89) | 0.75 (0.59; 0.96) | |||
| Age (years) | <41 | Reference | |||
| 41–50 | 1.97 (1.54; 2.52) | ||||
| 51–60 | 2.21 (1.72; 2.84) | ||||
| 61+ | 0.64 (0.39; 1.06) | ||||
| ASUGI Site | Gorizia-Monfalcone | Reference | |||
| Trieste | 1.00 (0.79; 1.24) | ||||
| Vaccine type | Comirnaty (Pfitzer/BioNTech) | Reference | |||
| Spikevax (Moderna) | 1.07 (0.68; 1.70) | ||||
| Other * | 135.78 (16.34; 1127.95) | ||||
| Doses of COVID-19 vaccines | 0 | Reference | Reference | ||
| 1 | 0.66 (0.43; 1.00) | 0.95 (0.59; 1.54) | |||
| 2 | 0.85 (0.65; 1.12) | 1.04 (0.76; 1.43) | |||
| 3 | 0.34 (0.26; 0.44) | 0.58 (0.42; 0.81) | |||
| Swab tests (1 December 2021– 31 May 2022) | 1–3 | Reference | Reference | ||
| 4–6 | 3.49 (1.50; 8.09) | 2.20 (0.67; 7.29) | |||
| 7–10 | 5.02 (2.21; 11.40) | 2.27 (0.69; 7.41) | |||
| 11+ | 4.46 (1.98; 10.06) | 1.49 (0.46; 4.86) | |||
| JOB TASK | Administrative clerks | Reference | Years of age | <41 | Reference |
| 41–50 | 4.11 (1.29; 13.09) | ||||
| 51–60 | 2.29 (0.69; 7.65) | ||||
| 61+ | 4.27 (1.05; 17.41) | ||||
| Doctor | 1.79 (1.08; 2.97) | Years of age | <41 | 1.84 (0.72; 4.71) | |
| 41–50 | 3.20 (1.20; 8.52) | ||||
| 51–60 | 4.32 (1.50; 12.39) | ||||
| 61+ | 1.73 (0.39; 7.58) | ||||
| Nurses | 3.80 (2.43; 5.95) | Years of age | <41 | 7.47 (3.26; 17.10) | |
| 41–50 | 5.33 (2.22; 12.79) | ||||
| 51–60 | 2.73 (1.09; 6.84) | ||||
| 61+ | 13.51 (3.20; 57.04) | ||||
| Other HCWs | 3.51 (2.21; 5.56) | Years of age | <41 | 4.57 (1.87; 11.15) | |
| 41–50 | 4.70 (1.97; 11.22) | ||||
| 51–60 | 5.01 (2.07; 12.17) | ||||
| 61+ | 1.12 (0.22; 5.57) | ||||
| Health technician | 1.72 (1.05; 2.82) | Years of age | <41 | 2.32 (0.99; 5.44) | |
| 41–50 | 3.89 (1.47; 10.26) | ||||
| 51–60 | 2.28 (0.76; 6.84) | ||||
| 61+ | 3.50 (0.91; 13.54) | ||||
| WORKPLACE | Administrative services | Reference | Reference | ||
| Community health services | 2.68 (1.88; 3.83) | 1.48 (0.96; 2.29) | |||
| Radiology services (technicians) | 1.89 (1.11; 3.20) | 1.95 (1.04; 3.65) | |||
| Surgical wards | 1.80 (1.19; 2.71) | 1.40 (0.87; 2.27) | |||
| Medical and geriatric wards | 2.28 (1.59; 3.26) | 2.09 (1.37; 3.21) | |||
| COVID-19 areas | 1.52 (0.85; 2.73) | 1.71 (0.90; 3.25) | |||
| Accident and emergency (A&E) | 2.65 (1.80; 3.89) | 2.00 (1.26; 3.17) | |||
| Non-clinical and other | 3.59 (1.75; 7.35) | 3.06 (1.30; 7.18) | |||
| Years of employment (linear term) | 1.06 (1.05; 1.07) | 1.05 (1.03; 1.07) | |||
| Educational level | Junior secondary | Reference | |||
| Secondary | 0.46 (0.28; 0.75) | ||||
| Bachelor | 0.88 (0.67; 1.16) | ||||
| Post-graduate diploma | 0.49 (0.36; 0.68) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cegolon, L.; Negro, C.; Mastrangelo, G.; Filon, F.L., on behalf of ORCHESTRA working group. Primary SARS-CoV-2 Infections, Re-infections and Vaccine Effectiveness during the Omicron Transmission Period in Healthcare Workers of Trieste and Gorizia (Northeast Italy), 1 December 2021–31 May 2022. Viruses 2022, 14, 2688. https://doi.org/10.3390/v14122688
Cegolon L, Negro C, Mastrangelo G, Filon FL on behalf of ORCHESTRA working group. Primary SARS-CoV-2 Infections, Re-infections and Vaccine Effectiveness during the Omicron Transmission Period in Healthcare Workers of Trieste and Gorizia (Northeast Italy), 1 December 2021–31 May 2022. Viruses. 2022; 14(12):2688. https://doi.org/10.3390/v14122688
Chicago/Turabian StyleCegolon, Luca, Corrado Negro, Giuseppe Mastrangelo, and Francesca Larese Filon on behalf of ORCHESTRA working group. 2022. "Primary SARS-CoV-2 Infections, Re-infections and Vaccine Effectiveness during the Omicron Transmission Period in Healthcare Workers of Trieste and Gorizia (Northeast Italy), 1 December 2021–31 May 2022" Viruses 14, no. 12: 2688. https://doi.org/10.3390/v14122688
APA StyleCegolon, L., Negro, C., Mastrangelo, G., & Filon, F. L., on behalf of ORCHESTRA working group. (2022). Primary SARS-CoV-2 Infections, Re-infections and Vaccine Effectiveness during the Omicron Transmission Period in Healthcare Workers of Trieste and Gorizia (Northeast Italy), 1 December 2021–31 May 2022. Viruses, 14(12), 2688. https://doi.org/10.3390/v14122688