
Loss to Follow-Up from HIV Pre-Exposure Prophylaxis Care in Men Who Have Sex with Men in West Africa

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Measures
2.3.1. Event of Interest (Outcome)
2.3.2. Covariates
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Sample Characteristics
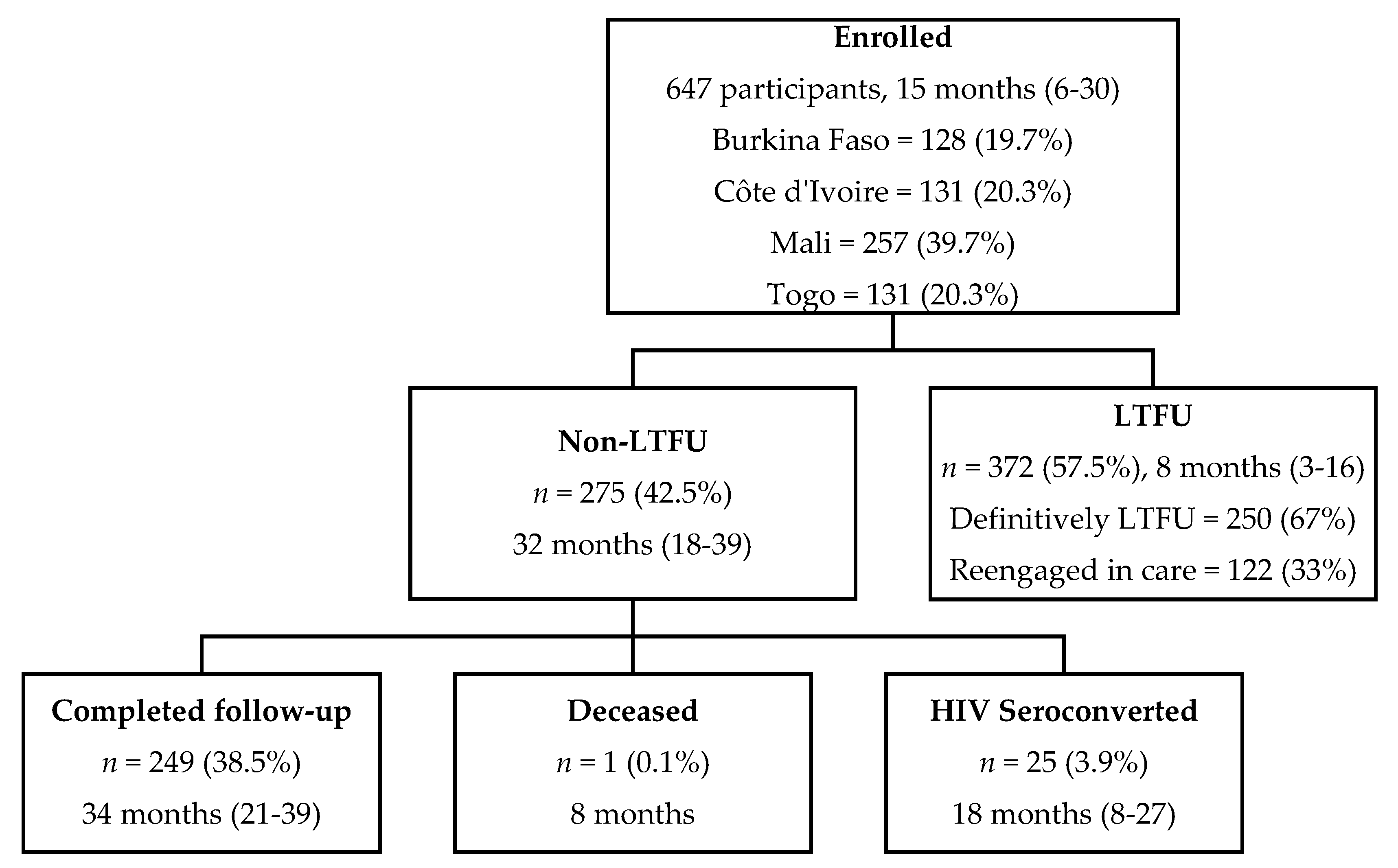
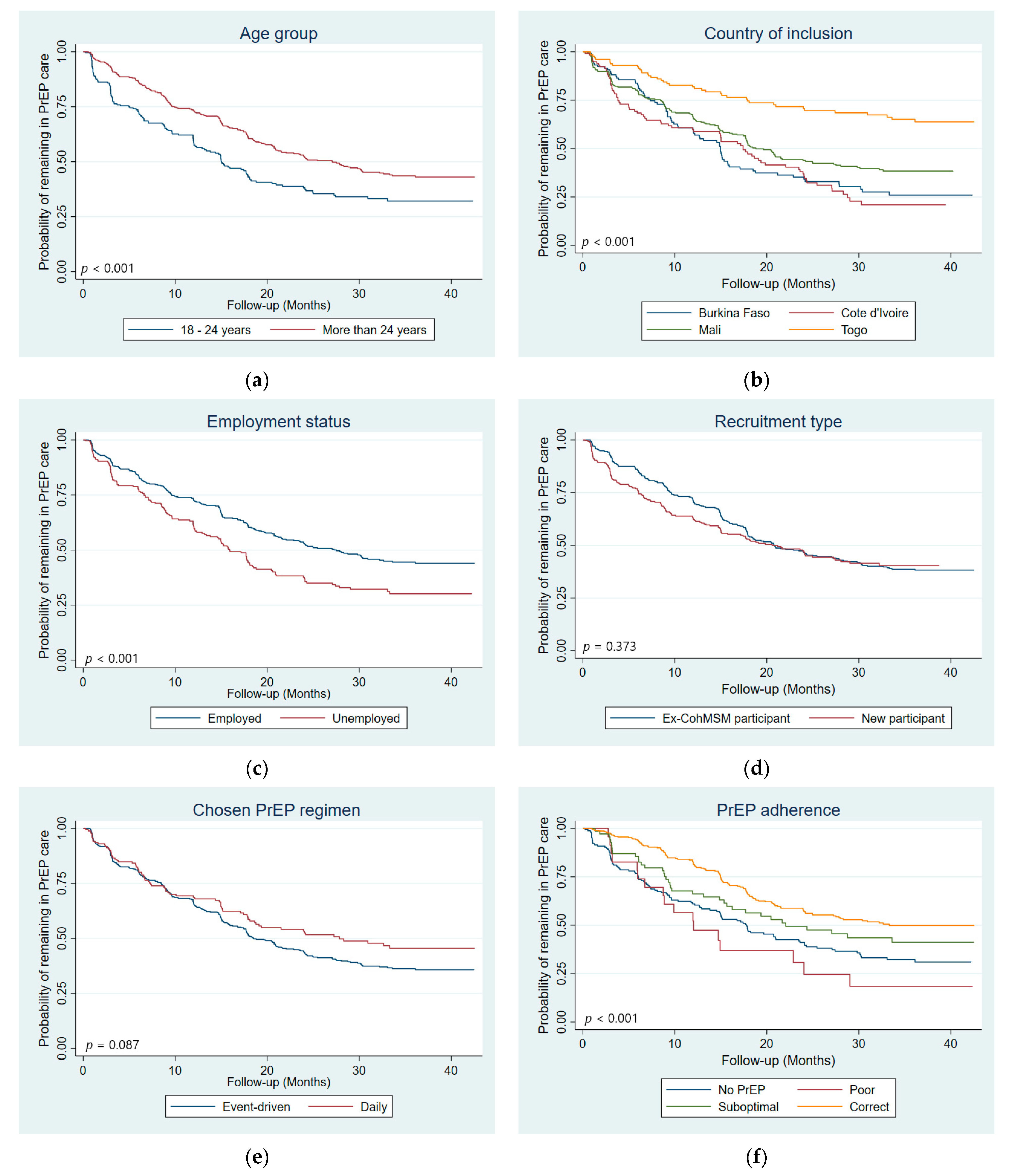
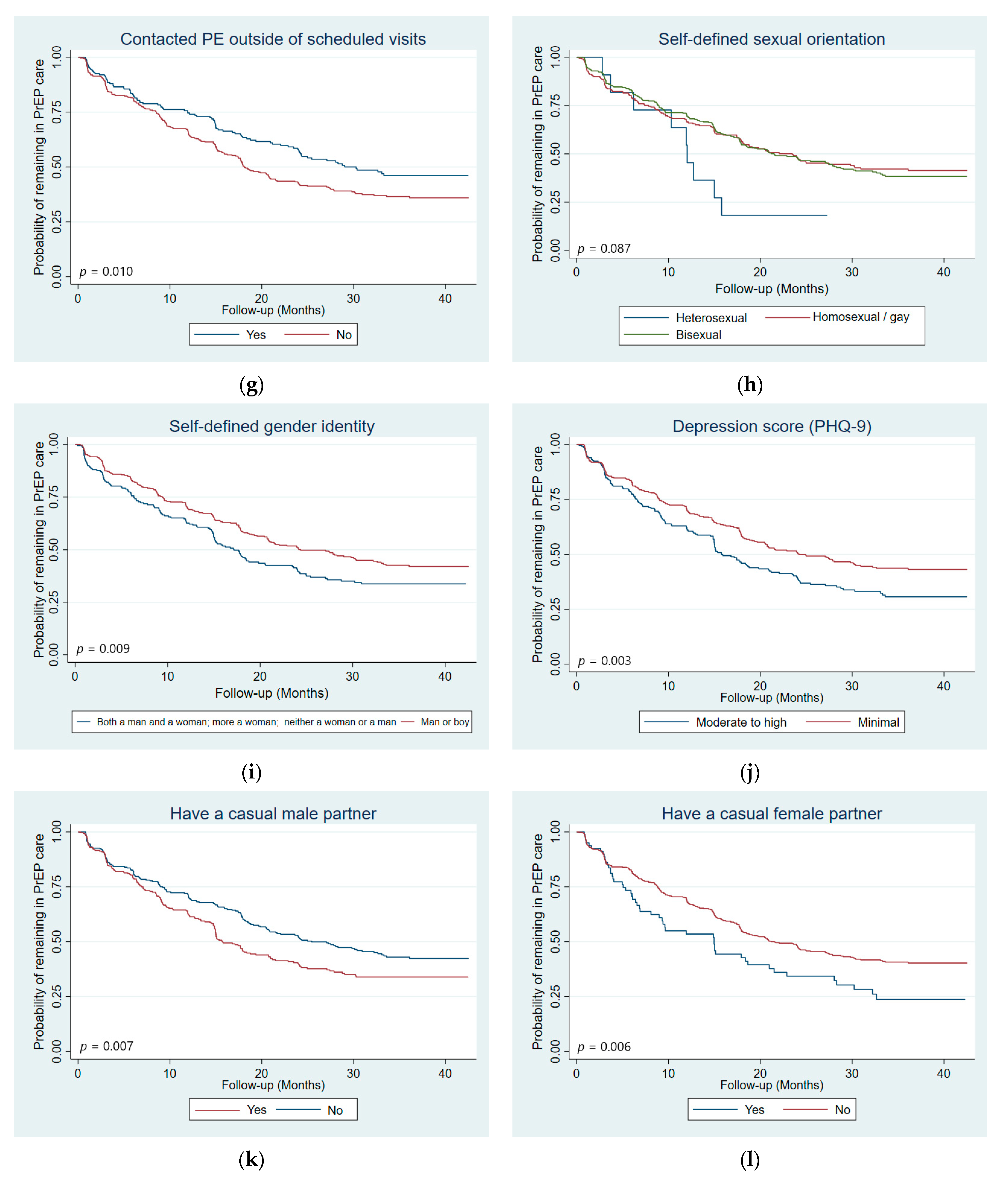
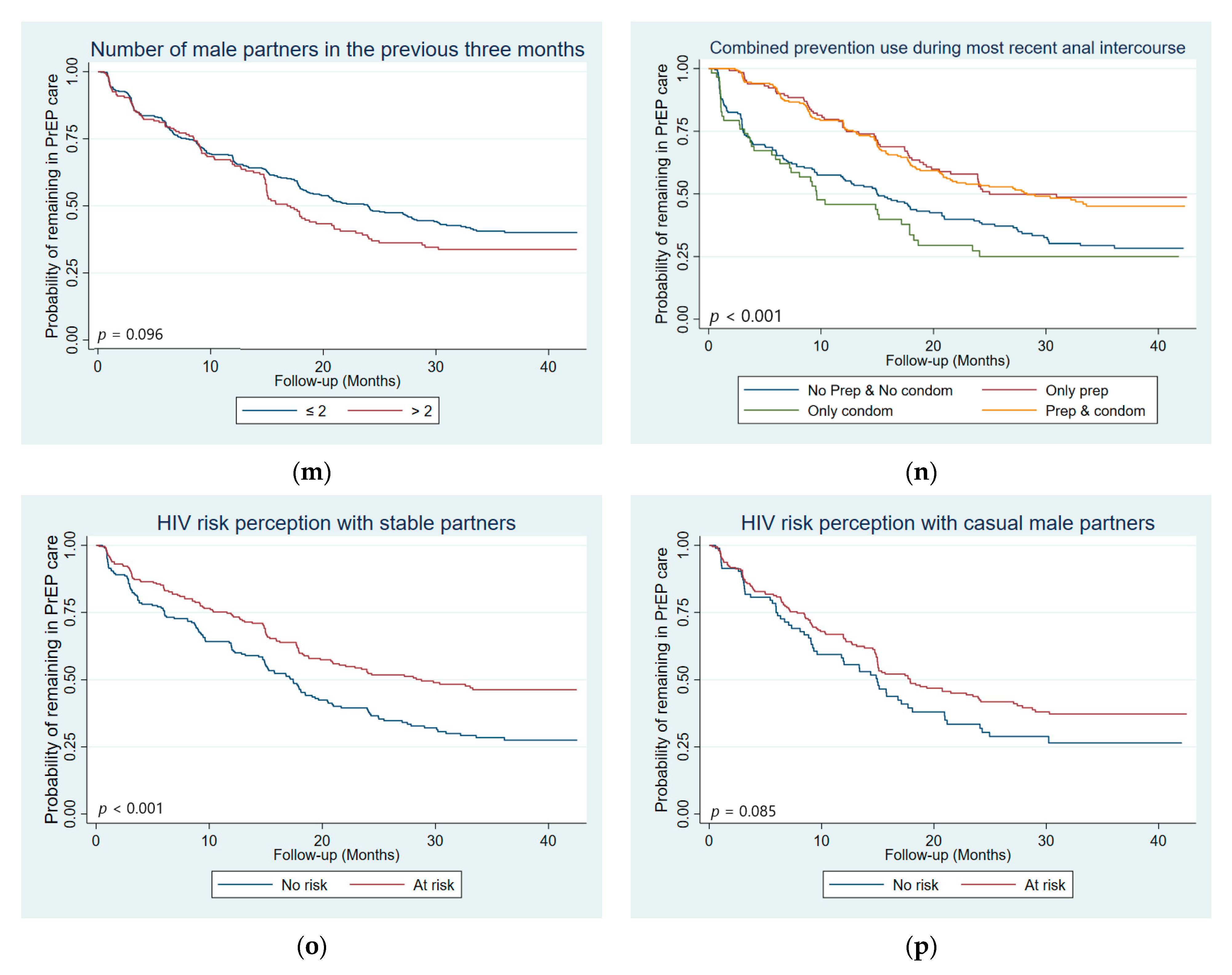
3.2. Loss to Follow-Up and Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS UNAIDS Data 2021. Available online: https://www.unaids.org/en/resources/documents/2021/2021_unaids_data (accessed on 11 May 2022).
- United Nations United Nations Political Declaration on Ending AIDS Sets World on the Fast-Track to End the Epidemic by 2030. Available online: https://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2016/june/20160608_PS_HLM_PoliticalDeclaration (accessed on 1 June 2022).
- United Nations United Nations Sustainable Development Goals (SDGs) 3: Ensure Healthy Lives and Promote Wellbeing for All at All Ages. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 19 September 2022).
- Bavinton, B.R.; Grulich, A.E. HIV Pre-Exposure Prophylaxis: Scaling up for Impact Now and in the Future. Lancet Public Health 2021, 6, e528–e533. [Google Scholar] [CrossRef]
- Grulich, A.E.; Bavinton, B.R. Scaling up Preexposure Prophylaxis to Maximize HIV Prevention Impact. Curr. Opin. HIV AIDS 2022, 17, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Estcourt, C.; Yeung, A.; Nandwani, R.; Goldberg, D.; Cullen, B.; Steedman, N.; Wallace, L.; Hutchinson, S. Population-Level Effectiveness of a National HIV Preexposure Prophylaxis Programme in MSM. AIDS 2021, 35, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Grulich, A.E.; Guy, R.; Amin, J.; Jin, F.; Selvey, C.; Holden, J.; Schmidt, H.-M.A.; Zablotska, I.; Price, K.; Whittaker, B.; et al. Population-Level Effectiveness of Rapid, Targeted, High-Coverage Roll-out of HIV Pre-Exposure Prophylaxis in Men Who Have Sex with Men: The EPIC-NSW Prospective Cohort Study. Lancet HIV 2018, 5, e629–e637. [Google Scholar] [CrossRef]
- Public Health England towards Zero HIV Transmissions by 2030. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/965765/HIV_in_the_UK_2019_towards_zero_HIV_transmissions_by_2030.pdf (accessed on 1 July 2022).
- San Francisco Department of Public Health Population Health Division HIV Epidemiology Annual Report 2020. Available online: https://www.sfdph.org/dph/comupg/oprograms/hivepisec/hivepisecreports.asp (accessed on 3 July 2022).
- Beyrer, C.; Baral, S.D.; van Griensven, F.; Goodreau, S.M.; Chariyalertsak, S.; Wirtz, A.L.; Brookmeyer, R. Global Epidemiology of HIV Infection in Men Who Have Sex with Men. Lancet 2012, 380, 367–377. [Google Scholar] [CrossRef]
- Baral, S.; Scheibe, A.; Sullivan, P.; Trapence, G.; Lambert, A.; Bekker, L.-G.; Beyrer, C. Assessing Priorities for Combination HIV Prevention Research for Men Who Have Sex with Men (MSM) in Africa. AIDS Behav. 2013, 17 (Suppl. 1), S60–S69. [Google Scholar] [CrossRef]
- Beyrer, C.; Baral, S.D.; Collins, C.; Richardson, E.T.; Sullivan, P.S.; Sanchez, J.; Trapence, G.; Katabira, E.; Kazatchkine, M.; Ryan, O.; et al. The Global Response to HIV in Men Who Have Sex with Men. Lancet 2016, 388, 198–206. [Google Scholar] [CrossRef]
- Grosso, A.; Ryan, O.; Tram, K.H.; Baral, S. Financing the Response to HIV among Gay Men and Other Men Who Have Sex with Men: Case Studies from Eight Diverse Countries. Glob. Public Health 2015, 10, 1172–1184. [Google Scholar] [CrossRef] [PubMed]
- Djomand, G.; Quaye, S.; Sullivan, P.S. HIV Epidemic among Key Populations in West Africa. Curr. Opin. HIV AIDS 2014, 9, 506–513. [Google Scholar] [CrossRef]
- Smith, A.D.; Tapsoba, P.; Peshu, N.; Sanders, E.J.; Jaffe, H.W. Men Who Have Sex with Men and HIV/AIDS in Sub-Saharan Africa. Lancet 2009, 374, 416–422. [Google Scholar] [CrossRef]
- Kushwaha, S.; Lalani, Y.; Maina, G.; Ogunbajo, A.; Wilton, L.; Agyarko-Poku, T.; Adu-Sarkodie, Y.; Boakye, F.; Zhang, N.; Nelson, L.E. “But the Moment They Find out That You Are MSM…”: A Qualitative Investigation of HIV Prevention Experiences among Men Who Have Sex with Men (MSM) in Ghana’s Health Care System. BMC Public Health 2017, 17, 770. [Google Scholar] [CrossRef] [PubMed]
- Ogunbajo, A.; Kershaw, T.; Kushwaha, S.; Boakye, F.; Wallace-Atiapah, N.-D.; Nelson, L.E. Barriers, Motivators, and Facilitators to Engagement in HIV Care Among HIV-Infected Ghanaian Men Who Have Sex with Men (MSM). AIDS Behav. 2018, 22, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Mendos, L.R. State Sponsored Homophobia; International Lesbian, Gay, Bisexual, Trans and Intersex Association (ILGA): Geneva, Switzerland, 2019. [Google Scholar]
- Poteat, T.; Diouf, D.; Drame, F.M.; Ndaw, M.; Traore, C.; Dhaliwal, M.; Beyrer, C.; Baral, S. HIV Risk among MSM in Senegal: A Qualitative Rapid Assessment of the Impact of Enforcing Laws That Criminalize Same Sex Practices. PLoS ONE 2011, 6, e28760. [Google Scholar] [CrossRef] [PubMed]
- Aho, J.; Hakim, A.; Vuylsteke, B.; Semde, G.; Gbais, H.G.; Diarrassouba, M.; Thiam, M.; Laga, M. Exploring Risk Behaviors and Vulnerability for HIV among Men Who Have Sex with Men in Abidjan, Cote d’Ivoire: Poor Knowledge, Homophobia and Sexual Violence. PLoS ONE 2014, 9, e99591. [Google Scholar] [CrossRef]
- Grinsztejn, B.; Hoagland, B.; Moreira, R.I.; Kallas, E.G.; Madruga, J.V.; Goulart, S.; Leite, I.C.; Freitas, L.; Martins, L.M.S.; Torres, T.S.; et al. Retention, Engagement, and Adherence to Pre-Exposure Prophylaxis for Men Who Have Sex with Men and Transgender Women in PrEP Brasil: 48 Week Results of a Demonstration Study. Lancet HIV 2018, 5, e136–e145. [Google Scholar] [CrossRef]
- Shover, C.L.; Shoptaw, S.; Javanbakht, M.; Lee, S.-J.; Bolan, R.K.; Cunningham, N.J.; Beymer, M.R.; DeVost, M.A.; Gorbach, P.M. Mind the Gaps: Prescription Coverage and HIV Incidence among Patients Receiving Pre-Exposure Prophylaxis from a Large Federally Qualified Health Center in Los Angeles, California. AIDS Behav. 2019, 23, 2730–2740. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.A.; Mena, L.; Patel, R.; Oldenburg, C.E.; Beauchamps, L.; Perez-Brumer, A.G.; Parker, S.; Mayer, K.H.; Mimiaga, M.J.; Nunn, A. Retention in Care Outcomes for HIV Pre-Exposure Prophylaxis Implementation Programmes among Men Who Have Sex with Men in Three US Cities. J. Int. AIDS Soc. 2016, 19, 20903. [Google Scholar] [CrossRef]
- Phanuphak, N.; Sungsing, T.; Jantarapakde, J.; Pengnonyang, S.; Trachunthong, D.; Mingkwanrungruang, P.; Sirisakyot, W.; Phiayura, P.; Seekaew, P.; Panpet, P.; et al. Princess PrEP Program: The First Key Population-Led Model to Deliver Pre-Exposure Prophylaxis to Key Populations by Key Populations in Thailand. Sex. Health 2018, 15, 542–555. [Google Scholar] [CrossRef]
- Kimani, M.; van der Elst, E.M.; Chirro, O.; Wahome, E.; Ibrahim, F.; Mukuria, N.; de Wit, T.F.R.; Graham, S.M.; Operario, D.; Sanders, E.J. “I Wish to Remain HIV Negative”: Pre-Exposure Prophylaxis Adherence and Persistence in Transgender Women and Men Who Have Sex with Men in Coastal Kenya. PLoS ONE 2021, 16, e0244226. [Google Scholar] [CrossRef]
- Wahome, E.W.; Graham, S.M.; Thiong’o, A.N.; Mohamed, K.; Oduor, T.; Gichuru, E.; Mwambi, J.; van der Elst, E.M.; Sanders, E.J. Risk Factors for Loss to Follow-up among at-Risk HIV Negative Men Who Have Sex with Men Participating in a Research Cohort with Access to Pre-Exposure Prophylaxis in Coastal Kenya. J. Int. AIDS Soc. 2020, 23, e25593. [Google Scholar] [CrossRef]
- Wahome, E.; Boyd, A.; Thiong’o, A.N.; Mohamed, K.; Oduor, T.; Gichuru, E.; Mwambi, J.; van der Elst, E.; Graham, S.M.; Prins, M.; et al. Stopping and Restarting PrEP and Loss to Follow-up among PrEP-Taking Men Who Have Sex with Men and Transgender Women at Risk of HIV-1 Participating in a Prospective Cohort Study in Kenya. HIV Med. 2022, 23, 750–763. [Google Scholar] [CrossRef] [PubMed]
- Pillay, D.; Stankevitz, K.; Lanham, M.; Ridgeway, K.; Murire, M.; Briedenhann, E.; Jenkins, S.; Subedar, H.; Hoke, T.; Mullick, S. Factors Influencing Uptake, Continuation, and Discontinuation of Oral PrEP among Clients at Sex Worker and MSM Facilities in South Africa. PLoS ONE 2020, 15, e0228620. [Google Scholar] [CrossRef] [PubMed]
- Parmley, L.E.; Harris, T.G.; Chingombe, I.; Mapingure, M.; Mugurungi, O.; Rogers, J.H.; Gozhora, P.; Wu, Y.; Samba, C.; Musuka, G.; et al. Engagement in the Pre-Exposure Prophylaxis (PrEP) Cascade among a Respondent-Driven Sample of Sexually Active Men Who Have Sex with Men and Transgender Women during Early PrEP Implementation in Zimbabwe. J. Int. AIDS Soc. 2022, 25, e25873. [Google Scholar] [CrossRef]
- Laurent, C.; Keita, B.D.; Yaya, I.; Guicher, G.L.; Sagaon-Teyssier, L.; Agboyibor, M.K.; Coulibaly, A.; Traoré, I.; Malan, J.-B.; Baetselier, I.D.; et al. HIV Pre-Exposure Prophylaxis for Men Who Have Sex with Men in West Africa: A Multicountry Demonstration Study. Lancet HIV 2021, 8, e420–e428. [Google Scholar] [CrossRef]
- Zhang, J.; Li, C.; Xu, J.; Hu, Z.; Rutstein, S.E.; Tucker, J.D.; Ong, J.J.; Jiang, Y.; Geng, W.; Wright, S.T.; et al. Discontinuation, Suboptimal Adherence, and Reinitiation of Oral HIV Pre-Exposure Prophylaxis: A Global Systematic Review and Meta-Analysis. Lancet HIV 2022, 9, e254–e268. [Google Scholar] [CrossRef]
- Rutstein, S.E.; Smith, D.K.; Dalal, S.; Baggaley, R.C.; Cohen, M.S. Initiation, Discontinuation, and Restarting HIV Pre-Exposure Prophylaxis: Ongoing Implementation Strategies. Lancet HIV 2020, 7, e721–e730. [Google Scholar] [CrossRef]
- Garrison, L.E.; Haberer, J.E. Pre-Exposure Prophylaxis Uptake, Adherence, and Persistence: A Narrative Review of Interventions in the U.S. Am. J. Prev. Med. 2021, 61, S73–S86. [Google Scholar] [CrossRef]
- Golub, S.A.; Enemchukwu, C.U. The Critical Importance of Retention in HIV Prevention. Lancet HIV 2018, 5, e475–e476. [Google Scholar] [CrossRef]
- Nunn, A.S.; Brinkley-Rubinstein, L.; Oldenburg, C.E.; Mayer, K.H.; Mimiaga, M.; Patel, R.; Chan, P.A. Defining the HIV Pre-Exposure Prophylaxis Care Continuum. AIDS 2017, 31, 731–734. [Google Scholar] [CrossRef]
- Parsons, J.T.; Rendina, H.J.; Lassiter, J.M.; Whitfield, T.H.F.; Starks, T.J.; Grov, C. Uptake of HIV Pre-Exposure Prophylaxis (PrEP) in a National Cohort of Gay and Bisexual Men in the United States: The Motivational PrEP Cascade. J. Acquir. Immune Defic. Syndr. 2017, 74, 285–292. [Google Scholar] [CrossRef]
- Liu, A.; Cohen, S.; Follansbee, S.; Cohan, D.; Weber, S.; Sachdev, D.; Buchbinder, S. Early Experiences Implementing Pre-Exposure Prophylaxis (PrEP) for HIV Prevention in San Francisco. PLoS Med. 2014, 11, e1001613. [Google Scholar] [CrossRef] [PubMed]
- Newman, P.A.; Guta, A.; Lacombe-Duncan, A.; Tepjan, S. Clinical Exigencies, Psychosocial Realities: Negotiating HIV Pre-Exposure Prophylaxis beyond the Cascade among Gay, Bisexual and Other Men Who Have Sex with Men in Canada. J. Int. AIDS Soc. 2018, 21, e25211. [Google Scholar] [CrossRef] [PubMed]
- Hillis, A.; Germain, J.; Hope, V.; McVeigh, J.; Van Hout, M.C. Pre-Exposure Prophylaxis (PrEP) for HIV Prevention Among Men Who Have Sex with Men (MSM): A Scoping Review on PrEP Service Delivery and Programming. AIDS Behav. 2020, 24, 3056–3070. [Google Scholar] [CrossRef] [PubMed]
- Beach, L.B.; Greene, G.J.; Lindeman, P.; Johnson, A.K.; Adames, C.N.; Thomann, M.; Washington, P.C.T.; Phillips, G. Barriers and Facilitators to Seeking HIV Services in Chicago Among Young Men Who Have Sex with Men: Perspectives of HIV Service Providers. AIDS Patient Care STDS 2018, 32, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Galindo, G.R.; Garrett-Walker, J.J.; Hazelton, P.; Lane, T.; Steward, W.T.; Morin, S.F.; Arnold, E.A. Community Member Perspectives from Transgender Women and Men Who Have Sex with Men on Pre-Exposure Prophylaxis as an HIV Prevention Strategy: Implications for Implementation. Implement. Sci. 2012, 7, 116. [Google Scholar] [CrossRef]
- Kelley, C.F.; Kahle, E.; Siegler, A.; Sanchez, T.; del Rio, C.; Sullivan, P.S.; Rosenberg, E.S. Applying a PrEP Continuum of Care for Men Who Have Sex With Men in Atlanta, Georgia. Clin. Infect. Dis. 2015, 61, 1590–1597. [Google Scholar] [CrossRef]
- Hosek, S.; Rudy, B.; Landovitz, R.; Kapogiannis, B.; Siberry, G.; Rutledge, B.; Liu, N.; Brothers, J.; Mulligan, K.; Zimet, G.; et al. An HIV Pre-Exposure Prophylaxis (PrEP) Demonstration Project and Safety Study for Young MSM. J. Acquir. Immune Defic. Syndr. 2017, 74, 21–29. [Google Scholar] [CrossRef]
- Stankevitz, K.; Grant, H.; Lloyd, J.; Gomez, G.B.; Kripke, K.; Torjesen, K.; Ong, J.J.; Terris-Prestholt, F. Oral Preexposure Prophylaxis Continuation, Measurement and Reporting. AIDS 2020, 34, 1801–1811. [Google Scholar] [CrossRef]
- Whitfield, T.H.F.; John, S.A.; Rendina, H.J.; Grov, C.; Parsons, J.T. Why I Quit Pre-Exposure Prophylaxis (PrEP)? A Mixed-Method Study Exploring Reasons for PrEP Discontinuation and Potential Re-Initiation among Gay and Bisexual Men. AIDS Behav. 2018, 22, 3566–3575. [Google Scholar] [CrossRef]
- Marcus, J.L.; Hurley, L.B.; Hare, C.B.; Nguyen, D.P.; Phengrasamy, T.; Silverberg, M.J.; Stoltey, J.E.; Volk, J.E. Preexposure Prophylaxis for HIV Prevention in a Large Integrated Health Care System: Adherence, Renal Safety, and Discontinuation. J. Acquir. Immune Defic. Syndr. 2016, 73, 540–546. [Google Scholar] [CrossRef]
- Spinelli, M.A.; Scott, H.M.; Vittinghoff, E.; Liu, A.Y.; Gonzalez, R.; Morehead-Gee, A.; Gandhi, M.; Buchbinder, S.P. Missed Visits Associated with Future Preexposure Prophylaxis (PrEP) Discontinuation among PrEP Users in a Municipal Primary Care Health Network. Open Forum Infect. Dis. 2019, 6, ofz101. [Google Scholar] [CrossRef] [PubMed]
- Hojilla, J.C.; Vlahov, D.; Crouch, P.-C.; Dawson-Rose, C.; Freeborn, K.; Carrico, A. HIV Pre-Exposure Prophylaxis (PrEP) Uptake and Retention among Men Who Have Sex with Men in a Community-Based Sexual Health Clinic. AIDS Behav. 2018, 22, 1096–1099. [Google Scholar] [CrossRef]
- Morgan, E.; Ryan, D.T.; Newcomb, M.E.; Mustanski, B. High Rate of Discontinuation May Diminish PrEP Coverage Among Young Men Who Have Sex with Men. AIDS Behav. 2018, 22, 3645–3648. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.Y.; Cohen, S.E.; Vittinghoff, E.; Anderson, P.L.; Doblecki-Lewis, S.; Bacon, O.; Chege, W.; Postle, B.S.; Matheson, T.; Amico, K.R.; et al. Preexposure Prophylaxis for HIV Infection Integrated With Municipal- and Community-Based Sexual Health Services. JAMA Intern. Med. 2016, 176, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Krakower, D.; Maloney, K.M.; Powell, V.E.; Levine, K.; Grasso, C.; Melbourne, K.; Marcus, J.L.; Mayer, K.H. Patterns and Clinical Consequences of Discontinuing HIV Preexposure Prophylaxis during Primary Care. J. Int. AIDS Soc. 2019, 22, e25250. [Google Scholar] [CrossRef] [PubMed]
- Dombrowski, J.C.; Golden, M.R.; Barbee, L.A.; Khosropour, C.M. Patient Disengagement from an HIV Pre-Exposure Prophylaxis Program in a Sexually Transmitted Disease Clinic. Sex Transm. Dis. 2018, 45, e62–e64. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, E.; Knapper, C. Audit of Patient Retention in Pre-Exposure Prophylaxis (PrEP) Services in an Integrated Sexual Reproductive Health Service Setting. Int. J. STD AIDS 2019, 30, 1432–1435. [Google Scholar] [CrossRef]
- Haberer, J.E.; Bangsberg, D.R.; Baeten, J.M.; Curran, K.; Koechlin, F.; Amico, K.R.; Anderson, P.; Mugo, N.; Venter, F.; Goicochea, P.; et al. Defining Success with HIV Pre-Exposure Prophylaxis: A Prevention-Effective Adherence Paradigm. AIDS 2015, 29, 1277–1285. [Google Scholar] [CrossRef]
- Spinelli, M.A.; Glidden, D.V.; Anderson, P.L.; Gandhi, M.; Cohen, S.; Vittinghoff, E.; Coleman, M.E.; Scott, H.; Bacon, O.; Elion, R.; et al. Brief Report: Short-Term Adherence Marker to PrEP Predicts Future Nonretention in a Large PrEP Demo Project: Implications for Point-of-Care Adherence Testing. JAIDS J. Acquir. Immune Defic. Syndr. 2019, 81, 158–162. [Google Scholar] [CrossRef]
- Doblecki-Lewis, S.; Liu, A.Y.; Feaster, D.J.; Cohen, S.E.; Elion, R.; Bacon, O.; Coleman, M.; Cardenas, G.; Kolber, M.A. Patterns and Correlates of Participant Retention in a Multi-City Pre-Exposure Prophylaxis Demonstration Project. J. Acquir. Immune Defic. Syndr. 2018, 79, 62–69. [Google Scholar] [CrossRef]
- Huang, Y.-L.A.; Tao, G.; Smith, D.K.; Hoover, K.W. Persistence With Human Immunodeficiency Virus Pre-Exposure Prophylaxis in the United States, 2012–2017. Clin. Infect. Dis. 2021, 72, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Holloway, I.; Dougherty, R.; Gildner, J.; Beougher, S.C.; Pulsipher, C.; Montoya, J.A.; Plant, A.; Leibowitz, A. PrEP Uptake, Adherence, and Discontinuation among California YMSM Using Geosocial Networking Applications. J. Acquir. Immune Defic. Syndr. 2017, 74, 15–20. [Google Scholar] [CrossRef] [PubMed]
- AVAC PrEPWatch. Available online: https://www.prepwatch.org/ (accessed on 12 May 2022).
- Eubanks, A.; Coulibaly, B.; Dembélé Keita, B.; Anoma, C.; Dah, T.T.E.; Mensah, E.; Kaba, S.; Lokrou, K.J.; Ouedraogo, F.R.; Badjassim, A.M.F.; et al. Socio-Behavioral Correlates of Pre-Exposure Prophylaxis Use and Correct Adherence in Men Who Have Sex with Men in West Africa. BMC Public Health 2022, 22, 1832. [Google Scholar] [CrossRef] [PubMed]
- Eubanks, A.; Dembélé Keita, B.; Anoma, C.; Dah, T.T.E.; Mensah, E.; Maradan, G.; Bourrelly, M.; Mora, M.; Riegel, L.; Rojas Castro, D.; et al. Reaching a Different Population of MSM in West Africa With the Integration of PrEP Into a Comprehensive Prevention Package (CohMSM-PrEP ANRS 12369-Expertise France). J. Acquir. Immune Defic. Syndr. 2020, 85, 292–301. [Google Scholar] [CrossRef]
- Eubanks, A.; Coulibaly, B.; Dembélé Keita, B.; Anoma, C.; DAH, T.T.E.; Mensah, E.; Maradan, G.; Bourrelly, M.; Mora, M.; Riegel, L.; et al. Rate and Predictors of Ineffective HIV Protection in African Men Who Have Sex with Men Taking Pre-Exposure Prophylaxis. AIDS Behav. 2022, 26, 3524–3537. [Google Scholar] [CrossRef]
- Dah, T.T.E.; Yaya, I.; Sagaon-Teyssier, L.; Coulibaly, A.; Kouamé, M.J.-B.; Agboyibor, M.K.; Maiga, K.; Traoré, I.; Mora, M.; Palvadeau, P.; et al. Adherence to Quarterly HIV Prevention Services and Its Impact on HIV Incidence in Men Who Have Sex with Men in West Africa (CohMSM ANRS 12324—Expertise France). BMC Public Health 2021, 21, 972. [Google Scholar] [CrossRef]
- World Health Organization. What’s the 2 + 1 + 1? Event-Driven Oral Pre-Exposure Prophylaxis to Prevent HIV for Men Who Have Sex with Men: Update to Who’s Recommendation on Oral Prep. Available online: http://www.who.int (accessed on 3 June 2021).
- Molina, J.-M.; Capitant, C.; Spire, B.; Pialoux, G.; Cotte, L.; Charreau, I.; Tremblay, C.; Le Gall, J.-M.; Cua, E.; Pasquet, A.; et al. On-Demand Preexposure Prophylaxis in Men at High Risk for HIV-1 Infection. N. Engl. J. Med. 2015, 373, 2237–2246. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kelly, J.A.; Amirkhanian, Y.A.; Walsh, J.L.; Brown, K.D.; Quinn, K.G.; Petroll, A.E.; Pearson, B.M.; Rosado, A.N.; Ertl, T. AIDSImpact Special Issue Social Network Intervention to Increase Pre-Exposure Prophylaxis (PrEP) Awareness, Interest, and Use Among African American Men Who Have Sex with Men. AIDS Care 2020, 32, 40–46. [Google Scholar] [CrossRef]
- Schneider, J.A.; Young, L.; Ramachandran, A.; Michaels, S.; Cohen, H.; Robinson, I.; Alon, L.; Hill, B.; Nakasone, S.; Balenciaga, M.; et al. A Pragmatic Randomized Controlled Trial to Increase PrEP Uptake for HIV Prevention: 55-Week Results From PrEPChicago. J. Acquir. Immune Defic. Syndr. 2021, 86, 31–37. [Google Scholar] [CrossRef]
- McMahan, V.M.; Martin, A.; Garske, L.; Violette, L.R.; Andrasik, M.P.; Baeten, J.M.; Banta-Green, C.; Stekler, J.D.; McMahan, V.M.; Martin, A.; et al. Development of a Targeted Educational Intervention to Increase Pre-Exposure Prophylaxis Uptake among Cisgender Men and Transgender Individuals Who Have Sex with Men and Use Methamphetamine in Seattle (WA, USA). Sex. Health 2019, 16, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Daughtridge, G.W.; Conyngham, S.C.; Ramirez, N.; Koenig, H.C. I Am Men’s Health: Generating Adherence to HIV Pre-Exposure Prophylaxis (PrEP) in Young Men of Color Who Have Sex with Men. J. Int. Assoc. Provid. AIDS Care (JIAPAC) 2015, 14, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Klassen, B.J.; Lachowsky, N.J.; Lin, S.Y.; Edward, J.B.; Chown, S.A.; Hogg, R.S.; Moore, D.M.; Roth, E.A. Gay Men’s Understanding and Education of New HIV Prevention Technologies in Vancouver, Canada. Qual. Health Res. 2017, 27, 1775–1791. [Google Scholar] [CrossRef] [PubMed]
- Raifman, J.R.G.; Flynn, C.; German, D. Healthcare Provider Contact and Pre-Exposure Prophylaxis in Baltimore Men Who Have Sex With Men. Am. J. Prev. Med. 2017, 52, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, J.; Griffin, M.; Singer, S.N.; Greene, R.E.; Acosta, I.L.Z.; Kaudeyr, S.K.; Kapadia, F.; Halkitis, P.N. Structural Barriers to Pre-Exposure Prophylaxis Use Among Young Sexual Minority Men: The P18 Cohort Study. Curr. HIV Res. 2018, 16, 237–249. [Google Scholar] [CrossRef]
- John, S.A.; Rendina, H.J.; Grov, C.; Parsons, J.T. Home-Based Pre-Exposure Prophylaxis (PrEP) Services for Gay and Bisexual Men: An Opportunity to Address Barriers to PrEP Uptake and Persistence. PLoS ONE 2017, 12, e0189794. [Google Scholar] [CrossRef]
- Anand, T.; Nitpolprasert, C.; Trachunthong, D.; Kerr, S.J.; Janyam, S.; Linjongrat, D.; Hightow-Weidman, L.B.; Phanuphak, P.; Ananworanich, J.; Phanuphak, N.; et al. A Novel Online-to-Offline (O2O) Model for Pre-Exposure Prophylaxis and HIV Testing Scale Up. J. Int. AIDS Soc. 2017, 20, 21326. [Google Scholar] [CrossRef]
- Aloysius, I.; Savage, A.; Zdravkov, J.; Korologou-Linden, R.; Hill, A.; Smith, R.; Houghton-Price, V.; Boffito, M.; Nwokolo, N. InterPrEP. Internet-Based Pre-Exposure Prophylaxis with Generic Tenofovir DF/Emtricitabine in London: An Analysis of Outcomes in 641 Patients. J. Virus Erad. 2017, 3, 218–222. [Google Scholar] [CrossRef]
- Levy, M.E.; Watson, C.C.; Glick, S.N.; Kuo, I.; Wilton, L.; Brewer, R.A.; Fields, S.D.; Criss, V.; Magnus, M. Receipt of HIV Prevention Interventions Is More Common in Community-Based Clinics than in Primary Care or Acute Care Settings for Black Men Who Have Sex with Men in the District of Columbia. AIDS Care 2016, 28, 660–664. [Google Scholar] [CrossRef]
- Eaton, L.A.; Matthews, D.D.; Bukowski, L.A.; Friedman, M.R.; Chandler, C.J.; Whitfield, D.L.; Sang, J.M.; Stall, R.D. Elevated HIV Prevalence and Correlates of PrEP Use among a Community Sample of Black Men Who Have Sex with Men. J. Acquir. Immune Defic. Syndr. 2018, 79, 339–346. [Google Scholar] [CrossRef]
- Doblecki-Lewis, S.; Liu, A.; Feaster, D.; Cohen, S.E.; Cardenas, G.; Bacon, O.; Andrew, E.; Kolber, M.A. Healthcare Access and PrEP Continuation in San Francisco and Miami After the US PrEP Demo Project. J. Acquir. Immune Defic. Syndr. 2017, 74, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Clement, M.E.; Okeke, N.L.; Munn, T.; Hunter, M.; Alexis, K.; Corneli, A.; Seña, A.C.; McGee, K.; McKellar, M.S. Partnerships Between a University-Affiliated Clinic and Community-Based Organizations to Reach Black Men Who Have Sex with Men for PrEP Care. J. Acquir. Immune Defic. Syndr. 2018, 77, e25–e27. [Google Scholar] [CrossRef] [PubMed]
- Arnold, E.A.; Hazelton, P.; Lane, T.; Christopoulos, K.A.; Galindo, G.R.; Steward, W.T.; Morin, S.F. A Qualitative Study of Provider Thoughts on Implementing Pre-Exposure Prophylaxis (PrEP) in Clinical Settings to Prevent HIV Infection. PLoS ONE 2012, 7, e40603. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.J.; Anderson, K.M.; Bangsberg, D.; Toevs, K.; Morrison, D.; Wells, C.; Clark, P.; Nicolaidis, C. Access to HIV Pre-Exposure Prophylaxis in Practice Settings: A Qualitative Study of Sexual and Gender Minority Adults’ Perspectives. J. Gen. Intern. Med. 2019, 34, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.; Guidry, J.A.; Collier, K.L.; Mantell, J.E.; Boccher-Lattimore, D.; Kaighobadi, F.; Sandfort, T.G.M. A Clinical Home for Preexposure Prophylaxis: Diverse Health Care Providers’ Perspectives on the “Purview Paradox”. J. Int. Assoc. Provid. AIDS Care 2016, 15, 59–65. [Google Scholar] [CrossRef]
- World Health Organization. Briefs on Young Key Populations; World Health Organization: Geneva, Switzerland, 2016.
- Stephenson, R.; Darbes, L.A.; Chavanduka, T.; Essack, Z.; van Rooyen, H. HIV Testing, Knowledge and Willingness to Use PrEP Among Partnered Men Who Have Sex with Men in South Africa and Namibia. AIDS Behav. 2021, 25, 1993–2004. [Google Scholar] [CrossRef]
- Coulaud, P.; Sagaon-Teyssier, L.; M’madi Mrenda, B.; Maradan, G.; Mora, M.; Bourrelly, M.; Dembélé Keita, B.; Keita, A.A.; Anoma, C.; Babo Yoro, S.-A.; et al. Interest in HIV Pre-Exposure Prophylaxis in Men Who Have Sex with Men in West Africa (CohMSM ANRS 12324—Expertise France). Trop. Med. Int. Health 2018, 23, 1084–1091. [Google Scholar] [CrossRef]
- Grant, R.M.; Anderson, P.L.; McMahan, V.; Liu, A.; Amico, K.R.; Mehrotra, M.; Hosek, S.; Mosquera, C.; Casapia, M.; Montoya, O.; et al. Uptake of Pre-Exposure Prophylaxis, Sexual Practices, and HIV Incidence in Men and Transgender Women Who Have Sex with Men: A Cohort Study. Lancet Infect. Dis. 2014, 14, 820–829. [Google Scholar] [CrossRef]
- Wahome, E.W.; Graham, S.M.; Thiong’o, A.N.; Mohamed, K.; Oduor, T.; Gichuru, E.; Mwambi, J.; Prins, M.; van der Elst, E.; Sanders, E.J. PrEP Uptake and Adherence in Relation to HIV-1 Incidence among Kenyan Men Who Have Sex with Men. EClinicalMedicine 2020, 26, 100541. [Google Scholar] [CrossRef]
- Hanum, N.; Cambiano, V.; Sewell, J.; Phillips, A.N.; Rodger, A.J.; Speakman, A.; Nwokolo, N.; Asboe, D.; Gilson, R.; Clarke, A.; et al. Use of HIV Pre-Exposure Prophylaxis among Men Who Have Sex with Men in England: Data from the AURAH2 Prospective Study. Lancet Public Health 2020, 5, e501–e511. [Google Scholar] [CrossRef]
- Hammoud, M.A.; Vaccher, S.; Jin, F.; Bourne, A.; Maher, L.; Holt, M.; Bavinton, B.R.; Haire, B.; Degenhardt, L.; Grulich, A.; et al. HIV Pre-Exposure Prophylaxis (PrEP) Uptake among Gay and Bisexual Men in Australia and Factors Associated with the Nonuse of PrEP among Eligible Men: Results from a Prospective Cohort Study. J. Acquir. Immune Defic. Syndr. 2019, 81, e73–e84. [Google Scholar] [CrossRef] [PubMed]
- Gafos, M.; Horne, R.; Nutland, W.; Bell, G.; Rae, C.; Wayal, S.; Rayment, M.; Clarke, A.; Schembri, G.; Gilson, R.; et al. The Context of Sexual Risk Behaviour among Men Who Have Sex with Men Seeking PrEP, and the Impact of PrEP on Sexual Behaviour. AIDS Behav. 2019, 23, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wahome, E.; Graham, S.; Thiong’o, A.; Chirro, O.; Mohamed, K.; Gichuru, E.; Mwambi, J.; Price, M.; Sanders, E.J. Assessment of PrEP Eligibility and Uptake among At-Risk MSM Participating in a HIV-1 Vaccine Feasibility Cohort in Coastal Kenya. Wellcome Open Res. 2019, 4, 138. [Google Scholar] [CrossRef] [PubMed]
- Elsesser, S.A.; Oldenburg, C.E.; Biello, K.B.; Mimiaga, M.J.; Safren, S.A.; Egan, J.E.; Novak, D.S.; Krakower, D.S.; Stall, R.; Mayer, K.H. Seasons of Risk: Anticipated Behavior on Vacation and Interest in Episodic Antiretroviral Pre-Exposure Prophylaxis (PrEP) among a Large National Sample of U.S. Men Who Have Sex with Men (MSM). AIDS Behav. 2016, 20, 1400–1407. [Google Scholar] [CrossRef]
- Ngure, K.; Ortblad, K.F.; Mogere, P.; Bardon, A.R.; Thomas, K.K.; Mangale, D.; Kiptinness, C.; Gakuo, S.; Mbaire, S.; Nyokabi, J.; et al. Efficiency of 6-Month PrEP Dispensing with HIV Self-Testing in Kenya: An Open-Label, Randomised, Non-Inferiority, Implementation Trial. Lancet HIV 2022, 9, e464–e473. [Google Scholar] [CrossRef]
- AVAC about Cabotegravir (CAB-LA). Available online: https://www.prepwatch.org (accessed on 3 July 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Age group (in years) 1 | |
| 18–24 | 314 (48.5) |
| >24 | 275 (42.5) |
| Country of inclusion | |
| Burkina Faso | 128 (19.7) |
| Cote d’Ivoire | 131 (20.3) |
| Mali | 257 (39.7) |
| Togo | 131 (20.3) |
| Employment status 2 | |
| Employed | 283 (43.7) |
| Unemployed | 299 (46.2) |
| Recruitment type | |
| Ex-CohMSM participant | 322 (49.8) |
| New participant | 325 (50.2) |
| Chosen PrEP regimen | |
| Event-driven | 451 (73.1) |
| Daily | 164 (26.6) |
| PrEP adherence 3,* | |
| No PrEP | 111 (21.3) |
| Poor | 27 (5.2) |
| Suboptimal | 84 (16.1) |
| Optimal | 213 (40.8) |
| Contacted PE outside of scheduled visits 4 | |
| Yes | 162 (25.0) |
| No | 405 (62.6) |
| Self-defined sexual orientation 5 | |
| Heterosexual | 15 (2.3) |
| Homosexual/gay | 228 (35.2) |
| Bisexual | 334 (51.6) |
| Self-defined gender identity 6 | |
| Both a man and a woman; more a woman; neither a woman or a man | 229 (35.4) |
| Man or boy | 354 (54.7) |
| Depression score (PHQ-9) | |
| Moderate to high | 295 (45.6) |
| Minimal | 352 (54.4) |
| Had a casual male sexual partner in the previous three months 7 | |
| Yes | 379 (58.6) |
| No | 261 (40.3) |
| Had a casual female sexual partner in the previous three months 8 | |
| Yes | 131 (20.3) |
| No | 510 (78.8) |
| Number of male sexual partners in the previous three months 7 | |
| ≤2 | 416 (64.3) |
| >2 | 224 (34.6) |
| HIV risk perception with stable male partner 9 | |
| No risk | 192 (29.7) |
| At risk | 265 (41.0) |
| No stable partner | 181 (28.0) |
| HIV risk perception with casual male partners 10 | |
| No risk | 96 (14.8) |
| At risk | 281 (43.4) |
| No casual partners | 260 (40.2) |
| Combined prevention use during most recent anal intercourse 11,* | |
| No PrEP & no condom use | 139 (26.7) |
| PrEP use only | 149 (28.6) |
| Condom use only | 50 (9.6) |
| PrEP & condom use | 172 (33) |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variable | n (%) 2 | Mean Follow-Up Time in Months (SD) | HR [95% CI], p-Value | aHR [95% CI], p-Value |
| Age group (in years) | ||||
| 18–24 | 759 (35.9) | 7.9 (7.7) | 1.64 [1.31–2.05], <0.001 | 1.50 [1.17–1.94], 0.002 |
| >24 | 1253 (59.4) | 12 (9.1) | 1 (ref) | 1 (ref) |
| Employment status | ||||
| Employed | 1137 (53.9) | 11.4 (9.3) | 1 (ref) | 1 (ref) |
| Unemployed | 863 (40.9) | 9.0 (8.0) | 1.44 [1.5–1.8], 0.001 | 1.33 [1.03–1.71], 0.027 |
| Chosen PrEP regimen | ||||
| Event-driven | 1356 (64.3) | 11.3 (8.5) | 0.82 [0.64–1.06], 0.125 | |
| Daily | 370 (17.5) | 10.3 (8.6) | 1 (ref) | |
| PrEP adherence | ||||
| No PrEP | 561 (26.6) | 10.8 (8.9) | 1.89 [1.44–2.49], <0.001 | |
| Poor | 114 (5.4) | 11.0 (7.9) | 2.22 [1.32–3.73], 0.003 | |
| Suboptimal | 205 (9.7) | 11.6 (8.3) | 1.53 [1.05–2.23], 0.026 | |
| Optimal | 751 (35.6) | 14.2 (7.6) | 1 (ref) | |
| Contacted PE outside of scheduled visits | ||||
| Yes | 601 (28.4) | 11.4 (9.7) | 0.73 [0.56–0.94], 0.014 | 0.74 [0.57–0.97], 0.032 |
| No | 1349 (63.9) | 9.9 (8.4) | 1 (ref) | 1 (ref) |
| Self-defined sexual orientation | ||||
| Heterosexual | 43 (2.0) | 9.0 (5.5) | 1.9 [0.96–3.75], 0.066 | 1.84 [0.92–3.69], 0.086 |
| Homosexual/gay | 730 (34.6) | 9.8 (8.8) | 1.18 [0.93–1.49], 0.170 | 1.20 [0.94–1.53], 0.149 |
| Bisexual | 1210 (57.4) | 10.8 (9.1) | 1 (ref) | 1 (ref) |
| Self-defined gender identity | ||||
| Both a man and a woman; more a woman; neither a woman or a man | 784 (37.2) | 9.9 (8.2) | 1.29 [1.04–1.61], 0.023 | |
| Man or boy | 1216 (57.6) | 10.5 (9.2) | 1 (ref) | |
| Depression score (PHQ-9) | ||||
| Moderate to high | 954 (45.2) | 9.4 (8.5) | 1.44 [1.04–1.98], 0.029 | 1.63 [1.12–2.38], 0.010 |
| Minimal | 1156 (54.8) | 10.7 (8.9) | 1 (ref) | 1 (ref) |
| Had a casual male sexual partner in the previous three months | ||||
| Yes | 1058 (50.1) | 9.3 (7.8) | 1.33 [1.04–1.69], 0.022 | |
| No | 1058 (49.7) | 10.9 (9.6) | 1 (ref) | |
| Had a casual female sexual partner in the previous three months | ||||
| Yes | 345 (16.4) | 8.7 (8.9) | 1.40 [1.03–1.90] 0.030 | 1.40 [1.00–1.95], 0.047 |
| No | 1762 (83.5) | 10.4 (8.7) | 1 (ref) | 1 (ref) |
| Number of male sexual partners in the previous three months | ||||
| ≤2 | 1497 (70.9) | 10.3 (9.2) | 1 (ref) | 1 (ref) |
| >2 | 609 (28.9) | 9.9 (7.7) | 1.26 [0.99–1.61], 0.058 | 1.37 [1.03–1.83], 0.031 |
| HIV risk perception with stable male partner | ||||
| No risk | 760 (36.0) | 10.2 (9.1) | 1.41 [1.10–1.81], 0.007 | 1.61 [1.23–2.10], <0.001 |
| At risk | 790 (35.4) | 1 (ref) | 1 (ref) | |
| No stable partner | 597 (28.3) | 9.1 (7.7) | 1.04 [0.78–1.39], 0.766 | 1.04 [0.73–1.46], 0.843 |
| HIV risk perception with casual male partners | ||||
| No risk | 321 (15.2) | 8.6 (7.6) | 1.08 [0.78–1.49], 0.639 | |
| At risk | 728 (34.5) | 9.7(7.8) | 1 (ref) | |
| No casual partners | 1055 (50.0) | 10.9 (9.5) | 0.79 [0.60–1.03], 0.083 | |
| Combined prevention use during most recent anal intercourse | ||||
| No PrEP & no condom use | 801 (37.9) | 8.35 (9.2) | 2.25 [1.71–2.96], <0.001 | 2.56 [1.92–3.42], <0.001 |
| PrEP use only | 367 (17.4) | 13.1 (7.2) | 1.32 [0.95–1.84], 0.100 | 1.50 [1.05–2.13], 0.025 |
| Condom use only | 267 (12.7) | 5.6 (6.8) | 2.21 [1.52–3.23], <0.001 | 2.19 [1.47–3.25], <0.001 |
| PrEP & condom use | 635 (30.1) | 13.7 (8.1) | 1 (ref) | 1 (ref) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eubanks, A.; Coulibaly, B.; Keita, B.D.; Anoma, C.; Dah, T.T.E.; Mensah, E.; Maradan, G.; Bourrelly, M.; Mora, M.; Riegel, L.; et al. Loss to Follow-Up from HIV Pre-Exposure Prophylaxis Care in Men Who Have Sex with Men in West Africa. Viruses 2022, 14, 2380. https://doi.org/10.3390/v14112380
Eubanks A, Coulibaly B, Keita BD, Anoma C, Dah TTE, Mensah E, Maradan G, Bourrelly M, Mora M, Riegel L, et al. Loss to Follow-Up from HIV Pre-Exposure Prophylaxis Care in Men Who Have Sex with Men in West Africa. Viruses. 2022; 14(11):2380. https://doi.org/10.3390/v14112380
Chicago/Turabian StyleEubanks, August, Bakary Coulibaly, Bintou Dembélé Keita, Camille Anoma, Ter Tiero Elias Dah, Ephrem Mensah, Gwenaëlle Maradan, Michel Bourrelly, Marion Mora, Lucas Riegel, and et al. 2022. "Loss to Follow-Up from HIV Pre-Exposure Prophylaxis Care in Men Who Have Sex with Men in West Africa" Viruses 14, no. 11: 2380. https://doi.org/10.3390/v14112380
APA StyleEubanks, A., Coulibaly, B., Keita, B. D., Anoma, C., Dah, T. T. E., Mensah, E., Maradan, G., Bourrelly, M., Mora, M., Riegel, L., Rojas Castro, D., Yaya, I., Spire, B., Laurent, C., Sagaon-Teyssier, L., & the CohMSM-PrEP Study Group. (2022). Loss to Follow-Up from HIV Pre-Exposure Prophylaxis Care in Men Who Have Sex with Men in West Africa. Viruses, 14(11), 2380. https://doi.org/10.3390/v14112380