

Isolation and Genotyping of Adenoviruses from Wastewater and Diarrheal Samples in Egypt from 2016 to 2020

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Fecal Samples Processing
2.3. Environmental Samples Collection
2.4. Sewage Samples Preparation
2.5. Detection and Genotyping of Adenoviruses by Nested PCR
2.6. Isolation of Adenoviruses Using HEp-2 Cell Line
2.7. Amplification Using qPCR
2.8. Sequencing of PCRproducts
2.9. Nucleotide Sequence Accession Numbers
2.10. Statistical Analysis
3. Results
3.1. Incidence of Adenovirus and Viral Load Analysis in Clinical Samples
3.2. Incidence of Adenovirus and Viral Load in Environmental Samples
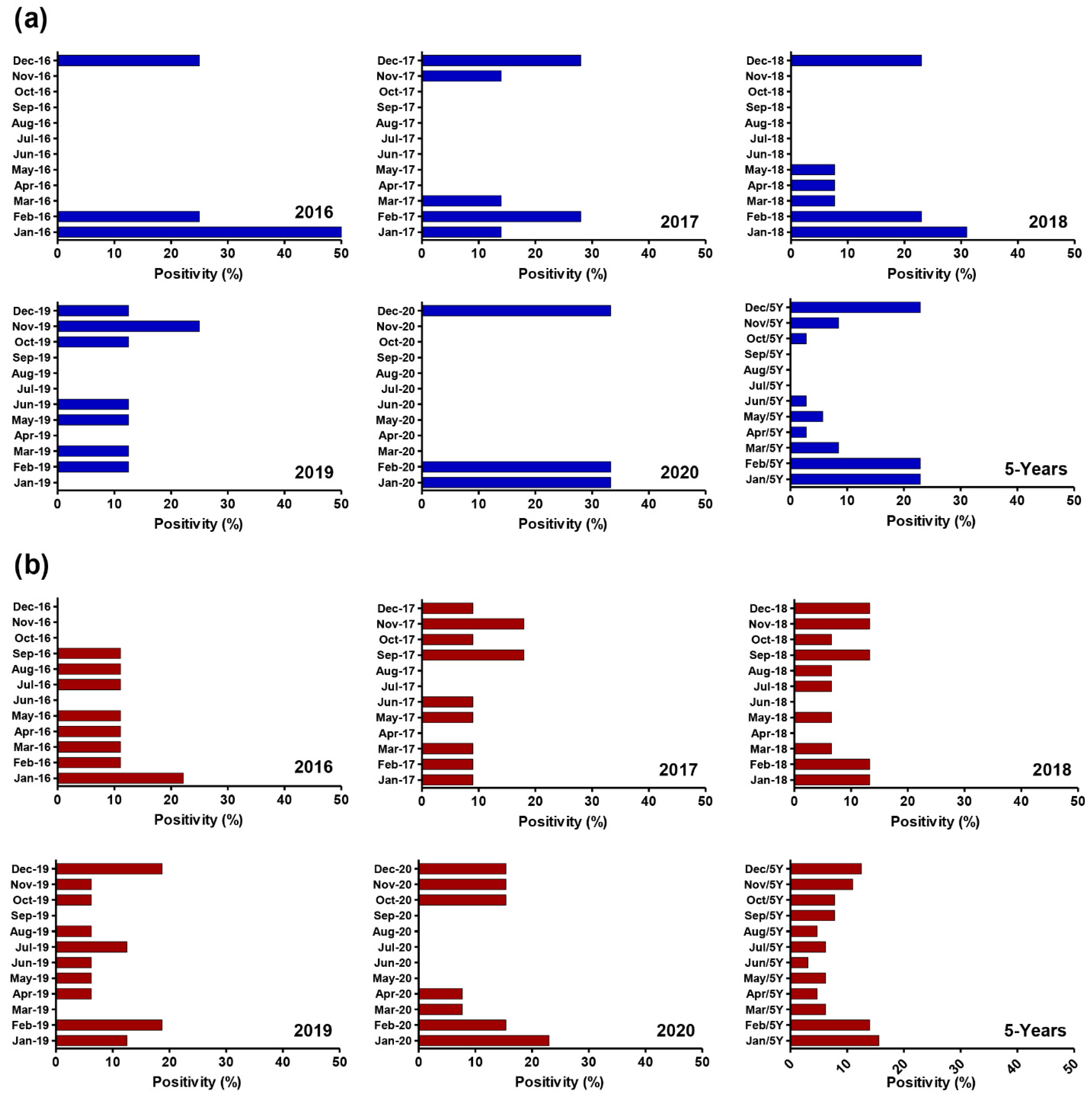
3.3. Comprehensive Distribution of Adenoviruses in Clinical and Environmental Samples on a Monthly Basis
3.4. Comprehensive Distribution of Adenovirus Genotypes in Clinical and Environmental Samples
3.5. Specific Cell Culture Isolation of Adenovirus-Positive Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mostafa-Hedeab, G.; Allayeh, A.K.; Elhady, H.A.; Eledrdery, A.Y.; Mraheil, M.A.; Mostafa, A. Viral eco-genomic tools: Development and implementation for aquatic biomonitoring. Int. J. Environ. Res. Public Health 2022, 19, 7707. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Wang, Z.; Zhang, G.; Sai, L. Molecular and epidemiological characterization of human adenoviruses infection among children with acute diarrhea in shandong province, china. Virol. J. 2021, 18, 195. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.P., 3rd; Kajon, A.E. Adenovirus: Epidemiology, global spread of novel serotypes, and advances in treatment and prevention. Semin. Respir. Crit. Care Med. 2016, 37, 586–602. [Google Scholar]
- Gasparinho, C.; Mirante, M.C.; Centeno-Lima, S.; Istrate, C.; Mayer, A.C.; Tavira, L.; Nery, S.V.; Brito, M. Etiology of diarrhea in children younger than 5 years attending the bengo general hospital in angola. Pediatr. Infect. Dis. J. 2016, 35, e28–e34. [Google Scholar] [CrossRef] [PubMed]
- Primo, D.; Pacheco, G.T.; Timenetsky, M.; Luchs, A. Surveillance and molecular characterization of human adenovirus in patients with acute gastroenteritis in the era of rotavirus vaccine, brazil, 2012–2017. J. Clin. Virol. 2018, 109, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Benkő, M.; Aoki, K.; Arnberg, N.; Davison, A.J.; Echavarría, M.; Hess, M.; Jones, M.S.; Kaján, G.L.; Kajon, A.E.; Mittal, S.K.; et al. Ictv virus taxonomy profile: Adenoviridae 2022. J. Gen. Virol. 2022, 103, 001721. [Google Scholar] [CrossRef]
- Fletcher, S.M.; McLaws, M.L.; Ellis, J.T. Prevalence of gastrointestinal pathogens in developed and developing countries: Systematic review and meta-analysis. J. Public Health Res. 2013, 2, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Harb, A.; Abraham, S.; Rusdi, B.; Laird, T.; O’Dea, M.; Habib, I. Molecular detection and epidemiological features of selected bacterial, viral, and parasitic enteropathogens in stool specimens from children with acute diarrhea in thi-qar governorate, iraq. Int. J. Environ. Res. Public Health 2019, 16, 1573. [Google Scholar] [CrossRef] [PubMed]
- Kumthip, K.; Khamrin, P.; Ushijima, H.; Maneekarn, N. Enteric and non-enteric adenoviruses associated with acute gastroenteritis in pediatric patients in thailand, 2011 to 2017. PLoS ONE 2019, 14, e0220263. [Google Scholar] [CrossRef]
- Mousavi Nasab, S.D.; Zali, F.; Kaghazian, H.; Aghasadeghi, M.R.; Mardani, R.; Gachkar, L.; Ahmadi Vasmehjani, A.; Ahmadi, N.; Ghasemzadeh, A. Prevalence of astrovirus, adenovirus, and sapovirus infections among iranian children with acute gastroenteritis. Gastroenterol. Hepatol. Bed. Bench. 2020, 13, S122–S127. [Google Scholar]
- Qiu, F.-Z.; Shen, X.-X.; Li, G.-X.; Zhao, L.; Chen, C.; Duan, S.-X.; Guo, J.-Y.; Zhao, M.-C.; Yan, T.-F.; Qi, J.-J.; et al. Adenovirus associated with acute diarrhea: A case-control study. BMC Infect. Dis. 2018, 18, 450. [Google Scholar] [CrossRef] [PubMed]
- Kamal Allayeh, A.; Mostafa El Baz, R.; Mohamed Saeed, N.; El Sayed Osman, M. Detection and genotyping of viral gastroenteritis in hospitalized children below five years old in cairo, egypt. Arch. Pediatric Infect. Dis. 2018, 6, e60288. [Google Scholar] [CrossRef]
- Gad, M.; Allayeh, A.; Elmahdy, E.M.; Shaheen, M.N.F.; Rizk, N.M.; Al-Herrawy, A.; Saleh, F.E.-Z.R.; Marouf, M.A. Genotyping and interaction-reality of acanthamoeba, enteric adenovirus and rotavirus in drinking water, egypt. Egypt. J. Aquat. Biol. Fish. 2019, 23, 65–79. [Google Scholar] [CrossRef]
- Elmahdy, E.M.; Ahmed, N.I.; Shaheen, M.N.F.; Mohamed, E.B.; Loutfy, S.A. Molecular detection of human adenovirus in urban wastewater in egypt and among children suffering from acute gastroenteritis. J. Water Health 2019, 17, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Demian, P.N.; Horton, K.C.; Kajon, A.; Siam, R.; Hasanin, A.M.N.; Elgohary Sheta, A.; Cornelius, C.; Gaynor, A.M. Molecular identification of adenoviruses associated with respiratory infection in egypt from 2003 to 2010. BMC Infect. Dis. 2014, 14, 50. [Google Scholar] [CrossRef]
- Patel, M.M.; Widdowson, M.A.; Glass, R.I.; Akazawa, K.; Vinje, J.; Parashar, U.D. Systematic literature review of role of noroviruses in sporadic gastroenteritis. Emerg. Infect. Dis. 2008, 14, 1224–1231. [Google Scholar] [CrossRef]
- Kreidieh, K.; Charide, R.; Dbaibo, G.; Melhem, N.M. The epidemiology of norovirus in the middle east and north africa (mena) region: A systematic review. Virol. J. 2017, 14, 220. [Google Scholar] [CrossRef]
- Fathy, M.; Amer, R.m.; Almalky, M.A.; El Gebaly, S. Genotyping and severity of rotavirus infection among infants and children with acute diarrhea. Egypt. J. Hosp. Med. 2021, 82, 205–211. [Google Scholar] [CrossRef]
- Williams, F.P.; Stetler, R.E.; Safferman, R.S. Usepa Manual of Methods for Virology; EPA/600/4-84/013 (N16); U.S. Environmental Protection Agency: Washington, DC, USA, 2001.
- Clesceri, L.S.; Greenberg, A.E.; Eaton, A.D. Standard Methods for the Examination of Water and Wastewater, 20th ed.; APHA American Public Health Association: Washington, DC, USA, 1998. [Google Scholar]
- Katzenelson, E.; Fattal, B.; Hostovesky, T. Organic flocculation: An efficient second-step concentration method for the detection of viruses in tap water. Appl. Environ. Microbiol. 1976, 32, 638–639. [Google Scholar] [CrossRef] [PubMed]
- Puig, M.; Jofre, J.; Lucena, F.; Allard, A.; Wadell, G.; Girones, R. Detection of adenoviruses and enteroviruses in polluted waters by nested pcr amplification. Appl. Environ. Microbiol. 1994, 60, 2963–2970. [Google Scholar] [CrossRef] [PubMed]
- Pring-Akerblom, P.; Adrian, T. Type- and group-specific polymerase chain reaction for adenovirus detection. Res. Virol. 1994, 145, 25–35. [Google Scholar] [CrossRef]
- Yan, H.; Nguyen, T.A.; Phan, T.G.; Okitsu, S.; Li, Y.; Ushijima, H. Development of rt-multiplex pcr assay for detection of adenovirus and group a and c rotaviruses in diarrheal fecal specimens from children in china. Kansenshogaku Zasshi 2004, 78, 699–709. [Google Scholar] [CrossRef]
- Audu, R.; Omilabu, A.S.; Peenze, I.; Steele, D.A. Isolation and identification of adenovirus recovered from the stool of children with diarrhoea in lagos, nigeria. Afr. J Health Sci. 2002, 9, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Xagoraraki, I.; Kuo, D.H.; Wong, K.; Wong, M.; Rose, J.B. Occurrence of human adenoviruses at two recreational beaches of the great lakes. Appl. Environ. Microbiol. 2007, 73, 7874–7881. [Google Scholar] [CrossRef]
- Verma, H.; Chitambar, S.D.; Varanasi, G. Identification and characterization of enteric adenoviruses in infants and children hospitalized for acute gastroenteritis. J. Med. Virol. 2009, 81, 60–64. [Google Scholar] [CrossRef]
- Silva, H.D.; García-Zapata, M.T.A.; Anunciação, C.E. Why the use of adenoviruses as water quality virologic marker? Food Environ. Virol. 2011, 3, 138–140. [Google Scholar] [CrossRef]
- Nakanishi, K.; Tsugawa, T.; Honma, S.; Nakata, S.; Tatsumi, M.; Yoto, Y.; Tsutsumi, H. Detection of enteric viruses in rectal swabs from children with acute gastroenteritis attending the pediatric outpatient clinics in sapporo, japan. J. Clin. Virol. 2009, 46, 94–97. [Google Scholar] [CrossRef]
- Dey, S.K.; Hoq, I.; Okitsu, S.; Hayakawa, S.; Ushijima, H. Prevalence, seasonality, and peak age of infection of enteric adenoviruses in japan, 1995–2009. Epidemiol. Infect. 2013, 141, 958–960. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Qian, Y.; Zhang, Y.; Deng, J.; Jia, L.; Dong, H. Adenoviruses associated with acute diarrhea in children in beijing, china. PLoS ONE 2014, 9, e88791. [Google Scholar] [CrossRef]
- Banerjee, A.; De, P.; Manna, B.; Chawla-Sarkar, M. Molecular characterization of enteric adenovirus genotypes 40 and 41 identified in children with acute gastroenteritis in kolkata, india during 2013–2014. J. Med. Virol. 2017, 89, 606–614. [Google Scholar] [CrossRef]
- Sun, S.; Shi, Y.; Tong, H.-I.; Kang, W.; Wang, Z.; Allmann, E.; Lu, Y. Effective concentration, recovery, and detection of infectious adenoviruses from environmental waters. J. Virol. Methods 2016, 229, 78–85. [Google Scholar] [CrossRef]
- Wieczorek, M.; Krzysztoszek, A.; Witek, A. Species-specific identification of human adenoviruses in sewage. Pol. J. Microbiol. 2015, 64, 23–28. [Google Scholar] [CrossRef]
- Afrad, M.H.; Avzun, T.; Haque, J.; Haque, W.; Hossain, M.E.; Rahman, A.R.; Ahmed, S.; Faruque, A.S.G.; Rahman, M.Z.; Rahman, M. Detection of enteric- and non-enteric adenoviruses in gastroenteritis patients, bangladesh, 2012–2015. J. Med. Virol. 2018, 90, 677–684. [Google Scholar] [CrossRef]
- Lim, M.C.; Wang, Y.F.; Huang, S.W.; Yang, J.Y.; Wang, J.R. High incidence of mammalian orthoreovirus identified by environmental surveillance in taiwan. PLoS ONE 2015, 10, e0142745. [Google Scholar] [CrossRef]
- Amdiouni, H.; Faouzi, A.; Fariat, N.; Hassar, M.; Soukri, A.; Nourlil, J. Detection and molecular identification of human adenoviruses and enteroviruses in wastewater from morocco. Lett. Appl. Microbiol. 2012, 54, 359–366. [Google Scholar] [CrossRef]
- Rigotto, C.; Victoria, M.; Moresco, V.; Kolesnikovas, C.K.; Corrêa, A.A.; Souza, D.S.; Miagostovich, M.P.; Simões, C.M.; Barardi, C.R. Assessment of adenovirus, hepatitis a virus and rotavirus presence in environmental samples in florianopolis, south brazil. J. Appl. Microbiol. 2010, 109, 1979–1987. [Google Scholar] [CrossRef]
- Adefisoye, M.A.; Nwodo, U.U.; Green, E.; Okoh, A.I. Quantitative pcr detection and characterisation of human adenovirus, rotavirus and hepatitis a virus in discharged effluents of two wastewater treatment facilities in the eastern cape, south africa. Food Environ. Virol. 2016, 8, 262–274. [Google Scholar] [CrossRef]
- Grøndahl-Rosado, R.C.; Yarovitsyna, E.; Trettenes, E.; Myrmel, M.; Robertson, L.J. A one year study on the concentrations of norovirus and enteric adenoviruses in wastewater and a surface drinking water source in norway. Food Environ. Virol. 2014, 6, 232–245. [Google Scholar] [CrossRef]
- Moyo, S.J.; Hanevik, K.; Blomberg, B.; Kommedal, O.; Nordbø, S.A.; Maselle, S.; Langeland, N. Prevalence and molecular characterisation of human adenovirus in diarrhoeic children in tanzania; a case control study. BMC Infect. Dis. 2014, 14, 666. [Google Scholar] [CrossRef]
- Perron-Henry, D.M.; Herrmann, J.E.; Blacklow, N.R. Isolation and propagation of enteric adenoviruses in hep-2 cells. J. Clin. Microbiol. 1988, 26, 1445–1447. [Google Scholar] [CrossRef]
- Nour, I.; Hanif, A.; Zakri, A.M.; Al-Ashkar, I.; Alhetheel, A.; Eifan, S. Human adenovirus molecular characterization in various water environments and seasonal impacts in riyadh, saudi arabia. Int. J. Environ. Res. Public Health 2021, 18, 4773. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Year | No. of Samples | Positive Samples Number, (%) | % of Positive Samples | |
|---|---|---|---|---|
| Female | Male | |||
| 2016 | 69 | 4 (5.8) | 2/30 (6.6) | 2/39 (5.1) |
| 2017 | 90 | 7 (7.7) | 1/38 (2.6) | 6/52 (11.5) |
| 2018 | 101 | 13 (12.8) | 5/47 (10.6) | 8/54 (14.8) |
| 2019 | 110 | 8 (7.3) | 3/41 (7.3) | 5/69 (7.2) |
| 2020 | 77 | 3 (3.9) | 0/33 (0) | 3/44 (6.8) |
| 5 years | 447 | 35 (7.83) | 11/189 (5.8) | 24/258 (9.3) |
| Age (Months) | 2016 | 2017 | 2018 | 2019 | 2020 | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M * | F ** | M | F | M | F | M | F | M | F | ||
| <12 | 2/12 (16.6) | 1/10 (10) | 3/21 (25) | 1/17 (5.8) | 2/16 (12.5) | 2/15 (13.3) | 1/30 (3.3) | 1/12 (8.3) | 2/21 (9.5) | 0/3 (0) | 15/157 (9.5) |
| 12 ≤ 24 | 0/11 (0) | 1/8 (12.5) | 1/12 (8.3) | 0/9 (0) | 3/11 (27.2) | 3/13 (23) | 1/14 (7.1) | 2/9 (22) | 1/20 (5) | 0/21 (0) | 12/128 (9.3) |
| 24 ≤ 36 | 0/10 (0) | 0/5 (0) | 1/8 (12.5) | 0/12 (0) | 1/14 (7.1) | 0/7 (0) | 2/9 (22) | 0/3 (0) | NA | 0/5 (0) | 4/73 (5.4) |
| 36 ≤ 48 | 0/3 (0) | 0/7 (0) | 1/11 (9) | NA | 1/7 (14.2) | 0/5 (0) | 1/7 (14) | 0/5 | 0/3 (0) | 0/2 (0) | 3/50 (6) |
| 48 ≤ 60 | 0/3 (0) | NA | NA | NA | 1/6 (16.6) | 0/7 (0) | 0/9 (0) | 0/12 (0) | NA | 0/2 (0) | 1/39 (2.5) |
| Total | 2/39 (5.2) | 2/30 (6.6) | 6/52 (11.5) | 1/38 (2.6) | 8/54 (14.8) | 5/47 (10.6) | 5/69 (7.2) | 3/41 (7.3) | 3/44 (6.8) | 0/33 (0) | 35/447 (7.8) |
| Year | No. of Samples | Positive Samples Number, (%) | % of Positive Samples | |
|---|---|---|---|---|
| Inlet | Outlet | |||
| 2016 | 24 | 9 (37.5) | 7/12 (58.3) | 2/12 (16.6) |
| 2017 | 24 | 11 (45.8) | 6/12 (50) | 5/12 (41.6) |
| 2018 | 24 | 15 (62.5) | 11/12 (91.6) | 4/12 (33.3) |
| 2019 | 24 | 16 (66.6) | 9/12 (75) | 7/12 (58.3) |
| 2020 | 24 | 13 (54.1) | 10/12 (83.3) | 3/12 (25) |
| 5 years | 120 | 64 (53.3) | 43/60 (71.7) | 21/60 (35) |
| Genotypes | 2016 | 2017 | 2018 | 2019 | 2020 | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Raw | Treated | Raw | Treated | Raw | Treated | Raw | Treated | Raw | Treated | ||
| Adenovirus-41 | 4 | 2 | 3 | 3 | 5 | 2 | 6 | 5 | 8 | 3 | 41 |
| Adenovirus-40 | 2 | 0 | 1 | 1 | 3 | 2 | 2 | 2 | 1 | 0 | 14 |
| Adenovirus-6 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 5 |
| Adenovirus-2 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| Adenovirus-1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 3 |
| Total | 7 | 2 | 6 | 5 | 11 | 4 | 9 | 7 | 10 | 3 | 64 |
| Strain Name | Source of Isolation | Year of Collection | Titration by qPCR | Isolated Genotype | Isolation Passages | ||
|---|---|---|---|---|---|---|---|
| 1st Passage | 2nd Passage | 3rd Passage | |||||
| AMDT-148 | Sewage, Inlet | 2017 | 2.5 × 104 | Ad-41 | * | ** | ** |
| AMDT-149 | Stool | 2018 | 1.4 × 106 | Ad-41 | ** | ** | ** |
| AMDT-021 | Stool | 2019 | 2.7 × 105 | Ad-40 | * | ** | ** |
| AMDT-014 | Sewage, Inlet | 2018 | 3.8 × 103 | Ad-41 | * | * | ** |
| AMDT-057 | Stool | 2019 | 1.6 × 104 | Ad-40 | * | * | ** |
| AMDT-201 | Stool | 2019 | 1.1 × 106 | Ad-41 | ** | ** | ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allayeh, A.K.; Al-Daim, S.A.; Ahmed, N.; El-Gayar, M.; Mostafa, A. Isolation and Genotyping of Adenoviruses from Wastewater and Diarrheal Samples in Egypt from 2016 to 2020. Viruses 2022, 14, 2192. https://doi.org/10.3390/v14102192
Allayeh AK, Al-Daim SA, Ahmed N, El-Gayar M, Mostafa A. Isolation and Genotyping of Adenoviruses from Wastewater and Diarrheal Samples in Egypt from 2016 to 2020. Viruses. 2022; 14(10):2192. https://doi.org/10.3390/v14102192
Chicago/Turabian StyleAllayeh, Abdou Kamal, Sahar Abd Al-Daim, Nehal Ahmed, Mona El-Gayar, and Ahmed Mostafa. 2022. "Isolation and Genotyping of Adenoviruses from Wastewater and Diarrheal Samples in Egypt from 2016 to 2020" Viruses 14, no. 10: 2192. https://doi.org/10.3390/v14102192
APA StyleAllayeh, A. K., Al-Daim, S. A., Ahmed, N., El-Gayar, M., & Mostafa, A. (2022). Isolation and Genotyping of Adenoviruses from Wastewater and Diarrheal Samples in Egypt from 2016 to 2020. Viruses, 14(10), 2192. https://doi.org/10.3390/v14102192