
Evaluation of Production Lots of a Rapid Point-of-Care Lateral Flow Serological Test Intended for Identification of IgM and IgG against the N-Terminal Part of the Spike Protein (S1) of SARS-CoV-2


Abstract
1. Introduction
2. Materials and Methods
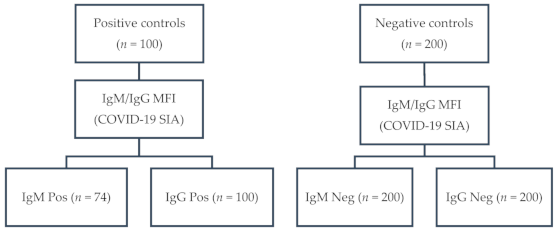
2.1. Serum Samples
2.2. Reference Method
2.3. Index Test
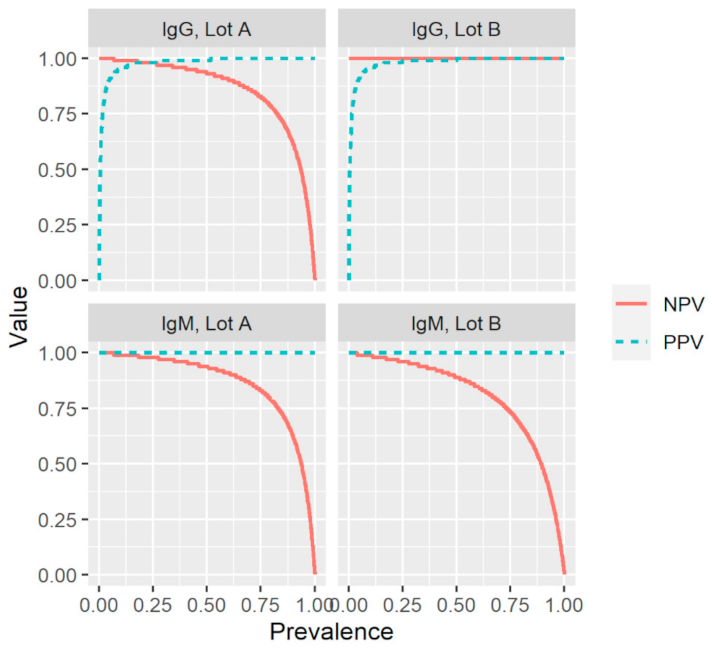
2.4. Analysis
3. Results
3.1. Selected Serum Samples
3.2. Index Test
3.3. Sensitivity, Specificity, and Predictive Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worldometer. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 7 March 2021).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel Coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Pollan, M.; Perez-Gomez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernan, M.A.; Perez-Olmeda, M.; Sanmartin, J.L.; Fernandez-Garcia, A.; Cruz, I.; Fernandez de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 181, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor recognition by the novel coronavirus from Wuhan: An analysis based on decade-long structural studies of SARS coronavirus. J. Virol. 2020, 94, e00127-20. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Ye, G.; Shi, K.; Wan, Y.; Luo, C.; Aihara, H.; Geng, Q.; Auerbach, A.; Li, F. Structural basis of receptor recognition by SARS-CoV-2. Nature 2020, 581, 221–224. [Google Scholar] [CrossRef]
- Wu, F.; Liu, M.; Wang, A.; Lu, L.; Wang, Q.; Gu, C.; Chen, J.; Wu, Y.; Xia, S.; Ling, Y.; et al. Evaluating the association of clinical characteristics with neutralizing antibody levels in patients who have recovered from mild COVID-19 in Shanghai, China. JAMA Intern. Med. 2020, 180, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, T.; Kolstad, L.; Lindahl, J.F.; Albinsson, B.; Bergqvist, A.; Rönnberg, B.; Lundkvist, Å. Diagnostic potential of a Luminex-based coronavirus disease 2019 suspension immunoassay (COVID-19 SIA) for the detection of antibodies against SARS-CoV-2. Viruses 2021, 13, 993. [Google Scholar] [CrossRef]
- United States Food and Drug Administration (FDA). Serology Test Evaluation Report for “COVID-19 IgG/IgM Rapid Test Cassette” from Healgen. Available online: https://www.accessdata.fda.gov/cdrh_docs/presentations/maf/maf3247-a001.pdf (accessed on 21 June 2020).
- Folkhälsomyndigheten (Swedish Public Health Agency). Vägledning för antikroppspåvisning vid covid-19. Version 6. 2021. 21043. Available online: https://www.folkhalsomyndigheten.se/contentassets/2c3d8e40926e4bcc942aa640922bb758/vagledning-antikroppspavisning.pdf (accessed on 7 March 2021).
- Wickham, H. Ggplot2 Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009. [Google Scholar]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef] [PubMed]
- Tollånes, M.; Abildsnes, E.; Baevre-Jensen, R.; Kierkegaard, H.; Jenum, P.; Breivik, A.; Sandberg, S. Report 2: Evaluation of 17 Rapid Tests for Detection of Antibodies against SARS-CoV-2; NOKLUS: 2020. Available online: https://www.noklus.no/media/4k3hjwdh/report_2_covid19_rapidtests_noklus_2020.pdf (accessed on 7 March 2021).
- Grandjean, L.; Saso, A.; Ortiz, A.; Lam, T.; Hatcher, J.; Thistlethwaite, R.; Harris, M.; Best, T.; Johnson, M.; Wagstaffe, H.; et al. Humoral response dynamics following infection with SARS-CoV-2. medRxiv 2020. [Google Scholar]
- Huang, J.; Mao, T.; Li, S.; Wu, L.; Xu, X.; Li, H.; Xu, C.; Su, F.; Dai, J.; Shi, J.; et al. Long period dynamics of viral load and antibodies for SARS-CoV-2 infection: An observational cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Fenwick, C.; Croxatto, A.; Coste, A.; Pojer, F.; Andre, C.; Pellaton, C.; Farina, A.; Campos, J.; Hacker, D.; Lau, K.; et al. Changes in SARS-CoV-2 antibody responses impact the estimates of infections in population-based seroprevalence studies. J. Virol. 2021, 95, e01828-20. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Index Test | ||||||
|---|---|---|---|---|---|---|
| Lot A | Lot B | |||||
| Reference Method | IgM Positive | IgM Negative | Total | IgM Positive | IgM Negative | Total |
| IgM Positive | 69 | 5 | 74 | 65 | 9 | 74 |
| IgM Negative | 0 | 200 | 200 | 0 | 200 | 200 |
| Total | 69 | 205 | 274 | 65 | 209 | 274 |
| Index Test | ||||||
|---|---|---|---|---|---|---|
| Lot A | Lot B | |||||
| Reference Method | IgG Positive | IgG Negative | Total | IgG Positive | IgG Negative | Total |
| IgG Positive | 93 | 7 | 100 | 100 | 0 | 100 |
| IgG Negative | 1 | 199 | 200 | 1 | 199 | 200 |
| Total | 94 | 206 | 300 | 101 | 199 | 300 |
| Index Test Performance | ||||
|---|---|---|---|---|
| IgM | IgG | |||
| n | % (95% CI) | n | % (95% CI) | |
| Lot A | ||||
| Sensitivity | 69/74 | 93.2 (85.1–97.1) | 93/100 | 93.0 (86.3–96.6) |
| Specificity | 200/200 | 100 (98.1–100) | 199/200 | 99.5 (97.2–99.9) |
| PPV | 69/69 | 100 (94.7–100) | 93/94 | 98.9 (94.2–99.8) |
| NPV | 200/205 | 97.6 (94.4–99.0) | 199/206 | 96.6 (93.2–98.3) |
| Lot B | ||||
| Sensitivity | 65/74 | 87.8 (78.5–93.5) | 100/100 | 100 (96.3–100) |
| Specificity | 200/200 | 100 (98.1–100) | 199/200 | 99.5 (97.2–99.9) |
| PPV | 65/65 | 100 (94.4–100) | 100/101 | 99.0 (94.6–99.8) |
| NPV | 200/209 | 95.7 (92.0–97.7) | 199/199 | 100 (98.1–100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoffman, T.; Kolstad, L.; Rönnberg, B.; Lundkvist, Å. Evaluation of Production Lots of a Rapid Point-of-Care Lateral Flow Serological Test Intended for Identification of IgM and IgG against the N-Terminal Part of the Spike Protein (S1) of SARS-CoV-2. Viruses 2021, 13, 1043. https://doi.org/10.3390/v13061043
Hoffman T, Kolstad L, Rönnberg B, Lundkvist Å. Evaluation of Production Lots of a Rapid Point-of-Care Lateral Flow Serological Test Intended for Identification of IgM and IgG against the N-Terminal Part of the Spike Protein (S1) of SARS-CoV-2. Viruses. 2021; 13(6):1043. https://doi.org/10.3390/v13061043
Chicago/Turabian StyleHoffman, Tove, Linda Kolstad, Bengt Rönnberg, and Åke Lundkvist. 2021. "Evaluation of Production Lots of a Rapid Point-of-Care Lateral Flow Serological Test Intended for Identification of IgM and IgG against the N-Terminal Part of the Spike Protein (S1) of SARS-CoV-2" Viruses 13, no. 6: 1043. https://doi.org/10.3390/v13061043
APA StyleHoffman, T., Kolstad, L., Rönnberg, B., & Lundkvist, Å. (2021). Evaluation of Production Lots of a Rapid Point-of-Care Lateral Flow Serological Test Intended for Identification of IgM and IgG against the N-Terminal Part of the Spike Protein (S1) of SARS-CoV-2. Viruses, 13(6), 1043. https://doi.org/10.3390/v13061043