Re-Emergence of Yellow Fever in Brazil during 2016–2019: Challenges, Lessons Learned, and Perspectives



 , ,
, ,  , , , ,
, , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
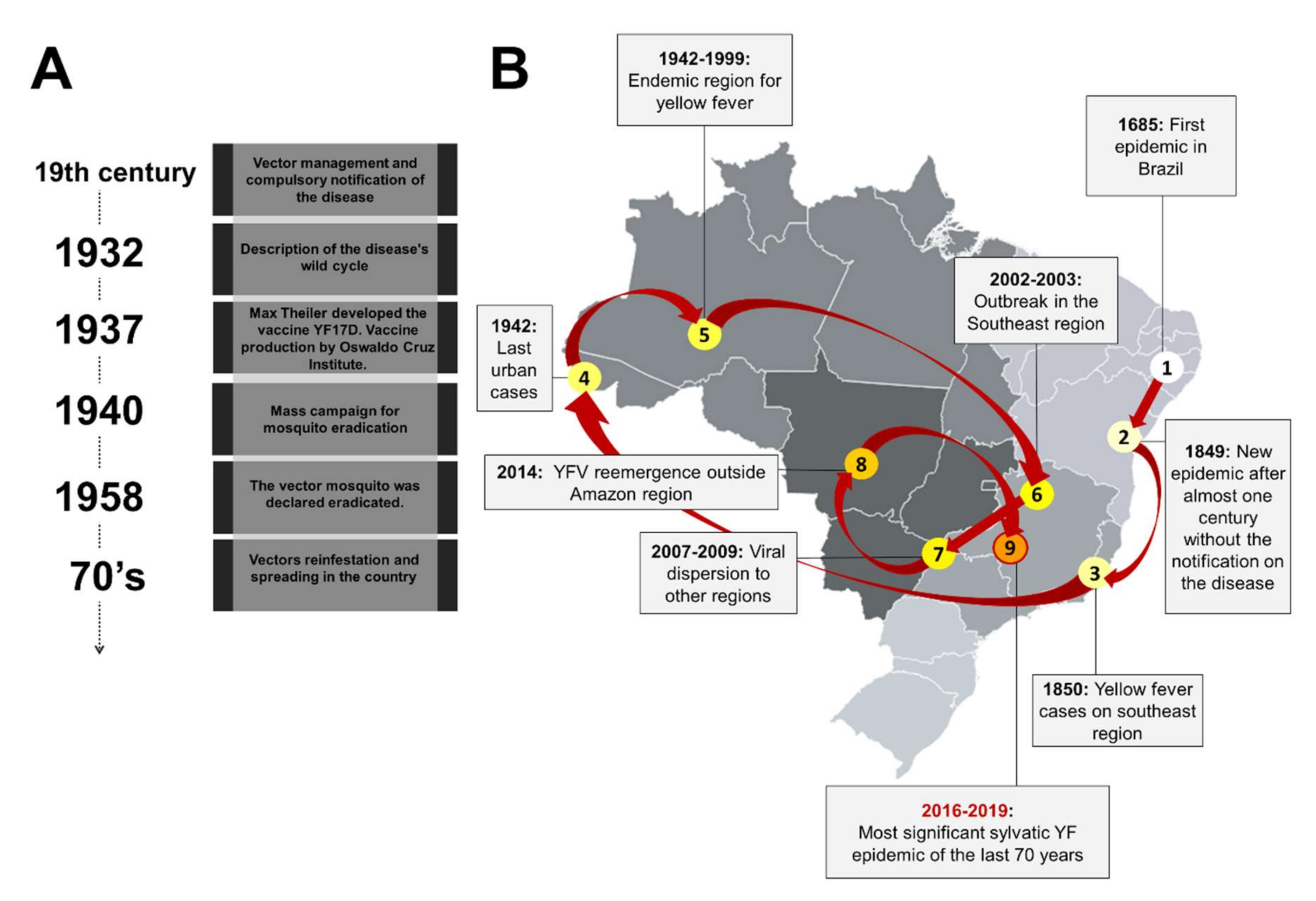
2. A Brief History of Yellow Fever in Brazil
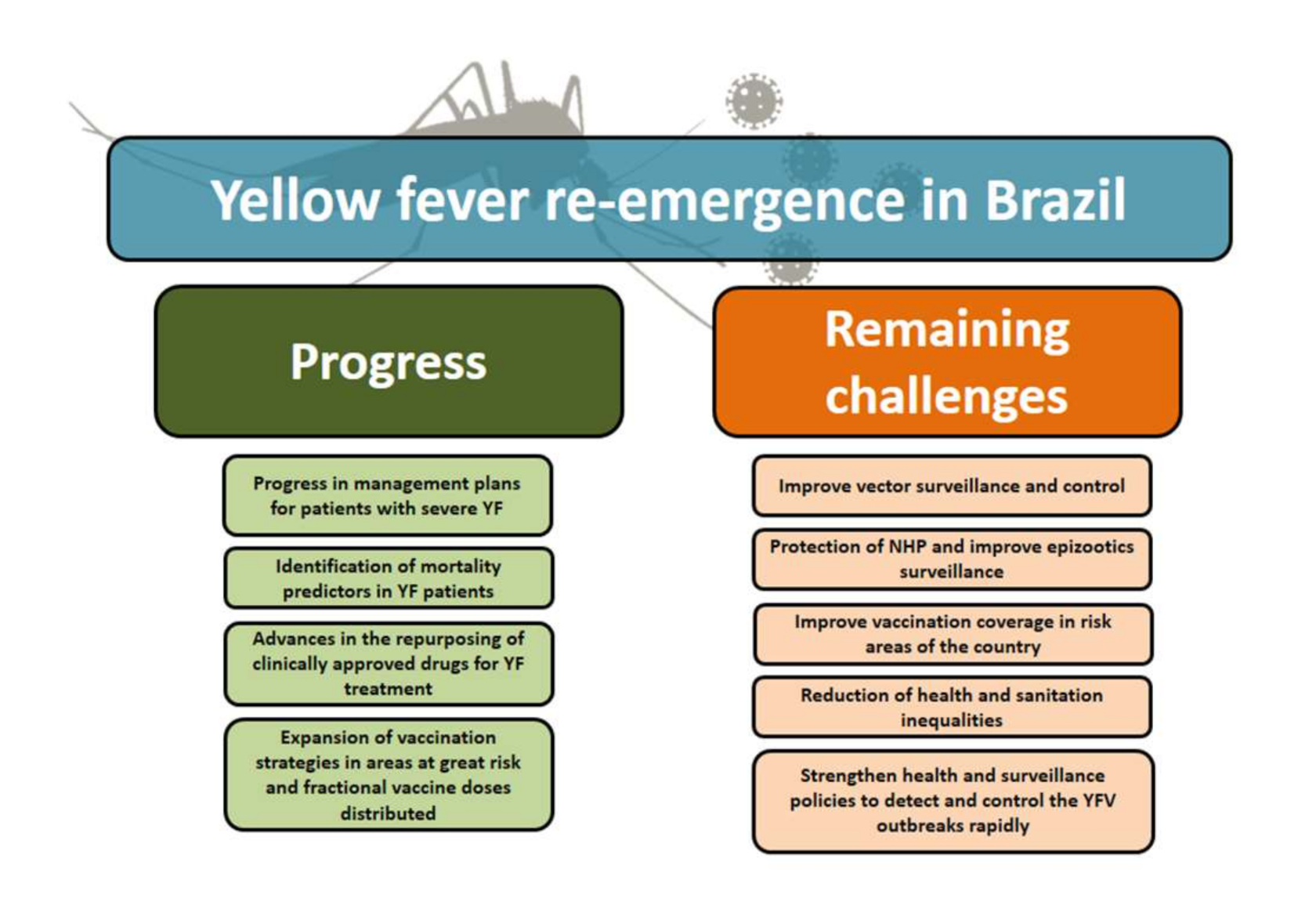
3. Challenges and Lessons Learned
4. Progress and Perspectives
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lindenbach, B.D.; Murray, C.L.; Thiel, H.J.; Rice, C.M. Flaviviridae. In Fields Virology; Knipe, D.M., Howley, P.M., Eds.; Lippincott-Raven: Philadelphia, PA, USA, 2013; Volume 6, pp. 747–794. [Google Scholar]
- Brasil, Secretaria de atenção à saúde, Ministério da Saúde. Febre Amarela. In Guia Para Profissionais da Saúde, 1st ed.; Ministry of Health of Brazil: Brasília, Brazil, 2019. [Google Scholar]
- Vasconcelos, P.F.C. Yellow fever. Rev. Soc. Bras. Med. Trop. 2003, 36, 275–293. [Google Scholar] [CrossRef]
- Pan American Health Organization. Control of Yellow Fever: Field Guide. Washington, DC. Available online: https://www.paho.org/hq/dmdocuments/2013/PAHO-fieldguide-yellowfever-2005.pdf (accessed on 15 October 2020).
- Douam, F.; Ploss, A. Yellow Fever Virus: Knowledge Gaps Impeding the Fight against an Old Foe. Trends Microbiol. 2018, 26, 913–928. [Google Scholar] [CrossRef]
- Monath, T.P.; Vasconcelos, P.F. Yellow fever. J. Clin. Virol. 2015, 64, 160–173. [Google Scholar] [CrossRef]
- Barrett, D.T.; Higgs, S. Yellow Fever: A Disease that has yet to be conquered. Annu. Rev. Entomol. 2007, 52, 209–229. [Google Scholar] [CrossRef]
- Klitting, R.; Gould, E.A.; Paupy, C.; De Lamballerie, X. What Does the Future Hold for Yellow Fever Virus? (I). Genes 2018, 9, 291. [Google Scholar] [CrossRef]
- Christian, K.A.; Iuliano, A.D.; Uyeki, T.M.; Mintz, E.D.; Nichol, S.T.; Rollin, P.; Staples, J.E.; Arthur, R.R. What We are Watching—Top Global Infectious Disease Threats, 2013–2016: An Update from CDC’s Global Disease Detection Operations Center. Health Secur. 2017, 15, 453–462. [Google Scholar] [CrossRef]
- Pan American Health Organization. Yellow Fever: Number of Confirmed Cases and Deaths by Country in the Americas, 1960-Health Emergencies Department (PHE). Available online: https://ais.paho.org/phip/viz/ed_yellowfever.asp (accessed on 12 August 2020).
- Possas, C.; Lourenço-de-Oliveira, R.; Tauil, P.L.; Pinheiro, F.P.; Pissinatti, A.; Cunha, R.V.; Freire, M.; Martins, R.M.; Homma, A. Yellow fever outbreak in Brazil: The puzzle of rapid viral spread and challenges for immunisation. Mem. Inst. Oswaldo Cruz. 2018, 113, e180278. [Google Scholar] [CrossRef]
- Ministério da Saúde. Monitoramento do Período Sazonal da Febre Amarela Brasil, 2017/2018; Informe nº27, Ministério da Saúde, CGDT/DEVIT/SVS/MS: Brasília, Brazil, 2018. [Google Scholar]
- Couto-Lima, D.; Madec, Y.; Bersot, M.I.; Campos, S.S.; Mota, M.A.; Santos, F.B.; Vazeille, M.; Vasconcelos, P.F.C.; Lourenço-de-Oliveira, R.; Failloux, A.B. Potential risk of re-emergence of urban transmission of Yellow Fever virus in Brazil facilitated by competent Aedes populations. Sci. Rep. 2017, 7, 4848. [Google Scholar] [CrossRef]
- Pierson, T.C.; Diamond, M.S. The continued threat of emerging flaviviruses. Nat. Microbiol. 2020, 5, 796–812. [Google Scholar] [CrossRef]
- Massad, E.; Amaku, M.; Coutinho, F.; Struchiner, C.J.; Lopez, L.F.; Coelho, G.; Wilder-Smith, A.; Burattini, M.N. The risk of urban yellow fever resurgence in Aedes-infested American cities. Epidemiol. Infect. 2018, 146, 1219–1225. [Google Scholar] [CrossRef]
- Franco, O. História da Febre Amarela no Brasil; Ministério da Saúde, Departamento de Endemias Rurais: Rio de Janeiro, Brazil, 1969.
- Chippaux, J.P.; Chippaux, A. Yellow fever in Africa and the Americas: A historical and epidemiological perspective. J. Venom. Anim. Toxins Incl. Trop. Dis. 2018, 24, 20. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, L. Da transmissão hídrica a culicidiana: A febre amarela na sociedade de medicina e cirurgia de São Paulo. Rev. Bras. História 2001, 21, 217–242. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Benchimol, J. Febre Amarela: A Doença e a Vacina, Uma História Inacabada; Fiocruz: Rio de Janeiro, Brazil, 2001; p. 469. [Google Scholar]
- Finlay, C.J. El mosquito hipotéticamente considerado como agente de transmision de la fiebre amarilla. An. Real Acad. Cienc. Médicas Físicas Nat. Habana 1881, 18, 147–169. [Google Scholar]
- Finlay, C.J.; Matas, R. The mosquito hypothetically considered as an agent in the transmission of yellow fever poison. Yale J. Biol. Med. 1881, 9, 589–604. [Google Scholar]
- Faerstein, E.; Winkelstein, W., Jr. Carlos Juan Finlay: Rejected, respected, and right. Epidemiology 2010, 21, 158. [Google Scholar] [CrossRef]
- Soper, F.L.; Penna, H.; Cardoso, E.; Serafim, J., Jr.; Frobisher, M., Jr.; Pinheiro, J. Yellow fever whithout Aedes aegypti. Study of a rural epidemic in the Valle do Chanaan, Espirito Santo, Brazil. Am. J. Epidemiol. 1933, 18, 555–587. [Google Scholar] [CrossRef]
- Soper, F.L. Jungle yellow fever. A new epidemiological entity in South America. Rev. Hyg. Saude Publica 1936, 10, 107–144. [Google Scholar]
- Costa, Z.G.A.; Romano, A.P.M.; Elkhoury, A.N.M.; Flannery, B. Evolução histórica da vigilância epidemiológica e do controle da febre amarela no Brasil. Rev. Pan-Amaz. Saude 2011, 2, 11–26. [Google Scholar] [CrossRef]
- Cope, S. Yellow Jack—How Yellow Fever Ravaged America and Walter Reed Discovered Its Deadly Secrets. Emerg. Infect. Dis. 2005, 11, 1652. [Google Scholar] [CrossRef]
- Soper, F.L. Recent extensions of knowledge of yellow fever. Quart. Bull. Health Organ. Leag. Nation 1935, 5, 1–50. [Google Scholar]
- Roukens, A.H.; Visser, L.G. Yellow fever vaccine: Past, present and future. Expert Opin. Biol. Ther. 2008, 8, 1787–1795. [Google Scholar] [CrossRef] [PubMed]
- Soper, F.L.; Smith, H.H. Vaccination with virus 17D in control of jungle yellow fever in Brazil. In Acta Conventus Tertii de Tropicis Atque Malariae Morbis; Reprinted from the Transactions of the Third International Congress of Tropical Medicine and Malaria; C.A. Spin & Zoon N.V.: Holland, The Netherlands, 1938; Volume 1, pp. 295–313. [Google Scholar]
- Rigau-Pérez, J.G.; Clark, G.G.; Gubler, D.J.; Reiter, P.; Sanders, E.J.; Vorndam, A.V. Dengue and dengue haemorrhagic fever. Lancet 1998, 352, 971–977. [Google Scholar] [CrossRef]
- Gubler, D.J. Epidemic dengue/dengue hemorrhagic fever as a public health, social and economic problem in the 21st century. Trends Microbiol. 2002, 10, 100–103. [Google Scholar] [CrossRef]
- Mackenzie, J.S.; Gubler, D.J.; Petersen, L.R. Emerging flaviviruses: The spread and resurgence of Japanese encephalitis, West Nile and dengue viruses. Nat. Med. 2004, 10, S98–S109. [Google Scholar] [CrossRef]
- Carrington, C.V.; Foster, J.E.; Pybus, O.G.; Bennett, S.N.; Holmes, E.C. Invasion and maintenance of dengue virus type 2 and type 4 in the Americas. J. Virol. 2005, 79, 14680–14687. [Google Scholar] [CrossRef]
- Brasil, Ministério da Saúde. Febre amarela: Sintomas, Tratamento, Diagnóstico e Prevenção. 2013/2020. Available online: https://saude.gov.br/saude-de-a-z/febre-amarela-sintomas-transmissao-e-prevencao (accessed on 12 August 2020).
- Vasconcelos, P.F.C. Yellow fever in Brazil: Thoughts and hypotheses on the emergence in previously free areas. Rev. Saude Publica 2010, 44, 1144–1149. [Google Scholar] [CrossRef] [PubMed]
- Pessanha, J.E.M. Yellow Fever: A vision of the current scenario. Rev. Med. Minas Gerais 2009, 19, 97–102. [Google Scholar]
- Brasil, Ministério da Saúde. Reemergência da febre amarela silvestre no Brasil, 2014/2015: Situação epidemiológica e a importância da vacinação preventiva e da vigilância intensificada no período sazonal. Bol. Epidemiológico 2015, 46. Available online: http://portalarquivos2.saude.gov.br/images/pdf/2015/outubro/19/2015-032---FA-ok.pdf (accessed on 12 August 2020).
- Silva, N.I.O.; Sacchetto, L.; Rezende, I.M.; Trindade, G.S.; LaBeaud, A.D.; Thoisy, B.; Drumond, B.P. Recent sylvatic yellow fever virus transmission in Brazil: The news from an old disease. Virol. J. 2020, 17, 9. [Google Scholar] [CrossRef]
- Brasil, Secretaria de Vigilância em Saúde. Monitoramento de Febre Amarela, Informe nº18, 9 Junho. Available online: https://www.saude.gov.br/images/pdf/2019/junho/13/Informe-de-Monitoramento-de-Febre-Amarela-Brasil--n-18.pdf (accessed on 12 August 2020).
- Faria, N.R.; Kraemer, M.U.G.; Hill, S.C.; Jesus, J.G.; Aguiar, R.S.; Iani, F.C.M.; Xavier, J.; Quick, J.; du Plessis, L.; Dellicour, S.; et al. Genomic and epidemiological monitoring of yellow fever virus transmission potential. Science 2018, 361, 894–899. [Google Scholar] [CrossRef]
- Giovanetti, M.; Mendonça, M.C.L.; Fonseca, V.; Mares-Guia, M.A.; Fabri, A.; Xavier, J.; Jesus, J.G.; Gräf, T.; Rodrigues, C.D.S.; Santos, C.C.; et al. Yellow Fever Virus Reemergence and Spread in Southeast Brazil, 2016. J. Virol. 2019, 94, e01623. [Google Scholar] [CrossRef]
- Vasconcelos, P.F.C.; Costa, Z.G.; Travassos da Rosa, E.S.; Luna, E.; Rodrigues, S.G.; Barros, V.L.R.S.; Dias, J.P.; Monteiro, H.A.; Oliva, O.F.; Vasconcelos, H.B.; et al. Epidemic of jungle yellow fever in Brazil, 2000: Implications of climatic alterations in disease spread. J. Med. Virol. 2001, 65, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C. Urbanization and geographic expansion of zoonotic arboviral diseases: Mechanisms and potential strategies for prevention. Trends Microbiol. 2013, 21, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Morens, D.M.; Folkers, G.K.; Fauci, A.S. The challenge of emerging and reemerging infectious diseases. Nature 2004, 430, 242–249. [Google Scholar] [CrossRef]
- Rezende, I.M.; Pereira, L.S.; Fradico, J.R.B.; Xavier, M.A.P.; Alves, P.A.; Campi-Azevedo, A.C.; Speziali, E.; Dos Santos, L.Z.M.; Albuquerque, N.S.; Penido, I.; et al. Late-Relapsing Hepatitis after Yellow Fever. Viruses 2020, 12, 222. [Google Scholar] [CrossRef] [PubMed]
- Denis, B.; Chirio, D.; Ponscarme, D.; Brichler, S.; Verdière, N.C.; Simon, F.; Molina, J.M. Hepatitis Rebound after Infection with Yellow Fever Virus. Emerg. Infect. Dis. 2019, 25, 1248–1249. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.L.; Joelsons, D.; Leite, G.F.C.; Malbouisson, L.M.S.; Song, A.T.W.; Perodini, B.; Andrade, L.C.; Pinto, L.F.; D’Albuquerque, L.A.C.; Segurado, A.A.C.; et al. Severe yellow fever in Brazil: Clinical characteristics and management. J. Travel. Med. 2019, 26, taz040. [Google Scholar] [CrossRef] [PubMed]
- Marinho, P.E.S.; Alvarenga, P.P.M.; Crispim, A.P.C.; Candiani, T.M.S.; Alvarenga, A.M.; Bechler, I.M.; Alves, P.A.; Dornas, F.P.; Oliveira, D.B.; Bentes, A.A.; et al. Wild-Type Yellow Fever Virus RNA in Cerebrospinal Fluid of Child. Emerg. Infect. Dis. 2019, 25, 1567. [Google Scholar] [CrossRef]
- Kallas, E.G.; Zanella, L.G.F.A.B.D.; Moreira, C.H.V.; Buccheri, R.; Diniz, G.B.F.; Castiñeiras, A.C.P.; Costa, P.R.; Dias, J.Z.C.; Marmorato, M.P.; Song, A.T.W.; et al. Predictors of mortality in patients with yellow fever: An observational cohort study. Lancet Infect. Dis. 2019, 19, 750–758. [Google Scholar] [CrossRef]
- De Freitas, C.S.; Higa, L.M.; Sacramento, C.Q.; Ferreira, A.C.; Reis, P.A.; Delvecchio, R.; Monteiro, F.L.; Barbosa-Lima, G.; Westgarth, H.J.; Vieira, Y.R.; et al. Yellow fever virus is susceptible to sofosbuvir both in vitro and in vivo. PLoS Negl. Trop. Dis. 2019, 13, e0007072. [Google Scholar] [CrossRef]
- Mendes, E.A.; Pilger, D.R.B.; Nastri, A.C.S.S.; Malta, F.M.; Pascoalino, B.S.; D’Albuquerque, L.A.C.; Balan, A.; de Freitas Jr, L.H.G.; Durigon, E.L.; Carrilho, F.J.; et al. Sofosbuvir inhibits yellow fever virus in vitro and in patients with acute liver failure. Ann. Hepatol. 2019, 18, 816–824. [Google Scholar] [CrossRef]
- Brasil, Ministério da Saúde. Vacina de Febre Amarela Será Ampliada Para Todo o Brasil. Available online: https://www.saude.gov.br/noticias/agencia-saude/42849-vacina-de-febre-amarela-sera-ampliada-para-todo-o-brasil (accessed on 20 March 2020).
- Nnaji, C.A.; Shey, M.S.; Adetokunboh, O.O.; Wiysonge, C.S. Immunogenicity and safety of fractional dose yellow fever vaccination: A systematic review and meta-analysis. Vaccine 2020, 38, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Casey, R.M.; Harris, J.B.; Ahuka-Mundeke, S.; Dixon, M.G.; Kizito, G.M.; Nsele, P.M.; Umutesi, G.; Laven, J.; Kosoy, O.; Paluku, G.; et al. Immunogenicity of fractional-dose vaccine during a yellow fever outbreak–Final report. N. Engl. J. Med. 2019, 381, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.T.; Peak, C.M.; Leung, G.M.; Lipsitch, M. Fractional dosing of yellow fever vaccine to extend supply: A modelling study. Lancet 2016, 388, 2904–2911. [Google Scholar] [CrossRef]
- Pan American Health Organization. Brazil Launches World’s Largest Campaign with Fractional-Dose Yellow Fever Vaccine. Available online: https://www.paho.org/hq/index.php?option=com_content&view=article&id=14065&Itemid=135&lang=en (accessed on 12 August 2020).
- Boëte, C. Yellow Fever Outbreak: O Vector Control, Where Art Thou? J. Med. Entomol. 2016, 53, 1048–1049. [Google Scholar] [CrossRef]
- Estofolete, C.F.; Nogueira, M.L. Is a dose of 17D vaccine in the current context of Yellow Fever enough? Braz. J. Microbiol. 2018, 49, 683–684. [Google Scholar] [CrossRef] [PubMed]
- Costa-Rocha, I.A.; Campi-Azevedo, A.C.; Peruhype-Magalhães, V.; Coelho-dos-Reis, J.G.; Fradico, J.R.B.; Souza-Lopes, T.; Reis, L.R.; Freire, L.C.; Costa-Pereira, C.; Mambrini, J.V.M.; et al. Duration of Humoral and Cellular Immunity 8 Years after Administration of Reduced Doses of the 17DD-Yellow Fever Vaccine. Front. Immunol. 2019, 10, 1211. [Google Scholar] [CrossRef] [PubMed]
- Campi-Azevedo, A.C.; Peruhype-Magalhães, V.; Coelho-dos-Reis, J.G.; Antonelli, L.R.; Costa-Pereira, C.; Speziali, E.; Reis, L.R.; Lemos, J.A.; Ribeiro, J.G.L.; Camacho, L.A.B.; et al. 17DD Yellow Fever Revaccination and Heightened Long-Term Immunity in Populations of Disease-Endemic Areas, Brazil. Emerg. Infec. Dis. 2019, 25, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Collaborative group for studies on yellow fever vaccines. Duration of post-vaccination immunity against yellow fever in adults. Vaccine 2014, 32, 4977–4984. [Google Scholar] [CrossRef]
- Campi-Azevedo, A.C.; Costa-Pereira, C.; Antonelli, L.R.; Fonseca, C.T.; Teixeira-Carvalho, A.; Villela-Rezende, G.; Santos, R.A.; Batista, M.A.; Campos, F.M.; Pacheco-Porto, L.; et al. Booster dose after 10 years is recommended following 17DD-YF primary vaccination. Hum. Vaccine Immunother. 2016, 12, 491–502. [Google Scholar] [CrossRef]
- World Health Organization. Vaccines and vaccination against yellow fever. Wkly. Epidemiol. Rec. 2013, 88, 269–284. Available online: https://www.who.int/wer/2013/wer8827.pdf?ua=1 (accessed on 12 August 2020).
- Ferreira, C.d.; Campi-Azevedo, A.C.; Peruhype-Magalhāes, V.; Costa-Pereira, C.; de Albuquerque, C.P.; Muniz, L.F.; de Souza, T.Y.; Oliveira, A.C.V.; Martins-Filho, O.A.; da Mota, L.M.H. The 17D–204 and 17DD yellow fever vaccines: An overview of major similarities and subtle differences. Expert Rev. Vaccines 2018, 17, 79–90. [Google Scholar] [CrossRef]
- Vasconcelos, P.F.C. Single shot of 17D vaccine may not confer life-long protection against yellow fever. Mem. Inst. Oswaldo Cruz. 2018, 113, 135–136. [Google Scholar] [CrossRef]
- Ortiz-Martínez, Y.; Patiño-Barbosa, A.M.; Rodriguez-Morales, A.J. Yellow fever in the Americas: The growing concern about new epidemics. F1000Research 2017, 6, 398. [Google Scholar] [CrossRef]
- Stoffella-Dutra, A.G.; de Oliveira, J.S.; Costa, G.B.; Kroon, E.G.; Abrahão, J.S.; LaBeaud, A.D.; Drumond, B.P.; Trindade, G.S. Absence of YF-neutralizing antibodies in vulnerable populations of Brazil: A warning for epidemiological surveillance and potential risks for future outbreaks. Vaccine 2020, 38, 6592–6599. [Google Scholar] [CrossRef]
- Secretaria de Estado de Saúde de Minas Gerais. Dados de Cobertura Vacinal em Minas Gerais. Available online: http://www.saude.mg.gov.br/febreamarela (accessed on 12 August 2020).
- Machado, V.W.; Vasconcelos, P.F.C.; Silva, E.V.P.; Santos, J.B. Serologic assessment of yellow fever immunity in the rural population of a yellow fever-endemic area in Central Brazil. Rev. Soc. Bras. Med. Trop. 2013, 46, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Miyaji, K.T.; Avelino-Silva, V.I.; Simões, M.; Freire, M.S.; Medeiros, C.R.; Braga, P.E.; Neves, M.A.A.; Lopes, M.H.; Kallas, E.G.; Sartori, A.M.C. Prevalence and titers of yellow fever virus neutralizing antibodies in previously vaccinated adults. Rev. Inst. Med. Trop. Sao Paulo 2017, 59, e2. [Google Scholar] [CrossRef]
- World Health Organization. A Global Strategy to Eliminate Yellow Fever Epidemics (EYE) 2017–2026; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Vasconcelos, P.F.C.; Calisher, C.H. Emergence of Human Arboviral Diseases in the Americas, 2000–2016. Vector Borne Zoonotic Dis. 2016, 16, 295–301. [Google Scholar] [CrossRef]
- Pan-American Health Organization. Plano de Ação sobre Entomologia e Controle de Vetores. 56° Conselho Diretor, 70º Sessão do Comitê Regional da OMS para as Américas Washington, D.C.; EUA, 23 a 27 de setembro de. Available online: https://iris.paho.org/bitstream/handle/10665.2/49612/CD56-11-p.pdf (accessed on 12 August 2020).
- Mir, D.; Delatorre, E.; Bonaldo, M.; Lourenço-de-Oliveira, R.; Vicente, A.C.; Bello, G. Phylodynamics of Yellow Fever Virus in the Americas: New insights into the origin of the 2017 Brazilian outbreak. Sci. Rep. 2017, 7, 7385. [Google Scholar] [CrossRef]
- Bonaldo, M.C.; Gómez, M.M.; Santos, A.A.C.; Abreu, F.V.S.; Ferreira-de-Brito, A.; Miranda, R.M.; Castro, M.G.; Lourenço-de-Oliveira, R. Genome analysis of yellow fever virus of the ongoing outbreak in Brazil reveals polymorphisms. Mem. Inst. Oswaldo Cruz. 2017, 112, 447–451. [Google Scholar] [CrossRef]
- Rezende, I.M.; Sacchetto, L.; Mello, E.M.; Alves, P.A.; Iani, F.C.M.; Adelino, T.E.R.; Duarte, M.M.; Cury, A.L.F.; Bernardes, A.F.L.; Santos, T.A.; et al. Persistence of Yellow fever virus outside the Amazon Basin, causing epidemics in Southeast Brazil, from 2016 to 2018. PLoS Negl. Trop. Dis. 2018, 12, e0006538. [Google Scholar] [CrossRef]
- Barbosa, C.M.; Di Paola, N.; Cunha, M.P.; Jesus, M.J.R.; Araújo, D.B.; Silveira, D.B.; Leal, F.B.; Mesquita, F.S.; Botosso, V.F.; Zanotto, P.M.A.; et al. Yellow Fever Virus in Urine and Semen of Convalescent Patient, Brazil. Emerg. Infect. Dis. 2018, 24, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Soto, A.; Torres, M.C.; Mendonça, M.C.L.; Mares-Guia, M.A.; Rodrigues, C.D.S.; Fabri, A.A.; Dos Santos, C.C.; Machado Araújo, E.S.; Fischer, C.; Ribeiro Nogueira, R.M.; et al. Evidence for multiple sylvatic transmission cycles during the 2016–2017 yellow fever virus outbreak, Brazil. Clin. Microbiol. Infect. 2018, 24, 1019. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, P.O.; Silva, A.T.S.; Oliveira, J.S.; Marinho, P.E.; Rocha, F.T.; Domingos, G.P.; Poblete, P.C.P.; Oliveira, L.B.S.; Duarte, D.C.; Bonjardim, C.A.; et al. Detection and Molecular Characterization of Yellow Fever Virus, 2017, Brazil. EcoHealth 2018, 15, 864. [Google Scholar] [CrossRef] [PubMed]
- Delatorre, E.; Abreu, F.V.S.; Ribeiro, I.P.; Gómez, M.M.; dos Santos, A.A.C.; Ferreira-de-Brito, A.; Neves, M.S.A.S.; Bonelly, I.; de Miranda, R.M.; Furtado, N.D.; et al. Distinct YFV Lineages Co-circulated in the Central-Western and Southeastern Brazilian Regions from 2015 to 2018. Front. Microbiol. 2019, 10, 1079. [Google Scholar] [CrossRef]
- Carvalho, R.G.; Lourenço-de-Oliveira, R.; Braga, I.A. Updating the geographical distribution and frequency of Aedes albopictus in Brazil with remarks regarding its range in the Americas. Mem. Inst. Oswaldo Cruz. 2014, 109, 787–796. [Google Scholar] [CrossRef]
- World Mosquito Program. 2020. Available online: https://www.worldmosquitoprogram.org/ (accessed on 15 October 2020).
- Dutra, H.L.C.; Dos Santos, L.M.B.; Caragata, E.P.; Silva, J.B.L.; Villela, D.A.M.; Maciel-de-Freitas, R.; Moreira, L.A. From Lab to Field: The Influence of Urban Landscapes on the Invasive Potential of Wolbachia in Brazilian Aedes aegypti Mosquitoes. PLoS Negl. Trop. Dis. 2015, 9, e0003689. [Google Scholar] [CrossRef]
- Dutra, H.L.C.; Rocha, M.N.; Dias, F.B.S.; Mansur, S.B.; Caragata, E.P.; Moreira, L.A. Wolbachia Blocks Currently Circulating Zika Virus Isolates in Brazilian Aedes aegypti Mosquitoes. Cell Host Microbe 2016, 19, 771–774. [Google Scholar] [CrossRef]
- Flores, H.A.; de Bruyne, J.T.; O’Donnell, T.B.; Nhu, V.T.; Giang, N.T.; Trang, H.T.X.; Van, H.T.T.; Long, V.T.; Dui, L.; Huy, H.L.; et al. Multiple Wolbachia strains provide comparative levels of protection against dengue virus infection in Aedes aegypti. PLoS Pathog. 2020, 16, e1008433. [Google Scholar] [CrossRef]
- Rocha, M.N.; Duarte, M.M.; Mansur, S.B.; Silva, B.D.M.E.; Pereira, T.N.; Adelino, T.É.R.; Giovanetti, M.; Alcantara, L.C.J.; Santos, F.M.; Costa, V.R.M.; et al. Pluripotency of Wolbachia against Arboviruses: The case of yellow fever. Gates Open Res. 2019, 3, 161. [Google Scholar] [CrossRef]
- Bicca-Marques, J.C.; Freitas, D.S. The role of monkeys, mosquitoes, and humans in the occurrence of a yellow fever outbreak in a fragmented landscape in south Brazil: Protecting howler monkeys is a matter of public health. Trop. Conserv. Sci. 2010, 3, 78–89. [Google Scholar] [CrossRef]
- Amraoui, F.; Pain, A.; Piorkowski, G.; Vazeille, M.; Couto-Lima, D.; Lamballerie, X.; Lourenço-de-Oliveira, R.; Failloux, A.B. Experimental Adaptation of the Yellow Fever Virus to the Mosquito Aedes albopictus and Potential risk of urban epidemics in Brazil, South America. Sci. Rep. 2018, 8, 14337. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira Figueiredo, P.; Stoffella-Dutra, A.G.; Barbosa Costa, G.; Silva de Oliveira, J.; Dourado Amaral, C.; Duarte Santos, J.; Soares Rocha, K.L.; Araújo Júnior, J.P.; Lacerda Nogueira, M.; Zazá Borges, M.A.; et al. Re-Emergence of Yellow Fever in Brazil during 2016–2019: Challenges, Lessons Learned, and Perspectives. Viruses 2020, 12, 1233. https://doi.org/10.3390/v12111233
de Oliveira Figueiredo P, Stoffella-Dutra AG, Barbosa Costa G, Silva de Oliveira J, Dourado Amaral C, Duarte Santos J, Soares Rocha KL, Araújo Júnior JP, Lacerda Nogueira M, Zazá Borges MA, et al. Re-Emergence of Yellow Fever in Brazil during 2016–2019: Challenges, Lessons Learned, and Perspectives. Viruses. 2020; 12(11):1233. https://doi.org/10.3390/v12111233
Chicago/Turabian Stylede Oliveira Figueiredo, Poliana, Ana Gabriella Stoffella-Dutra, Galileu Barbosa Costa, Jaqueline Silva de Oliveira, Carolina Dourado Amaral, Juliane Duarte Santos, Kamila Lorene Soares Rocha, João Pessoa Araújo Júnior, Maurício Lacerda Nogueira, Magno Augusto Zazá Borges, and et al. 2020. "Re-Emergence of Yellow Fever in Brazil during 2016–2019: Challenges, Lessons Learned, and Perspectives" Viruses 12, no. 11: 1233. https://doi.org/10.3390/v12111233
APA Stylede Oliveira Figueiredo, P., Stoffella-Dutra, A. G., Barbosa Costa, G., Silva de Oliveira, J., Dourado Amaral, C., Duarte Santos, J., Soares Rocha, K. L., Araújo Júnior, J. P., Lacerda Nogueira, M., Zazá Borges, M. A., Pereira Paglia, A., Desiree LaBeaud, A., Santos Abrahão, J., Geessien Kroon, E., Bretas de Oliveira, D., Paiva Drumond, B., & de Souza Trindade, G. (2020). Re-Emergence of Yellow Fever in Brazil during 2016–2019: Challenges, Lessons Learned, and Perspectives. Viruses, 12(11), 1233. https://doi.org/10.3390/v12111233