
Human Health and Outdoor Adventure Recreation: Perceived Health Outcomes



Abstract
:1. Background
1.1. Adventure-Based Activities and Health
1.2. Research on OAR in Natural and Forest Landscapes
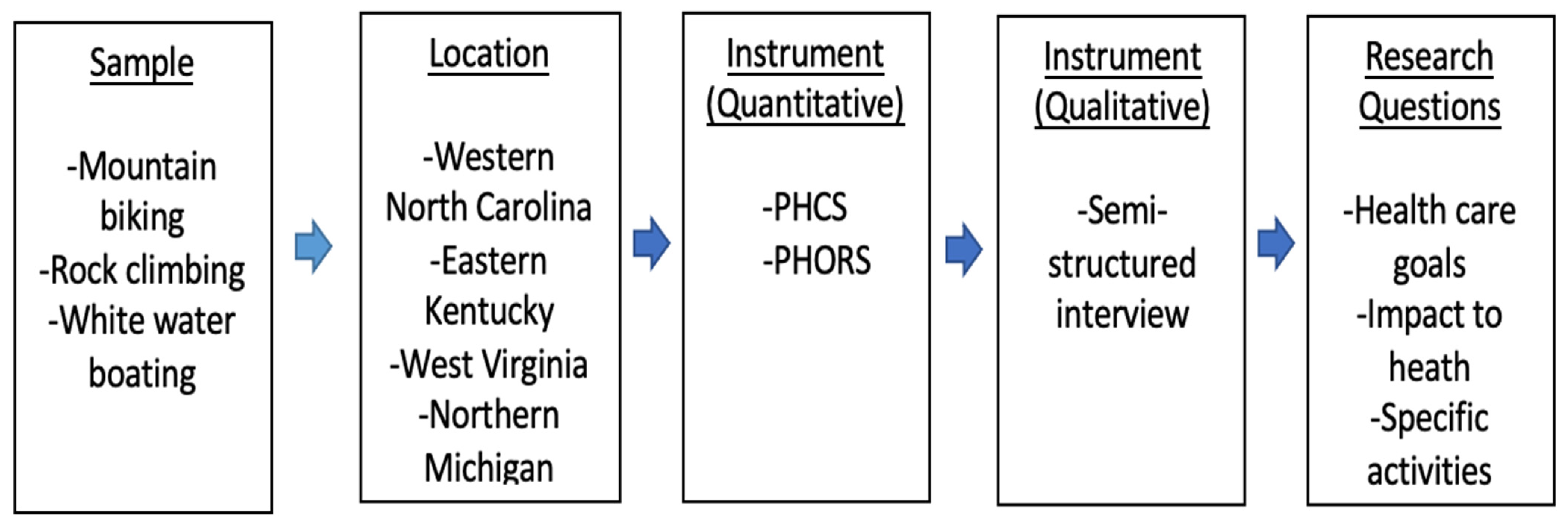
2. Methods
2.1. Data Collection
2.2. Data Storage and Protection
2.3. Multiple-Method Design
2.4. Theoretical Considerations
3. Results
3.1. Quantitative
3.1.1. Health Prevention
3.1.2. Health Improvement
3.2. Qualitative
3.2.1. Physical Health Outcomes and Goals, Management, and Support
3.2.2. Physical Health Enhancement and Management
3.2.3. Mental Health
3.2.4. Natural Environment
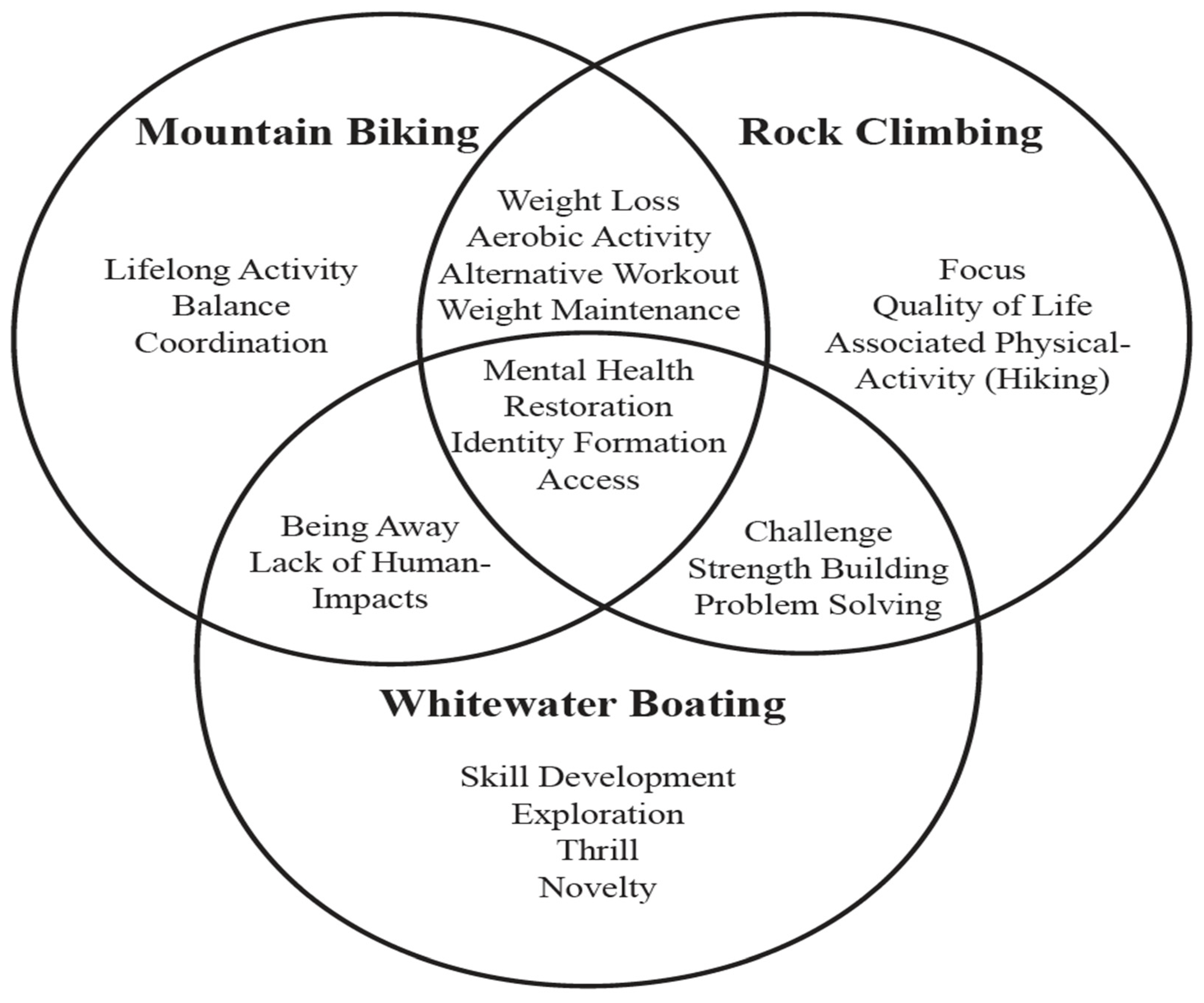
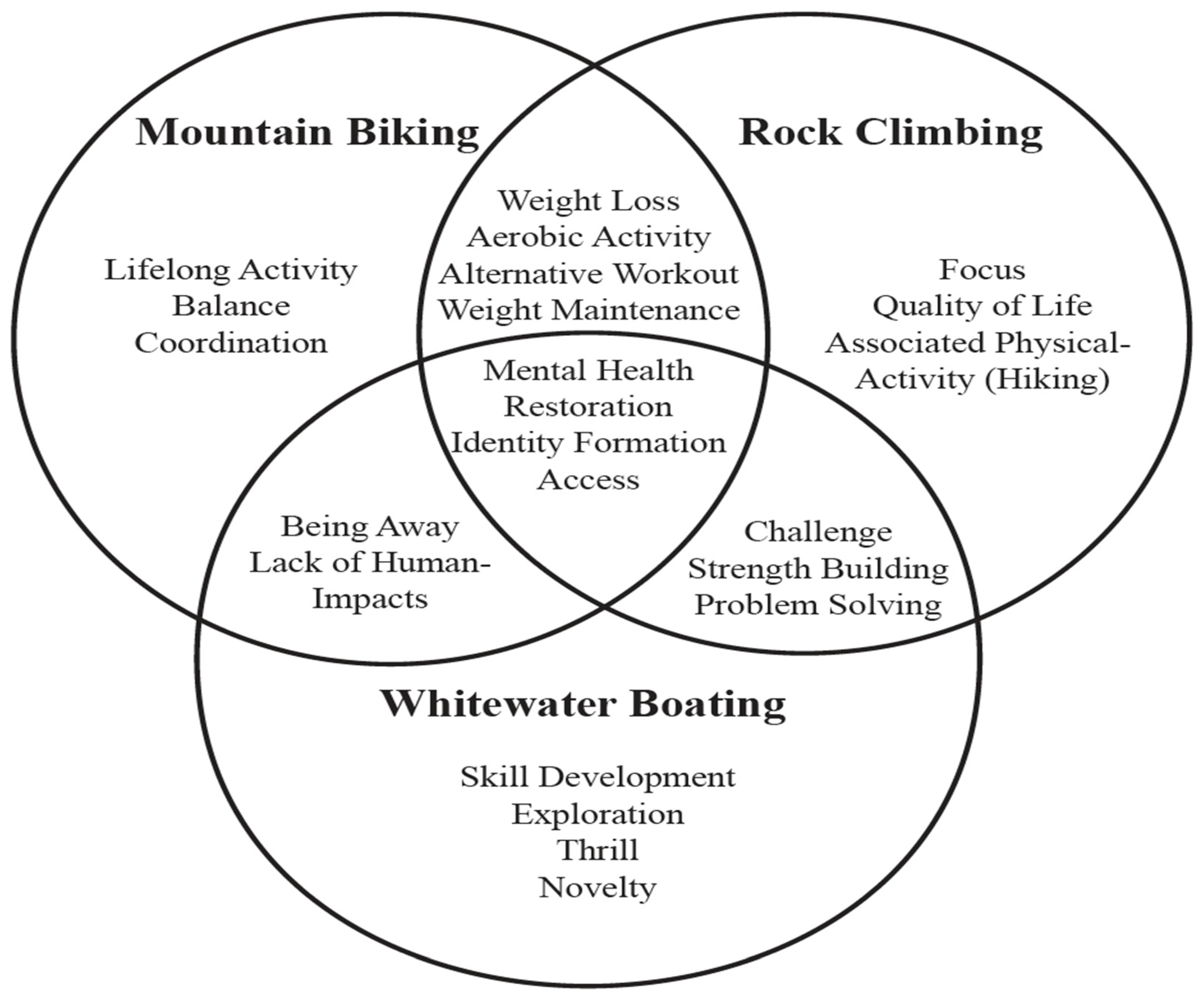
3.2.5. Differences between OAR Activities
4. Discussion
4.1. Health-Focused OAR
4.2. Connection to Theory
4.3. Limitations and Recommendations for Further Study
4.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Perceived Health Competency Scale (PHCS)
| Strongly Disagree | Disagree Somewhat | Neutral | Agree Somewhat | Strongly Agree | |
| I handle myself well with respect to my health | 1 | 2 | 3 | 4 | 5 |
| No matter how hard I try, my health just doesn’t turn out the way I would like | 1 | 2 | 3 | 4 | 5 |
| It is difficult for me to find effective solutions to the health problems that come my way | 1 | 2 | 3 | 4 | 5 |
| I succeed in the projects I undertake to improve my health | 1 | 2 | 3 | 4 | 5 |
| I’m generally able to accomplish my goals with respect to my health | 1 | 2 | 3 | 4 | 5 |
| I find my efforts to change things I don’t like about my health to be ineffective | 1 | 2 | 3 | 4 | 5 |
| Typically, my plans for my health don’t work out well | 1 | 2 | 3 | 4 | 5 |
| I am able to manage my health as well as most other people | 1 | 2 | 3 | 4 | 5 |
Appendix B. Perceived Health Outcomes of Recreation Scale (PHORS)
| Strongly Disagree | Disagree | Neither Agree nor Disagree | Agree | Strongly Agree | |
| Causes me to appreciate life more | 1 | 2 | 3 | 4 | 5 |
| Causes me to enjoy life more | 1 | 2 | 3 | 4 | 5 |
| Gives me a sense of self-reliance | 1 | 2 | 3 | 4 | 5 |
| Gives me a sense of higher self-esteem | 1 | 2 | 3 | 4 | 5 |
| Makes me more aware of who I am | 1 | 2 | 3 | 4 | 5 |
| Is connected to other positive aspects of my life | 1 | 2 | 3 | 4 | 5 |
| Causes me to be more satisfied with my life | 1 | 2 | 3 | 4 | 5 |
| Reduces my chances of developing diabetes | 1 | 2 | 3 | 4 | 5 |
| Reduces my changes of weight gain | 1 | 2 | 3 | 4 | 5 |
| Reduces my chances of having a heart attack | 1 | 2 | 3 | 4 | 5 |
| Reduces my chances of premature death | 1 | 2 | 3 | 4 | 5 |
| Reduces my number of illnesses | 1 | 2 | 3 | 4 | 5 |
| Improves my overall fitness | 1 | 2 | 3 | 4 | 5 |
| Improves my overall health | 1 | 2 | 3 | 4 | 5 |
| Improves my muscle strength | 1 | 2 | 3 | 4 | 5 |
| Improves my physical flexibility | 1 | 2 | 3 | 4 | 5 |
Appendix C. Perceived Health Outcomes of Recreation (PHORS) Structure Matrix
| Factor | |||
| Item | PSYC | PREV | IMPV |
| Appreciate life more | 0.642 | 0.170 | 0.355 |
| Enjoy life more | 0.604 | 0.207 | 0.365 |
| Self-reliance | 0.599 | 0.279 | 0.334 |
| Self Esteem | 00.671 | 0.350 | 0.456 |
| Part of who I am | 0.705 | 0.309 | 0.294 |
| Related to other positive aspects of my life | 0.637 | 0.300 | 0.367 |
| Increase life satisfaction | 0.709 | 0.233 | 0.351 |
| Reduce chance of diabetes | 0.315 | 0.852 | 0.432 |
| Reduce weight | 0.394 | 0.836 | 0.596 * |
| Reduce chance of heart attack | 0.382 | 0.945 | 0.541 |
| Reduce chance of premature death | 0.277 | 0.842 | 0.457 |
| Reduce chance of illness | 0.364 | 0.835 | 0.504 |
| Improves fitness | 0.399 | 0.464 | 0.873 |
| Improves health | 0.502 | 0.583 * | 0.824 |
| Improves strength | 0.453 | 0.432 | 0.784 |
| Improves flexibility | 0.387 | 0.380 | 0.551 |
| Chronbach’s Alpha | 0.829 | 0.937 | 0.806 |
| Extraction method: principal axis factoring. Rotation method: Promax with Kaiser normalization. Note * identified potential items that also aligned (>0.55) with the factor outside of what was found in previous studies. | |||
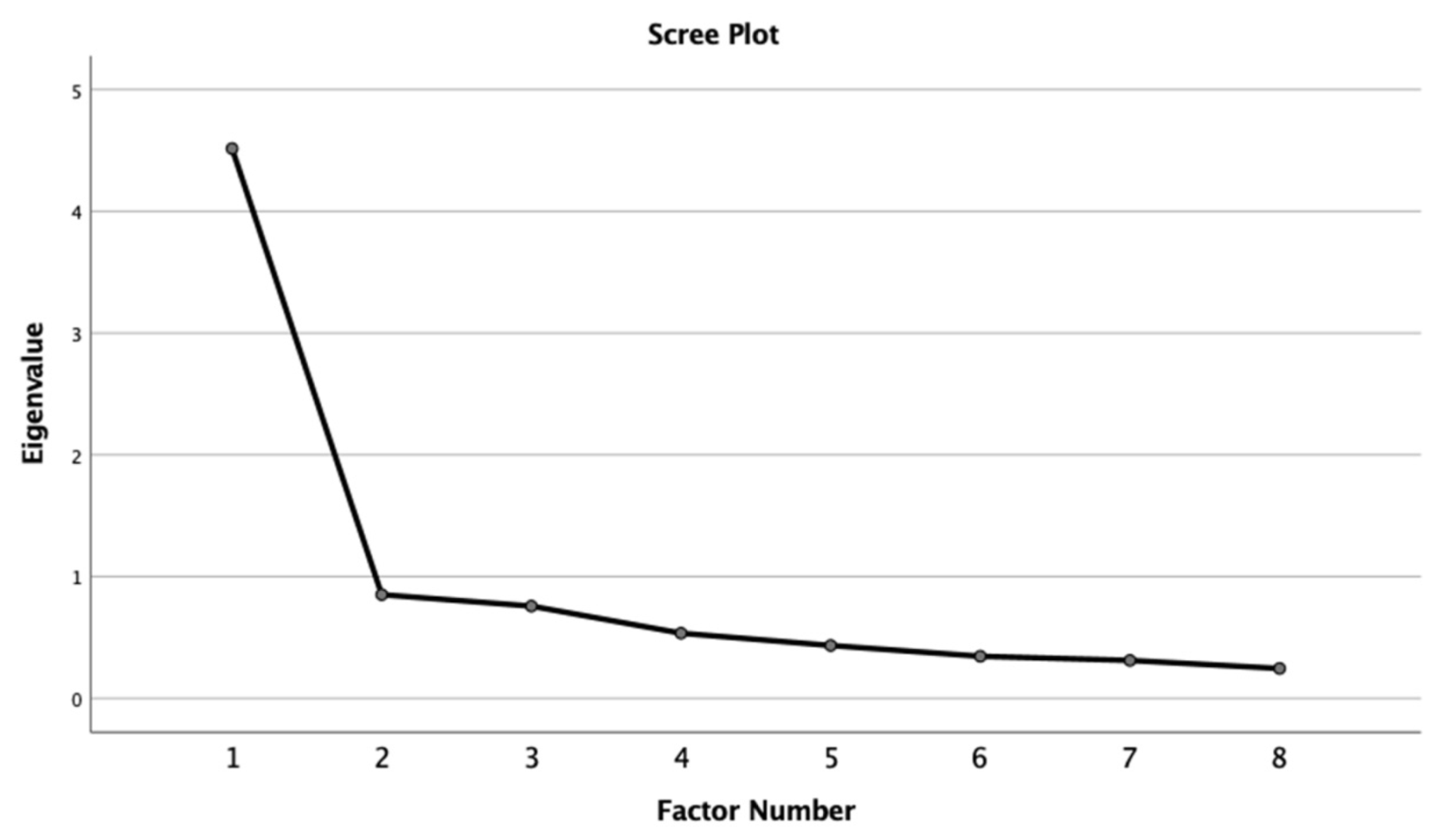
Appendix D. Scree Plot Perceived Health Competency Scale Factor Analysis
References
- Ewert, E.; Mitten, D.; Overholt, J. Natural Environments and Human Health; CABI: Wallingford, UK, 2014. [Google Scholar]
- Hartig, T.; Berg, A.E.V.D.; Hagerhall, C.M.; Tomalak, M.; Bauer, N.; Hansmann, R.; Ojala, A.; Syngollitou, E.; Carrus, G.; van Herzele, A.; et al. Health Benefits of Nature Experience: Psychological, Social and Cultural Processes. In Forests, Trees and Human Health; Springer: Berlin/Heidelberg, Germany, 2011; pp. 127–168. [Google Scholar]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beil, K.; Hanes, D. The influence of urban natural and built environments on physiological and psychological measures of stress—A pilot study. Int. J. Environ. Res. Public Health 2013, 10, 1250–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewert, A.; Chang, Y. Levels of nature and stress response. Behav. Sci. 2018, 8, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.J.; Hur, J.; Yang, K.-S.; Lee, M.-K.; Lee, S.-J. Acute biophysical responses and psychological effects of different types of forests in patients with metabolic syndrome. Environ. Behav. 2018, 50, 298–323. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Physiological and psychological effects of viewing forests on young women. Forests 2019, 10, 635. [Google Scholar] [CrossRef] [Green Version]
- Ewert, A.W.; Sibthorp, J.; and. Outdoor Adventure Education: Foundations, Theory, and Research; Human Kinetics: Champaign, IL, USA, 2014. [Google Scholar]
- Houge Mackenzie, S.; Hodge, K. Adventure recreation and subjective well-being: A conceptual framework. Leis. Stud. 2020, 39, 26–40. [Google Scholar] [CrossRef]
- Houge Mackenzie, S.; Kerr, J.H. Positive motivational experience over a three-day outdoor adventure trek in Peru. J. Adventure Educ. Outdoor Learn. 2017, 17, 4–17. [Google Scholar] [CrossRef]
- Ewert, A.; Hollenhorst, S. Risking it on wildlands: The evolution of adventure recreation. J. Environ. Educ. 1990, 21, 29–35. [Google Scholar] [CrossRef]
- Prouty, D.; Panicucci, J.; Collinson, R. Adventure Education: Theory and Applications; Human Kinetics: Champaign, IL, USA, 2007. [Google Scholar]
- Outdoor Industry Association. Outdoor Participation Report 2018; Outdoor Industry Association: Washington, DC, USA, 2019. [Google Scholar]
- Bratton, R.D.; Kinnear, G.; Koroluk, G. Why Man Climbs Mountains. Int. Rev. Sport Sociol. 1979, 14, 23–36. [Google Scholar] [CrossRef]
- Pan, S.; Ryan, C. Mountain areas and visitor usage–motivations and determinants of satisfaction: The case of Pirongia Forest Park, New Zealand. J. Sustain. Tour. 2007, 15, 288–308. [Google Scholar] [CrossRef]
- Mutz, M.; Müller, J. Mental health benefits of outdoor adventures: Results from two pilot studies. J. Adolesc. 2016, 49, 105–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, R. Tourism and Mental Health: Foundations, Frameworks, and Futures. J. Travel Res. 2022. [Google Scholar] [CrossRef]
- Pomfret, G. Conceptualising family adventure tourist motives, experiences and benefits. J. Outdoor Recreat. Tour. 2019, 28. [Google Scholar] [CrossRef]
- Pomfret, G.; Varley, P. Families at leisure outdoors: Well-being through adventure. Leis. Stud. 2019, 38, 494–508. [Google Scholar] [CrossRef]
- Boyes, M. Outdoor adventure and successful ageing. Ageing Soc. 2013, 33, 644–665. [Google Scholar] [CrossRef]
- Buckley, R. Nature sports, health and ageing: The value of euphoria. Ann. Leis. Res. 2020, 23, 92–109. [Google Scholar] [CrossRef] [Green Version]
- Zwart, R. An Exploratory Analysis of the Relationship between Outdoor Adventure Recreation Activity Type and Environmental Self-selection Strategies for Health Promotion; Indiana University: Bloomington, IN, USA, 2020. [Google Scholar]
- McCurdy, L.E.; Winterbottom, K.E.; Mehta, S.S.; Roberts, J.R. Using nature and outdoor activity to improve children’s health. Curr. Probl. Pediatric Adolesc. Health Care 2010, 40, 102–117. [Google Scholar] [CrossRef]
- Pretty, J.; Peacock, J.; Sellens, M.; Griffin, M. The mental and physical health outcomes of green exercise. Int. J. Environ. Health Res. 2005, 15, 319–337. [Google Scholar] [CrossRef]
- Thomsen, J.M.; Powell, R.B.; Monz, C. A systematic review of the physical and mental health benefits of wildland recreation. J. Park Recreat. Adm. 2018, 36. [Google Scholar] [CrossRef]
- Pasanen, T.P.; Tyrväinen, L.; Korpela, K.M. The relationship between perceived health and physical activity indoors, outdoors in built environments, and outdoors in nature. Appl. Psychol. Health Well-Being 2014, 6, 324–346. [Google Scholar] [CrossRef] [Green Version]
- Hamann, G.A.; Ivtzan, I. 30 minutes in nature a day can increase mood, well-being, meaning in life and mindfulness: Effects of a pilot programme. Soc. Inq. Into Well-Being 2016, 2, 34–46. [Google Scholar]
- Park, B.-J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of shinrin-yoku (taking in the atmosphere of the forest): Using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blonna, R. Coping with Stress in a Changing World; McGraw-Hill Humanities/Social Sciences/Languages: St Louis, MO, USA, 2006. [Google Scholar]
- Smith, M.S.; Wallston, K.A.; Smith, C.A. The development and validation of the Perceived Health Competence Scale. Health Educ. Res. 1995, 10, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Gomez, E.; Hill, E.; Zhu, X.; Freidt, B. Perceived Health Outcomes of Recreation Scale (PHORS): Reliability, Validity and Invariance. Meas. Phys. Educ. Exerc. Sci. 2016, 20, 27–37. [Google Scholar] [CrossRef]
- Tracy, S.J. Qualitative Research Methods; Wiley-Blackwell: Oxford, UK, 2013. [Google Scholar]
- Kaplan, R. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Hartig, T. Three steps to understanding restorative environments as health resources. Open Space People Space; Thompson, C.W., Travlow, P., Eds.; Taylor & Francis: Oxford, UK, 2007; pp. 163–179. [Google Scholar]
- Osborne, J.W. Best Practices in Quantitative Methods; Sage: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Driver, B.; Nash, R.; Haas, G. Wilderness benefits: A state-of-knowledge review. In Proceedings of the National Wilderness Research Conference: Issues, State of Knowledge, Future Directions, Fort Collins, CO, USA, 23–26 July 1987. [Google Scholar]
- Warner, S.E.; Shaw, J.M.; Dalsky, G.P. Bone mineral density of competitive male mountain and road cyclists. Bone 2002, 30, 281–286. [Google Scholar] [CrossRef]
- Lion, A.; Gauchard, G.C.; Deviterne, D.; Perrin, P.P. Differentiated influence of off-road and on-road cycling practice on balance control and the related-neurosensory organization. J. Electromyogr. Kinesiol. 2009, 19, 623–630. [Google Scholar] [CrossRef]
- Siegel, S.R.; Fryer, S.M. Rock climbing for promoting physical activity in youth. Am. J. Lifestyle Med. 2017, 11, 243–251. [Google Scholar] [CrossRef]
- Aras, D.; Akalan, C. Sport climbing as a means to improve health-related physical fitness parameters. J. Sports Med. Phys. Fit. 2015, 56, 1304–1310. [Google Scholar]
- Piff, P.K.; Dietze, P.; Feinberg, M.; Stancato, D.M.; Keltner, D. Awe, the small self, and prosocial behavior. J. Personal. Soc. Psychol. 2015, 108, 883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslow, A.H. Religions, Values and Peak-Experiences; Ohio State University Press: Columbus, OH, USA, 1964; Volume 51, p. 882888. [Google Scholar]
- Csikszentmihalyi, M.; Csikszentmihalyi, I. Adventure and the Flow Experience. In Adventure Programming; Miles, J.C., Priest, S., Eds.; Venture Publishing: State College, PA, USA, 1999; pp. 153–158. [Google Scholar]
- Ballew, M.T.; Omoto, A.M. Absorption: How nature experiences promote awe and other positive emotions. Ecopsychology 2018, 10, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Zeiler, M.; Peer, S.; Philipp, J.; Truttmann, S.; Wagner, G.; Karwautz, A.; Waldherr, K. Web-based versus paper-pencil assessment of behavioral problems using the youth self-report. Eur. J. Psychol. Assess. 2021, 37, 95–103. [Google Scholar] [CrossRef]
- Houge Mackenzie, S.; Brymer, E. Conceptualizing adventurous nature sport: A positive psychology perspective. Ann. Leis. Res. 2018, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Ewert, A.; Zwart, R.; Davidson, C. Underlying Motives for Selected Adventure Recreation Activities: The Case for Eudaimonics and Hedonics. Behav. Sci. 2020, 10, 185. [Google Scholar] [CrossRef]
- Jackson, S.B.; Stevenson, K.T.; Larson, L.R.; Peterson, M.N.; Seekamp, E. Connection to Nature Boosts Adolescents’ Mental Well-Being during the COVID-19 Pandemic. Sustainability 2021, 13, 12297. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Activity | Number of Participants in 2018 (000’s) | Percent of U.S. Population |
|---|---|---|
| Backpacking | 10,540 | 3.5% |
| Climbing | 5025 | 1.50% |
| Kayak (Sea) | 2805 | 0.90% |
| Kayak (Whitewater) | 2562 | 0.90% |
| Rafting | 3404 | 1.10% |
| Scuba diving | 2849 | 0.90% |
| Canoeing | 9129 | 3.00% |
| OAR Activity | Data Collection Location |
|---|---|
| Rock Climbing (RC) | Red River Gorge, Kentucky Linville Gorge, North Carolina Marquette, Michigan |
| Whitewater Boating (WW) | Gauley River, West Virginia Nantahala River, North Carolina |
| Mountain Biking (MTB) | Brown County, Indiana Asheville, North Carolina Marquette, Michigan |
| Activity | |||
|---|---|---|---|
| Mountain Bikers | Rock Climbers | Whitewater Boaters | |
| Age Range | 18–69 years | 19–68 years | 18–63 years |
| Gender | 33 females, 79 males, 1 other, 2 preferred not to answer | 42 females, 47 males, 1 other, 1 preferred not to answer | 28 females, 50 males |
| Race | 1 Other, 114 White | 3 Asian, 2 Other, 1 Black or African American, 84 White | 2 Asian, 3 Other, 73 White |
| Dependent Variable/Factors | Df | p | F-Test | n2 |
|---|---|---|---|---|
| Perceived Health Competence (PHCS) | 2 | 0.174 | 1.758 | 0.012 |
| Realization of a Psychological Experience (PSYC) | 2 | 0.999 | 0.001 | 0.000 |
| Prevention of a Worsening Condition (PREV) | 2 | 0.001 | 22.232 | 0.137 |
| Improved Condition (IMPV) | 2 | 0.001 | 7.400 | 0.050 |
| Variable | Activity | Mean | SD | Activity (I, J) | Mean Difference (I-J) | p |
|---|---|---|---|---|---|---|
| PREV | RC | 0.4110 | 0.16617 | RC, WW | 0.0096 | 0.934 |
| WW | 0.4206 | 0.17625 | RC, MTB | 0.1371 * | 0.000 | |
| MTB | 0.2739 | 0.18240 | WW, MTB | 0.1467 * | 0.000 | |
| IMPV | RC | 0.1545 | 0.13656 | RC, WW | 0.0705 * | 0.003 |
| WW | 0.2301 | 0.16339 | RC, MTB | 0.0003 | 1.000 | |
| MTB | 0.1548 | 0.14404 | WW, MTB | 0.0753 * | 0.002 |
| Mountain Biking | Whitewater Paddling | Rock Climbing |
|---|---|---|
| Natural Environment | Natural Environment | Social Group |
| Social Group | Social Group | Natural Environment |
| Physical Activity | Progression * | |
| Novelty * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwart, R.; Ewert, A. Human Health and Outdoor Adventure Recreation: Perceived Health Outcomes. Forests 2022, 13, 869. https://doi.org/10.3390/f13060869
Zwart R, Ewert A. Human Health and Outdoor Adventure Recreation: Perceived Health Outcomes. Forests. 2022; 13(6):869. https://doi.org/10.3390/f13060869
Chicago/Turabian StyleZwart, Ryan, and Alan Ewert. 2022. "Human Health and Outdoor Adventure Recreation: Perceived Health Outcomes" Forests 13, no. 6: 869. https://doi.org/10.3390/f13060869
APA StyleZwart, R., & Ewert, A. (2022). Human Health and Outdoor Adventure Recreation: Perceived Health Outcomes. Forests, 13(6), 869. https://doi.org/10.3390/f13060869