
Dimensional Accuracy of Regular- and Fast-Setting Vinyl Polysiloxane Impressions Using Customized Metal and Plastic Trays—An In Vitro Study



Abstract
1. Introduction
2. Materials and Methods
3. Results
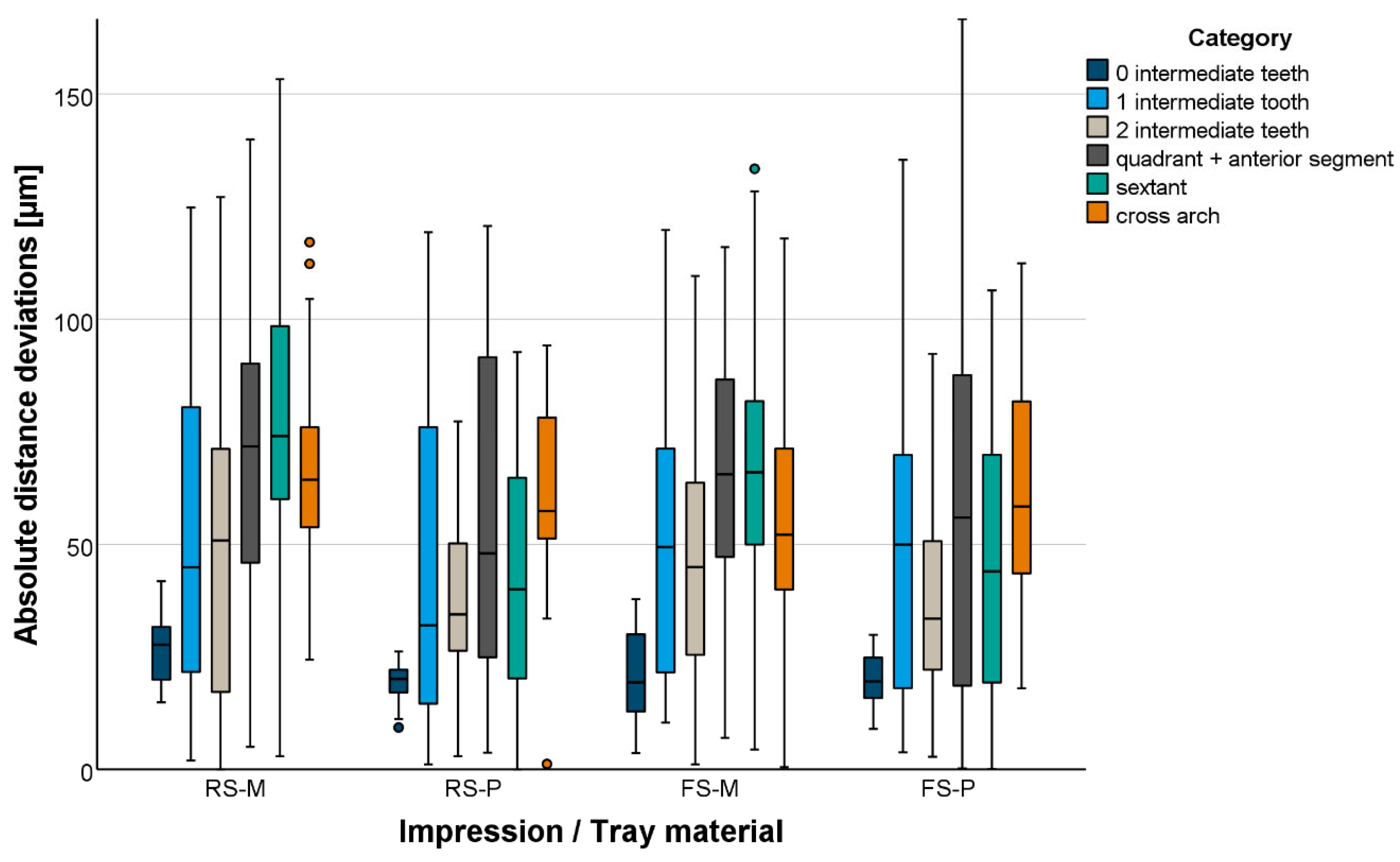
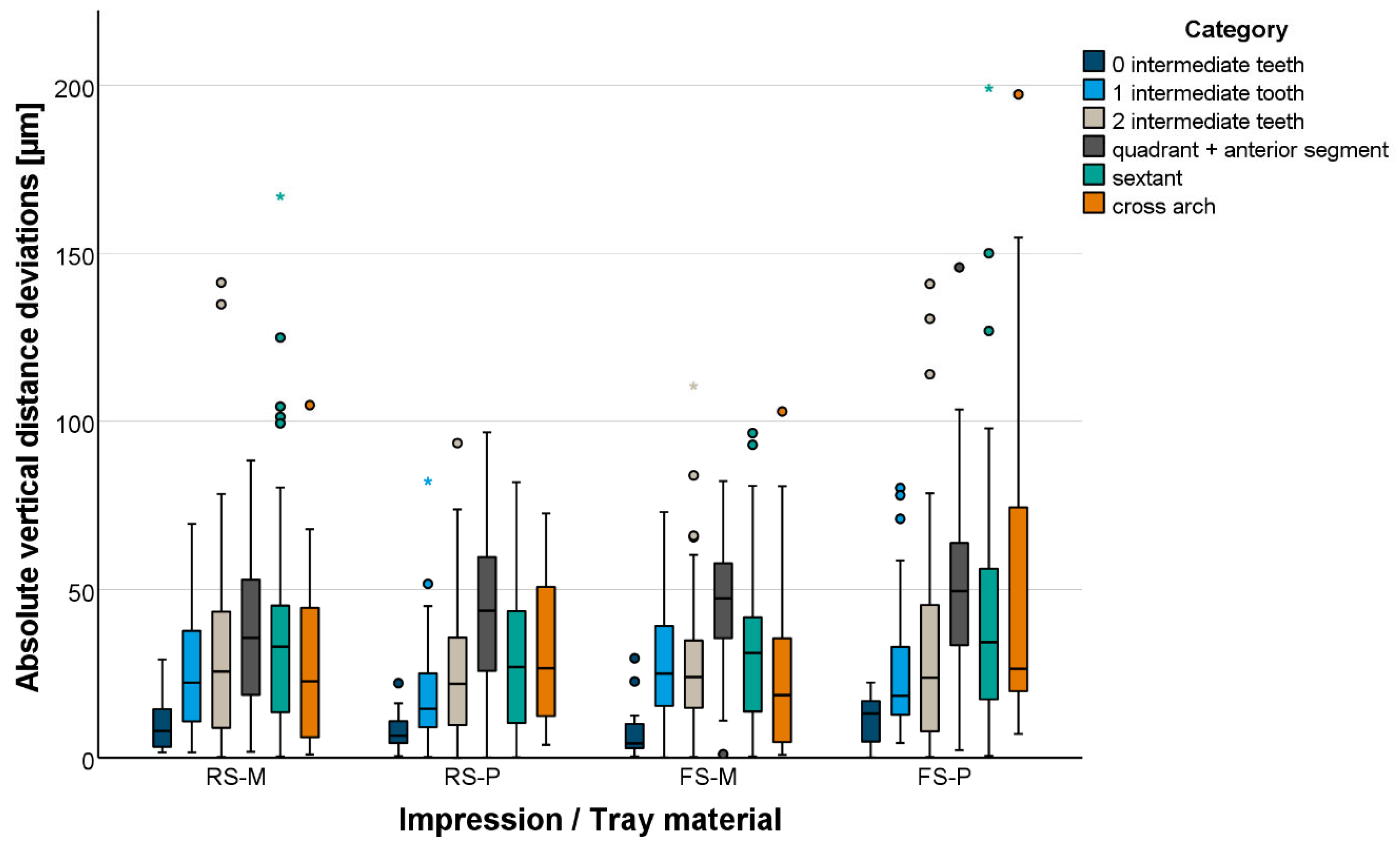
3.1. Global Accuracy
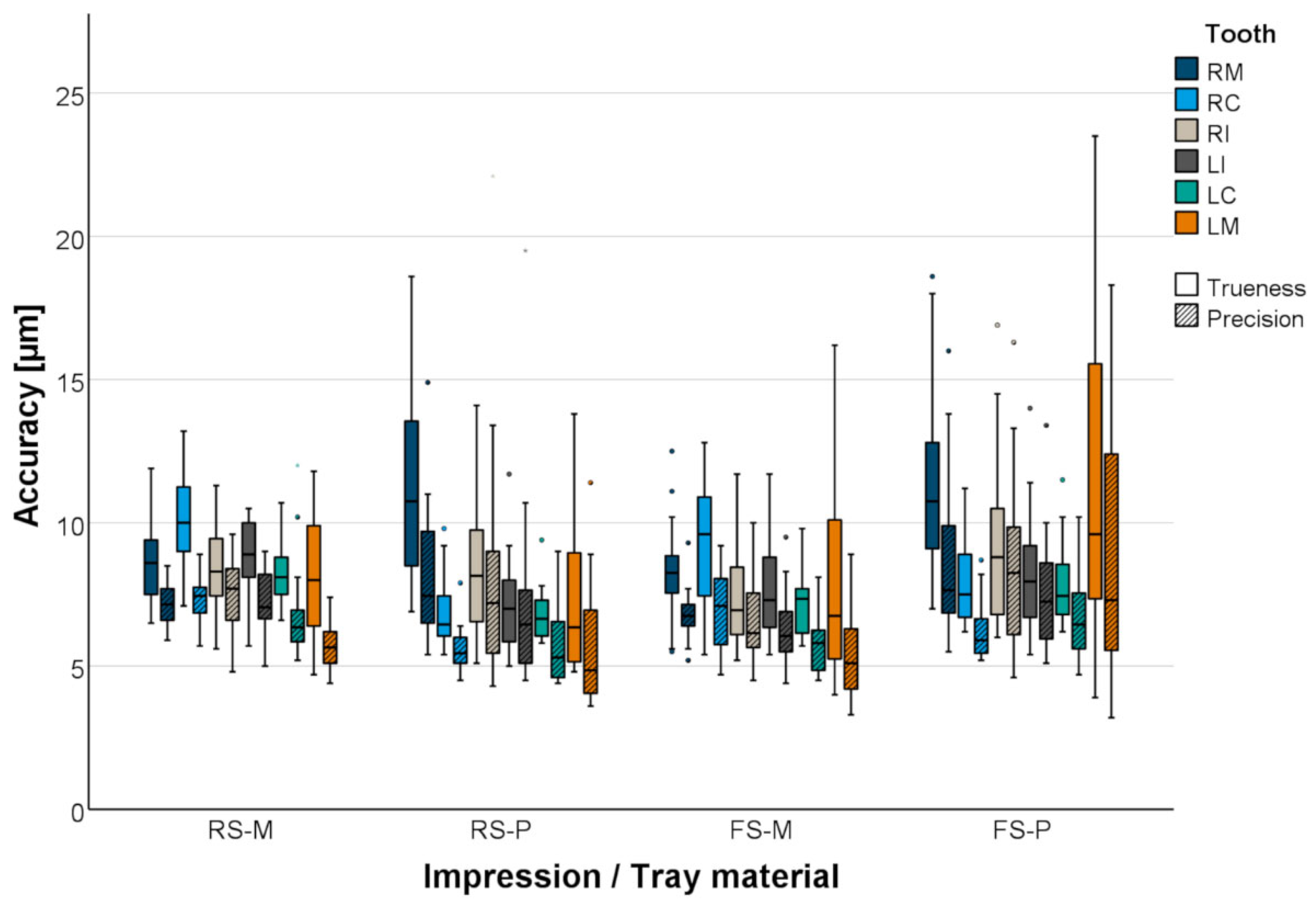
3.2. Local Accuracy
4. Discussion
5. Conclusions
- RS-VPS and FS-VPS have adequate accuracy in vitro, which suggests a successful clinical application.
- The use of metallic trays or plastic trays leads to adequate accuracy in vitro, which suggests a successful clinical application.
- Short distances are displayed more accurately than long distances regardless of material variant or tray material.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral. Health 2014, 14, 10. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406.e1. [Google Scholar] [PubMed]
- Chochlidakis, K.M.; Papaspyridakos, P.; Geminiani, A.; Chen, C.J.; Feng, I.J.; Ercoli, C. Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 184–190.e12. [Google Scholar] [CrossRef]
- Hasanzade, M.; Shirani, M.; Afrashtehfar, K.I.; Naseri, P.; Alikhasi, M. In Vivo and In Vitro Comparison of Internal and Marginal Fit of Digital and Conventional Impressions for Full-Coverage Fixed Restorations: A Systematic Review and Meta-analysis. J. Evid. Based Dent. Pract. 2019, 19, 236–254. [Google Scholar]
- Hamalian, T.A.; Nasr, E.; Chidiac, J.J. Impression materials in fixed prosthodontics: Influence of choice on clinical procedure. J. Prosthodont. 2011, 20, 153–160. [Google Scholar] [PubMed]
- Jayaraman, S.; Singh, B.P.; Ramanathan, B.; Pillai, M.P.; MacDonald, L.; Kirubakaran, R. Final-impression techniques and materials for making complete and removable partial dentures. Cochrane Database Syst. Rev. 2018, 4, CD012256. [Google Scholar] [PubMed]
- Huettig, F.; Klink, A.; Kohler, A.; Mutschler, M.; Rupp, F. Flowability, Tear Strength, and Hydrophilicity of Current Elastomers for Dental Impressions. Materials 2021, 14, 2994. [Google Scholar] [CrossRef]
- Guo, Y.Q.; Ma, Y.; Cai, S.N.; Yu, H. Optimal impression materials for implant-supported fixed complete dentures: A systematic review and meta-analysis. J. Prosthet. Dent. 2023. epub ahead of print. [Google Scholar] [CrossRef]
- Sailer, I.; Mühlemann, S.; Fehmer, V.; Hämmerle, C.H.F.; Benic, G.I. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic fixed partial dentures. Part I: Time efficiency of complete-arch digital scans versus conventional impressions. J. Prosthet. Dent. 2019, 121, 69–75. [Google Scholar] [CrossRef]
- Joda, T.; Bragger, U. Patient-centered outcomes comparing digital and conventional implant impression procedures: A randomized crossover trial. Clin. Oral. Implants Res. 2016, 27, e185–e189. [Google Scholar]
- Grunheid, T.; McCarthy, S.D.; Larson, B.E. Clinical use of a direct chairside oral scanner: An assessment of accuracy, time, and patient acceptance. Am. J. Orthod. Dentofacial Orthop. 2014, 146, 673–682. [Google Scholar] [CrossRef]
- Gjelvold, B.; Chrcanovic, B.R.; Korduner, E.K.; Collin-Bagewitz, I.; Kisch, J. Intraoral Digital Impression Technique Compared to Conventional Impression Technique. A Randomized Clinical Trial. J. Prosthodont. 2016, 25, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Bragger, U. Time-Efficiency Analysis Comparing Digital and Conventional Workflows for Implant Crowns: A Prospective Clinical Crossover Trial. Int. J. Oral. Maxillofac. Implants 2015, 30, 1047–1053. [Google Scholar] [CrossRef]
- Luthardt, R.G.; Walter, M.H.; Quaas, S.; Koch, R.; Rudolph, H. Comparison of the three-dimensional correctness of impression techniques: A randomized controlled trial. Quintessence Int. 2010, 41, 845–853. [Google Scholar] [PubMed]
- Luthardt, R.G.; Walter, M.H.; Weber, A.; Koch, R.; Rudolph, H. Clinical parameters influencing the accuracy of 1- and 2-stage impressions: A randomized controlled trial. Int. J. Prosthodont. 2008, 21, 322–327. [Google Scholar] [PubMed]
- Wöstmann, B.; Rehmann, P.; Trost, D.; Balkenhol, M. Effect of different retraction and impression techniques on the marginal fit of crowns. J. Dent. 2008, 36, 508–512. [Google Scholar] [CrossRef]
- Wöstmann, B.; Rehmann, P.; Balkenhol, M. Influence of different retraction techniques on crevicular fluid flow. Int. J. Prosthodont. 2008, 21, 215–216. [Google Scholar]
- Rues, S.; Stober, T.; Bargum, T.; Rammelsberg, P.; Zenthöfer, A. Disposable plastic trays and their effect on polyether and vinyl polysiloxane impression accuracy—An in vitro study. Clin. Oral. Investig. 2021, 25, 1475–1484. [Google Scholar] [CrossRef]
- Waldecker, M.; Rues, S.; Rammelsberg, P.; Bömicke, W. Dimensional Accuracy of Novel Vinyl Polysiloxane Compared with Polyether Impression Materials: An In Vitro Study. Materials 2024, 17, 4221. [Google Scholar] [CrossRef]
- Zenthöfer, A.; Rues, S.; Rammelsberg, P.; Ruckes, D.; Stober, T. Accuracy of a New Fast-Setting Polyether Impression Material. Int. J. Prosthodont. 2020, 33, 410–417. [Google Scholar] [CrossRef]
- Carrotte, P.V.; Johnson, A.; Winstanley, R.B. The influence of the impression tray on the accuracy of impressions for crown and bridge work--an investigation and review. Br. Dent. J. 1998, 185, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Hoyos, A.; Soderholm, K.J. Influence of tray rigidity and impression technique on accuracy of polyvinyl siloxane impressions. Int. J. Prosthodont. 2011, 24, 49–54. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Group | Impression Material | Tray Material |
|---|---|---|
| RS-M | Aquasil Ultra+ Heavy Regular Set/Aquasil Ultra+ XLV Regular Set | Metal |
| RS-P | Plastic | |
| FS-M | Aquasil Ultra+ Heavy Fast Set/Aquasil Ultra+ XLV Fast Set | Metal |
| FS-P | Plastic |
| Level | Distance Category | Distance |
|---|---|---|
| Precision ball | No intermediate precision ball | P1–P4, P2–P5, P3–P4, P3–P5 |
| 1 intermediate precision ball | P1–P3, P2–P3, P4–P5 | |
| 2 intermediate precision balls | P1–P5, P2–P4 | |
| 3 intermediate precision balls | P1–P2 | |
| Prepared teeth | No intermediate tooth | RI-LI |
| 1 intermediate tooth | RI-RC, LI-LC | |
| 2 intermediate teeth | RC-RM, LC-LM, RC-LI, RI-LC | |
| Quadrant + anterior segment | RI-RM, LI-LM, RC-LC | |
| Sextant | RM-LC, RC-LM | |
| Cross-arch | RM-LM |
| Test Group | Level | Distance | Distance Deviations [µm] | ||||
|---|---|---|---|---|---|---|---|
| Mean Value | Standard Deviation | Minimum | Median | Maximum | |||
| RS-M | Precision ball | P1–P2 | 75 | 25 | 27 | 78 | 113 |
| P1–P3 | 72 | 21 | 33 | 74 | 110 | ||
| P1–P4 | 42 | 15 | 8 | 42 | 76 | ||
| P1–P5 | 77 | 29 | 23 | 83 | 146 | ||
| P2–P3 | 80 | 22 | 32 | 79 | 122 | ||
| P2–P4 | 89 | 26 | 46 | 93 | 134 | ||
| P2–P5 | 52 | 21 | 12 | 47 | 103 | ||
| P3–P4 | 40 | 19 | 4 | 42 | 74 | ||
| P3–P5 | 33 | 13 | 6 | 30 | 57 | ||
| P4–P5 | 60 | 23 | 6 | 61 | 103 | ||
| Prepared teeth | RM-RC | 16 | 14 | 0 | 12 | 60 | |
| RM-RI | 81 | 29 | 27 | 79 | 140 | ||
| RM-LI | 55 | 28 | 6 | 59 | 123 | ||
| RM-LC | 78 | 32 | 14 | 73 | 146 | ||
| RM-LM | 68 | 24 | 24 | 64 | 117 | ||
| RC-RI | 72 | 26 | 22 | 80 | 125 | ||
| RC-LI | 65 | 29 | 9 | 71 | 127 | ||
| RC-LC | 81 | 36 | 22 | 75 | 150 | ||
| RC-LM | 79 | 36 | 3 | 74 | 153 | ||
| RI-LI | 27 | 8 | 15 | 28 | 42 | ||
| RI-LC | 64 | 26 | 9 | 68 | 108 | ||
| RI-LM | 104 | 35 | 16 | 103 | 176 | ||
| LI-LC | 27 | 16 | 2 | 22 | 55 | ||
| LI-LM | 58 | 30 | 5 | 52 | 113 | ||
| LC-LM | 48 | 24 | 0 | 49 | 94 | ||
| RS-P | Precision ball | P1–P2 | 60 | 27 | 1 | 66 | 94 |
| P1–P3 | 43 | 17 | 10 | 44 | 72 | ||
| P1–P4 | 20 | 13 | 1 | 22 | 46 | ||
| P1–P5 | 59 | 22 | 23 | 62 | 104 | ||
| P2–P3 | 54 | 15 | 29 | 53 | 78 | ||
| P2–P4 | 71 | 21 | 30 | 70 | 100 | ||
| P2–P5 | 35 | 14 | 13 | 37 | 63 | ||
| P3–P4 | 31 | 12 | 1 | 31 | 45 | ||
| P3–P5 | 25 | 13 | 4 | 25 | 47 | ||
| P4–P5 | 55 | 18 | 10 | 56 | 86 | ||
| Prepared teeth | RM-RC | 29 | 19 | 4 | 28 | 76 | |
| RM-RI | 85 | 24 | 10 | 92 | 121 | ||
| RM-LI | 54 | 16 | 19 | 58 | 82 | ||
| RM-LC | 68 | 17 | 24 | 71 | 93 | ||
| RM-LM | 60 | 22 | 1 | 57 | 94 | ||
| RC-RI | 72 | 21 | 17 | 76 | 119 | ||
| RC-LI | 47 | 16 | 3 | 49 | 77 | ||
| RC-LC | 33 | 20 | 1 | 30 | 69 | ||
| RC-LM | 23 | 18 | 0 | 23 | 69 | ||
| RI-LI | 19 | 5 | 9 | 20 | 26 | ||
| RI-LC | 43 | 15 | 10 | 44 | 71 | ||
| RI-LM | 76 | 15 | 42 | 77 | 101 | ||
| LI-LC | 16 | 10 | 1 | 15 | 33 | ||
| LI-LM | 26 | 14 | 4 | 29 | 50 | ||
| LC-LM | 28 | 13 | 4 | 30 | 57 | ||
| FS-M | Precision ball | P1–P2 | 60 | 29 | 11 | 60 | 112 |
| P1–P3 | 65 | 32 | 4 | 66 | 118 | ||
| P1–P4 | 33 | 25 | 0 | 36 | 76 | ||
| P1–P5 | 69 | 29 | 20 | 69 | 129 | ||
| P2–P3 | 64 | 28 | 5 | 64 | 119 | ||
| P2–P4 | 72 | 28 | 6 | 82 | 107 | ||
| P2–P5 | 44 | 23 | 5 | 40 | 103 | ||
| P3–P4 | 39 | 14 | 7 | 37 | 73 | ||
| P3–P5 | 29 | 9 | 14 | 27 | 47 | ||
| P4–P5 | 54 | 20 | 10 | 58 | 89 | ||
| Prepared teeth | RM-RC | 21 | 18 | 1 | 16 | 68 | |
| RM-RI | 75 | 21 | 32 | 74 | 116 | ||
| RM-LI | 55 | 20 | 8 | 51 | 92 | ||
| RM-LC | 68 | 18 | 23 | 67 | 99 | ||
| RM-LM | 57 | 28 | 1 | 52 | 118 | ||
| RC-RI | 69 | 20 | 31 | 70 | 120 | ||
| RC-LI | 61 | 23 | 15 | 58 | 110 | ||
| RC-LC | 71 | 27 | 19 | 68 | 122 | ||
| RC-LM | 64 | 35 | 4 | 62 | 133 | ||
| RI-LI | 21 | 10 | 4 | 19 | 38 | ||
| RI-LC | 59 | 17 | 31 | 64 | 95 | ||
| RI-LM | 92 | 20 | 59 | 92 | 133 | ||
| LI-LC | 29 | 18 | 10 | 22 | 77 | ||
| LI-LM | 55 | 28 | 7 | 49 | 110 | ||
| LC-LM | 38 | 22 | 3 | 38 | 91 | ||
| FS-P | Precision ball | P1–P2 | 54 | 34 | 3 | 54 | 129 |
| P1–P3 | 44 | 28 | 3 | 44 | 98 | ||
| P1–P4 | 25 | 20 | 2 | 18 | 77 | ||
| P1–P5 | 54 | 34 | 8 | 45 | 131 | ||
| P2–P3 | 43 | 23 | 2 | 40 | 101 | ||
| P2–P4 | 57 | 26 | 20 | 55 | 121 | ||
| P2–P5 | 29 | 18 | 1 | 27 | 68 | ||
| P3–P4 | 32 | 18 | 4 | 33 | 67 | ||
| P3–P5 | 18 | 14 | 0 | 19 | 49 | ||
| P4–P5 | 46 | 23 | 20 | 46 | 95 | ||
| Prepared teeth | RM-RC | 29 | 22 | 3 | 24 | 92 | |
| RM-RI | 87 | 29 | 51 | 79 | 169 | ||
| RM-LI | 55 | 22 | 18 | 56 | 95 | ||
| RM-LC | 73 | 20 | 33 | 72 | 106 | ||
| RM-LM | 62 | 27 | 18 | 58 | 112 | ||
| RC-RI | 74 | 26 | 42 | 70 | 135 | ||
| RC-LI | 50 | 15 | 25 | 52 | 75 | ||
| RC-LC | 35 | 26 | 7 | 31 | 104 | ||
| RC-LM | 35 | 28 | 0 | 32 | 105 | ||
| RI-LI | 20 | 5 | 9 | 20 | 30 | ||
| RI-LC | 35 | 20 | 6 | 31 | 79 | ||
| RI-LM | 66 | 17 | 23 | 64 | 106 | ||
| LI-LC | 25 | 19 | 4 | 18 | 61 | ||
| LI-LM | 22 | 20 | 0 | 19 | 88 | ||
| LC-LM | 31 | 14 | 7 | 30 | 59 | ||
| Test Group | Category | Angular Deviations [°] | ||||
|---|---|---|---|---|---|---|
| Mean Value | Standard Deviation | Minimum | Median | Maximum | ||
| RS-M | 0 intermediate teeth | 0.10 | 0.07 | 0.02 | 0.10 | 0.27 |
| 1 intermediate tooth | 0.17 | 0.11 | 0.01 | 0.16 | 0.43 | |
| 2 intermediate teeth | 0.18 | 0.10 | 0.00 | 0.14 | 0.50 | |
| Quadrant + anterior segment | 0.14 | 0.08 | 0.03 | 0.14 | 0.38 | |
| Sextant | 0.32 | 0.08 | 0.15 | 0.31 | 0.53 | |
| Cross-arch | 0.21 | 0.09 | 0.04 | 0.19 | 0.39 | |
| RS-P | 0 intermediate teeth | 0.10 | 0.03 | 0.04 | 0.09 | 0.14 |
| 1 intermediate tooth | 0.16 | 0.12 | 0.00 | 0.13 | 0.50 | |
| 2 intermediate teeth | 0.17 | 0.09 | 0.01 | 0.15 | 0.45 | |
| Quadrant + anterior segment | 0.24 | 0.14 | 0.00 | 0.24 | 0.66 | |
| Sextant | 0.33 | 0.15 | 0.01 | 0.32 | 0.61 | |
| Cross-arch | 0.47 | 0.20 | 0.07 | 0.46 | 0.78 | |
| FS-M | 0 intermediate teeth | 0.08 | 0.04 | 0.03 | 0.08 | 0.16 |
| 1 intermediate tooth | 0.17 | 0.10 | 0.02 | 0.15 | 0.49 | |
| 2 intermediate teeth | 0.13 | 0.10 | 0.02 | 0.10 | 0.51 | |
| Quadrant + anterior segment | 0.16 | 0.09 | 0.02 | 0.14 | 0.38 | |
| Sextant | 0.25 | 0.09 | 0.06 | 0.25 | 0.40 | |
| Cross-arch | 0.23 | 0.09 | 0.08 | 0.24 | 0.38 | |
| FS-P | 0 intermediate teeth | 0.09 | 0.03 | 0.04 | 0.08 | 0.15 |
| 1 intermediate tooth | 0.18 | 0.14 | 0.01 | 0.14 | 0.58 | |
| 2 intermediate teeth | 0.19 | 0.11 | 0.02 | 0.16 | 0.57 | |
| Quadrant + anterior segment | 0.30 | 0.17 | 0.07 | 0.26 | 0.74 | |
| Sextant | 0.39 | 0.25 | 0.06 | 0.33 | 1.18 | |
| Cross-arch | 0.57 | 0.31 | 0.07 | 0.55 | 1.31 | |
| Test Group | Prepared Tooth | Accuracy [µm] | ||||
|---|---|---|---|---|---|---|
| Mean Value | Standard Deviation | Minimum | Median | Maximum | ||
| RS-M | RM | 9 (7) | 1 (1) | 7 (6) | 9 (7) | 12 (9) |
| RC | 10 (7) | 2 (1) | 7 (6) | 10 (7) | 13 (9) | |
| RI | 8 (8) | 1 (1) | 6 (5) | 8 (8) | 11 (10) | |
| LI | 9 (7) | 1 (1) | 6 (5) | 9 (7) | 11 (9) | |
| LC | 8 (7) | 1 (2) | 7 (5) | 8 (6) | 11 (12) | |
| LM | 8 (6) | 2 (1) | 5 (4) | 8 (6) | 12 (7) | |
| RS-P | RM | 11 (8) | 3 (2) | 7 (5) | 11 (7) | 19 (15) |
| RC | 7 (6) | 1 (1) | 5 (5) | 6 (5) | 10 (8) | |
| RI | 8 (8) | 2 (4) | 5 (4) | 8 (7) | 14 (22) | |
| LI | 7 (7) | 2 (3) | 5 (5) | 7 (6) | 12 (20) | |
| LC | 7 (6) | 1 (1) | 6 (4) | 7 (5) | 9 (9) | |
| LM | 7 (6) | 3 (2) | 5 (4) | 6 (5) | 14 (11) | |
| FS-M | RM | 8 (7) | 2 (1) | 6 (5) | 8 (7) | 13 (9) |
| RC | 9 (7) | 2 (1) | 5 (5) | 10 (7) | 13 (9) | |
| RI | 7 (7) | 2 (1) | 5 (5) | 7 (6) | 12 (10) | |
| LI | 8 (6) | 2 (1) | 5 (4) | 7 (6) | 12 (10) | |
| LC | 7 (6) | 1 (1) | 6 (5) | 7 (6) | 10 (8) | |
| LM | 8 (5) | 3 (2) | 4 (3) | 7 (5) | 16 (9) | |
| FS-P | RM | 11 (9) | 3 (3) | 7 (6) | 11 (8) | 19 (16) |
| RC | 8 (6) | 2 (1) | 6 (5) | 8 (6) | 11 (9) | |
| RI | 9 (8) | 3 (3) | 6 (5) | 9 (8) | 17 (16) | |
| LI | 8 (8) | 2 (2) | 5 (5) | 8 (7) | 14 (13) | |
| LC | 8 (7) | 1 (1) | 6 (5) | 7 (6) | 12 (10) | |
| LM | 11 (9) | 6 (5) | 4 (3) | 10 (7) | 24 (18) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waldecker, M.; Jetter, K.; Rues, S.; Rammelsberg, P.; Zenthöfer, A. Dimensional Accuracy of Regular- and Fast-Setting Vinyl Polysiloxane Impressions Using Customized Metal and Plastic Trays—An In Vitro Study. Materials 2025, 18, 2164. https://doi.org/10.3390/ma18092164
Waldecker M, Jetter K, Rues S, Rammelsberg P, Zenthöfer A. Dimensional Accuracy of Regular- and Fast-Setting Vinyl Polysiloxane Impressions Using Customized Metal and Plastic Trays—An In Vitro Study. Materials. 2025; 18(9):2164. https://doi.org/10.3390/ma18092164
Chicago/Turabian StyleWaldecker, Moritz, Karla Jetter, Stefan Rues, Peter Rammelsberg, and Andreas Zenthöfer. 2025. "Dimensional Accuracy of Regular- and Fast-Setting Vinyl Polysiloxane Impressions Using Customized Metal and Plastic Trays—An In Vitro Study" Materials 18, no. 9: 2164. https://doi.org/10.3390/ma18092164
APA StyleWaldecker, M., Jetter, K., Rues, S., Rammelsberg, P., & Zenthöfer, A. (2025). Dimensional Accuracy of Regular- and Fast-Setting Vinyl Polysiloxane Impressions Using Customized Metal and Plastic Trays—An In Vitro Study. Materials, 18(9), 2164. https://doi.org/10.3390/ma18092164