
Accuracy Evaluation of Indirect Bonding Techniques for Clear Aligner Attachments Using 3D-Printed Models: An In Silico and Physical Model-Based Study

 ,
,  and
and 
Highlights
- Attachment Bonding Accuracy: The study evaluates the precision of bonding horizontal vs. vertical orthodontic clear aligner attachments.
- Study Design: 140 attachments (70 horizontal, 70 vertical) bonded on 10 anatomically based acrylic resin models, analyzed using digital imaging and cephalometric measurements.
- Key Findings: Vertical attachments showed superior bonding accuracy compared to horizontal attachments, except for two cephalometric parameters (PAPver and PMVhor).
- Clinical Relevance: These results suggest vertical attachments may provide better predictability in clear aligner therapy when using an indirect bonding technique.
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Procedure
2.3. Alignment Procedure
2.4. Measurement Procedure
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paglia, L.; Marzo, G. Aligners, can my child use them too? Eur. J. Paediatr. Dent. 2023, 24, 259. [Google Scholar]
- Bolas-Colvee, B.; Tarazona, B.; Paredes-Gallardo, V.; Arias-De Luxan, S. Relationship between perception of smile esthetics and orthodontic treatment in Spanish patients. PLoS ONE 2018, 13, e0201102. [Google Scholar] [CrossRef] [PubMed]
- Saccomanno, S.; Saran, S.; Laganà, D.; Mastrapasqua, R.F.; Grippaudo, C. Motivation, Perception, and Behavior of the Adult Orthodontic Patient: A Survey Analysis. BioMed Res. Int. 2022, 4, 2754051. [Google Scholar] [CrossRef]
- Alhasyimi, A.A.; Ayub, A.; Farmasyanti, C.A. Effectiveness of the Attachment Design and Thickness of Clear Aligners during Orthodontic Anterior Retraction: Finite Element Analysis. Eur. J. Dent. 2024, 18, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Baron, P. Les appareils orthodontiques invisibles et presque invisibles [Invisible and almost invisible orthodontic appliances]. L’Orthodontie Française 2014, 85, 59–91. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Du, Y.; Yang, K. Comparison of pain intensity and impacts on oral health-related quality of life between orthodontic patients treated with clear aligners and fixed appliances: A systematic review and meta-analysis. BMC Oral Health 2023, 23, 920. [Google Scholar] [CrossRef]
- Mendes Ribeiro, S.M.; Aragón, M.L.S.C.; Espinosa, D.D.S.G.; Shibasaki, W.M.M.; Normando, D. Orthodontic aligners: Between passion and science. Dent. Press J. Orthod. 2024, 28, e23spe6. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Huang, X.; Huo, S.; Zhang, C.; Zhao, S.; Cen, X.; Zhao, Z. Effect of clear aligners on oral health-related quality of life: A systematic review. Orthod. Craniofacial Res. 2020, 23, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Alami, S.; Sahim, S.; Hilal, F.; Essamlali, A.; El Quars, F. Perception and satisfaction of patients treated with orthodontic clear aligners. Open Access Lib J. 2022, 9, e9300. [Google Scholar] [CrossRef]
- Chhibber, A.; Agarwal, S.; Yadav, S.; Kuo, C.-L.; Upadhyay, M. Which orthodontic appliance is best for oral hygiene? A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Abay, F.; Buyuk, S.K.; Korkmaz, Y.N. Prevalence of white spot lesions during clear aligner therapy: A systematic review. Australas. Orthod. J. 2022, 38, 368–379. [Google Scholar] [CrossRef]
- Galluccio, G. Is the use of clear aligners a real critical change in oral health prevention and treatment? Clin. Ter. 2021, 172, 113–115. [Google Scholar] [PubMed]
- Zheng, M.; Liu, R.; Ni, Z.; Yu, Z. Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod. Craniofacial Res. 2017, 20, 127–133. [Google Scholar] [CrossRef]
- AlMogbel, A. Clear Aligner Therapy: Up to date review article. J. Orthod. Sci. 2023, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.Q.; Xiang, F.; Fan, M.Y.; Song, Y.; Wang, X.H.; Zhang, L.; Qian, W.H. Clinical efficacy of the combination of miniscrew with clear aligner in controlling the roller coaster effect. Shanghai Kou Qiang Yi Xue 2022, 31, 193–197. [Google Scholar]
- Bellocchio, A.M.; Portelli, M.; Ciraolo, L.; Ciancio, E.; Militi, A.; Peditto, M.; Barbera, S.; Nucera, R. Evaluation of the Clinical Variables Affecting Attachment Reproduction Accuracy during Clear Aligner Therapy. Materials 2023, 16, 6811. [Google Scholar] [CrossRef] [PubMed]
- Putrino, A.; Barbato, E.; Galluccio, G. Clear Aligners: Between Evolution and Efficiency—A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2870. [Google Scholar] [CrossRef]
- Castroflorio, T.; Sedran, A.; Parrini, S.; Garino, F.; Reverdito, M.; Capuozzo, R.; Mutinelli, S.; Grybauskas, S.; Vaitiekūnas, M.; Deregibus, A. Predictability of orthodontic tooth movement with aligners: Effect of treatment design. Prog. Orthod. 2023, 24, 2. [Google Scholar] [CrossRef]
- Nucera, R.; Dolci, C.; Bellocchio, A.M.; Costa, S.; Barbera, S.; Rustico, L.; Farronato, M.; Militi, A.; Portelli, M. Effects of Composite Attachments on Orthodontic Clear Aligners Therapy: A Systematic Review. Materials 2022, 15, 533. [Google Scholar] [CrossRef]
- Gazzani, F.; Bellisario, D.; Quadrini, F.; Danesi, C.; Alberti, A.; Cozza, P.; Pavoni, C. Light-curing process for clear aligners’ attachment reproduction: Comparison between two nanocomposites cured by the auxiliary of a new tool. BMC Oral Health 2022, 22, 376. [Google Scholar] [CrossRef]
- Jedliński, M.; Mazur, M.; Greco, M.; Belfus, J.; Grocholewicz, K.; Janiszewska-Olszowska, J. Attachments for the Orthodontic Aligner Treatment-State of the Art-A Comprehensive Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4481. [Google Scholar] [CrossRef] [PubMed]
- Yaosen, C.; Mohamed, A.M.; Jinbo, W.; Ziwei, Z.; Al-Balaa, M.; Yan, Y. Risk Factors of Composite Attachment Loss in Orthodontic Patients During Orthodontic Clear Aligner Therapy: A Prospective Study. BioMed Res. Int. 2021, 23, 6620377. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Yang, K. Surface wear of attachments in patients during clear aligner therapy: A prospective clinical study. Prog. Orthod. 2024, 25, 7. [Google Scholar] [CrossRef]
- Brandão, N.M.C.B.; Maia, R.M.; Gomes, V.M.; Resende, C.; Antunes, A.N.D.G.; Souki, B.Q. Bonding positional accuracy of attachments and marginal adaptation of in-house aligners—A quality improvement laboratory study. Orthod. Craniofacial Res. 2024, 27 (Suppl. S2), 120–130. [Google Scholar] [CrossRef]
- Topsakal, K.G.; Gökmen, Ş.; Yurdakurban, E.; Duran, G.S.; Görgülü, S. The effect of layer thıckness on the accuracy of the dıfferent ın-house clear alıgner attachments. Clin. Oral Investig. 2023, 27, 5331–5341. [Google Scholar] [CrossRef]
- Narongdej, P.; Hassanpour, M.; Alterman, N.; Rawlins-Buchanan, F.; Barjasteh, E. Advancements in Clear Aligner Fabrication: A Comprehensive Review of Direct-3D Printing Technologies. Polymers 2024, 16, 371. [Google Scholar] [CrossRef] [PubMed]
- Aljabaa, A.H. Clear Aligner Therapy—Narrative Review. J. Int. Oral Health 2020, 12, S1–S4. [Google Scholar] [CrossRef]
- Moutawakil, A. Biomechanics of aligners: Literature Review. Adv. Dent. Oral Health 2021, 13, 555872. [Google Scholar] [CrossRef]
- Katib, H.S.; Hakami, A.M.; Albalawei, M.; Alhajri, S.A.; Alruwaily, M.S.; Almusallam, M.I.; Alqahtani, G.H. Stability and Success of Clear Aligners in Orthodontics: A Narrative Review. Cureus 2024, 16, e52038. [Google Scholar] [CrossRef]
- Yu, X.; Li, G.; Zheng, Y.; Gao, J.; Fu, Y.; Wang, Q.; Huang, L.; Pan, X.; Ding, J. ‘Invisible’ orthodontics by polymeric ‘clear’ aligners molded on 3D-printed personalized dental models. Regen. Biomater. 2022, 9, rbac007. [Google Scholar] [CrossRef]
- Izhar, A.; Singh, G.; Goyal, V.; Singh, R.; Gupta, N.; Pahuja, P. Comparative Assessment of Clinical and Predicted Treatment Outcomes of Clear Aligner Treatment: An in Vivo Study. Turk. J. Orthod. 2019, 32, 229–235. [Google Scholar] [CrossRef]
- Upadhyay, M.; Arqub, S.A. Biomechanics of Clear Aligners: Hidden Truths & First Principles. J. World Fed. Orthod. 2022, 11, 12–21. [Google Scholar]
- Lombardo, L.; Palone, M.; Carlucci, A.; Siciliani, G. Clear Aligner Hybrid Approach: A Case Report. J. World Fed. Orthod. 2020, 9, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Weir, T. Clear Aligners in Orthodontic Treatment. Aust. Dent. J. 2017, 62, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Elshazly, T.M.; Keilig, L.; Salvatori, D.; Chavanne, P.; Aldesoki, M.; Bourauel, C. Effect of Trimming Line Design and Edge Extension of Orthodontic Aligners on Force Transmission: An in Vitro Study. J. Dent. 2022, 125, 104276. [Google Scholar] [CrossRef] [PubMed]
- Ammann, R.; Tanner, C.; Schulz, G.; Osmani, B.; Nalabothu, P.; Töpper, T.; Müller, B. Three-Dimensional Analysis of Aligner Gaps and Thickness Distributions, Using Hard X-ray Tomography with Micrometer Resolution. J. Med. Imaging 2022, 9, 031509. [Google Scholar] [CrossRef]
- Ho, C.-T.; Huang, Y.-T.; Chao, C.-W.; Huang, T.-H.; Kao, C.-T. Effects of Different Aligner Materials and Attachments on Orthodontic Behavior. J. Dent. Sci. 2021, 16, 1001–1009. [Google Scholar] [CrossRef]
- Hartshorne, J.; Wertheimer, M.B. Emerging Insights and New Developments in Clear Aligner Therapy: A Review of the Literature. AJO-DO Clin. Companion 2022, 2, 311–324. [Google Scholar] [CrossRef]
- Panayi, N.C. Directly Printed Aligner: Aligning with the Future. Turk. J. Orthod. 2023, 36, 62–69. [Google Scholar] [CrossRef] [PubMed]
- ISO 20795-2; Dentistry—Base polymers. Part 2: Orthodontic Base Polymers. International Organization for Standardization: Geneva, Switzerland, 2013.
- Meto, A.; Colombari, B.; Castagnoli, A.; Sarti, M.; Denti, L.; Blasi, E. Efficacy of a Copper-Calcium-Hydroxide Solution in Reducing Microbial Plaque on Orthodontic Clear Aligners: A Case Report. Eur. J. Dent. 2019, 13, 478–484. [Google Scholar] [CrossRef]
- Fiorillo, G.; Campobasso, A.; Croce, S.; Hussain, U.; Battista, G.; Lo Muzio, E.; Mandelli, G.; Ambrosi, A.; Gastaldi, G. Accuracy of clear aligners in the orthodontic rotational movement using different attachment configurations. Orthod. Craniofacial Res. 2024, 27, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Valeri, C.; Aloisio, A.; Mummolo, S.; Quinzi, V. Performance of Rigid and Soft Transfer Templates Using Viscous and Fluid Resin-Based Composites in the Attachment Bonding Process of Clear Aligners. Int. J. Dent. 2022, 12, 1637594. [Google Scholar] [CrossRef]
- Chen, W.; Qian, L.; Qian, Y.; Zhang, Z.; Wen, X. Comparative study of three composite materials in bonding attachments for clear aligners. Orthod. Craniofacial Res. 2021, 24, 520–527. [Google Scholar] [CrossRef]
- D’Antò, V.; Muraglie, S.; Castellano, B.; Candida, E.; Sfondrini, M.F.; Scribante, A.; Grippaudo, C. Influence of Dental Composite Viscosity in Attachment Reproduction: An Experimental In Vitro Study. Materials 2019, 12, 4001. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
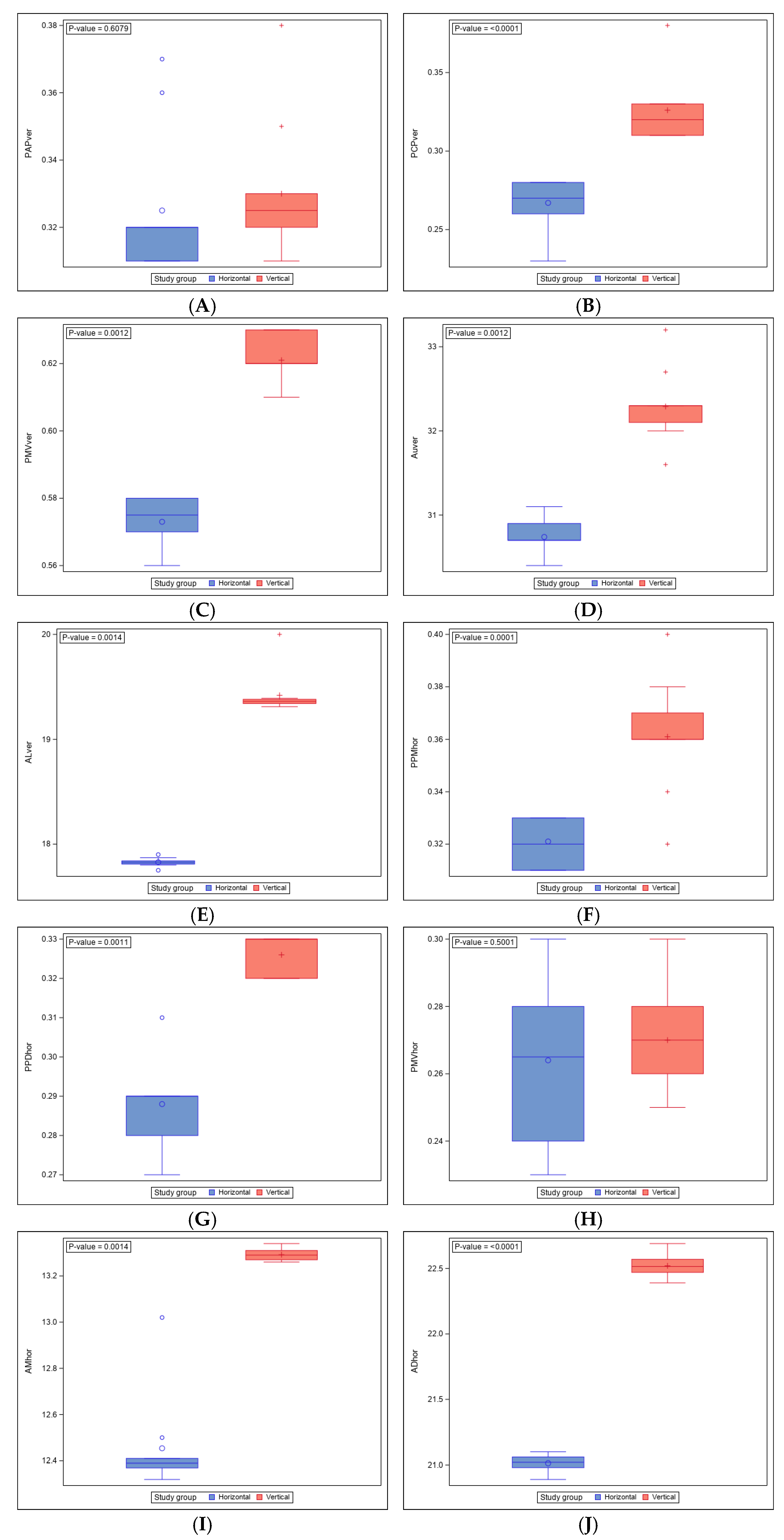
| PAPver Linear Measurement (mm) | ||||||
| Study Group | n | Mean | Median | SD | Minimum | Maximum |
| Horizontal | 70 | 0.330 | 0.325 | 0.021 | 0.310 | 0.380 |
| Vertical | 70 | 0.325 | 0.320 | 0.022 | 0.310 | 0.370 |
| PCPver linear measurement (mm) | ||||||
| Horizontal | 70 | 0.326 | 0.320 | 0.021 | 0.310 | 0.380 |
| Vertical | 70 | 0.267 | 0.270 | 0.016 | 0.230 | 0.280 |
| PMVver linear measurement (mm) | ||||||
| Horizontal | 70 | 0.621 | 0.620 | 0.007 | 0.610 | 0.630 |
| Vertical | 70 | 0.573 | 0.575 | 0.008 | 0.560 | 0.580 |
| AUver angle measurement (°) | ||||||
| Horizontal | 70 | 32.290 | 32.300 | 0.425 | 31.600 | 33.200 |
| Vertical | 70 | 30.740 | 30.700 | 0.190 | 30.400 | 31.100 |
| ALver angle measurement (°) | ||||||
| Horizontal | 70 | 19.418 | 19.360 | 0.206 | 19.310 | 20.000 |
| Vertical | 70 | 17.827 | 17.825 | 0.040 | 17.750 | 17.900 |
| PPMhor linear measurement (mm) | ||||||
| Horizontal | 70 | 0.361 | 0.360 | 0.021 | 0.320 | 0.400 |
| Vertical | 70 | 0.321 | 0.320 | 0.009 | 0.310 | 0.330 |
| PPDhor linear measurement (mm) | ||||||
| Horizontal | 70 | 0.326 | 0.330 | 0.005 | 0.320 | 0.330 |
| Vertical | 70 | 0.288 | 0.290 | 0.010 | 0.270 | 0.310 |
| PMVhor linear measurement (mm) | ||||||
| Horizontal | 70 | 0.270 | 0.270 | 0.016 | 0.250 | 0.300 |
| Vertical | 70 | 0.264 | 0.265 | 0.023 | 0.230 | 0.300 |
| AMhor angle measurement (°) | ||||||
| Horizontal | 70 | 13.292 | 13.290 | 0.025 | 13.260 | 13.340 |
| Vertical | 70 | 12.454 | 12.390 | 0.204 | 12.320 | 13.020 |
| ADhor angle measurement (°) | ||||||
| Horizontal | 70 | 22.520 | 22.515 | 0.084 | 22.390 | 22.690 |
| Vertical | 70 | 21.013 | 21.020 | 0.062 | 20.890 | 21.100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raluca Fratila, C.; Alonso-Ezpeleta, L.Ó.; Poveda-Saenz, M.; Giovannini, G.; Lobo-Galindo, A.B.; Flores-Fraile, J.; Zubizarreta-Macho, Á. Accuracy Evaluation of Indirect Bonding Techniques for Clear Aligner Attachments Using 3D-Printed Models: An In Silico and Physical Model-Based Study. Materials 2025, 18, 780. https://doi.org/10.3390/ma18040780
Raluca Fratila C, Alonso-Ezpeleta LÓ, Poveda-Saenz M, Giovannini G, Lobo-Galindo AB, Flores-Fraile J, Zubizarreta-Macho Á. Accuracy Evaluation of Indirect Bonding Techniques for Clear Aligner Attachments Using 3D-Printed Models: An In Silico and Physical Model-Based Study. Materials. 2025; 18(4):780. https://doi.org/10.3390/ma18040780
Chicago/Turabian StyleRaluca Fratila, Cosmina, Luis Óscar Alonso-Ezpeleta, Manuel Poveda-Saenz, Giovanni Giovannini, Ana Belén Lobo-Galindo, Javier Flores-Fraile, and Álvaro Zubizarreta-Macho. 2025. "Accuracy Evaluation of Indirect Bonding Techniques for Clear Aligner Attachments Using 3D-Printed Models: An In Silico and Physical Model-Based Study" Materials 18, no. 4: 780. https://doi.org/10.3390/ma18040780
APA StyleRaluca Fratila, C., Alonso-Ezpeleta, L. Ó., Poveda-Saenz, M., Giovannini, G., Lobo-Galindo, A. B., Flores-Fraile, J., & Zubizarreta-Macho, Á. (2025). Accuracy Evaluation of Indirect Bonding Techniques for Clear Aligner Attachments Using 3D-Printed Models: An In Silico and Physical Model-Based Study. Materials, 18(4), 780. https://doi.org/10.3390/ma18040780