
Thermal Treatment Prevents Effects of Downward Loads on the Screw-In Force Generation and Canal-Centering Ability of Nickel–Titanium Rotary Instruments

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Estimation
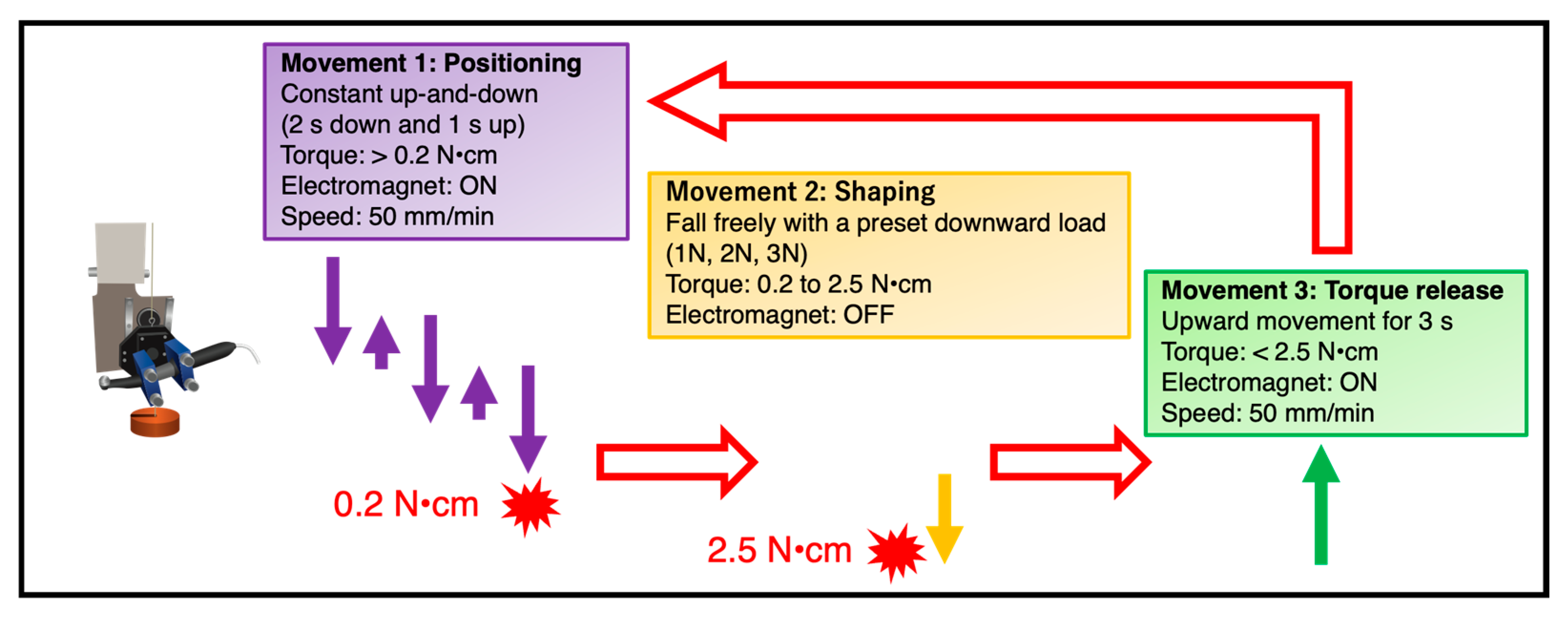
2.2. Automated Root Canal Instrumentation Device
2.3. Root Canal Instrumentation
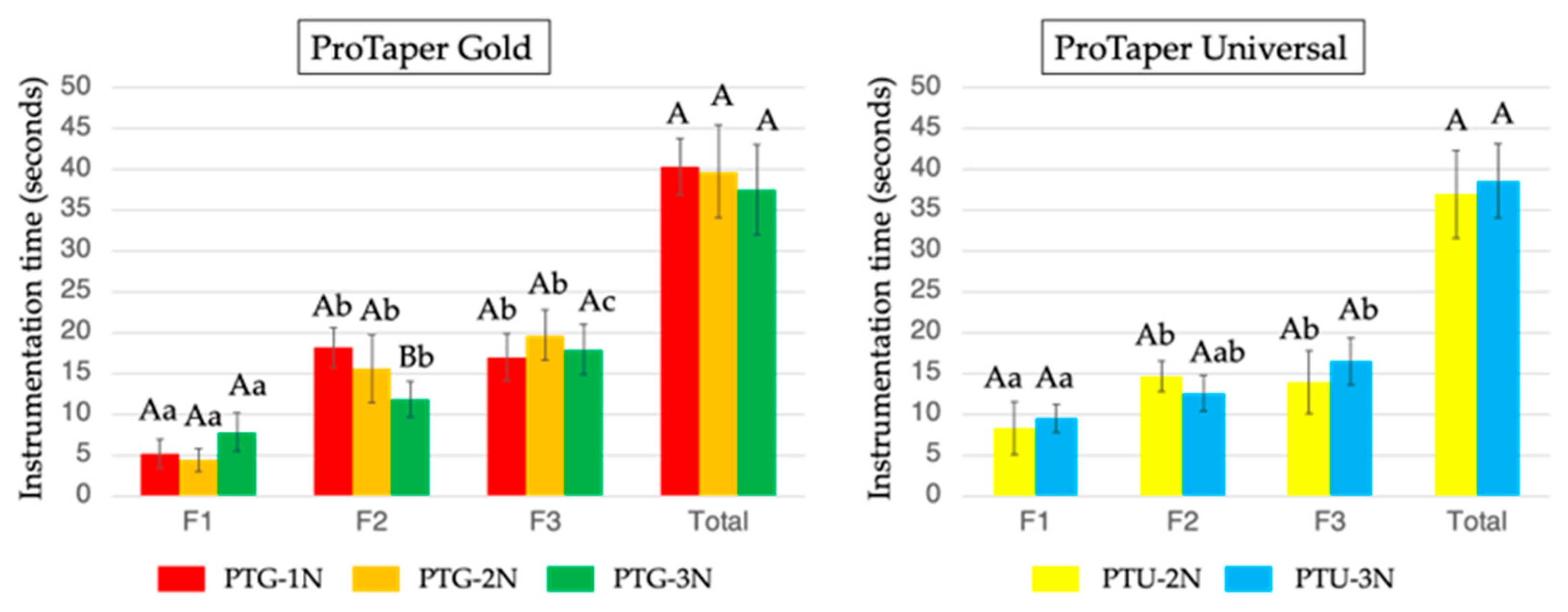
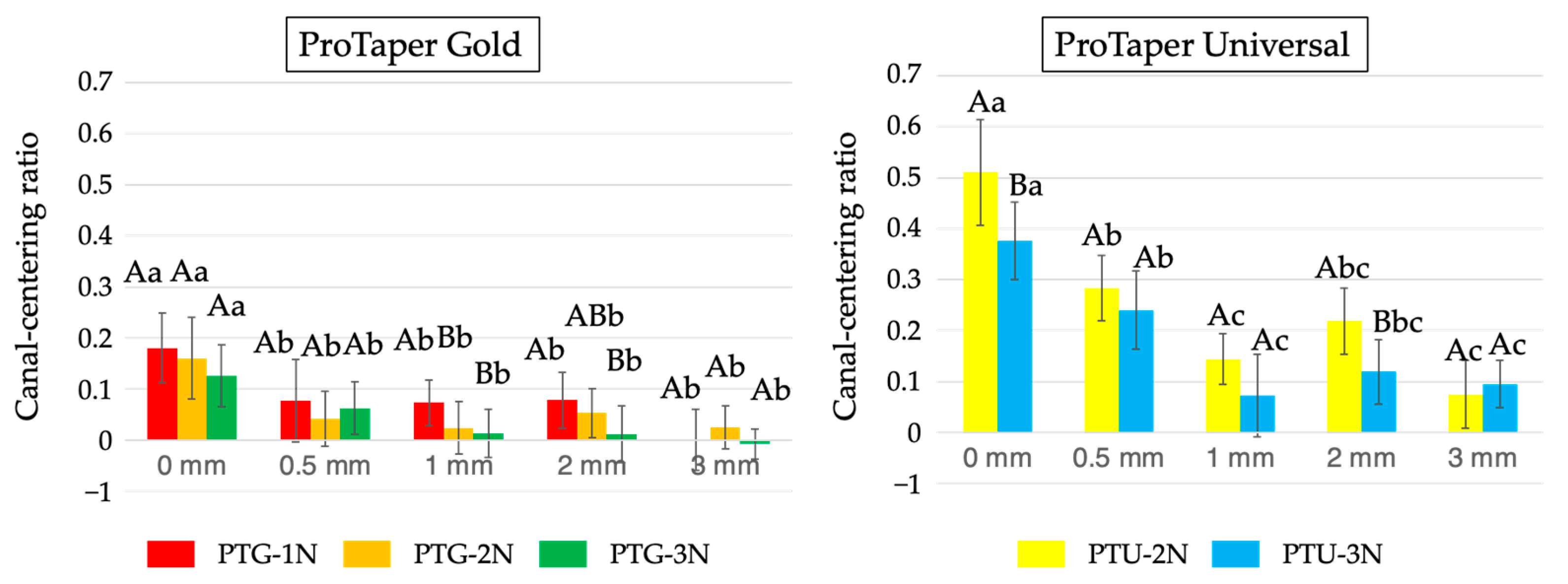
2.4. Assessment of the Instrumentation Time and Canal-Centering Ratio
2.5. Statistical Analysis
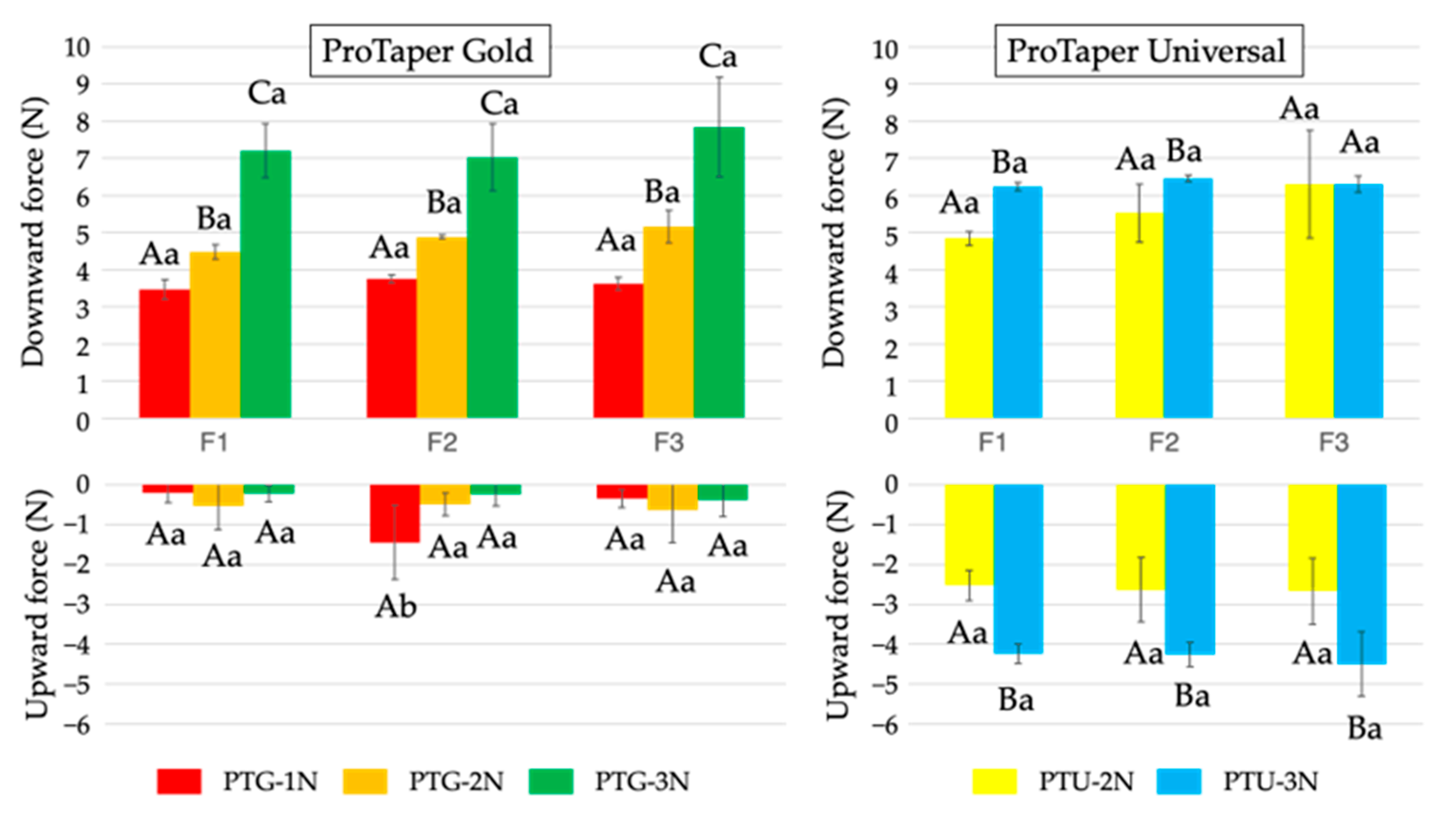
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siqueira, J.F., Jr.; Silva, W.O.; Romeiro, K.; Gominho, L.F.; Alves, F.R.F.; Rôças, I.N. Apical root canal microbiome associated with primary and posttreatment apical periodontitis: A systematic review. Int. Endod. J. 2024, 57, 1043–1058. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F., Jr.; Bate, A.L.; Pitt Ford, T.R. Histologic investigation of root canal-treated teeth with apical periodontitis: A retrospective study from twenty-four patients. J. Endod. 2009, 35, 493–502. [Google Scholar] [CrossRef]
- Schilder, H. Cleaning and shaping the root canal. Dent. Clin. N. Am. 1974, 18, 269–296. [Google Scholar] [CrossRef]
- Sjögren, U.; Hagglund, B.; Sundqvist, G.; Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 1990, 16, 498–504. [Google Scholar] [CrossRef]
- Shen, Y.; Zhou, H.M.; Zheng, Y.F.; Peng, B.; Haapasalo, M. Current challenges and concepts of the thermomechanical treatment of nickel-titanium instruments. J. Endod. 2013, 39, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Zupanc, J.; Vahdat-Pajouh, N.; Schäfer, E. New thermomechanically treated NiTi alloys—A review. Int. Endod. J. 2018, 51, 1088–1103. [Google Scholar] [CrossRef]
- Gambill, J.M.; Alder, M.; del Rio, C.E. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J. Endod. 1996, 22, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Peters, O.A. Current challenges and concepts in the preparation of root canal systems: A review. J. Endod. 2004, 30, 559–567. [Google Scholar] [CrossRef]
- Glossen, C.R.; Haller, R.H.; Dove, S.B.; del Rio, C.E. A comparison of root canal preparations using Ni-Ti hand, Ni-Ti engine-driven, and K-Flex endodontic instruments. J. Endod. 1995, 21, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Parashos, P.; Messer, H.H. Rotary NiTi instrument fracture and its consequences. J. Endod. 2006, 32, 1031–1043. [Google Scholar] [CrossRef]
- McGuigan, M.B.; Louca, C.; Duncan, H.F. Endodontic instrument fracture: Causes and prevention. Br. Dent. J. 2013, 214, 341–348. [Google Scholar] [CrossRef]
- Maki, K.; Ebihara, A.; Kimura, S.; Nishijo, M.; Tokita, D.; Okiji, T. Effect of different speeds of up-and-down motion on canal centering ability and vertical force and torque generation of nickel-titanium rotary instruments. J. Endod. 2019, 45, 68–72. [Google Scholar] [CrossRef]
- Maki, K.; Ebihara, A.; Unno, H.; Omori, S.; Nakatsukasa, T.; Kimura, S.; Okiji, T. Effect of different downward loads on canal centering ability, vertical force, and torque generation during nickel-titanium rotary instrumentation. Materials 2022, 15, 2724. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.H.; Kwak, S.W.; Sigurdsson, A.; Chang, S.W.; Kim, S.K.; Kim, H.C. Stress generation during pecking motion of rotary nickel-titanium instruments with different pecking depth. J. Endod. 2017, 43, 1688–1691. [Google Scholar] [CrossRef] [PubMed]
- Hirano, K.; Kimura, S.; Maki, K.; Omori, S.; Ebihara, A.; Okiji, T. Impact of varying amplitudes of upward and downward motion on the torque/force generation, canal-centering ability, and cyclic fatigue resistance of nickel–titanium reciprocating instrument. Appl. Sci. 2025, 15, 288. [Google Scholar] [CrossRef]
- Pedullà, E.; Carlesi, T.; Pappalardo, A.; Canova, F.S.; Malagnino, V.A.; La Sora, G.R.M.; Generali, L. Impact of pecking amplitude on cyclic fatigue of new nickel-titanium files. Clin. Exp. Dent. Res. 2024, 10, e811. [Google Scholar] [CrossRef]
- La Rosa, G.R.M.; Canova, F.S.; Generali, L.; Pedullà, E. The role of pecking motion depths in dynamic cyclic fatigue resistance: In vitro study. Int. Dent. J. 2024, 74, 855–861. [Google Scholar] [CrossRef]
- Chicon, J.B.; Fernandes Pavão, V.M.; Gonçalves Cunha, M.H.; Frozoni, M. Influence of the brushing motions on the dynamic cyclic fatigue resistance of the reciproc blue instrument: In vitro study. J. Endod. 2024, 50, 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Romeiro, K.; Brasil, S.C.; Souza, T.M.; Gominho, L.F.; Pérez, A.R.; Perez, R.; Alves, F.R.F.; Rôças, I.N.; Siqueira, J.F., Jr. Influence of brushing motions on the shaping of oval canals by rotary and reciprocating instruments. Clin. Oral Investig. 2023, 27, 3973–3981. [Google Scholar] [CrossRef]
- Yanık, D.; Özel, Ş.; Dağlı Taşman Cömert, F. Brushing motion caused no microcracks: A micro-computed tomography study. Clin. Oral Investig. 2025, 29, 173. [Google Scholar] [CrossRef]
- Ha, J.H.; Cheung, G.S.; Versluis, A.; Lee, C.J.; Kwak, S.W.; Kim, H.C. ‘Screw-in’ tendency of rotary nickel-titanium files due to design geometry. Int. Endod. J. 2015, 48, 666–672. [Google Scholar] [CrossRef]
- Ha, J.H.; Kwak, S.W.; Kim, S.K.; Kim, H.C. Screw-in forces during instrumentation by various file systems. Restor. Dent. Endod. 2016, 41, 304–309. [Google Scholar] [CrossRef]
- Maki, K.; Ebihara, A.; Kimura, S.; Nishijo, M.; Tokita, D.; Miyara, K.; Okiji, T. Enhanced root canal-centering ability and reduced screw-in force generation of reciprocating nickel-titanium instruments with a post-machining thermal treatment. Dent. Mater. J. 2020, 39, 251–255. [Google Scholar] [CrossRef]
- Plotino, G.; Ahmed, H.M.; Grande, N.M.; Cohen, S.; Bukiet, F. Current assessment of reciprocation in endodontic preparation: A comprehensive review–part II: Properties and effectiveness. J. Endod. 2015, 41, 1939–1950. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.Y.; Kim, H.C.; Kim, E. Kinematic effects of nickel-titanium instruments with reciprocating or continuous rotation motion: A systematic review of in vitro studies. J. Endod. 2016, 42, 1009–1017. [Google Scholar] [CrossRef]
- Omori, S.; Ebihara, A.; Hirano, K.; Kasuga, Y.; Unno, H.; Nakatsukasa, T.; Kimura, S.; Maki, K.; Hanawa, T.; Okiji, T. Effect of rotational modes on torque/force generation and canal centering ability during rotary root canal instrumentation with differently heat-treated nickel-titanium instruments. Materials 2022, 15, 6850. [Google Scholar] [CrossRef] [PubMed]
- Yahata, Y.; Yoneyama, T.; Hayashi, Y.; Ebihara, A.; Doi, H.; Hanawa, T.; Suda, H. Effect of heat treatment on transformation temperatures and bending properties of nickel-titanium endodontic instruments. Int. Endod. J. 2009, 42, 621–626. [Google Scholar] [CrossRef]
- Hieawy, A.; Haapasalo, M.; Zhou, H.; Wang, Z.J.; Shen, Y. Phase transformation behavior and resistance to bending and cyclic fatigue of ProTaper Gold and ProTaper Universal instruments. J. Endod. 2015, 41, 1134–1138. [Google Scholar] [CrossRef] [PubMed]
- Kaval, M.E.; Capar, I.D.; Ertas, H. Evaluation of the cyclic fatigue and torsional resistance of novel nickel-titanium rotary files with various alloy properties. J. Endod. 2016, 42, 1840–1843. [Google Scholar] [CrossRef]
- Pessoa, O.F.; da Silva, J.M.; Gavini, G. Cyclic fatigue resistance of rotary NiTi instruments after simulated clinical use in curved root canals. Braz. Dent. J. 2013, 24, 117–120. [Google Scholar] [CrossRef]
- Uygun, A.D.; Kol, E.; Topcu, M.K.; Seckin, F.; Ersoy, I.; Tanriver, M. Variations in cyclic fatigue resistance among ProTaper Gold, ProTaper Next and ProTaper Universal instruments at different levels. Int. Endod. J. 2016, 49, 494–499. [Google Scholar] [CrossRef]
- Elnaghy, A.M.; Elsaka, S.E. Mechanical properties of ProTaper Gold nickel-titanium rotary instruments. Int. Endod. J. 2016, 49, 1073–1078. [Google Scholar] [CrossRef]
- Gagliardi, J.; Versiani, M.A.; de Sousa-Neto, M.D.; Plazas-Garzon, A.; Basrani, B. Evaluation of the shaping characteristics of ProTaper Gold, ProTaper NEXT, and ProTaper Universal in curved canals. J. Endod. 2015, 41, 1718–1724. [Google Scholar] [CrossRef]
- Vasconcelos, R.A.; Arias, A.; Peters, O.A. Lateral and axial cutting efficiency of instruments manufactured with conventional nickel-titanium and novel gold metallurgy. Int. Endod. J. 2018, 51, 577–583. [Google Scholar] [CrossRef]
- Ha, J.H.; Kwak, S.W.; Versluis, A.; Lee, C.J.; Park, S.H.; Kim, H.C. The geometric effect of an off-centered cross-section on nickel-titanium rotary instruments: A finite element analysis study. J. Dent. Sci. 2017, 12, 173–178. [Google Scholar] [CrossRef] [PubMed]
- de Cristofaro Almeida, G.; Aun, D.P.; Resende, P.D.; Peixoto, I.F.; Viana, A.C.; Buono, V.T.; de Azevedo Bahia, M.G. Comparative analysis of torque and apical force to assess the cutting behaviour of ProTaper Next and ProTaper Universal endodontic instruments. Aust. Endod. J. 2020, 46, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.C.; Cheung, G.S.; Lee, C.J.; Kim, B.M.; Park, J.K.; Kang, S.I. Comparison of forces generated during root canal shaping and residual stresses of three nickel-titanium rotary files by using a three-dimensional finite-element analysis. J. Endod. 2008, 34, 743–747. [Google Scholar] [CrossRef]
- Elnaghy, A.M.; Elsaka, S.E. Laboratory comparison of the mechanical properties of TRUShape with several nickel-titanium rotary instruments. Int. Endod. J. 2017, 50, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, M.S.; Ebihara, A.; Kasuga, Y.; Maki, K.; Kimura, S.; Htun, P.H.; Nakatsukasa, T.; Okiji, T. Influence of rotational speed on torque/force generation and shaping ability during root canal instrumentation of extracted teeth with continuous rotation and optimum torque reverse motion. Int. Endod. J. 2021, 54, 1614–1622. [Google Scholar] [CrossRef]
- Lim, K.C.; Webber, J. The validity of simulated root canals for the investigation of the prepared root canal shape. Int. Endod. J. 1985, 18, 240–246. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maki, K.; Ebihara, A.; Luo, Y.; Kasuga, Y.; Unno, H.; Omori, S.; Kimura, S.; Okiji, T. Thermal Treatment Prevents Effects of Downward Loads on the Screw-In Force Generation and Canal-Centering Ability of Nickel–Titanium Rotary Instruments. Materials 2025, 18, 3610. https://doi.org/10.3390/ma18153610
Maki K, Ebihara A, Luo Y, Kasuga Y, Unno H, Omori S, Kimura S, Okiji T. Thermal Treatment Prevents Effects of Downward Loads on the Screw-In Force Generation and Canal-Centering Ability of Nickel–Titanium Rotary Instruments. Materials. 2025; 18(15):3610. https://doi.org/10.3390/ma18153610
Chicago/Turabian StyleMaki, Keiichiro, Arata Ebihara, Yanshan Luo, Yuka Kasuga, Hayate Unno, Satoshi Omori, Shunsuke Kimura, and Takashi Okiji. 2025. "Thermal Treatment Prevents Effects of Downward Loads on the Screw-In Force Generation and Canal-Centering Ability of Nickel–Titanium Rotary Instruments" Materials 18, no. 15: 3610. https://doi.org/10.3390/ma18153610
APA StyleMaki, K., Ebihara, A., Luo, Y., Kasuga, Y., Unno, H., Omori, S., Kimura, S., & Okiji, T. (2025). Thermal Treatment Prevents Effects of Downward Loads on the Screw-In Force Generation and Canal-Centering Ability of Nickel–Titanium Rotary Instruments. Materials, 18(15), 3610. https://doi.org/10.3390/ma18153610