

Innovative Strategies in Hernia Mesh Design: Materials, Mechanics, and Modeling

 ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Complications
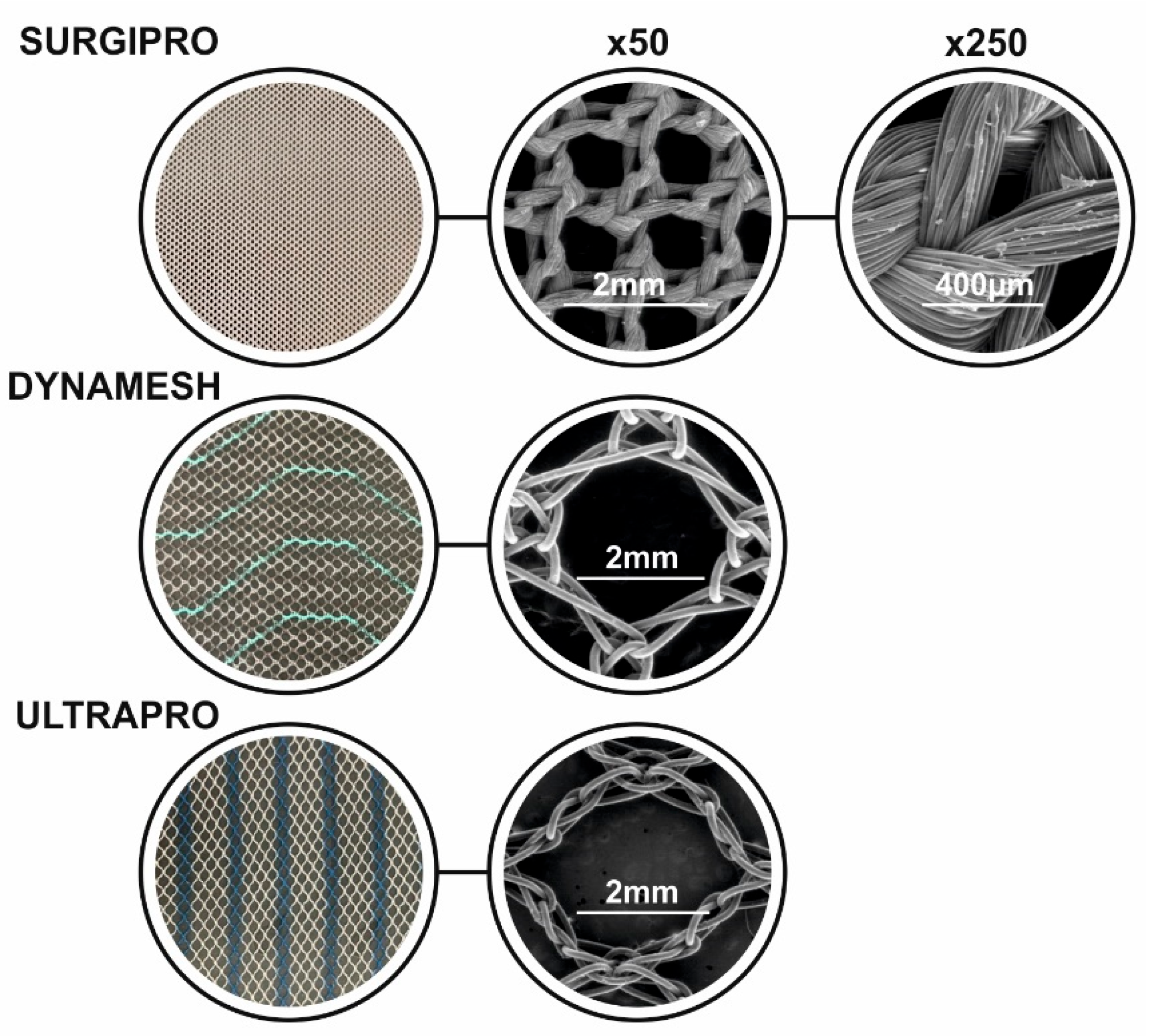
3. Commercial Synthetic Hernia Mesh Implants: Mesh Geometries

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Synthetic Mesh Implants | ||||||
|---|---|---|---|---|---|---|
| Mesh Name | Material | Filament Type | Pore Size | Weight (g/m2) | Manufacturer | References |
| Marlex | PP | monofilament | 0.6 mm | 95 | Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA | [13,16] |
| Prolene | PP | dual-filament | 1.0–2 mm | 105 | Ethicon, Johnson & Johnson, Somerville, NJ, USA | [13,16] |
| Trelex | PP | monofilament | 0.6 mm | 95 | Meadox Medicals, Boston Scientific, Marlborough, MA, USA | [13,16] |
| Surgipro | PP | multifilament | 0.9 mm | 87 | USSC, Norwalk, CT, USA | [13,17] |
| Lars | POL | multifilament | N/A | N/A | Corin Group, Gloucestershire, UK | [13] |
| Fluoropassiv | POL | multifilament | N/A | N/A | PFM Medical, Cologne, Germany | [13] |
| Bard Teflon | PTFE | multifilament | N/A | N/A | Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA | [13] |
| Goretex | ePTFE | N/A | 0–25 μm | 200–400 | Gore Medical, Flagstaff, AZ, USA | [16] |
| Optilene | PP | monofilament | 1 mm | 36 | B-Braun, Melsungen, Germany | [17] |
| Bard Mesh | PP | monofilament | 0.0007–0.6500 mm2 | 97 | Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA | [16] |
| Parietene LW | PP | monofilament | 1.8 × 1.5 mm | 38 | Medtronic, Minneapolis, MN, USA | [16] |
| Prolite | PP | monofilament | 0.8 mm | 85 | Atrium Medical Corporation, Hudson, NH, USA | [16,18] |
| Infinit Mesh | PTFE | monofilament | 4.05 ± 0.22 mm2 | 70 | N/A | [16] |
| Mersilene | POL | multifilament | 0.6–1 mm | 40 | Ethicon, Johnson & Johnson, Somerville, NJ, USA | [16] |
| Composite Mesh Implants | ||||||
| Vypro II | PP/Polyglactin 910 | multifilament | 3.0 mm | 50 | Ethicon, Johnson & Johnson, Somerville, NJ, USA | [17] |
| Dual Mesh | ePTFE | N/A | N/A | N/A | Gore Medical, Flagstaff, AZ, USA | [13] |
| Parietex | POL-Collagen | monofilament | 2.4 mm | 78 | Covidien, Mansfield, MA, USA | [17] |
| Composix | PP-ePTFE | monofilament | N/A | N/A | Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA | [13] |
| Proceed | PP-Celluose | monofilament | N/A | N/A | Ethicon, Johnson & Johnson, Somerville, NJ, USA | [13] |
| Dynamesh | PP-PVDF | N/A | N/A | N/A | FEG, Aachen, Germany | [13] |
| Sepramesh | PP-Sodium | monofilament | N/A | N/A | Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA | [13] |
| Ultrapro | PP-Polyglecaprone | monofilament | 3.5 mm | 54 | Ethicon, Johnson & Johnson, Somerville, NJ, USA | [17] |
| Ti-mesh | PP-Titanium | monofilament | N/A | N/A | PFM Medical, Cologne, Germany | [13] |
| C-Qur | PP-Ω3 | N/A | N/A | N/A | Atrium Medical Corporation, Hudson, NH, USA | [13] |
4. Mechanical Characterization and Finite Element Analysis
4.1. Mechanical Characterization of Soft Tissues in Hernia Repair
4.2. Hernia-Soft Tissue Simulation
4.3. Synthetic Mesh
4.4. Constitutive Laws
5. New Approaches for Hernia Mesh Implants
5.1. Methods
5.1.1. Three-Dimensional Printing
5.1.2. Electrospinning
5.1.3. Melt Electrowriting (MEW)
5.2. Types of Mesh Implants
5.2.1. Biologically Based Materials
5.2.2. Smart Materials
5.2.3. Drug-Eluting Meshes
5.3. Hernia Regeneration Attempts
6. Future Perspectives and Market Analysis
6.1. Future Perspectives
6.2. Market Analysis
6.3. Patent Analysis
7. Discussion
8. Conclusions
- Rigorous in vivo and long-term clinical studies evaluating safety and efficacy;
- Greater integration of FEM and 3D design tools into early-stage development and surgical planning;
- Comparative effectiveness studies that benchmark new solutions against current standards of care;
- Development of regulatory frameworks and surgical guidelines that support innovation while ensuring patient safety;
- Continuous interdisciplinary collaboration between engineers, materials scientists, clinicians, and regulatory bodies.
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saha, T.; Wang, X.; Padhye, R.; Houshyar, S. A review of recent developments of polypropylene surgical mesh for hernia repair. OpenNano 2022, 7, 100046. [Google Scholar] [CrossRef]
- Elango, S.; Perumalsamy, S.; Ramachandran, K.; Vadodaria, K. Mesh materials and hernia repair. Biomed. Pharmacother. 2017, 7, 16. [Google Scholar] [CrossRef]
- Özant, A.; Arslan, K. Synthetic Meshes in Hernia Surgery. Cyprus J. Med. Sci. 2023, 8, 1–7. [Google Scholar] [CrossRef]
- Read, R.C. Milestones in the history of hernia surgery: Prosthetic repair. Hernia 2004, 8, 8–14. [Google Scholar] [CrossRef]
- Read, R.C. Hstory. In Francis C. Usher, Herniologist of the Twentieth Century; Springer Nature: Berlin/Heidelberg, Germany, 1999. [Google Scholar]
- Food, U.S.; Administration, D. Surgical Mesh for Hernia Repair: FDA Activities. Available online: https://www.fda.gov/medical-devices/surgical-mesh-used-hernia-repair/surgical-mesh-hernia-repair-fda-activities (accessed on 15 January 2024).
- Robinson, T.N.; Clarke, J.H.; Schoen, J.; Walsh, M.D. Major mesh-related complications following hernia repair: Events reported to the Food and Drug Administration. Surg. Endosc. Other Interv. Tech. 2005, 19, 1556–1560. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kasiakou, S.K. Mesh-related infections after hernia repair surgery. Clin. Microbiol. Infect. 2005, 11, 3–8. [Google Scholar] [CrossRef]
- Mavros, M.N.; Athanasiou, S.; Alexiou, V.G.; Mitsikostas, P.K.; Peppas, G.; Falagas, M.E. Risk factors for mesh-related infections after hernia repair surgery: A meta-analysis of cohort studies. World J. Surg. 2011, 35, 2389–2398. [Google Scholar] [CrossRef]
- Wang, G.; Liu, Z. Comment to: Is surgeon annual case volume related with intra and postoperative complications after ventral hernia repair? Hernia 2025, 29, 6. [Google Scholar] [CrossRef]
- Detry, O. Comment to: Initial and recurrent management of parastomal hernia after cystectomy and ileal conduit urinary diversion. Hernia 2025, 29, 87. [Google Scholar] [CrossRef]
- Lovén, H.; Erichsen, R.; Tøttrup, A.; Bisgaard, T. Mesh-related complications and recurrence after incisional hernia repair in patients with fistulizing versus non-fistulizing Crohn’s disease. Hernia 2025, 29, 36. [Google Scholar] [CrossRef]
- Bilsel, Y.; Abci, I. The search for ideal hernia repair; mesh materials and types. Int. J. Surg. 2012, 10, 317–321. [Google Scholar] [CrossRef]
- Panaro, F.; Matos-Azevedo, A.M.; Fatas, J.A.; Marin, J.; Navarro, F.; Zaragoza-Fernandez, C. Endoscopic and histological evaluations of a newly designed inguinal hernia mesh implant: Experimental studies on porcine animal model and human cadaver. Ann. Med. Surg. 2015, 4, 172–178. [Google Scholar] [CrossRef]
- Deeken, C.R.; Lake, S.P. Mechanical properties of the abdominal wall and biomaterials utilized for hernia repair. Mech. Behav. Biomed. Mater. 2017, 74, 411–427. [Google Scholar] [CrossRef]
- Sanbhal, N.; Miao, L.; Xu, R.; Khatri, A.; Wang, L. Physical structure and mechanical properties of knitted hernia mesh materials: A review. J. Ind. Text. 2018, 48, 333–360. [Google Scholar] [CrossRef]
- Pashkouleva, D.; Kirilova-Doneva, M. Comparative study of the viscoelastic behaviour of hernia meshes. Russ. J. Biomech. 2024, 28, 87–94. [Google Scholar] [CrossRef]
- Saberski, E.R.; Orenstein, S.B.; Novitsky, Y.W. Anisotropic evaluation of synthetic surgical meshes. Hernia 2011, 15, 47–52. [Google Scholar] [CrossRef]
- Simón-Allué, R.; Ortillés, A.; Calvo, B. Mechanical behavior of surgical meshes for abdominal wall repair: In vivo versus biaxial characterization. J. Mech. Behav. Biomed. Mater. 2017, 82, 102–111. [Google Scholar] [CrossRef]
- Ibrahim, M.M.; Poveromo, L.P.; Glisson, R.R.; Cornejo, A.; Farjat, A.E.; Gall, K.; Levinson, H. Modifying hernia mesh design to improve device mechanical performance and promote tension-free repair. J. Biomech. 2018, 71, 43–51. [Google Scholar] [CrossRef]
- Bakker, W.J.; Aufenacker, T.J.; Boschman, J.S.; Burgmans, J.P.J. Lightweight mesh is recommended in open inguinal (Lichtenstein) hernia repair: A systematic review and meta-analysis. Surgery 2020, 167, 581–589. [Google Scholar] [CrossRef]
- Bittner, J.G.; El-Hayek, K.; Strong, A.T.; LaPinska, M.P.; Yoo, J.S.; Pauli, E.M.; Kroh, M. First human use of hybrid synthetic/biologic mesh in ventral hernia repair: A multicenter trial. Surg. Endosc. 2018, 32, 1123–1130. [Google Scholar] [CrossRef]
- Smart, N.J.; Marshall, M.; Daniels, I.R. Biological meshes: A review of their use in abdominal wall hernia repairs. Surgeon 2012, 10, 159–171. [Google Scholar] [CrossRef]
- Hernández, B.; Peña, E.; Pascual, G.; Rodríguez, M.; Calvo, B.; Doblaré, M.; Bellón, J.M. Mechanical and histological characterization of the abdominal muscle. A previous step to modelling hernia surgery. J. Mech. Behav. Biomed. Mater. 2011, 4, 392–404. [Google Scholar] [CrossRef]
- Grasa, J.; Sierra, M.; Lauzeral, N.; Muñoz, M.J.; Miana-Mena, F.J.; Calvo, B. Active behavior of abdominal wall muscles: Experimental results and numerical model formulation. J. Mech. Behav. Biomed. Mater. 2016, 61, 444–454. [Google Scholar] [CrossRef]
- Jourdan, A.; Dhume, R.; Guérin, E.; Siegel, A.; Le Ruyet, A.; Palmer, M. Numerical investigation of a finite element abdominal wall model during breathing and muscular contraction. Comput. Methods Programs Biomed. 2024, 244, 107985. [Google Scholar] [CrossRef]
- Fortuny, G.; Rodríguez-Navarro, J.; Susín, A.; López-Cano, M. Simulation and study of the behaviour of the transversalis fascia in protecting against the genesis of inguinal hernias. J. Biomech. 2009, 42, 2263–2267. [Google Scholar] [CrossRef]
- Tomaszewska, A.; Lubowiecka, I.; Szymczak, C.; Śmietański, M.; Meronk, B.; Kłosowski, P.; Bury, K. Physical and mathematical modelling of implant-fascia system in order to improve laparoscopic repair of ventral hernia. Clin. Biomech. 2013, 28, 743–751. [Google Scholar] [CrossRef]
- Vaz, F.; Silva, T.; Silva, E.; Parente, M.; Brandão, S.; Fernandes, A.A. Biodegradable mesh implants for prolapse repair: Advances in computational modelling and experimental validation. Proc. Inst. Mech. Eng. Part H 2025, 239, 294–307. [Google Scholar] [CrossRef]
- Vaz, M.F.R.R.; Silva, M.E.; Parente, M.; Brandão, S.; Fernandes, A.A. 3D printing and development of computational models of biodegradable meshes for pelvic organ prolapse. Eng. Comput. 2024, 41, 1399–1423. [Google Scholar] [CrossRef]
- Hernández-Gascón, B.; Peña, E.; Melero, H.; Pascual, G.; Doblaré, M.; Ginebra, M.P.; Bellón, J.M.; Calvo, B. Mechanical behaviour of synthetic surgical meshes: Finite element simulation of the herniated abdominal wall. Acta Biomater. 2011, 7, 3905–3913. [Google Scholar] [CrossRef]
- Todros, S.; Pachera, P.; Baldan, N.; Pavan, P.G.; Pianigiani, S.; Merigliano, S.; Natali, A.N. Computational modeling of abdominal hernia laparoscopic repair with a surgical mesh. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 73–81. [Google Scholar] [CrossRef]
- Karami, M.; Zohoor, H.; Calvo, B.; Grasa, J. A 3D multi-scale skeletal muscle model to predict active and passive responses. Application to intra-abdominal pressure prediction. Comput. Methods Appl. Mech. Eng. 2023, 415, 116222. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, S.; Deng, Y.; Zhang, Y.; Yin, L.; Zheng, W. An improved method for soft tissue modeling. Biomed Signal Process Control. 2021, 65, 102367. [Google Scholar] [CrossRef]
- Chanda, A.; Ruchti, T.; Upchurch, W. Biomechanical modeling of prosthetic mesh and human tissue surrogate interaction. Biomimetics 2018, 3, 27. [Google Scholar] [CrossRef]
- Tomaszewska, A.; Reznikov, D.; Szymczak, C.; Lubowiecka, I. Constitutive Modelling of Knitted Abdominal Implants in Numerical Simulations of Repaired Hernia Mechanics. In Lecture Notes in Computational Vision and Biomechanics; Springer: Berlin/Heidelberg, Germany, 2020; Volume 36, pp. 550–559. [Google Scholar] [CrossRef]
- Tomaszewska, A.; Reznikov, D. Combined numerical and experimental approach to determine numerical model of abdominal scaffold. Comput. Methods Biomech. Biomed. Eng. 2022, 25, 1235–1248. [Google Scholar] [CrossRef]
- He, W.; Liu, X.; Wu, S.; Liao, J.; Cao, G.; Fan, Y.; Li, X. A numerical method for guiding the design of surgical meshes with suitable mechanical properties for specific abdominal hernias. Comput. Biol. Med. 2020, 116, 103531. [Google Scholar] [CrossRef]
- Siddiqui, A.; Lyons, N.B.; Anwoju, O.; Cohen, B.L.; Ramsey, W.A.; O’Neil, C.F.; Ali, Z.; Liang, M.K. Mesh Type With Ventral Hernia Repair: A Systematic Review and Meta-Analysis of Randomized Trials. J. Surg. Res. 2023, 291, 603–610. [Google Scholar] [CrossRef]
- Liu, T.; Ye, Z.; Yu, B.; Xuan, W.; Kang, J.; Chen, J. Biomechanical behaviors and visco-hyperelastic mechanical properties of human hernia patches with polypropylene mesh. Mech. Mater. 2023, 176, 104529. [Google Scholar] [CrossRef]
- Mosier, S.; Berbel, G.; Friis, E.A. Computational analysis of electrical stimulation to promote tissue healing for hernia repair at varying mesh placement planes. J. Biomater. Appl. 2024, 39, 58–65. [Google Scholar] [CrossRef]
- Humphrey, J.D.; Yin, F.C. A new constitutive formulation for characterizing the mechanical behavior of soft tissues. Biophys. J. 1987, 52, 563–570. [Google Scholar] [CrossRef]
- Pioletti, D.P.; Rakotomanana, L.R. Non-linear viscoelastic laws for soft biological tissues. Eur. J. Mech. A/Solids 2000, 19, 749–759. [Google Scholar] [CrossRef]
- Tuset, L.; Fortuny, G.; Herrero, J.; Puigjaner, D.; López, J.M. Implementation of a new constitutive model for abdominal muscles. Comput. Methods Programs Biomed. 2019, 179, 104988. [Google Scholar] [CrossRef]
- Tomaszewska, A.; Reznikov, D. Optimization of constitutive law for objective numerical modeling of knitted fabric. J. Mech. Phys. Solids 2025, 196, 106017. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Singh, R.P.; Suman, R. 3D printing applications for healthcare research and development. Glob. Health J. 2022, 6, 217–226. [Google Scholar] [CrossRef]
- Hurst, E.J. 3D Printing in Healthcare: Emerging Applications. J. Hosp. Libr. 2016, 16, 255–267. [Google Scholar] [CrossRef]
- George, M.; Aroom, K.R.; Hawes, H.G.; Gill, B.S.; Love, J. 3D Printed Surgical Instruments: The Design and Fabrication Process. World J. Surg. 2017, 41, 314–319. [Google Scholar] [CrossRef]
- Yang, Z.; Song, Z.; Nie, X.; Guo, K.; Gu, Y. A smart scaffold composed of three-dimensional printing and electrospinning techniques and its application in rat abdominal wall defects. Stem Cell Res. Ther. 2020, 11, 533. [Google Scholar] [CrossRef]
- Pérez-Köhler, B.; Benito-Martínez, S.; Gómez-Gil, V.; Rodríguez, M.; Pascual, G.; Bellón, J.M. New Insights into the Application of 3D-Printing Technology in Hernia Repair. Materials 2021, 14, 7092. [Google Scholar] [CrossRef]
- Erwin, E.; Etriwati, E.; Akhyar, A. Clinical observation, imaging, and histopathology of 3D polypropylene mesh for abdominal hernia in rabbits. Indian J. Anim. Sci. 2023, 93, 777–782. [Google Scholar] [CrossRef]
- Russo Serafini, M.; Mowat, A.; Mustafa, S.; Saifzadeh, S.; Shabab, T.; Bas, O.; O’Rourke, N.; W. Hutmacher, D.; Medeiros Savi, F. 3D-Printed Medical-Grade Polycaprolactone (mPCL) Scaffold for the Surgical Treatment of Vaginal Prolapse and Abdominal Hernias. Bioengineering 2023, 10, 1242. [Google Scholar] [CrossRef]
- da Cunha, M.N.B.; Rynkevic, R.; da Silva, M.E.T.; Da Silva Brandaõ, A.F.M.; Alves, J.L.; Fernandes, A.A. Melt Electrospinning Writing of Mesh Implants for Pelvic Organ Prolapse Repair. 3D Print. Addit. Manuf. 2022, 9, 389–398. [Google Scholar] [CrossRef]
- Hu, Q.; Zhang, Y.; Song, Y.; Shi, H.; Yang, D.; Zhang, H.; Gu, Y. 3D printing/electrospinning of bilayer composite patch with antibacterial and antiadhesive properties for the repair of abdominal wall defects. J. Mater. Chem. B 2024, 12, 10054–10067. [Google Scholar] [CrossRef]
- Agarwal, S.; Wendorff, J.H.; Greiner, A. Use of electrospinning technique for biomedical applications. Polymer 2008, 49, 5603–5621. [Google Scholar] [CrossRef]
- Serrano-Aroca, Á.; Pous-Serrano, S. Prosthetic meshes for hernia repair: State of art, classification, biomaterials, antimicrobial approaches, and fabrication methods. J. Biomed. Mater. Res. Part A 2021, 109, 2695–2719. [Google Scholar] [CrossRef]
- Kaya, M.; Ahi, Z.B.; Ergene, E.; Huri, P.Y.; Tuzlakoglu, K. Design of a new dual mesh with an absorbable nanofiber layer as a potential implant for abdominal hernia treatment. J. Tissue Eng. Regen. Med. 2020, 14, 347–354. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, L.; Ren, Y.; Chen, H.; Li, S.; Li, S.; Xu, S.; Liu, Y. Protective effectiveness of electrospinning fibrous membrane in inguinal hernia repair. Mater. Des. 2023, 231, 112074. [Google Scholar] [CrossRef]
- Kade, J.C.; Dalton, P.D. Polymers for Melt Electrowriting. Adv. Health Mater. 2021, 10, 2001232. [Google Scholar] [CrossRef]
- Hochleitner, G.; Jüngst, T.; Brown, T.D.; Hahn, K.; Moseke, C.; Jakob, F.; Dalton, P.D.; Groll, J. Additive manufacturing of scaffolds with sub-micron filaments via melt electrospinning writing. Biofabrication 2015, 7, 035002. [Google Scholar] [CrossRef]
- Xie, Y.; Fang, Q.; Zhao, H.; Li, Y.; Lin, Z.; Chen, J. Effects of Six Processing Parameters on the Size of PCL Fibers Prepared by Melt Electrospinning Writing. Micromachines 2023, 14, 1437. [Google Scholar] [CrossRef]
- Sterk, S.; Silva, M.E.T.; Fernandes, A.A.; Huß, A.; Wittek, A. Development of new surgical mesh geometries with different mechanical properties using the design freedom of 3D printing. J. Appl. Polym. Sci. 2023, 140, e54687. [Google Scholar] [CrossRef]
- Ren, J.; Murray, R.; Wong, C.S.; Qin, J.; Chen, M.; Totsika, M.; Riddell, A.D.; Warwick, A.; Rukin, N.; Woodruff, M.A. Development of 3D Printed Biodegradable Mesh with Antimicrobial Properties for Pelvic Organ Prolapse. Polymers 2022, 14, 763. [Google Scholar] [CrossRef]
- Rodríguez, M.; Gómez-Gil, V.; Pérez-Köhler, B.; Pascual, G.; Bellón, J.M. Polymer hernia repair materials: Adapting to patient needs and surgical techniques. Materials 2021, 14, 2790. [Google Scholar] [CrossRef]
- Zhang, W.; Li, Y.; Jiang, D.; Xie, S.; Zeng, M.; Chen, J.; Chen, L.; Ouyang, H.; Zou, X. Promotion of Hernia Repair with High-Strength, Flexible, and Bioresorbable Silk Fibroin Mesh in a Large Abdominal Hernia Model. ACS Biomater. Sci. Eng. 2018, 4, 2067–2080. [Google Scholar] [CrossRef]
- Luan, F.; Cao, W.; Cao, C.; Li, B.; Shi, X.; Gao, C. Construction and properties of the silk fibroin and polypropylene composite biological mesh for abdominal incisional hernia repair. Front. Bioeng. Biotechnol. 2022, 10, 949917. [Google Scholar] [CrossRef]
- Bokhari, N.; Ali, A.; Yasmeen, A.; Khan, R.; Haider, S.; Sharif, F. Fabrication of bioactive silk composite meshes for hernia repair and guided soft tissue remodeling: In silico, in vitro and in vivo models. Appl. Mater. Today 2024, 38, 102261. [Google Scholar] [CrossRef]
- Sanbhal, N.; Saitaer, X.; Peerzada, M.; Habboush, A.; Wang, F.; Wang, L. One-step surface functionalized hydrophilic polypropylene meshes for hernia repair using bio-inspired polydopamine. Fibers 2019, 7, 6. [Google Scholar] [CrossRef]
- Lanzalaco, S.; Valle, L.J.D.; Turon, P.; Weis, C.; Estrany, F.; Alemán, C.; Armelin, E. Polypropylene mesh for hernia repair with controllable cell adhesion/de-adhesion properties. J. Mater. Chem. B 2020, 8, 1049–1059. [Google Scholar] [CrossRef]
- Hu, W.; Zhang, Z.; Zhu, L.; Wen, Y.; Zhang, T.; Ren, P.; Wang, F.; Ji, Z. Combination of Polypropylene Mesh and in Situ Injectable Mussel-Inspired Hydrogel in Laparoscopic Hernia Repair for Preventing Post-Surgical Adhesions in the Piglet Model. ACS Biomater. Sci. Eng. 2020, 6, 1735–1743. [Google Scholar] [CrossRef]
- Mao, Y.; Meng, Y.; Li, S.; Li, Y.; Guidoin, R.; Qiao, Y.; Zhang, Z.; Brochu, G.; Tang, J.; Wang, L. Comparative study on nanofiber containing polypropylene-based composite mesh for abdominal wall hernia repair. Mater. Des. 2021, 212, 110227. [Google Scholar] [CrossRef]
- Liu, L.; Lin, H.; Cheng, G.; Chen, C.; Jiang, G.; Ma, P. Fabrication, characterization and in vitro accelerated degradation of polypropylene/poly (glycolide-ε-caprolactone) warp-knitted hernia repair mesh. J. Ind. Text. 2022, 51 (Suppl. S3), 4133S–4148S. [Google Scholar] [CrossRef]
- Deveci, M.Z.Y.; Enguven, G.; Ege, H.; Alakus, I.; Agturk, G.; Yontem, F.D.; Yilmaz, S.; Kirgiz, O.; Akcakavak, G.; Kazak, F.; et al. Multifunctional hernia repair biopatch: Development, characterization, in vitro and in vivo evaluation. J. Drug Deliv. Sci. Technol. 2024, 100, 106132. [Google Scholar] [CrossRef]
- Arik, B. Smart bio-textiles for medicine and healthcare applications. In Smart Textiles from Natural Resources; Elsevier: Amsterdam, The Netherlands, 2024; pp. 495–537. [Google Scholar] [CrossRef]
- Ghosh, S. Smart materials for healthcare industries. In Comprehensive Materials Processing; Elsevier: Amsterdam, The Netherlands, 2024; pp. 99–108. [Google Scholar] [CrossRef]
- Abyzova, E.; Dogadina, E.; Rodriguez, R.D.; Petrov, I.; Kolesnikova, Y.; Zhou, M.; Liu, C.; Sheremet, E. Beyond Tissue replacement: The Emerging role of smart implants in healthcare. Mater. Today Bio 2023, 22, 100784. [Google Scholar] [CrossRef]
- Pattanashetti, N.A.; Heggannavar, G.B.; Kariduraganavar, M.Y. Smart Biopolymers and their Biomedical Applications. Procedia Manuf. 2017, 12, 263–279. [Google Scholar] [CrossRef]
- Mishra, V.; Sunil, B.D.Y.; Judi, H.K.; Jain, A.K.; Anandhi, R.J.; Kaushik, A. A Review on Smart Materials in Biomedical Applications: Current Trends and Future Challenges. E3S Web Conf. 2024, 505, 01023. [Google Scholar] [CrossRef]
- Mantha, S.; Pillai, S.; Khayambashi, P.; Upadhyay, A.; Zhang, Y.; Tao, O.; Pham, H.M.; Tran, S.D. Smart hydrogels in tissue engineering and regenerative medicine. Materials 2019, 12, 3323. [Google Scholar] [CrossRef]
- Saiding, Q.; Chen, Y.; Wang, J.; Pereira, C.L.; Sarmento, B.; Cui, W.; Chen, X. Abdominal wall hernia repair: From prosthetic meshes to smart materials. Mater. Today Bio 2023, 21, 100691. [Google Scholar] [CrossRef]
- Jawarkar, S.G.; Pillai, M.; Chavan, P.; Sengupta, P. Next-generation smart biomaterials for storage and extraction of bioanalytical samples: Current standing and path forward. Microchem. J. 2024, 207, 111846. [Google Scholar] [CrossRef]
- Jaiswal, R.; Sherje, A.P. Recent advances in biopolymer-based smart hydrogel for wound healing. J. Drug Deliv. Sci. Technol. 2024, 99, 105990. [Google Scholar] [CrossRef]
- Kumi, M.; Ejeromedoghene, O.; Sudane, W.D.; Zhang, Z. Unlocking the biological response of smart Stimuli-Responsive hydrogels and their application in biological systems. Eur. Polym. J. 2024, 209, 112906. [Google Scholar] [CrossRef]
- Municoy, S.; Álvarez Echazú, M.I.; Antezana, P.E.; Galdopórpora, J.M.; Olivetti, C.; Mebert, A.M.; Foglia, M.L.; Tuttolomondo, M.V.; Alvarez, G.S.; Hardy, J.G.; et al. Stimuli-responsive materials for tissue engineering and drug delivery. Int. J. Mol. Sci. 2020, 21, 4724. [Google Scholar] [CrossRef]
- Nain, A.; Chakraborty, S.; Barman, S.B.; Gavit, P.; Indrakumar, S.; Agrawal, A.; Lin, Z.H.; Chatterjee, K. Progress in the development of piezoelectric biomaterials for tissue remodeling. Biomaterials 2024, 307, 122528. [Google Scholar] [CrossRef]
- Quiles, M.T.; Rodríguez-Contreras, A.; Guillem-Marti, J.; Punset, M.; Sánchez-Soto, M.; López-Cano, M.; Sabadell, J.; Velasco, J.; Armengol, M.; Manero, J.M.; et al. Effect of Functionalization of Texturized Polypropylene Surface by Silanization and HBII-RGD Attachment on Response of Primary Abdominal and Vaginal Fibroblasts. Polymers 2024, 16, 667. [Google Scholar] [CrossRef]
- Guillaume, O.; Lavigne, J.P.; Lefranc, O.; Nottelet, B.; Coudane, J.; Garric, X. New antibiotic-eluting mesh used for soft tissue reinforcement. Acta Biomater. 2011, 7, 3390–3397. [Google Scholar] [CrossRef]
- See, C.W.; Kim, T.; Zhu, D. Hernia Mesh and Hernia Repair: A Review. Eng. Regen. 2020, 1, 19–33. [Google Scholar] [CrossRef]
- MacIver, A.H.; McCall, M.D.; Edgar, R.L.; Thiesen, A.L.; Bigam, D.L.; Churchill, T.A.; Shapiro, A.M.J. Sirolimus drug-eluting, hydrogel-impregnated polypropylene mesh reduces intra-abdominal adhesion formation in a mouse model. Surgery 2011, 150, 907–915. [Google Scholar] [CrossRef]
- Wei, D.; Huang, Y.; Liang, M.; Ren, P.; Tao, Y.; Xu, L.; Zhang, T.; Ji, Z.; Zhang, Q. Polypropylene composite hernia mesh with anti-adhesion layer composed of PVA hydrogel and liposomes drug delivery system. Colloids Surf. B Biointerfaces 2023, 223, 113159. [Google Scholar] [CrossRef]
- Pérez-Köhler, B.; Linardi, F.; Pascual, G.; Bellón, J.M.; Eglin, D.; Guillaume, O. Efficacy of antimicrobial agents delivered to hernia meshes using an adaptable thermo-responsive hyaluronic acid-based coating. Hernia 2020, 24, 1201–1210. [Google Scholar] [CrossRef]
- Kühn, K.D.; Coraça-Huber, D.C.; Erdtmann, M.; Bernhardt, G.A.; Fölsch, C. Novel antimicrobial coating for hernia meshes. Front. Cell. Infect. Microbiol. 2024, 14, 1383680. [Google Scholar] [CrossRef]
- Shokrollahi, M.; Bahrami, S.H.; Nazarpak, M.H.; Solouk, A. Biomimetic double-sided polypropylene mesh modified by DOPA and ofloxacin loaded carboxyethyl chitosan/polyvinyl alcohol-polycaprolactone nanofibers for potential hernia repair applications. Int. J. Biol. Macromol. 2020, 165, 902–917. [Google Scholar] [CrossRef]
- Wang, Z.; Hu, K.; Jiang, Y.; Zhang, X.; Zhao, P.; Li, X.; Ding, F.; Liu, C.; Yi, S.; Ren, Z.; et al. Remodeling and Regenerative Properties of Fully Absorbable Meshes for Abdominal Wall Defect Repair: A Systematic Review and Meta-Analysis of Animal Studies. ACS Biomater. Sci. Eng. 2024, 10, 3968–3983. [Google Scholar] [CrossRef]
- Amato, G.; Agrusa, A.; Puleio, R.; Micci, G.; Cassata, G.; Cicero, L.; Di Buono, G.; Calò, P.G.; Galia, M.; Romano, G. A regenerative 3D scaffold for inguinal hernia repair. MR imaging and histological cross evidence. Qualitative study. Int. J. Surg. 2021, 96, 106170. [Google Scholar] [CrossRef]
- Liu, C.; Lin, Z.; Ruan, W.; Gai, X.; Qu, Q.; Wang, C.; Zhu, F.; Sun, Z.; Zhang, J. Safety and tissue remodeling assay of small intestinal submucosa meshes using a modified porcine surgical hernia model. Sci. Rep. 2023, 13, 23108. [Google Scholar] [CrossRef]
- Ibrahim, A.M.S.; Vargas, C.R.; Colakoglu, S.; Nguyen, J.T.; Lin, S.J.; Lee, B.T. Properties of meshes used in hernia repair: A comprehensive review of synthetic and biologic meshes. J. Reconstr. Microsurg. 2015, 31, 83–94. [Google Scholar] [CrossRef]
- Pott, P.P.; Schwarz, M.L.R.; Gundling, R.; Nowak, K.; Hohenberger, P.; Roessner, E.D. Mechanical Properties of Mesh Materials Used for Hernia Repair and Soft Tissue Augmentation. PLoS ONE 2012, 7, e46978. [Google Scholar] [CrossRef]
- Raminhos, J.M.S. Habilitações Additive Fabrication of Anepectic Meshes. Master’s Thesis, NOVA School of Science and Technology, Caparica, Portugal, November 2018. [Google Scholar]
- Sanami, M. Auxetic Materials for Biomedical Applications Mohammad Sanami. Ph.D. Thesis, The University of Bolton, Bolton, UK, September 2015. [Google Scholar]
- Warner, J.J.; Gillies, A.R.; Hwang, H.H.; Zhang, H.; Lieber, R.L.; Chen, S. 3D-printed biomaterials with regional auxetic properties. J. Mech. Behav. Biomed. Mater. 2017, 76, 145–152. [Google Scholar] [CrossRef]
- Knight, K.M.; Moalli, P.A.; Abramowitch, S.D. Preventing Mesh Pore Collapse by Designing Mesh Pores with Auxetic Geometrie A Comprehensive Evaluation Via Computational Modeling. J. Biomech. Eng. 2018, 140, 051005. [Google Scholar] [CrossRef]
- Ferreira, N.M.; Antoniadi, E.; Silva, A.T.; Silva, A.; Parente, M.; Fernandes, A.; Silva, E. Melt Electrowritten Biodegradable Mesh Implants with Auxetic Designs for Pelvic Organ Prolapse Repair. J. Manuf. Mater. Process. 2025, 9, 111. [Google Scholar] [CrossRef]
- Mardling, P.; Alderson, A.; Jordan-Mahy, N.; Le Maitre, C.L. The use of auxetic materials in tissue engineering. Biomater. Sci. 2020, 8, 2074–2083. [Google Scholar] [CrossRef]
- Kolken, H.M.A.; Garcia, A.F.; Plessis, A.D.; Rans, C.; Mirzaali, M.J.; Zadpoor, A.A. Fatigue performance of auxetic meta-biomaterials. Acta Biomater. 2021, 126, 511–523. [Google Scholar] [CrossRef]
- Jiang, D.; Thissen, H.; Hughes, T.C.; Yang, K.; Wilson, R.; Murphy, A.B.; Nguyen, V. Advances in additive manufacturing of auxetic structures for biomedical applications. Mater. Today Commun. 2024, 40, 110045. [Google Scholar] [CrossRef]
- Bhardwaj, S.; Mishra, D.K. Effect of different strut thickness on the mechanical behaviour of 3D printed auxetic structures. Mater Today Proc. 2024. [Google Scholar] [CrossRef]
- Rampado, S.; Geron, A.; Pirozzolo, G.; Ganss, A.; Pizzolato, E.; Bardini, R. Cost analysis of incisional hernia repair with synthetic mesh and biological mesh: An Italian study. Updat. Surg. 2017, 69, 375–381. [Google Scholar] [CrossRef]
- Hernia Repair Market: Growth, Size, Share, and Trends. Available online: https://www.marketsandmarkets.com/Market-Reports/hernia-mesh-devices-market-203245450.html (accessed on 26 June 2025).
- Rizk, S.; Shah, B.; Martin, D.P.; Williams, S.F. Calendered Surgical Meshes Comprising. Polyhydroxyalkanoates. Patent US10874498B2, 29 December 2020. Available online: https://patents.google.com/patent/US10874498B2/en (accessed on 26 June 2025).
- Tao, X.; Zeng, W.; Yuan, Y. Hernia Patch and Preparation Method. Thereof. Patent CN107756781B, 10 March 2020. Available online: https://patents.google.com/patent/CN107756781B/en (accessed on 27 June 2025).
- Alami, R.; Tehrani, A.; Sabban, M.E. Surgical Mesh Implant for Hernia Repair and Methods of. Use. Patent US20230149147A1, 18 May 2023. Available online: https://patents.google.com/patent/US20230149147A1/en (accessed on 27 June 2025).
- Lewitus, D.; Roisman, S.; Dotan, A. Catechol Based Hot-Melt Tissue Adhesive for Hernia Mesh Repair. Surgery. Patent WO2021059272A1, 1 April 2021. Available online: https://patents.google.com/patent/WO2021059272A1/en (accessed on 26 June 2025).





| Mesh Name | Type | Direction | T0 (MPa) | Teq (MPa) | ΔΤ (%) | E0 (MPa) | Eeq (MPa) |
|---|---|---|---|---|---|---|---|
| MicroVal 2D Mesh | PP | L | 0.238 ± 0.042 | 0 (t = 1400 s) | 100.00 | 4.76 | 0.00 |
| MicroVal 2D Mesh | PP | T | 0.182 ± 0.028 | 0 (t = 250 s) | 100.00 | 3.64 | 0.00 |
| Parietex Composite | PET/collagen | L | 0.064 ± 0.008 | 0.041 | 35.93 | 1.28 | 0.82 |
| Parietex Composite | PET/collagen | T | 0.039 ± 0.013 | 0 (t = 151 s) | 100.00 | 0.78 | 0.00 |
| Surgimesh | PP | L | 0.111 ± 0.050 | 0.059 | 46.85 | 2.22 | 1.18 |
| Surgimesh | PP | T | 0.168 ± 0.040 | 0.082 | 51.19 | 3.36 | 1.64 |
| Surgipro | PP | L | 0.144 ± 0.029 | 0.058 | 59.72 | 2.88 | 1.16 |
| Surgipro | PP | T | 0.321 ± 0.120 | 0.128 | 60.12 | 6.42 | 2.56 |
| TecnoMesh | PP | L | 0.187 ± 0.060 | 0.080 | 57.22 | 3.74 | 1.60 |
| TecnoMesh | PP | T | 0.511 ± 0.040 | 0.218 | 57.33 | 10.22 | 4.36 |
| Optilene | PP | L | 0.187 ± 0.149 | 0 (t = 180 s) | 100.00 | 3.74 | 0.00 |
| Optilene | PP | T | 1.028 ± 1.270 | 0.542 | 47.28 | 20.56 | 10.84 |
| Parietex LW | PET | L | 0.429 ± 0.040 | 0.306 | 28.67 | 8.58 | 6.12 |
| Parietex LW | PET | T | 0.245 ± 0.020 | 0.184 | 24.90 | 4.90 | 3.68 |
| Ultrapro | PP/PGC-25 | L | 0.141 ± 0.016 | 0 (t = 300 s) | 100.00 | 2.82 | 0.00 |
| Ultrapro | PP/PGC-25 | T | 0.154 ± 0.003 | 0.044 | 71.43 | 3.08 | 0.88 |
| Vypro II | PP/PG 910 | L | 0.510 ± 0.240 | 0.412 | 19.22 | 10.20 | 8.24 |
| Vypro II | PP/PG 910 | T | 0.098 ± 0.030 | 0.078 | 20.41 | 1.96 | 1.56 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antoniadi, E.; Ferreira, N.M.; Vaz, M.F.; Parente, M.; Ferraz, M.P.; Silva, E. Innovative Strategies in Hernia Mesh Design: Materials, Mechanics, and Modeling. Materials 2025, 18, 3509. https://doi.org/10.3390/ma18153509
Antoniadi E, Ferreira NM, Vaz MF, Parente M, Ferraz MP, Silva E. Innovative Strategies in Hernia Mesh Design: Materials, Mechanics, and Modeling. Materials. 2025; 18(15):3509. https://doi.org/10.3390/ma18153509
Chicago/Turabian StyleAntoniadi, Evangelia, Nuno Miguel Ferreira, Maria Francisca Vaz, Marco Parente, Maria Pia Ferraz, and Elisabete Silva. 2025. "Innovative Strategies in Hernia Mesh Design: Materials, Mechanics, and Modeling" Materials 18, no. 15: 3509. https://doi.org/10.3390/ma18153509
APA StyleAntoniadi, E., Ferreira, N. M., Vaz, M. F., Parente, M., Ferraz, M. P., & Silva, E. (2025). Innovative Strategies in Hernia Mesh Design: Materials, Mechanics, and Modeling. Materials, 18(15), 3509. https://doi.org/10.3390/ma18153509