
Dimensional Accuracy Assessment of 3D-Printed Edentulous Jaw Models: A Comparative Analysis Using Three Laboratory Scanners


Abstract
1. Introduction
1.1. Background
1.2. Objective
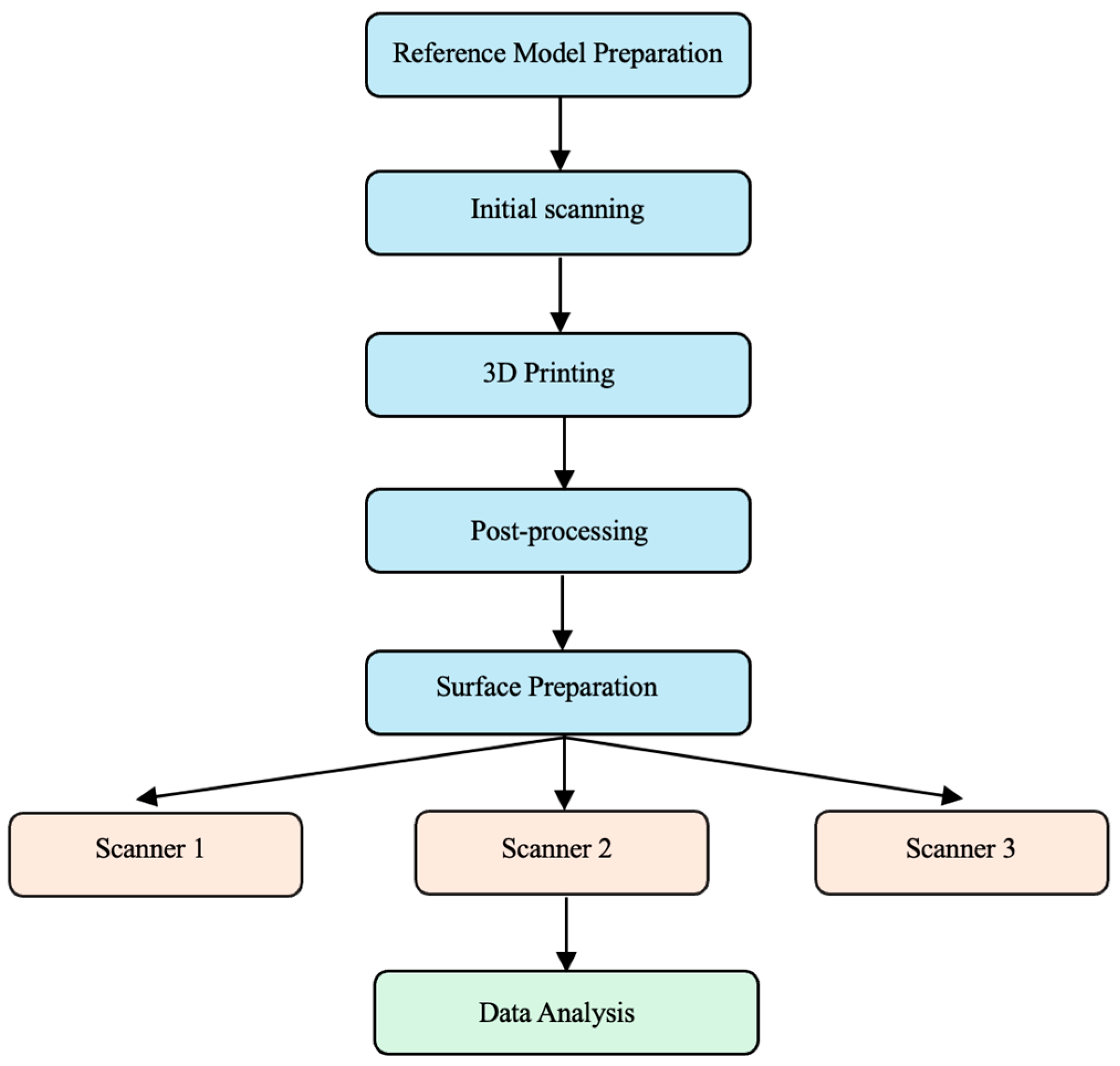
2. Materials and Methods
2.1. Study Design and Reference Model Preparation
2.2. Digital Workflow and Model Production
2.3. Model Preparation and Processing
2.4. Scanning Equipment
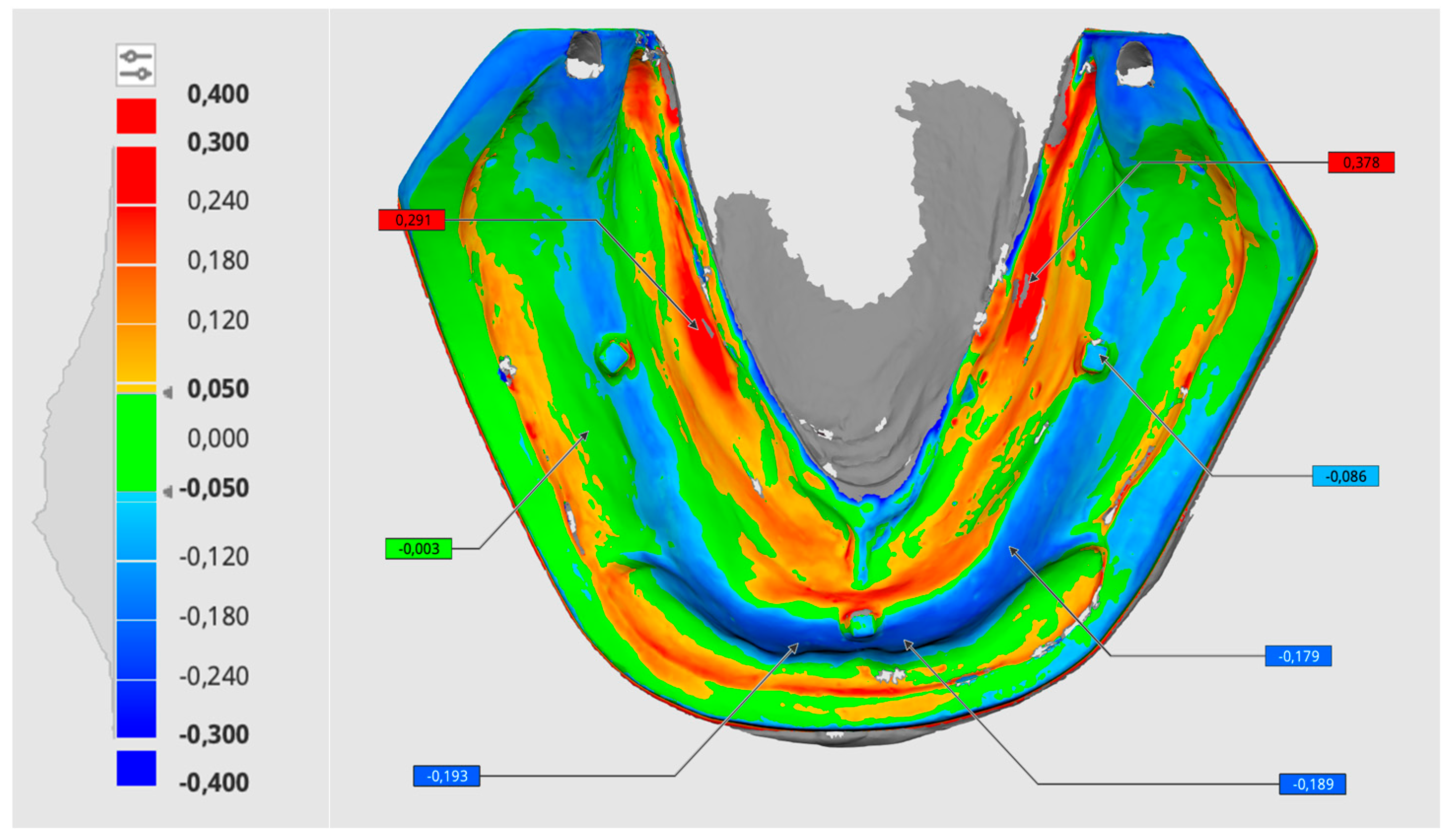
2.5. Digital Analysis Methodology
- Root mean square (RMS) deviation in millimeters, subsequently converted to micrometers;
- Percentage of values within the acceptable deviation range (±0.05 mm, green color).
2.6. Statistical Analysis
3. Results
3.1. Model Trueness
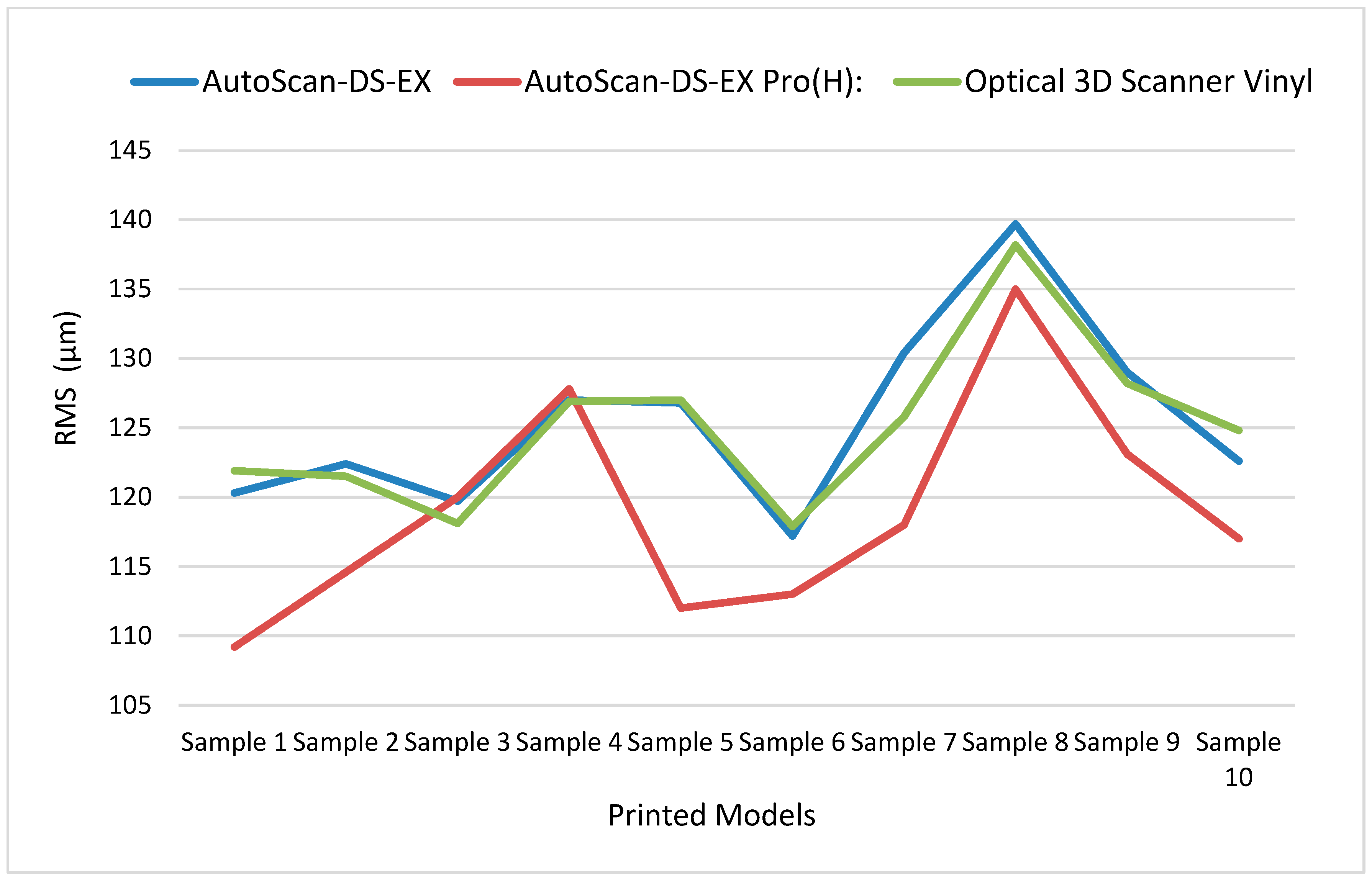
3.2. Model Precision
3.2.1. RMS (Root Mean Square)
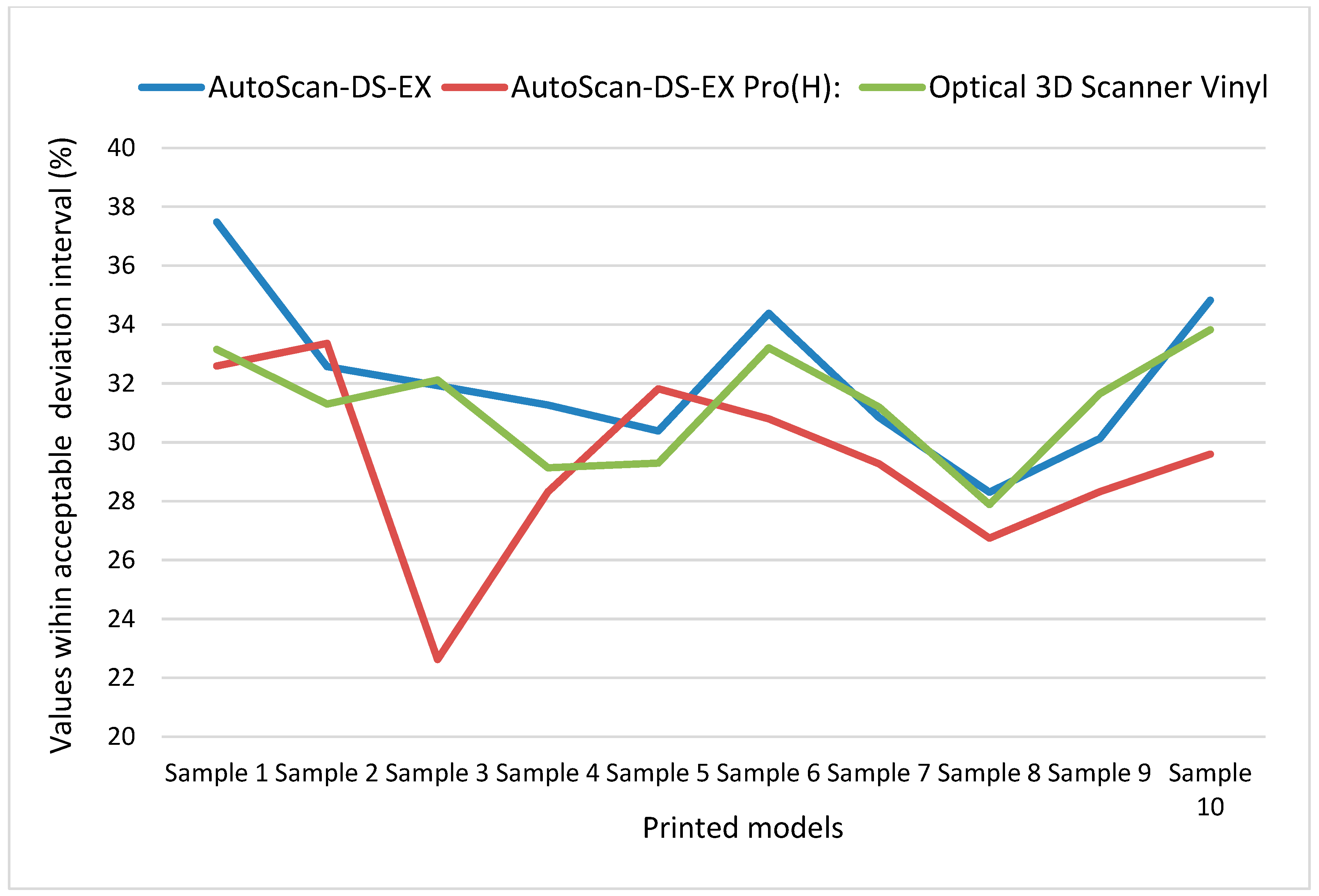
3.2.2. Acceptable Deviation
3.2.3. ICC, Confidence Interval (CI), and Correlation Analysis of RMS and Acceptable Deviation Percentage Metrics
AutoScan-DS-EX Data Analysis
AutoScan-DS-EX Pro(H) Data Analysis
Optical 3D Scanner Vinyl Data Analysis
3.3. Scanner Trueness Comparison
4. Discussion
4.1. Model Trueness
4.2. Model Precision
4.3. Scanner Trueness
4.4. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nulty, A.; Nguyen, V.; Nulty, A. A comparison of trueness and precision of 12 3D printers used in dentistry. BDJ Open 2022, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Czajkowska, M.; Walejewska, E.; Zadrożny, Ł.; Wieczorek, M.; Święszkowski, W.; Wagner, L.; Mijiritsky, E.; Markowski, J. Comparison of Dental Stone Models and Their 3D Printed Acrylic Replicas for the Accuracy and Mechanical Properties. Materials 2020, 13, 4066. [Google Scholar] [CrossRef] [PubMed]
- Etemad-Shahidi, Y.; Qallandar, O.B.; Evenden, J.; Alifui-Segbaya, F.; Ahmed, K.E. Accuracy of 3-Dimensionally Printed Full-Arch Dental Models: A Systematic Review. J. Clin. Med. 2020, 9, 3357. [Google Scholar] [CrossRef] [PubMed]
- Michaud, P.L.; Talmazov, G. Effects of remeshing algorithms on trueness of fit when used to compress.stl files for dental models: A narrative review. J. Dent. 2023, 134, 104531. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Peng, T.; Lin, Y.; Zhang, M.; Ren, G. Effect of internal structures on the accuracy of 3D printed full-arch dentition preparation models in different printing systems. J. Adv. Prosthodont. 2023, 15, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Yousef, H.; Harris, B.T.; Elathamna, E.N.; Morton, D.; Lin, W.S. Effect of additive manufacturing process and storage condition on the dimensional accuracy and stability of 3D-printed dental casts. J. Prosthet. Dent. 2022, 128, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Katheng, A.; Kanazawa, M.; Iwaki, M.; Minakuchi, S. Evaluation of dimensional accuracy and degree of polymerization of stereolithography photopolymer resin under different postpolymerization conditions: An in vitro study. J. Prosthet. Dent. 2021, 125, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Lim, J.H.; Kang, Y.J.; Kim, J.H.; Shim, J.S.; Kim, J.E. Evaluation of the 3D Printing Accuracy of a Dental Model According to Its Internal Structure and Cross-Arch Plate Design: An In Vitro Study. Materials 2020, 13, 5433. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Shin, Y.S.; Jung, H.D.; Hwang, C.J.; Baik, H.S.; Cha, J.Y. Precision and trueness of dental models manufactured with different 3-dimensional printing techniques. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, B.; Donmez, M.B.; Kahveci, Ç.; Cuellar, A.R.; de Paula, M.S.; Schimmel, M.; Abou-Ayash, S.; Çakmak, G. Effect of printing layer thickness on the trueness and fit of additively manufactured removable dies. J. Prosthet. Dent. 2022, 128, 1318.e1–1318.e9. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y. Influence of Different Postprocessing Rinsing Agents on the Manufacturing Accuracy of Dental Models Printed by LCD Resin 3D Printer. Master’s Thesis, Texas A&M University, College Station, TX, USA, 2022. Available online: https://hdl.handle.net/1969.1/197435 (accessed on 13 March 2025).
- Taneva, I.; Uzunov, T. Influence of post-polymerization processing on the mechanical characteristics of 3D-printed occlusal splints. J. Phys. Conf. Ser. 2020, 1492, 012018. [Google Scholar] [CrossRef]
- Kim, J.H.; Kwon, J.S.; Park, J.M.; Lo Russo, L.; Shim, J.S. Effects of postpolymerization conditions on the physical properties, cytotoxicity, and dimensional accuracy of a 3D printed dental restorative material. J. Prosthet. Dent. 2024, 132, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Väyrynen, V.O.; Tanner, J.; Vallittu, P.K. The anisotropicity of the flexural properties of an occlusal device material processed by stereolithography. J. Prosthet. Dent. 2016, 116, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.-h.; Son, K.; Lee, K.-b. Accuracy of Five Intraoral Scanners and Two Laboratory Scanners for a Complete Arch: A Comparative In Vitro Study. Appl. Sci. 2020, 10, 74. [Google Scholar] [CrossRef]
- Borbola, D.; Berkei, G.; Simon, B.; Romanszky, L.; Sersli, G.; DeFee, M.; Renne, W.; Mangano, F.; Vag, J. In vitro comparison of five desktop scanners and an industrial scanner in the evaluation of an intraoral scanner accuracy. J. Dent. 2023, 129, 104391. [Google Scholar] [CrossRef] [PubMed]
- Nulty, A. A Comparison of Full Arch Trueness and Precision of Nine Intra-Oral Digital Scanners and Four Lab Digital Scanners. Dent. J. 2021, 9, 75. [Google Scholar] [CrossRef] [PubMed]
- Kontis, P.; Güth, J.-F.; Schubert, O.; Keul, C. Accuracy of intraoral scans of edentulous jaws with different generations of intraoral scanners compared to laboratory scans. J. Adv. Prosthodont. 2021, 13, 316. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Chen, L.; Harris, B.T.; Bhandari, B.; Morton, D.; Lin, W.S. Accuracy and reproducibility of virtual edentulous casts created by laboratory impression scan protocols. J. Prosthet. Dent. 2018, 120, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, G.; Padhiary, S.K.; Mohanty, N.; Molinero-Mourelle, P.; Chebib, N. Accuracy of Intraoral Scanner for Recording Completely Edentulous Arches—A Systematic Review. Dent. J. 2023, 11, 241. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Ruggiero, G.; Ferrari, M.; Mangano, F.; Joda, T.; Sorrentino, R. Accuracy of a chairside intraoral scanner compared with a laboratory scanner for the completely edentulous maxilla: An in vitro 3-dimensional comparative analysis. J. Prosthet. Dent. 2020, 124, e1–e761. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.C.; Yang, C.C.; Levon, J.A.; Chu, T.G.; Morton, D.; Lin, W.S. The effects of additive manufacturing technologies and finish line designs on the trueness and dimensional stability of 3D-printed dies. J. Prosthodont. 2023, 32, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Al-Rafee, M.A. The epidemiology of edentulism and the associated factors: A literature Review. J. Family Med. Prim. Care 2020, 9, 1841–1843. [Google Scholar] [CrossRef] [PubMed]
- Galeva, H.; Uzunov, T.; Sofronov, Y.; Valcheva, Z. Evaluation of the accuracy of the optical scanners used in the modern dental practice. J. Phys. Conf. Ser. 2020, 1492, 012017. [Google Scholar] [CrossRef]
- Son, K.; Lee, W.-S.; Lee, K.-B. Effect of Different Software Programs on the Accuracy of Dental Scanner Using Three-Dimensional Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8449. [Google Scholar] [CrossRef] [PubMed]
- Morón-Conejo, B.; López-Vilagran, J.; Cáceres, D.; Berrendero, S.; Pradíes, G. Accuracy of five different 3D printing workflows for dental models comparing industrial and dental desktop printers. Clin. Oral Investig. 2023, 27, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Rungrojwittayakul, O.; Kan, J.Y.; Shiozaki, K.; Swamidass, R.S.; Goodacre, B.J.; Goodacre, C.J.; Lozada, J.L. Accuracy of 3D Printed Models Created by Two Technologies of Printers with Different Designs of Model Base. J. Prosthodont. 2020, 29, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Deng, K.; Chen, H.; Wang, Y.; Zhou, Y.; Sun, Y. Evaluation of functional suitable digital complete denture system based on 3D printing technology. J. Adv. Prosthodont. 2021, 13, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Al-Dulaijan, Y.A.; Alalawi, H.; Gad, M.M.; Al-Qarni, F.D.; Fouda, S.M.; Ellakany, P. Trueness and precision of complete denture digital impression compared to conventional impression: An in vitro study. PeerJ 2025, 13, e19075. [Google Scholar] [CrossRef] [PubMed]
- Emir, F.; Ayyildiz, S. Accuracy evaluation of complete-arch models manufactured by three different 3D printing technologies: A three-dimensional analysis. J. Prosthodont. Res. 2021, 65, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.A.; Papaioannou, W.; Papadopoulou, E.; Dalampira, M.; Tsolakis, A.I. Comparison in Terms of Accuracy between DLP and LCD Printing Technology for Dental Model Printing. Dent. J. 2022, 10, 181. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Hauschild, U.; Veronesi, G.; Imburgia, M.; Mangano, C.; Admakin, O. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: A comparative in vitro study. BMC Oral Health 2019, 19, 101. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Layers Thickness (mm) | 0.05 |
| Normal Exposure Time (s) | 3.00 |
| Off Time (s) | 1.00 |
| Bottom Exposure Time (s) | 50.00 |
| Bottom Layers | 5 |
| Anti-alias | 16 |
| Gray Level | 0 |
| Image Blur | 0 |
| Control Type | Basic |
| Z Lift Distance (mm) | 6.00 |
| Z Lift Speed (mm/s) | 4.00 |
| Z Retract Speed (mm/s) | 6.00 |
| Scanner | Manufacturer | Cameras | Resolution | Light Source | Powder Coating |
|---|---|---|---|---|---|
| Scanner 1—AutoScan-DS-EX | Shining 3D Tech Co., Ltd. | 1 camera × 1.3 megapixels | 15 µm | White light | No |
| Scanner 2—AutoScan-DS-EX Pro(H) | Shining 3D Tech Co., Ltd. | 2 cameras × 5 megapixels | 8 µm | Blue light | Yes |
| Scanner 3—Optical 3D Scanner Vinyl | Smart optics Sensortechnik GmbH (Bochum, Germany) | 1 camera × 3.2 megapixels | 4 µm | Blue light | Yes |
| Scanner | Model | RMS (µm) | Acceptable Deviation (%) | ||||
|---|---|---|---|---|---|---|---|
| n | Mean | Standard Deviation | n | Mean | Standard Deviation | ||
| AutoScan-DS-EX | Reference | 10 | 0.0 a | 0.0 | 10 | 100.00 a | 0.00 |
| Model 1 | 10 | 120.3 be | 12.3 | 10 | 37.49 b | 2.94 | |
| Model 2 | 10 | 122.4 b | 0.7 | 10 | 32.57 c | 0.29 | |
| Model 3 | 10 | 119.7 de | 0.8 | 10 | 31.93 d | 0.49 | |
| Model 4 | 10 | 127.0 fe | 0.0 | 10 | 31.26 e | 0.88 | |
| Model 5 | 10 | 126.8 fe | 1.0 | 10 | 30.38 f | 1.01 | |
| Model 6 | 10 | 117.2 ge | 0.8 | 10 | 34.38 g | 0.61 | |
| Model 7 | 10 | 130.4 he | 0.5 | 10 | 30.84 ef | 0.41 | |
| Model 8 | 10 | 139.7 c | 0.9 | 10 | 28.31 h | 0.76 | |
| Model 9 | 10 | 129.0 ie | 0.7 | 10 | 30.13 f | 0.63 | |
| Model 10 | 10 | 122.6 b | 0.7 | 10 | 34.83 g | 0.46 | |
| Scanner | Model | RMS (µm) | Acceptable Deviation (%) | ||||
|---|---|---|---|---|---|---|---|
| n | Mean | Standard Deviation | n | Mean | Standard Deviation | ||
| AutoScan-DS-EX Pro(H) | Reference | 10 | 0.0 a | 0.0 | 10 | 100.00 a | 0.00 |
| Model 1 | 10 | 109.2 b | 0.4 | 10 | 32.59 b | 0.33 | |
| Model 2 | 10 | 114.6 c | 0.5 | 10 | 33.37 c | 0.51 | |
| Model 3 | 10 | 120.0 d | 0.0 | 10 | 22.62 d | 0.16 | |
| Model 4 | 10 | 127.8 e | 0.8 | 10 | 28.32 e | 0.74 | |
| Model 5 | 10 | 112.0 f | 0.0 | 10 | 31.82 f | 0.25 | |
| Model 6 | 10 | 113.0 ᵍ | 0.0 | 10 | 30.80 g | 0.12 | |
| Model 7 | 10 | 118.0 h | 0.0 | 10 | 29.27 h | 0.42 | |
| Model 8 | 10 | 135.0 i | 0.0 | 10 | 26.74 i | 0.11 | |
| Model 9 | 10 | 123.1 j | 0.3 | 10 | 28.33 e | 0.17 | |
| Model 10 | 10 | 117.0 k | 0.0 | 10 | 29.60 h | 0.45 | |
| Scanner | Model | RMS (µm) | Acceptable Deviation (%) | ||||
|---|---|---|---|---|---|---|---|
| n | Mean | Standard Deviation | n | Mean | Standard Deviation | ||
| Optical 3D Scanner Vinyl | Reference | 10 | 0.0 a | 0.0 | 10 | 100.00 a | 0.00 |
| Model 1 | 10 | 121.9 b | 0.7 | 10 | 33.16 b | 0.78 | |
| Model 2 | 10 | 121.5 b | 1.9 | 10 | 31.30 c | 0.58 | |
| Model 3 | 10 | 118.1 c | 1.9 | 10 | 32.12 d | 0.73 | |
| Model 4 | 10 | 126.9 d | 0.7 | 10 | 29.14 e | 0.31 | |
| Model 5 | 10 | 127.0 dfi | 2.0 | 9 | 29.29 e | 0.53 | |
| Model 6 | 10 | 117.9 c | 0.6 | 10 | 33.21 di | 0.44 | |
| Model 7 | 10 | 125.8 ef | 1.2 | 10 | 31.20 c | 0.46 | |
| Model 8 | 10 | 138.2 g | 0.6 | 10 | 27.89 f | 0.45 | |
| Model 9 | 10 | 128.2 hi | 0.8 | 10 | 31.66 g | 0.17 | |
| Model 10 | 10 | 124.8 e | 1.5 | 10 | 33.83 hi | 0.73 | |
| Model | Average RMS (µm) | Standard Deviation (µm) | Average Match (%) | Standard Deviation (%) |
|---|---|---|---|---|
| Sample 1 | 117.1 | 6.92 | 34.41 | 2.67 |
| Sample 2 | 119.5 | 4.27 | 32.41 | 1.04 |
| Sample 3 | 119.3 | 1.02 | 28.88 | 5.42 |
| Sample 4 | 127.2 | 0.49 | 29.57 | 1.52 |
| Sample 5 | 121.9 | 8.60 | 30.49 | 1.26 |
| Sample 6 | 116.0 | 2.65 | 32.79 | 1.83 |
| Sample 7 | 124.7 | 6.27 | 30.43 | 1.03 |
| Sample 8 | 137.6 | 2.40 | 27.64 | 0.81 |
| Sample 9 | 126.8 | 3.20 | 30.04 | 1.67 |
| Sample 10 | 121.5 | 4.02 | 32.74 | 2.77 |
| Scanner | Mean | Std Dev |
|---|---|---|
| AutoScan-DS-EX, RMS (µm) | 125.5 | 6.5 |
| AutoScan-DS-EX, acceptable deviation in % | 32.21 | 2.69 |
| AutoScan-DS-EX Pro(H), RMS (µm) | 118.9 | 7.8 |
| AutoScan-DS-EX Pro(H), acceptable deviation in % | 29.34 | 3.15 |
| Optical 3D Scanner Vinyl, RMS (µm) | 125.0 | 5.8 |
| Optical 3D Scanner Vinyl, acceptable deviation in % | 31.27 | 1.96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanakiev, S.; Dimova-Gabrovska, M. Dimensional Accuracy Assessment of 3D-Printed Edentulous Jaw Models: A Comparative Analysis Using Three Laboratory Scanners. Materials 2025, 18, 3323. https://doi.org/10.3390/ma18143323
Yanakiev S, Dimova-Gabrovska M. Dimensional Accuracy Assessment of 3D-Printed Edentulous Jaw Models: A Comparative Analysis Using Three Laboratory Scanners. Materials. 2025; 18(14):3323. https://doi.org/10.3390/ma18143323
Chicago/Turabian StyleYanakiev, Spartak, and Mariana Dimova-Gabrovska. 2025. "Dimensional Accuracy Assessment of 3D-Printed Edentulous Jaw Models: A Comparative Analysis Using Three Laboratory Scanners" Materials 18, no. 14: 3323. https://doi.org/10.3390/ma18143323
APA StyleYanakiev, S., & Dimova-Gabrovska, M. (2025). Dimensional Accuracy Assessment of 3D-Printed Edentulous Jaw Models: A Comparative Analysis Using Three Laboratory Scanners. Materials, 18(14), 3323. https://doi.org/10.3390/ma18143323