
Influence of the Cortical Layer Thickness and Trabecular Layer Pattern Density on 3D-Printed Femur Strength



Abstract
1. Introduction
2. Materials and Methods
2.1. Three-Dimensional Printer Zortrax M300 Plus
2.2. Filament Used for Printing
2.3. Three-Dimensional Model Preparation
2.4. Laboratory Testing of the Composite Femur Bone Model
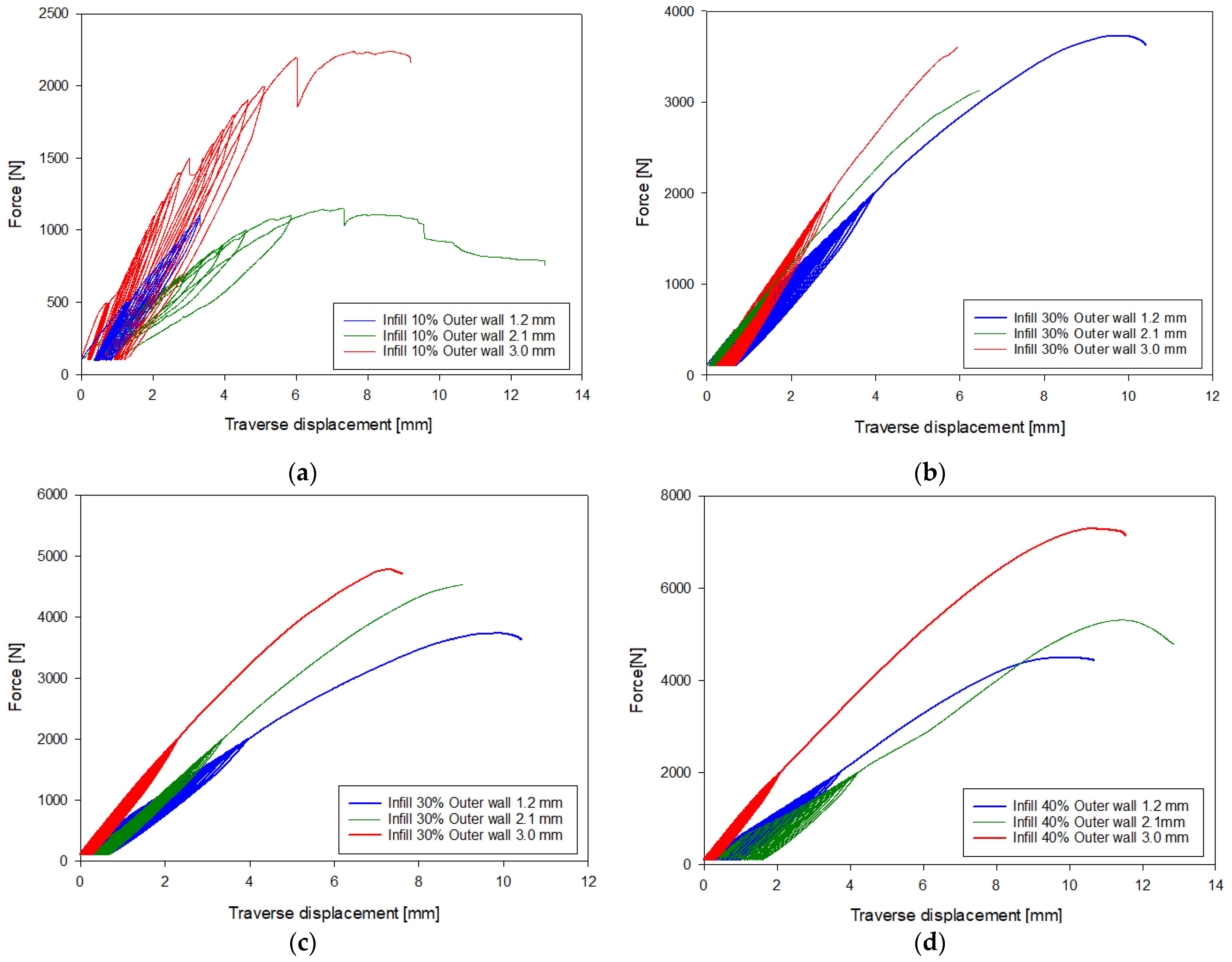
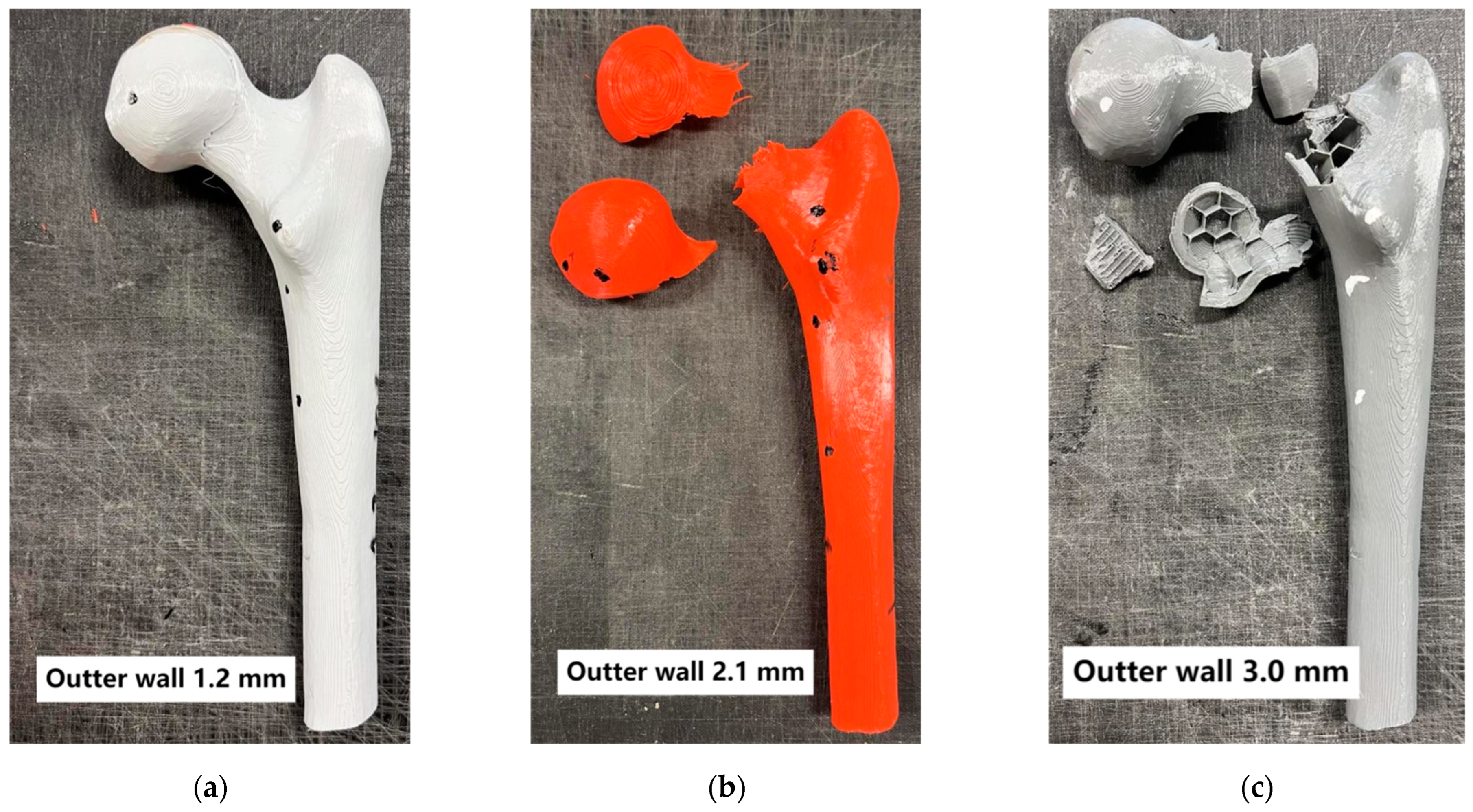
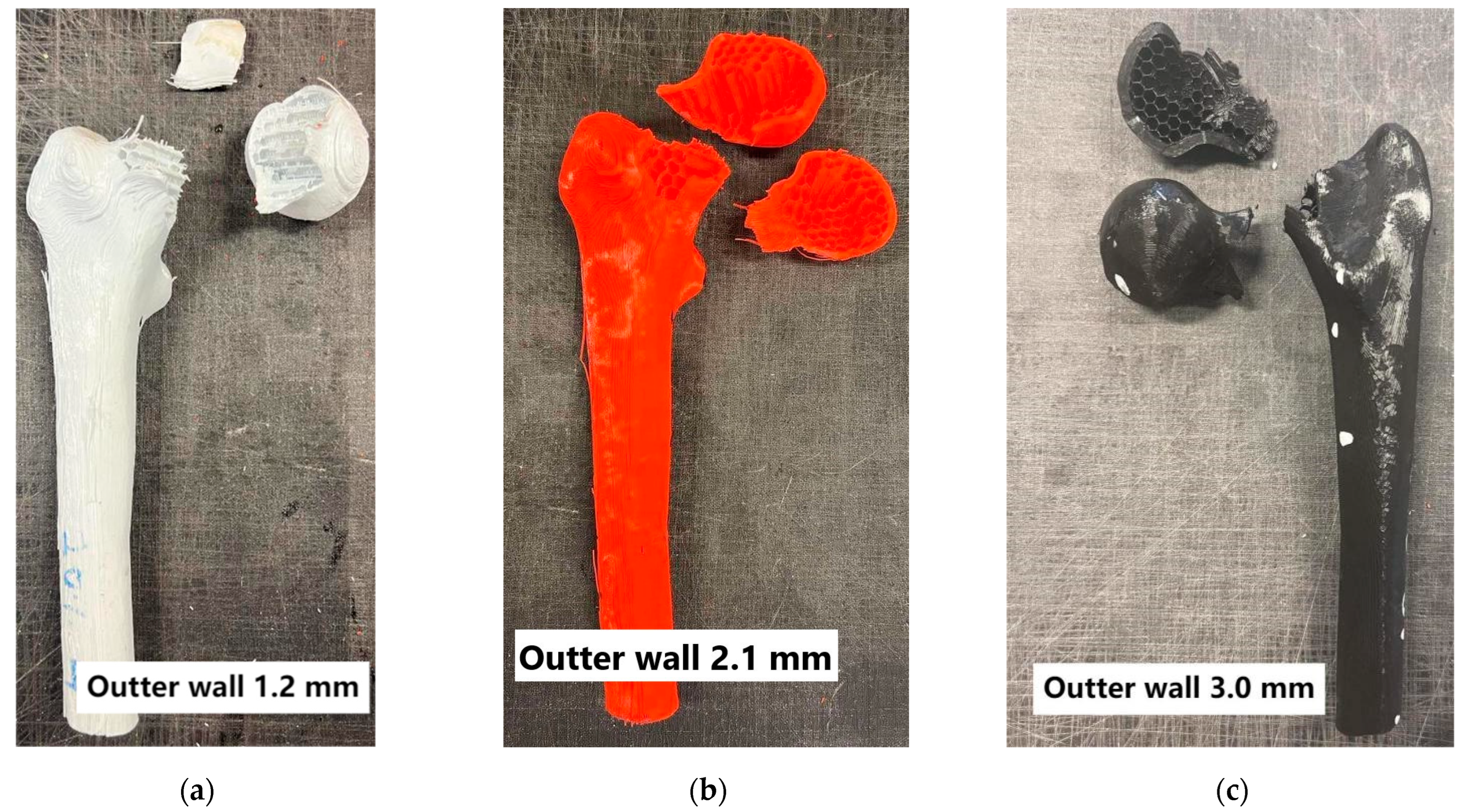
3. Results
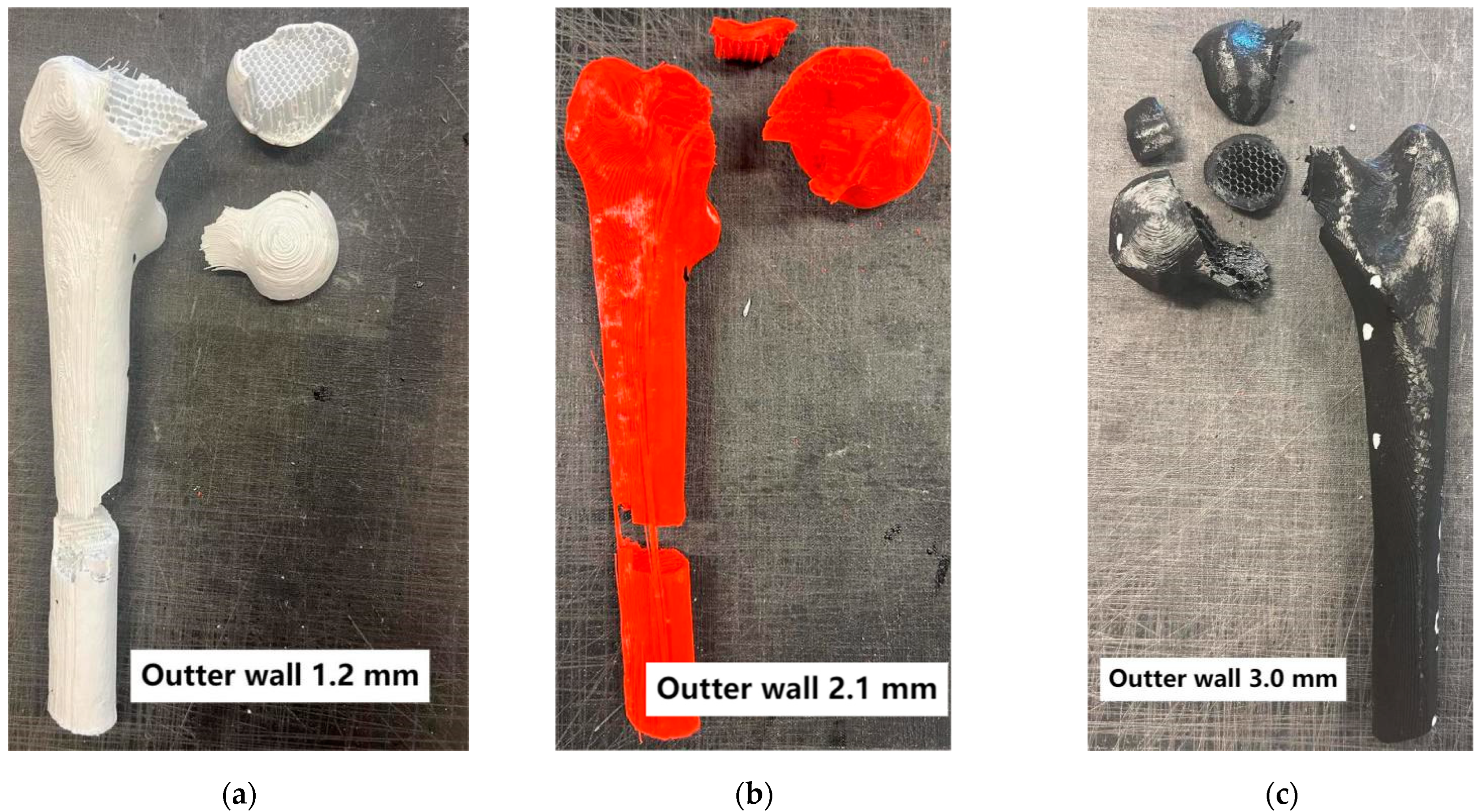
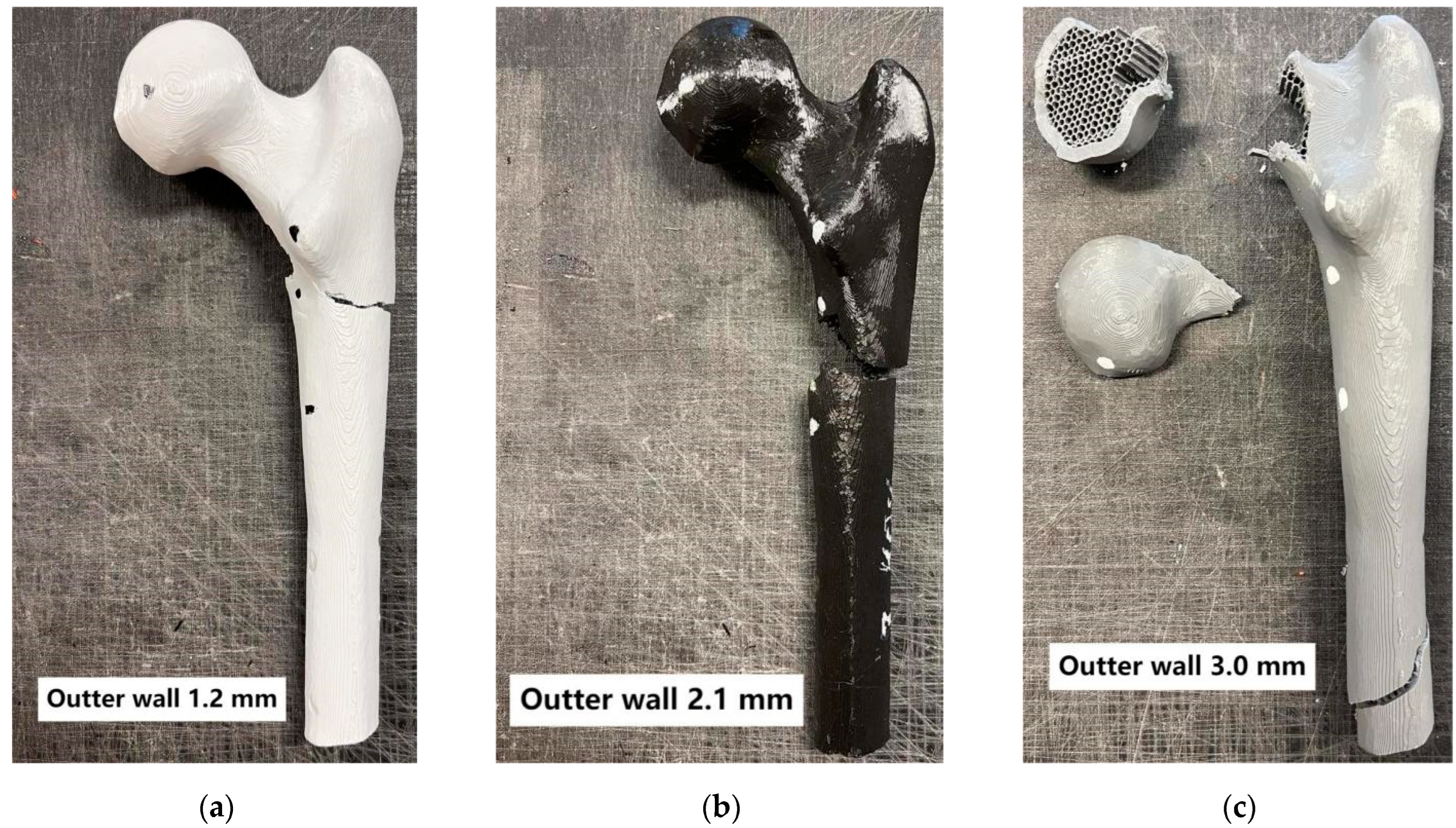
Analysis of 3D-Printed Bone
4. Discussion
4.1. Three-Dimensional-Printed Femur Bones by Other Authors vs. Three-Dimensional-Printed Bones
4.2. Commercial Bones vs. 3D-Printed Bones
4.3. Human vs. 3D-Printed Bones
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berman, B. 3-D printing: The new industrial revolution. Bus. Horiz. 2012, 55, 155–162. [Google Scholar] [CrossRef]
- Godoi, F.C.; Parakash, S.; Bhandari, B.R. 3D printing technologies applied for food design: Status and prospects. J. Food Eng. 2016, 179, 44–54. [Google Scholar] [CrossRef]
- Lim, C.W.J.; Le, K.Q.; Lu, Q.; Wong, C.H. An overview of 3D printing in manufacturing, aerospace, and automotive industries. IEEE Potentials 2016, 35, 18–22. [Google Scholar] [CrossRef]
- Chen, R.K.; Jin, Y.; Wensman, J.; Shih, A. Additive manufacturing of custom orthoses and prostheses—A review. Addit. Manuf. 2016, 12, 77–89. [Google Scholar] [CrossRef]
- Dombroski, C.E.; Balsdon, M.E.; Froats, A. The use of a low cost 3D scanning and printing tool in the manufacture of custom-made foot orthoses:a preliminary study. BMC Res. Notes 2014, 7, 443. [Google Scholar] [CrossRef]
- Telfer, S.; Pallari, J.; Munguia, J.; Dalgarno, K.; McGeough, M.; Woodburn, J. Embracing additive manufacture: Implications for foot and ankle orthosis design. BMC Musculoskelet. Disord. 2012, 13, 84. [Google Scholar] [CrossRef]
- Salles, A.S.; Gyi, D.E. An evaluation of personalised insoles developed using additive manufacturing. J. Sports Sci. 2013, 31, 442–450. [Google Scholar] [CrossRef]
- Ghai, S.I.; Sharma, Y.; Jain, N.; Satpathy, M.; Pillai, A.K. Use of 3-D printing technologies in caraniomaxillofacial surgery: A review. Oral Maxillofac. Surg. 2018, 22, 249–259. [Google Scholar] [CrossRef]
- Murphy, S.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef]
- Ventola, C.L. Medical Applications for 3D Printing: Current and Projected Uses. Pharm. Ther. 2014, 39, 704–711. [Google Scholar] [PubMed] [PubMed Central]
- Murr, L.E.; Gaytan, S.M.; Medina, F.; Lopez, H.; Martinez, E.; Machado, B.I.; Hernandez, D.H.; Martinez, L.; Lopez, M.I.; Wicker, R.B.; et al. Next-generation biomedical implants using additive manufacturing of complex, cellular and functional mesh arrays. Philos. Trans. A Math. Phys. Eng. Sci. 2010, 368, 1999–2032. [Google Scholar] [CrossRef] [PubMed]
- Rengier, F.; Mehndiratta, A.; von Tengg-Kobligk, H.; Zechmann, C.M.; Unterhinninghofen, R.; Kauczor, H.U.; Giesel, F.L. 3D printing based on imaging data: Review of medical applications. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ao, Q.; Tian, X.; Fan, J.; Wei, Y.; Hou, W.; Tong, H.; Bai, S. 3D Bioprinting Technologies for Hard Tissue and Organ Engineering. Materials 2016, 9, 802, Erratum in Materials 2016, 9, 911. https://doi.org/10.3390/ma9110911. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.Q.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. Part B Eng. 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Choudhari, C.; Patil, V. Product development and its comparative analysis by SLA, SLS and FDM rapid prototyping processes. IOP Conf. Ser. Mater. Sci. Eng. 2016, 149, 012009. [Google Scholar] [CrossRef]
- F42 Committee. Standard Terminology for Additive Manufacturingtechnologies; ASTM International: West Conshohocken, PA, USA, 2012. [Google Scholar] [CrossRef]
- Council, N.R. Accelerating Technology Transition: Bridging the Valley of Death for Materials and Processes in Defense Systems; The National Academies Press: Washington, DC, USA, 2004; Volume 4. [Google Scholar]
- Wohlers, T. Wohlers Report 2017: 3D Printing and Additive Manufacturing State of the Industry: Annual Worldwide Progress Report; Wohlers Associates, Inc.: Fort Collins, CO, USA, 2017. [Google Scholar]
- Yu, W.; Sun, X.; Meng, H.; Sun, B.; Chen, P.; Liu, X.; Zhang, K.; Yang, X.; Peng, J.; Lu, S. 3D-printed Porous Ceramic Scaffolds for Bone Tissue Engineering: A Review. Biomater. Sci. 2017, 5, 1690–1698. [Google Scholar] [CrossRef]
- Khoshnevis, B. Automated construction by contour crafting—Related robotics and information technologies. Autom. Constr. 2004, 13, 5–19. [Google Scholar] [CrossRef]
- Zadpoor, A.A.; Malda, J. Additive Manufacturing of Biomaterials, Tissues, and Organs. Ann. Biomed. Eng. 2017, 45, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Gungor-Ozkerim, P.S.; Zhang, Y.S.; Yue, K.; Zhu, K.; Liu, W.; Pi, Q.; Byambaa, B.; Dokmeci, M.R.; Shin, S.R.; et al. Direct 3D bioprinting of perfusable vascular constructs using a blend bioink. Biomaterials 2016, 106, 58–68. [Google Scholar] [CrossRef]
- Cui, X.; Breitenkamp, K.; Finn, M.G.; Lotz, M.; D’Lima, D.D. Direct Human Cartilage Repair Using Three-Dimensional Bioprinting Technology. Tissue Eng. Part A 2012, 18, 1304–1312. [Google Scholar] [CrossRef]
- Keriquel, V.; Guillemot, F.; Arnault, I.; Guillotin, B.; Miraux, S.; Amédée, J.; Fricain, J.-C.; Catros, S. In vivo bioprinting for computer- and robotic-assisted medical intervention: Preliminary study in mice. Biofabrication 2010, 2, 014101. [Google Scholar] [CrossRef]
- Zopf, D.A.; Hollister, S.J.; Nelson, M.E.; Ohye, R.G.; Green, G.E. Bioresorbable Airway Splint Created with a Three-Dimensional Printer. N. Engl. J. Med. 2013, 368, 2043–2045. [Google Scholar] [CrossRef] [PubMed]
- Cubo, N.; Garcia, M.; del Canizo, J.F.; Velasco, D.; Jorcano, J.L. 3D bioprinting of functional human skin: Production and in vivo analysis. Biofabrication 2016, 9, 015006. [Google Scholar] [CrossRef] [PubMed]
- Keriquel, V.; Oliveira, H.; Remy, M.; Zaine, S.; Delmond, S.; Rousseau, B.; Rey, S.; Catros, S.; Amedee, J.; Guillemont, F. In situ printing of mesenchymal stromal cells, by laserassisted bioprinting, for in vivo bone regeneration. Cartilage 2017, 8, 327–340. [Google Scholar] [CrossRef]
- Burkhard, M.; Fürnstahl, P.; Farshad, M. Three-dimensionally printed vertebrae with different bone densities for surgical training. Eur. Spine J. 2019, 28, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Clifton, W.; Pichelmann, M.; Vlasak, A.; Damon, A.; ReFaey, K.; Nottmeier, E. Investigation and Feasibility of Combined 3D Printed Thermoplastic Filament and Polymeric Foam to Simulate the Cortiocancellous Interface of Human Vertebrae. Sci. Rep. 2020, 10, 2912. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Clifton, W.; Damon, A.; Valero-Moreno, F.; Marenco-Hillembrand, L.; Nottmeier, E.; Tubbs, R.S.; Fox, W.C.; Pichelmann, M. Investigation of the “Superior Facet Rule” Using 3D-Printed Thoracic Vertebrae with Simulated Corticocancellous Interface. World Neurosurg. 2020, 143, e51–e59. [Google Scholar] [CrossRef] [PubMed]
- Metzner, F.; Neupetsch, C.; Carabello, A.; Pietsch, M.; Wendler, T.; Drossel, W.G. Biomechanical validation of additively manufactured artificial femoral bones. BMC Biomed. Eng. 2022, 4, 6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nägl, K.; Reisinger, A.; Pahr, D.H. The biomechanical behavior of 3D printed human femoral bones based on generic and patient-specific geometries. 3D Print Med. 2022, 8, 35. [Google Scholar] [CrossRef]
- Kumar, R.R.; Rajesh, D.; Kumaran, S.; Ranjieth, S.; Ali, M.I.; Karthik, K. Investigation on tensile characteristics of femur bone 3D model by using FDM. Mater. Today Proc. 2022, 52 Pt 3, 1504–1508. [Google Scholar] [CrossRef]
- Reznikov, N.; Alsheghri, A.A.; Piché, N.; Gendron, M.; Desrosiers, C.; Morozova, I.; Sanchez Siles, J.M.; Gonzalez-Quevedo, D.; Tamimi, I.; Song, J.; et al. Altered topological blueprint of trabecular bone associates with skeletal pathology in humans. Bone Rep. 2020, 12, 100264. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bini, F.; Pica, A.; Marinozzi, A.; Marinozzi, F. Prediction of Stress and Strain Patterns from Load Rearrangement in Human Osteoarthritic Femur Head: Finite Element Study with the Integration of Muscular Forces and Friction Contact. In New Developments on Computational Methods and Imaging in Biomechanics and Biomedical Engineering; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Chon, C.-s.; Yun, H.-s.; Kim, H.S.; Ko, C. Elastic Modulus of Osteoporotic Mouse Femur Based on Femoral Head Compression Test. Appl. Bionics Biomech. 2017, 2017, 7201769. [Google Scholar] [CrossRef]
- Gardner, M.P.; Chong, A.C.; Pollock, A.G.; Wooley, P.H. Mechanical evaluation of large-size fourth-generation composite femur and tibia models. Ann. Biomed. Eng. 2010, 38, 613–620. [Google Scholar] [CrossRef]
- Heiner, A.D.; Brown, T.D. Structural properties of a new design of composite replicate femurs and tibias. J. Biomech. 2001, 34, 773–781. [Google Scholar] [CrossRef]
- Miura, M.; Nakamura, J.; Matsuura, Y.; Wako, Y.; Suzuki, T.; Hagiwara, S.; Orita, S.; Inage, K.; Kawarai, Y.; Sugano, M.; et al. Prediction of fracture load and stiffness of the proximal femur by CT-based specimen specific finite element analysis: Cadaveric validation study. BMC Musculoskelet Disord. 2017, 18, 536. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Iori, G.; Peralta, L.; Reisinger, A.; Heyer, F.; Wyers, C.; van den Bergh, J.; Pahr, D.; Raum, K. Femur strength predictions by nonlinear homogenized voxel finite element models reflect the microarchitecture of the femoral neck. Med. Eng. Phys. 2020, 79, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Cody, D.D.; Gross, G.J.; Hou, F.J.; Spencer, H.J.; Goldstein, S.A.; Fyhrie, D.P. Femoral strength is better predicted by finite element models than QCT and DXA. J. Biomech. 1999, 32, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Link, T.M.; Vieth, V.; Langenberg, R.; Meier, N.; Lotter, A.; Newitt, D.; Majumdar, S. Structure analysis of high resolution magnetic resonance imaging of the proximal femur: In vitro correlation with biomechanical strength and BMD. Calcif. Tissue Int. 2003, 72, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Dall’Ara, E.; Luisier, B.; Schmidt, R.; Kainberger, F.; Zysset, P.; Pahr, D. A nonlinear QCT-based finite element model validation study for the human femur tested in two configurations in vitro. Bone 2013, 52, 27–38. [Google Scholar] [CrossRef]
- Mirzaali, M.J.; Zadpoor, A.A. Orthopedic meta-implants. APL Bioeng. 2024, 8, 010901. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Hardness in shore scale | 81 D |
| Shrinkage | ~0 [%] |
| Elongation at break | 4.83 [%] |
| Strength at break | 528.8 [N] |
| Resilience for V-Notch | 0.29 J/cm2 |
| Young Modulus | 1471.93 [MPa] |
| Tensil at break | 55.25 [MPa] |
| Print temp | 190–230 °C |
| Heated bed | Not require |
| Nozzle | 0.2–0.4 [mm] |
| Cooling | 0–60 [%] |
| Flow | 100 [%] |
| Cortical Layer Thickness | Axial Strength of Bone [N] | |||
|---|---|---|---|---|
| 10% | 20% | 30% | 40% | |
| 1.2 mm | 1073 | 2116 | 3727 | 4492 |
| 2.1 mm | 1110 | 3124 | 4519 | 5298 |
| 3.0 mm | 2240 | 3595 | 4779 | 7291 |
| Cortical Layer Thickness | Length of the Used Material [m] | |||
|---|---|---|---|---|
| 10% | 20% | 30% | 40% | |
| 1.2 mm | 36.63 | 41.05 | 46.74 | 53.03 |
| 2.1 mm | 40.21 | 45.20 | 50.76 | 56.79 |
| 3.0 mm | 47.05 | 51.85 | 56.95 | 62.34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Znaczko, A.; Żerdzicki, K.; Kłosowski, P. Influence of the Cortical Layer Thickness and Trabecular Layer Pattern Density on 3D-Printed Femur Strength. Materials 2025, 18, 2187. https://doi.org/10.3390/ma18102187
Znaczko A, Żerdzicki K, Kłosowski P. Influence of the Cortical Layer Thickness and Trabecular Layer Pattern Density on 3D-Printed Femur Strength. Materials. 2025; 18(10):2187. https://doi.org/10.3390/ma18102187
Chicago/Turabian StyleZnaczko, Aleksander, Krzysztof Żerdzicki, and Paweł Kłosowski. 2025. "Influence of the Cortical Layer Thickness and Trabecular Layer Pattern Density on 3D-Printed Femur Strength" Materials 18, no. 10: 2187. https://doi.org/10.3390/ma18102187
APA StyleZnaczko, A., Żerdzicki, K., & Kłosowski, P. (2025). Influence of the Cortical Layer Thickness and Trabecular Layer Pattern Density on 3D-Printed Femur Strength. Materials, 18(10), 2187. https://doi.org/10.3390/ma18102187