

Comparative Evaluation of the Digital Workflow and Conventional Method in Manufacturing Complete Removal Prostheses



Abstract
:1. Introduction
- Subtractive or milling technique. It utilizes pre-polymerized PMMA discs that are milled under high pressure and controlled conditions. Recent research has shown that milled resins have better mechanical and surface properties (greater color stability, reduced bacterial colonization, and lower monomer release) than thermopolymerizable resins [19]. It is commonly used for fabricating fixed dental prostheses, inlays, onlays, veneers, or crowns [20,21,22].
- Additive or 3D printing technique. The additive manufacturing involves layer-by-layer deposition of liquid resins on a support structure, followed by curing with visible light, ultraviolet light, heat, or laser. This process is repeated until the complete prosthesis takes the shape specified in the digital design software. The use of this technique is increasing in dentistry as it allows fabrication not only of complete dentures but also fixed prostheses, surgical guides, occlusal splints, and more [20].
- A comparison of the properties of the final prosthesis, as well as the advantages and disadvantages between both conventional and CAD/CAM methods of fabricating complete mucosa-supported dentures.
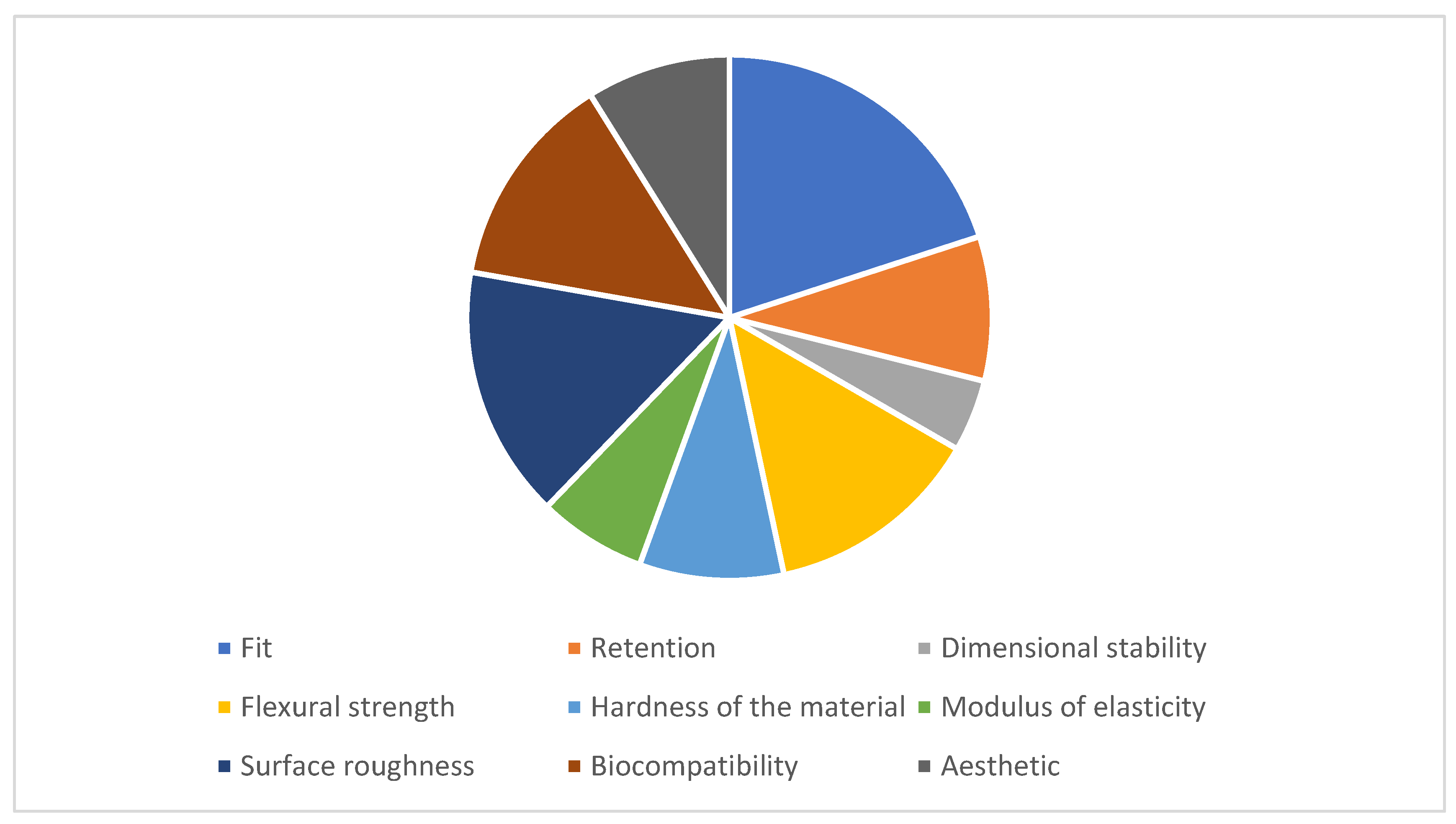
- A comparison of the fit, retention, fracture resistance, surface roughness, biocompatibility, and aesthetics of the base in conventional dentures and CAD/CAM-fabricated dentures.
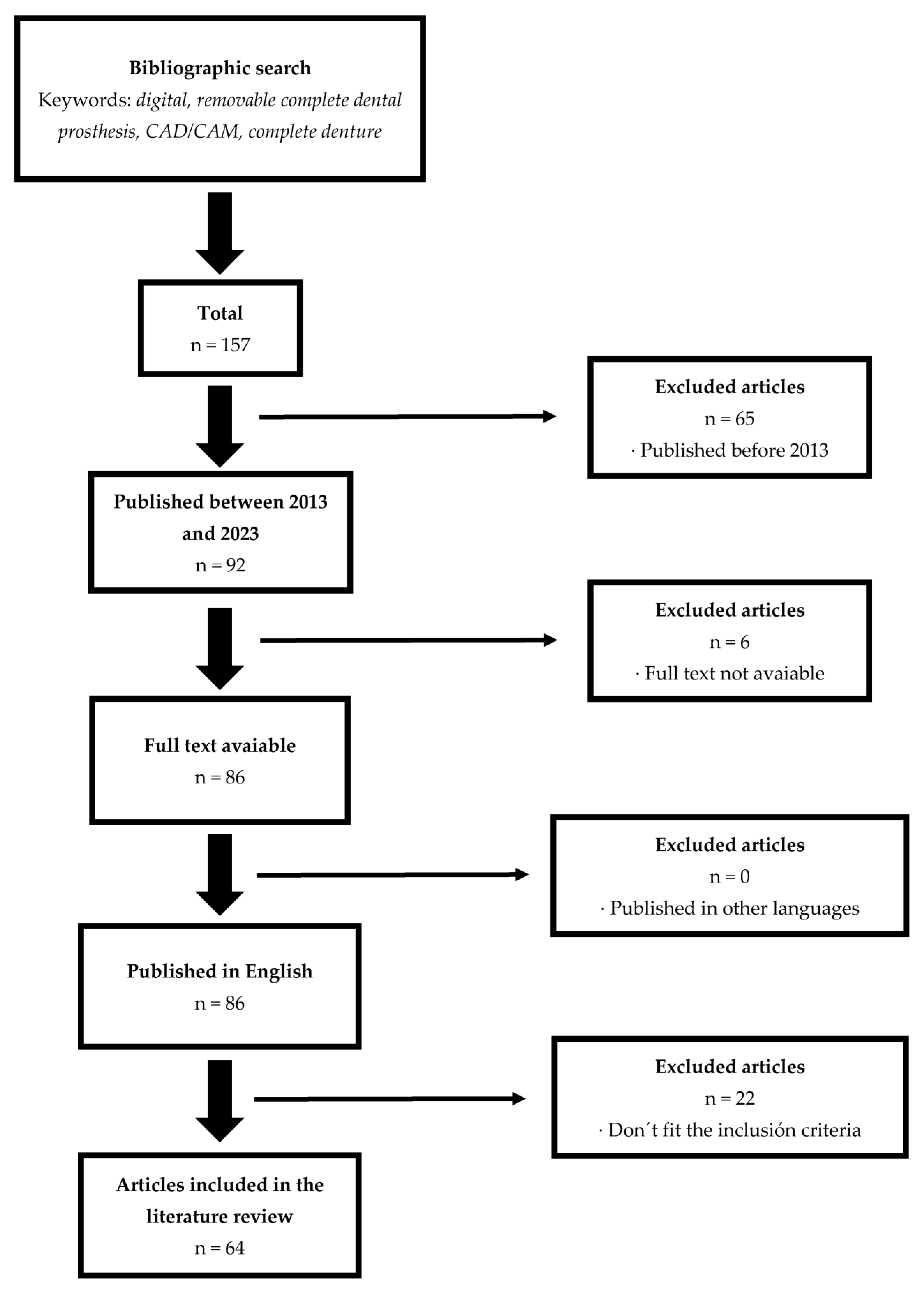
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
- Regarding fit, retention, fracture resistance, surface roughness, biocompatibility, and aesthetics, digital prostheses, particularly the milled ones, have demonstrated superior performance.
- The planning process of digital prostheses, with its advantage of preserving all data and prosthetic designs, except anatomical registers, facilitates quick retrieval at any time.
Author Contributions
Funding
Conflicts of Interest
References
- Alfadda, S.A. The relationship between various parameters of complete denture quality and patients’ satisfaction. J. Am. Dent. Assoc. 2014, 145, 941–948. [Google Scholar] [CrossRef]
- Sanjeevan, V.; Rajagopal, P.; Venkitachalam, R.; Aras, M. Efficiency of simplified versus traditional denture fabrication methods: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 126, 377–385. [Google Scholar] [CrossRef]
- Han, W.; Li, Y.; Zhang, Y.; Lv, Y.; Zhang, Y.; Hu, P.; Liu, H.; Ma, Z.; Shen, Y. Design and fabrication of complete dentures using CAD/CAM technology. Medicine 2017, 96, e5435. [Google Scholar] [CrossRef]
- Jokstad, A.; Ganeles, J. Systematic review of clinical and patient-reported outcomes following oral rehabilitation on dental implants with a tapered compared to a non-tapered implant design. Clin. Oral. Implants Res. 2018, 29, 41–54. [Google Scholar] [CrossRef]
- Romanos, G.E.; Delgado-Ruiz, R.; Sculean, A. Concepts for prevention of complications in implant therapy. Periodontology 2000 2019, 81, 7–17. [Google Scholar] [CrossRef]
- Jasiūnaitė, A.; Verenis, A.M.; Ivanauskienė, E.; Zilinskas, J. A comparison of mechanic properties regarding complete removable dentures, which were made from polymethylmetacrilate (PMMA) during conventional and CAD/CAM processes. Systemic literature review. Stomatologija 2022, 24, 3–12. [Google Scholar]
- Faty, M.; Sabet, M.; Thabet, Y. A Comparison of Denture Base Retention and Adaptation between CAD-CAM and Conventional Fabrication Techniques. Int. J. Prosthodont. 2023, 36, 469–478. Available online: http://quintpub.com/journals/ijp/abstract.php?iss2_id=1453&article_id=21203 (accessed on 18 May 2023). [CrossRef]
- de Villa Camargos, G.; Armenine, T.E.; Paleari, A.G.; Nascimento, G.M.O.; Munhoz, M.F.V. Teaching Complete Denture Procedures to Dental Students by Conventional or Simplified Methods: A Randomized Clinical Trial. J. Dent. Educ. 2019, 83, 303–313. [Google Scholar] [CrossRef]
- Emera, R.M.K.; Shady, M.; Alnajih, M.A. Comparison of retention and denture base adaptation between conventional and 3D-printed complete dentures. J. Dent. Res. Dent. Clin. Dent. Prospects 2022, 16, 179–185. [Google Scholar] [CrossRef]
- Vecchia, M.P.D.; Regis, R.R.; Cunha, T.R.; de Andrade, I.M.; da Matta, J.C.S.; de Souza, R.F. A Randomized Trial on Simplified and Conventional Methods for Complete Denture Fabrication: Cost Analysis: Cost of Simplified Complete Dentures. J. Prosthodont. 2014, 23, 182–191. [Google Scholar] [CrossRef]
- Ohara, K.; Isshiki, Y.; Hoshi, N.; Ohno, A.; Kawanishi, N.; Nagashima, S.; Inoue, M.; Kubo, D.; Yamaya, K.; Inoue, E.; et al. Patient satisfaction with conventional dentures vs. digital dentures fabricated using 3D-printing: A randomized crossover trial. J. Prosthodont. Res. 2022, 66, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, C.J.; Garbacea, A.; Naylor, W.P.; Daher, T.; Marchack, C.B.; Lowry, J. CAD/CAM fabricated complete dentures: Concepts and clinical methods of obtaining required morphological data. J. Prosthet. Dent. 2012, 107, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M.; Kalberer, N.; Naharro, M.; Marchand, L.; Lee, H.; Müller, F. CAD-CAM milled dentures: The Geneva protocols for digital dentures. J. Prosthet. Dent. 2020, 123, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Infante, L.; Yilmaz, B.; McGlumphy, E.; Finger, I. Fabricating complete dentures with CAD/CAM technology. J. Prosthet. Dent. 2014, 111, 351–355. [Google Scholar] [CrossRef]
- Yilmaz, B.; Azak, A.N.; Alp, G.; Ekşi, H. Use of CAD-CAM technology for the fabrication of complete dentures: An alternative technique. J. Prosthet. Dent. 2017, 118, 140–143. [Google Scholar] [CrossRef]
- Arslan, M.; Murat, S.; Alp, G.; Zaimoglu, A. Evaluation of flexural strength and surface properties of prepolymerized CAD/CAM PMMA-based polymers used for digital 3D complete dentures. Int. J. Comput. Dent. 2018, 21, 31–40. [Google Scholar]
- Ayman, A.D. The residual monomer content and mechanical properties of CAD\CAM resins used in the fabrication of complete dentures as compared to heat cured resins. Electron. Physician 2017, 9, 4766–4772. [Google Scholar] [CrossRef]
- Srinivasan, M.; Kalberer, N.; Kamnoedboon, P.; Mekki, M.; Durual, S.; Özcan, M.; Müller, F. CAD-CAM complete denture resins: An evaluation of biocompatibility, mechanical properties, and surface characteristics. J. Dent. 2021, 114, 103785. [Google Scholar] [CrossRef]
- Paolone, G.; Mandurino, M.; De Palma, F.; Mazzitelli, C.; Scotti, N.; Breschi, L.; Gherlone, E.; Cantatore, G.; Vichi, A. Color Stability of Polymer-Based Composite CAD/CAM Blocks: A Systematic Review. Polymers 2023, 15, 464. [Google Scholar] [CrossRef]
- Clark, W.A.; Brazile, B.; Matthews, D.; Solares, J.; De Kok, I.J. A Comparison of Conventionally Versus Digitally Fabricated Denture Outcomes in a University Dental Clinic. J. Prosthodont. 2021, 30, 47–50. [Google Scholar] [CrossRef]
- Wang, C.; Shi, Y.F.; Xie, P.J.; Wu, J.H. Accuracy of digital complete dentures: A systematic review of in vitro studies. J. Prosthet. Dent. 2021, 125, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Kattadiyil, M.T.; AlHelal, A. An update on computer-engineered complete dentures: A systematic review on clinical outcomes. J. Prosthet. Dent. 2017, 117, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M.; Kalberer, N.; Fankhauser, N.; Naharro, M.; Maniewicz, S.; Müller, F. CAD-CAM complete removable dental prostheses: A double-blind, randomized, crossover clinical trial evaluating milled and 3D-printed dentures. J. Dent. 2021, 115, 103842. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dent. Mater. 2016, 32, 54–64. [Google Scholar] [CrossRef] [PubMed]
- AlHelal, A.; AlRumaih, H.S.; Kattadiyil, M.T.; Baba, N.Z.; Goodacre, C.J. Comparison of retention between maxillary milled and conventional denture bases: A clinical study. J. Prosthet. Dent. 2017, 117, 233–238. [Google Scholar] [CrossRef]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z.; Kattadiyil, M.T. Comparison of denture base adaptation between CAD-CAM and conventional fabrication techniques. J. Prosthet. Dent. 2016, 116, 249–256. [Google Scholar] [CrossRef]
- Lozado, J.; Garbacea, A.; Goodacre, C.; Kattadiyil, M. Use of a Digitally Planned and Fabricated Mandibular Complete Denture for Easy Conversion to an Immediately Loaded Provisional Fixed Complete Denture. Part 1. Planning and Surgical Phase. Int. J. Prosthodont. 2014, 27, 417–421. [Google Scholar] [CrossRef]
- Fueki, K.; Inamochi, Y.; Wada, J.; Arai, Y.; Takaichi, A.; Murakami, N.; Ueno, T.; Wakabayashi, N. A systematic review of digital removable partial dentures. Part I: Clinical evidence, digital impression, and maxillomandibular relationship record. J. Prosthodont. Res. 2022, 66, 40–52. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of Complete- and Partial-Arch Impressions of Actual Intraoral Scanning Systems In Vitro. 2019. Available online: https://www.zora.uzh.ch/id/eprint/180700 (accessed on 7 February 2023).
- Srinivasan, M.; Kamnoedboon, P.; McKenna, G.; Angst, L.; Schimmel, M.; Özcan, M.; Müller, F. CAD-CAM removable complete dentures: A systematic review and meta-analysis of trueness of fit, biocompatibility, mechanical properties, surface characteristics, color stability, time-cost analysis, clinical and patient-reported outcomes. J. Dent. 2021, 113, 103777. [Google Scholar] [CrossRef]
- Paulino, M.R.; Alves, L.R.; Gurgel, B.C.V.; Calderon, P.S. Simplified versus traditional techniques for complete denture fabrication: A systematic review. J. Prosthet. Dent. 2015, 113, 12–16. [Google Scholar] [CrossRef]
- Bidra, A.S.; Taylor, T.D.; Agar, J.R. Computer-aided technology for fabricating complete dentures: Systematic review of historical background, current status, and future perspectives. J. Prosthet. Dent. 2013, 109, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Kanazawa, M.; Iwaki, M.; Jokanovic, A.; Minakuchi, S. Effects of offset values for artificial teeth positions in CAD/CAM complete denture. Comput. Biol. Med. 2014, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Klaiber, D.; Spintzyk, S.; Geis-Gerstorfer, J.; Klink, A.; Unkovskiy, A.; Huettig, F. Bonding Behavior of Conventional PMMA towards Industrial CAD/CAM PMMA and Artificial Resin Teeth for Complete Denture Manufacturing in a Digital Workflow. Materials 2021, 14, 3822. [Google Scholar] [CrossRef] [PubMed]
- Kattadiyil, M.T.; Jekki, R.; Goodacre, C.J.; Baba, N.Z. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J. Prosthet. Dent. 2015, 114, 818–825. [Google Scholar] [CrossRef]
- Prpić, V.; Schauperl, Z.; Ćatić, A.; Dulčić, N.; Čimić, S. Comparison of Mechanical Properties of 3D-Printed, CAD/CAM, and Conventional Denture Base Materials. J. Prosthodont. 2020, 29, 524–528. [Google Scholar] [CrossRef]
- Mubaraki, M.Q.; Al Moaleem, M.M.; Alzahrani, A.H.; Shariff, M.; Alqahtani, S.M.; Porwal, A.; Al-Sanabani, F.A.; Bhandi, S.; Tribst, J.P.M.; Heboyan, A.; et al. Assessment of Conventionally and Digitally Fabricated Complete Dentures: A Comprehensive Review. Materials 2022, 15, 3868. [Google Scholar] [CrossRef]
- AlRumaih, H.S.; AlHelal, A.; Baba, N.Z.; Goodacre, C.J.; Al-Qahtani, A.; Kattadiyil, M.T. Effects of denture adhesive on the retention of milled and heat-activated maxillary denture bases: A clinical study. J. Prosthet. Dent. 2018, 120, 361–366. [Google Scholar] [CrossRef]
- Einarsdottir, E.R.; Geminiani, A.; Chochlidakis, K.; Feng, C.; Tsigarida, A.; Ercoli, C. Dimensional stability of double-processed complete denture bases fabricated with compression molding, injection molding, and CAD-CAM subtraction milling. J. Prosthet. Dent. 2020, 124, 116–121. [Google Scholar] [CrossRef]
- McLaughlin, J.B.; Ramos, V.; Dickinson, D.P. Comparison of Fit of Dentures Fabricated by Traditional Techniques Versus CAD/CAM Technology. J. Prosthodont. 2019, 28, 428–435. [Google Scholar] [CrossRef]
- Steinmassl, O.; Dumfahrt, H.; Grunert, I.; Steinmassl, P.A. CAD/CAM produces dentures with improved fit. Clin. Oral. Investig. 2018, 22, 2829–2835. [Google Scholar] [CrossRef]
- Tasaka, A.; Matsunaga, S.; Odaka, K.; Ishizaki, K.; Ueda, T.; Abe, S.; Yoshinari, M.; Yamashita, S.; Sakurai, K. Accuracy and retention of denture base fabricated by heat curing and additive manufacturing. J. Prosthodont. Res. 2019, 63, 85–89. [Google Scholar] [CrossRef]
- Hwang, H.J.; Lee, S.J.; Park, E.J.; Yoon, H.I. Assessment of the trueness and tissue surface adaptation of CAD-CAM maxillary denture bases manufactured using digital light processing. J. Prosthet. Dent. 2019, 121, 110–117. [Google Scholar] [CrossRef]
- Srinivasan, M.; Cantin, Y.; Mehl, A.; Gjengedal, H.; Müller, F.; Schimmel, M. CAD/CAM milled removable complete dentures: An in vitro evaluation of trueness. Clin. Oral. Investig. 2017, 21, 2007–2019. [Google Scholar] [CrossRef]
- Steinmassl, P.A.; Wiedemair, V.; Huck, C.; Klaunzer, F.; Steinmassl, O.; Grunert, I.; Dumfahrt, H. Do CAD/CAM dentures really release less monomer than conventional dentures? Clin. Oral. Investig. 2017, 21, 1697–1705. [Google Scholar] [CrossRef]
- Lee, S.; Hong, S.J.; Paek, J.; Pae, A.; Kwon, K.R.; Noh, K. Comparing accuracy of denture bases fabricated by injection molding, CAD/CAM milling, and rapid prototyping method. J. Adv. Prosthodont. 2019, 11, 55. [Google Scholar] [CrossRef]
- Wemken, G.; Spies, B.C.; Pieralli, S.; Adali, U.; Beuer, F.; Wesemann, C. Do hydrothermal aging and microwave sterilization affect the trueness of milled, additive manufactured and injection molded denture bases? J. Mech. Behav. Biomed. Mater. 2020, 111, 103975. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Yang, T.C.; Wang, T.M.; Lin, L.D. Effects of fabrication techniques on denture base adaptation: An in vitro study. J. Prosthet. Dent. 2020, 124, 740–747. [Google Scholar] [CrossRef]
- Quaas, S.; Rudolph, H.; Luthardt, R.G. Direct mechanical data acquisition of dental impressions for the manufacturing of CAD/CAM restorations. J. Dent. 2007, 35, 903–908. [Google Scholar] [CrossRef]
- Al-Dwairi, Z.N.; Tahboub, K.Y.; Baba, N.Z.; Goodacre, C.J. A Comparison of the Flexural and Impact Strengths and Flexural Modulus of CAD/CAM and Conventional Heat-Cured Polymethyl Methacrylate (PMMA). J. Prosthodont. 2020, 29, 341–349. [Google Scholar] [CrossRef]
- Perea-Lowery, L.; Minja, I.K.; Lassila, L.; Ramakrishnaiah, R.; Vallittu, P.K. Assessment of CAD-CAM polymers for digitally fabricated complete dentures. J. Prosthet. Dent. 2021, 125, 175–181. [Google Scholar] [CrossRef]
- Al-Dwairi, Z.N.; Tahboub, K.Y.; Baba, N.Z.; Goodacre, C.J.; Özcan, M. A Comparison of the Surface Properties of CAD/CAM and Conventional Polymethylmethacrylate (PMMA). J. Prosthodont. 2019, 28, 452–457. [Google Scholar] [CrossRef]
- Alp, G.; Murat, S.; Yilmaz, B. Comparison of Flexural Strength of Different CAD/CAM PMMA-Based Polymers: Comparison of Flexural Strength of Interim Resin Materials. J. Prosthodont. 2019, 28, e491–e495. [Google Scholar] [CrossRef]
- Becerra, J.; Mainjot, A.; Hüe, O.; Sadoun, M.; Nguyen, J. Influence of High-Pressure Polymerization on Mechanical Properties of Denture Base Resins. J. Prosthodont. 2021, 30, 128–134. [Google Scholar] [CrossRef]
- Iwaki, M.; Kanazawa, M.; Arakida, T.; Minakuchi, S. Mechanical properties of a polymethyl methacrylate block for CAD/CAM dentures. J. Oral. Sci. 2020, 62, 420–422. [Google Scholar] [CrossRef]
- Angelara, K.; Bratos, M.; Sorensen, J.A. Comparison of strength of milled and conventionally processed PMMA complete-arch implant-supported immediate interim fixed dental prostheses. J. Prosthet. Dent. 2023, 129, 221–227. [Google Scholar] [CrossRef]
- Choi, J.J.E.; Uy, C.E.; Plaksina, P.; Ramani, R.S.; Ganjigatti, R.; Waddell, J.N. Bond Strength of Denture Teeth to Heat-Cured, CAD/CAM and 3D Printed Denture Acrylics. J. Prosthodont. 2020, 29, 415–421. [Google Scholar] [CrossRef]
- Chang, Y.H.; Lee, C.Y.; Hsu, M.S.; Du, J.K.; Chen, K.K.; Wu, J.H. Effect of toothbrush/dentifrice abrasion on weight variation, surface roughness, surface morphology and hardness of conventional and CAD/CAM denture base materials. Dent. Mater. J. 2021, 40, 220–227. [Google Scholar] [CrossRef]
- Murat, S.; Alp, G.; Alatalı, C.; Uzun, M. In Vitro Evaluation of Adhesion of Candida albicans on CAD/CAM PMMA-Based Polymers: Adhesion of C. albicans on CAD/CAM PMMA-Based Polymers. J. Prosthodont. 2019, 28, e873–e879. [Google Scholar] [CrossRef]
- Al-Fouzan, A.F.; Al-mejrad, L.A.; Albarrag, A.M. Adherence of Candida to complete denture surfaces in vitro: A comparison of conventional and CAD/CAM complete dentures. J. Adv. Prosthodont. 2017, 9, 402. [Google Scholar] [CrossRef]
- Engler, M.L.P.D.; Güth, J.F.; Keul, C.; Erdelt, K.; Edelhoff, D.; Liebermann, A. Residual monomer elution from different conventional and CAD/CAM dental polymers during artificial aging. Clin. Oral. Investig. 2020, 24, 277–284. [Google Scholar] [CrossRef]
- Dayan, C.; Celik Guven, M.; Gencel, B.; Bural, C. A Color Stability Comparison of Conventional and CAD/CAM Polymethyl Methacrylate Denture Base Materials. Acta Stomatol. Croat. 2019, 53, 158–167. [Google Scholar] [CrossRef]
- Gruber, S.; Kamnoedboon, P.; Özcan, M.; Srinivasan, M. CAD/CAM Complete Denture Resins: An In Vitro Evaluation of Color Stability. J. Prosthodont. 2021, 30, 430–439. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Articles published from 2012 onwards | Articles published before 2012, except for the Quaas study (2007), which was included due to its significance in the evolution of obtaining patient arch models through CAD/CAM |
| Articles available in full text Articles focused on human subjects or in vitro trial Systematic reviews and clinical trials were included Articles published in English | Articles whose content was not available Articles whose subject of study was animal species Other types of studies that were not clinical trials or systematic review Articles published in languages other than English Publications that did not align with the aim of the review |
| Author | Type of Study | Year | Studied Variable | Manufacturing Method | Sample Size | Conclusions |
|---|---|---|---|---|---|---|
| Tasaka et al. [42] | Clinical trial | 2019 | Fit and retention | Conventional method (flasking) | 1 | The prostheses manufactured using 3D printing demonstrated better fit and, therefore, better retention than conventional prostheses. |
| Digital method (3D printing) | 1 | |||||
| Hwang et al. [43] | Clinical trial | 2019 | Fit | Conventional method (flasking) | 10 | The adaptation to the tissues and fit was higher in the printed prostheses than in the other two groups studied. |
| Digital method (milling) | 10 | |||||
| Digital method (3D printing) | 10 | |||||
| Srinivasan et al. [44] | Clinical trial | 2017 | Fit | Conventional method (flasking) | 11 | Initially, all three techniques demonstrated acceptable fit, and there were no significant differences between them. However, after hydrating the prostheses with saliva, the fit of the prostheses fabricated using conventional flasking improved significantly. |
| Conventional method (resin injection) | 11 | |||||
| Digital method (milling) | 11 | |||||
| Steinmassl et al. [45] | Clinical trial | 2018 | Fit | Conventional method (flasking) | 5 | The digital prostheses exhibit better fit than conventional prostheses. |
| Digital method (milling) | 20 | |||||
| Lee et al. [46] | Clinical trial | 2019 | Fit | Conventional method (resin injection) | 10 | The prostheses fabricated via 3D printing exhibited better fit than the milled and conventional prostheses. |
| Digital method (milling) | 10 | |||||
| Digital method (3D printing) | 10 | |||||
| Faty et al. [7] | Clinical trial | 2021 | Fit and retention | Conventional method | 24 | The milled prostheses demonstrated better fit and retention than the other two groups. The printed prostheses showed better fit but similar retention to the conventional prostheses. |
| Digital method (milling) | 24 | |||||
| Digital method (3D printing) | 24 | |||||
| Goodacre et al. [26] | Clinical trial | 2016 | Fit | Conventional method (flasking) | 10 | The digital prostheses showed greater adaptation to the supporting tissues than any of the conventional methods. |
| Conventional method (resin injection) | 10 | |||||
| Conventional method (self-curing resin) | 10 | |||||
| Digital method (milling) | 10 | |||||
| McLaughlin et al. [40] | Clinical trial | 2019 | Fit | Conventional method (flasking) | 27 | The conventional prostheses fabricated using flasking exhibited a significantly lower fit than the other two groups. |
| Conventional method (resin injection) | 27 | |||||
| Digital method (milling) | 27 | |||||
| AlHelal et al. [25] | Clinical trial | 2017 | Retention | Conventional method (flasking) | 20 | The retention of digital prostheses was significantly higher than that of conventional prostheses. |
| Digital method (milling) | 20 | |||||
| Einarsdottir et al. [39] | Clinical trial | 2020 | Dimensional stability | Conventional method (resin injection) | 15 | Conventional prostheses have lower dimensional stability than the digitally milled prostheses. |
| Digital method (milling) | 15 | |||||
| Wemken et al. [47] | Clinical trial | 2020 | Dimensional stability | Conventional method (resin injection) | 16 | The milled prostheses demonstrated the highest dimensional stability, followed by the conventional prostheses, and finally, the printed prostheses. |
| Digital method (milling) | 16 | |||||
| Digital method (3D printing) | 16 | |||||
| AlRumaih et al. [38] | Clinical trial | 2018 | Retention | Conventional method (flasking) | 20 | The milled prostheses showed higher retention than the conventional prostheses. |
| Digital method (milling) | 20 | |||||
| Hsu et al. [48] | Clinical trial | 2020 | Fit | Conventional method (flasking) | 10 | Both the conventional and milled prostheses exhibited better fit than the printed prostheses, with the milled prostheses demonstrating the best adaptation to the supporting tissues. |
| Conventional method (resin injection) | 10 | |||||
| Digital method (milling) | 20 | |||||
| Digital method (3D printing) | 20 |
| Author | Type of Study | Year | Studied Variable | Manufacturing Method | Sample Size | Conclusions |
|---|---|---|---|---|---|---|
| Al-Dwairi et al. [50] | Clinical trial | 2020 | Flexural strength | Conventional method (flasking) | 15 | The flexural strength (rigidity) is higher in the digital prostheses |
| Digital method (milling) | 30 | |||||
| Al-Dwairi et al. [52] | Clinical trial | 2019 | Superficial hardness | Conventional method (flasking) | 15 | The surface hardness is higher in the digital prostheses than in the conventional prostheses |
| Digital method (milling) | 30 | |||||
| Perea-Lowery et al. [51] | Clinical trial | 2021 | Flexural strength | Conventional method (flasking) | 8 | Digital prostheses exhibit higher flexural strength than conventional prostheses, although the differences found were not significant |
| Conventional method (self-curing resin) | 8 | |||||
| Digital method (milling) | 24 | |||||
| Srinivasan et al. [30] | Clinical trail | 2021 | Modulus of elasticity and superficial hardness | Digital method (milling) | 10 | The milled prostheses showed higher surface hardness, higher modulus of elasticity and greater force absorption capacity than the printed prostheses |
| Digital method (3D printing) | 20 | |||||
| Alp et al. [53] | Clinical trial | 2019 | Flexural strength | Conventional method (flasking) | 15 | Digital prostheses exhibited greater flexural strength than conventional prostheses |
| Conventional method (self-curing resin) | 15 | |||||
| Digital method (milling) | 45 | |||||
| Arslan et al. [16] | Clinical trial | 2018 | Flexural strength | Conventional method (flasking) | 10 | The digital prostheses exhibited greater flexural strength than the conventional prostheses |
| Digital method (milling) | 30 | |||||
| Prpić et al. [36] | Clinical trial | 2020 | Flexural strength and superficial hardness | Conventional method (flasking) | 160 | The flexural strength is higher in the milled prostheses, as well as the hardness (with non-significant differences) |
| Digital method (milling) | 160 | |||||
| Digital method (3D printing) | 160 | |||||
| Digital method (milling) | 30 | |||||
| Becerra et al. [54] | Clinical trial | 2021 | Modulus of elasticity and mechanical strength | Conventional method (flasking) | 30 | The digital prostheses demonstrated higher mechanical strength and a lower modulus of elasticity compared to the conventional prostheses |
| Conventional method (resin injection) | 30 | |||||
| Digital method (milling) | 30 | |||||
| Iwaki et al. [55] | Clinical trial | 2020 | Modulus of elasticity | Conventional method (flasking) | 5 | The digital prostheses exhibited a higher modulus of elasticity than the conventional prostheses |
| Digital method (milling) | 5 | |||||
| Angelara et al. [56] | Clinical trial | 2023 | Flexural strength | Conventional method | 20 | The digital prostheses have greater flexural strength than the conventional prostheses |
| Digital method (milling) | 40 |
| Author | Type of Study | Year | Studied Variable | Manufacturing Method | Sample Size | Conclusions |
|---|---|---|---|---|---|---|
| Al-Dwairi et al. [52] | Clinical trial | 2019 | Surface roughness | Conventional method (flasking) | 15 | The surface roughness is higher in conventional prostheses than in digital prostheses |
| Digital method (milling) | 30 | |||||
| Srinivasan et al. [18] | Clinical trial | 2021 | Surface roughness | Digital method (milling) | 10 | Both types of prostheses exhibit similar surface roughness, although prostheses printed with resins not recommended by the manufacturer may result in rougher surfaces |
| Digital method (3D printing) | 20 | |||||
| Chang et al. [58] | Clinical trial | 2021 | Surface roughness | Conventional method (self-curing resins) | 10 | The digital prostheses showed lower surface roughness than the prostheses made with self-curing resins |
| Digital method (milling) | 5 | |||||
| Arslan et al. [16] | Clinical trial | 2018 | Surface roughness | Conventional method (flasking) | 10 | Conventional prostheses have higher surface roughness than digital prostheses, but the differences are not significant |
| Digital method (milling) | 30 | |||||
| Murat et al. [59] | Clinical trial | 2019 | Surface roughness | Conventional method (flasking) | 10 | The digital prostheses exhibited lower surface roughness than the conventional prostheses |
| Digital method (milling) | 30 | |||||
| Klaiber et al. [34] | Clinical trial | 2021 | Surface roughness | Conventional method | 60 | The conventional prostheses have higher surface roughness than the digital prostheses |
| Digital method (milling) | 60 | |||||
| Al-Fouzan et al. [60] | Clinical trial | 2017 | Surface roughness | Conventional method (flasking) | 10 | The surface roughness in conventional prostheses was significantly higher than in digital prostheses |
| Digital method (milling) | 10 |
| Author | Type of Study | Year | Studied Variable | Manufacturing Method | Sample Size | Conclusions |
|---|---|---|---|---|---|---|
| Al-Fouzan et al. [60] | Clinical trial | 2017 | Microbial adhesion | Conventional method (flasking) | 10 | The digital prostheses exhibited lower superficial adhesion of Candida albicans compared to conventional prostheses |
| Digital method (milling) | 10 | |||||
| Murat et al. [59] | Clinical trial | 2019 | Microbial adhesion | Conventional method (flasking) | 10 | Candida albicans adhesion was significantly higher in conventional prostheses compared to digital prostheses |
| Digital method (milling) | 30 | |||||
| Srinivasan et al. [18] | Clinical trial | 2021 | Biocompatibility | Digital method (milling) | 18 | Both methods demonstrated good compatibility with oral tissues, with no significant differences observed between them |
| Digital method (3D printing) | 18 | |||||
| Engler et al. [61] | Clinical trial | 2020 | Release of residual monomer | Conventional method (flasking) | 40 | The monomer release depends on the material used, remaining more stable over time in the case of material used in the fabrication of conventional prostheses |
| Digital method (milling) | 320 | |||||
| Ayman et al. [17] | Clinical trial | 2017 | Release of residual monomer | Conventional method (flasking) | 15 | The resins used for milling digital prostheses have a lower content of free monomers compared to thermopolymerizable resins |
| Digital method (milling) | 15 | |||||
| Steinmassl et al. [45] | Clinical trial | 2017 | Release of residual monomer | Conventional method (flasking) | 10 | Conventional prostheses exhibited a slightly higher monomer release compared to digital prostheses, but the difference was not significant |
| Digital method (milling) | 40 |
| Author | Type of Study | Year | Studied Variable | Manufacturing Method | Sample Size | Conclusions |
|---|---|---|---|---|---|---|
| Dayan et al. [62] | Clinical trial | 2019 | Color stability | Conventional method (thermopolymerizable, photocurable, and self-curing resins) | 45 | The color stability in the resins used for milling prostheses is superior to any other type of resins. |
| Digital method (milling) | 15 | |||||
| Gruber et al. [63] | Clinical trial | 2021 | Color stability | Conventional method (flasking) | 8 | There were no differences in color stability between conventional resins and those used in milling. However, the 3D printing resins showed significant changes in coloration compared to the other two groups. |
| Digital method (milling) | 28 | |||||
| Digital method (3D printing) | 8 | |||||
| Alp et al. [53] | Clinical trial | 2019 | Color stability | Conventional method (flasking) | 6 | The color changes (due to coffee exposure) were imperceptible in all groups. |
| Digital method (milling) | 18 | |||||
| Iwaki et al. [55] | Clinical trial | 2020 | Color stability | Conventional method (flasking) | 3 | The milled prostheses exhibited greater color stability than the conventional prostheses. |
| Digital method (milling) | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dib Zakkour, S.; Dib Zakkour, J.; Guadilla, Y.; Montero, J.; Dib, A. Comparative Evaluation of the Digital Workflow and Conventional Method in Manufacturing Complete Removal Prostheses. Materials 2023, 16, 6955. https://doi.org/10.3390/ma16216955
Dib Zakkour S, Dib Zakkour J, Guadilla Y, Montero J, Dib A. Comparative Evaluation of the Digital Workflow and Conventional Method in Manufacturing Complete Removal Prostheses. Materials. 2023; 16(21):6955. https://doi.org/10.3390/ma16216955
Chicago/Turabian StyleDib Zakkour, Sara, Juan Dib Zakkour, Yasmina Guadilla, Javier Montero, and Abraham Dib. 2023. "Comparative Evaluation of the Digital Workflow and Conventional Method in Manufacturing Complete Removal Prostheses" Materials 16, no. 21: 6955. https://doi.org/10.3390/ma16216955
APA StyleDib Zakkour, S., Dib Zakkour, J., Guadilla, Y., Montero, J., & Dib, A. (2023). Comparative Evaluation of the Digital Workflow and Conventional Method in Manufacturing Complete Removal Prostheses. Materials, 16(21), 6955. https://doi.org/10.3390/ma16216955