
Additive Manufacturing of an Extended-Release Tablet of Tacrolimus

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
2.1. Materials
2.2. Tablet Design and Filament Preparation
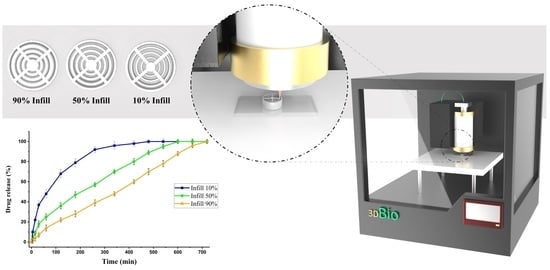
2.3. Preparation of 3D-Printed Tablets
2.4. Morphology of Filament and Tablets
2.5. Fourier-Transform Infrared Spectroscopy (FTIR)
2.6. Differential Scanning Calirometry (DSC) and Thermogravimetric Analysis (TGA)
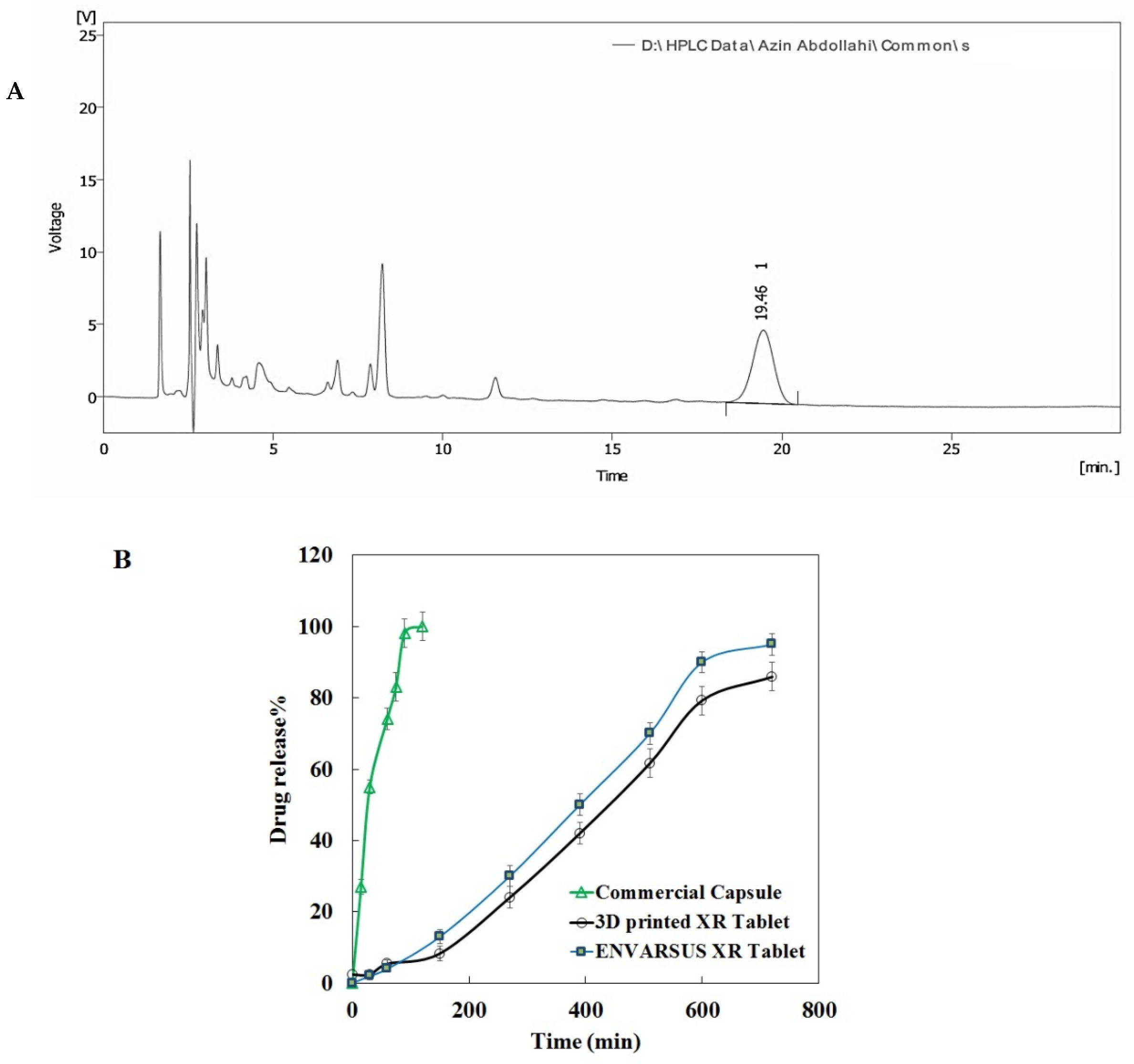
2.7. Assay, Content Uniformity, and Dissolution Studies
2.8. Hardness and Friability Measurement
2.9. Microbial Tests
2.10. Stability Study
3. Results
3.1. Results of Filaments Formulation and 3D Printing Process
3.2. Results of SEM Analysis
3.3. Results of FTIR Analysis
3.4. Results of DSC Thermal Analysis
3.5. Results of TGA Thermal Analysis
3.6. Results of Drug-Release Profiles, Assay, and Content Uniformity
3.7. Results of Microbial Tests
3.8. Results of Stability Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: http://www.transplant-observatory.org/2020-international-activities-report (accessed on 31 August 2022).
- Starzl, T.E. History of clinical transplantation. World J. Surg. 2000, 24, 759–782. [Google Scholar] [CrossRef]
- Van Sandwijk, M.; Bemelman, F.; Ten Berge, I. Immunosuppressive drugs after solid organ transplantation. Neth. J. Med. 2013, 71, 281–289. [Google Scholar] [PubMed]
- Kino, T.; Hatanaka, H.; Miyata, S.; Inamura, N.; Nishiyama, M.; Yajima, T.; Goto, T.; Okuhara, M.; Kohsaka, M.; Aoki, H.; et al. FK-506, a novel immunosuppressant isolated from a streptomyces II. Immunosuppressive effect of FK-506 in vitro. J. Antibiot. 1987, 40, 1256–1265. [Google Scholar] [CrossRef]
- Abou-Jaoude, M.; Najm, R.; Shaheen, J.; Nawfal, N.; Abboud, S.; AlHabash, M.; Darwish, M.; Mulhem, A.; Ojjeh, A.; Almawi, W. Tacrolimus (FK506) Versus Cyclosporine Microemulsion (Neoral) as Maintenance Immunosuppression Therapy in Kidney Transplant Recipients. Transplant. Proc. 2005, 37, 3025–3028. [Google Scholar] [CrossRef] [PubMed]
- Fung, J.J. Tacrolimus and transplantation: A decade in review. Transplantation 2004, 77, S41–S43. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Farmer, J.D., Jr.; Lane, W.S.; Friedman, J.; Weissman, I.; Schreiber, S.L. Calcineurin is a common target of cyclophilin-cyclosporin A and FKBP-FK506 complexes. Cell 1991, 66, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Levandoski, K.A.; Girardi, N.A.; Loss, M.J. Eruptive sebaceous hyperplasia as a side effect of oral tacrolimus in a renal transplant recipient. Dermatol. Online J. 2017, 23, 13030. [Google Scholar] [CrossRef]
- Zhang, R.; He, R.; Qian, J.; Guo, J.; Xue, K.; Yuan, Y.-F. Treatment of Experimental Autoimmune Uveoretinitis with Intravitreal Injection of Tacrolimus (FK506) Encapsulated in Liposomes. Investig. Opthalmol. Vis. Sci. 2010, 51, 3575–3582. [Google Scholar] [CrossRef]
- Tajdaran, K.; Shoichet, M.S.; Gordon, T.; Borschel, G.H. A novel polymeric drug delivery system for localized and sustained release of tacrolimus (FK506). Biotechnol. Bioeng. 2015, 112, 1948–1953. [Google Scholar] [CrossRef]
- Nabavi, M.H.; Salehi, M.; Ehterami, A.; Bastami, F.; Semyari, H.; Tehranchi, M.; Semyari, H. A collagen-based hydrogel containing tacrolimus for bone tissue engineering. Drug Deliv. Transl. Res. 2019, 10, 108–121. [Google Scholar] [CrossRef]
- Gultepe, E.; Nagesha, D.; Sridhar, S.; Amiji, M. Nanoporous inorganic membranes or coatings for sustained drug delivery in mplantable devices. Adv. Drug Deliv. Rev. 2010, 62, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Dheer, D.; Gupta, P.N.; Shankar, R. Tacrolimus: An updated review on delivering strategies for multifarious diseases. Eur. J. Pharm. Sci. 2018, 114, 217–227. [Google Scholar] [CrossRef]
- Kjar, A.; Huang, Y. Application of Micro-Scale 3D Printing in Pharmaceutics. Pharmaceutics 2019, 11, 390. [Google Scholar] [CrossRef] [PubMed]
- Lancia, P.; Jacqz-Aigrain, E.; Zhao, W. Choosing the right dose of tacrolimus. Arch. Dis. Child. 2014, 100, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Acosta-Vélez, G.F.; Wu, B. 3D pharming: Direct printing of personalized pharmaceutical tablets. Polym. Sci. 2016, 2, 11. [Google Scholar]
- Kotta, S.; Nair, A.; Alsabeelah, N. 3D Printing Technology in Drug Delivery: Recent Progress and Application. Curr. Pharm. Des. 2019, 24, 5039–5048. [Google Scholar] [CrossRef]
- West, T.G.; Bradbury, T.J. 3D Printing: A Case of ZipDose® Technology–World’s First 3D Printing Platform to Obtain FDA Approval for a Pharmaceutical Product. In 3D and 4D Printing in Biomedical Applications: Process Engineering and Additive Manufacturing; Wiley: Hoboken, NJ, USA, 2019; pp. 53–79. [Google Scholar]
- Mohammed, A.; Elshaer, A.; Sareh, P.; Elsayed, M.; Hassanin, H. Additive manufacturing technologies for drug delivery applications. Int. J. Pharmaceut. 2020, 580, 119245. [Google Scholar] [CrossRef]
- Sarode, A.L.; Obara, S.; Tanno, F.K.; Sandhu, H.; Iyer, R.; Shah, N. Stability assessment of hypromellose acetate succinate (HPMCAS) NF for application in hot melt extrusion (HME). Carbohydr. Polym. 2014, 101, 146–153. [Google Scholar] [CrossRef]
- Xu, X.; Zhao, J.; Wang, M.; Wang, L.; Yang, J. 3D Printed Polyvinyl Alcohol Tablets with Multiple Release Profiles. Sci. Rep. 2019, 9, 1–8. [Google Scholar] [CrossRef]
- Pereira, G.G.; Figueiredo, S.; Fernandes, A.I.; Pinto, J.F. Polymer Selection for Hot-Melt Extrusion Coupled to Fused Deposition Modelling in Pharmaceutics. Pharmaceutics 2020, 12, 795. [Google Scholar] [CrossRef]
- Nautyal, U.; Gupta, D. Oral Sustained Release Tablets: An Overview with A Special Emphasis on Matrix Tablet. Int. J. Health Biol. Sci. 2020, 3, 6–13. [Google Scholar]
- De Jaeghere, W.; De Beer, T.; Van Bocxlaer, J.; Remon, J.; Vervaet, C. Hot-melt extrusion of polyvinyl alcohol for oral immediate release applications. Int. J. Pharm. 2015, 492, 1–9. [Google Scholar] [CrossRef]
- Ponnammal, P.; Kanaujia, P.; Yani, Y.; Ng, W.K.; Tan, R.B.H. Orally Disintegrating Tablets Containing Melt Extruded Amorphous Solid Dispersion of Tacrolimus for Dissolution Enhancement. Pharmaceutics 2018, 10, 35. [Google Scholar] [CrossRef]
- Patel, N.; Cook, A.; Greenhalgh, E.; Rech, M.A.; Rusinak, J.; Heinrich, L. Overview of extended release tacrolimus in solid organ transplantation. World J. Transplant. 2016, 6, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Liu, L.; Li, X.; Ma, J.; Liu, R.; Wang, S. Extended tacrolimus release via the combination of lipid-based solid dispersion and HPMC hydrogel matrix tablets. Asian J. Pharm. Sci. 2019, 14, 445–454. [Google Scholar] [CrossRef]
- Seoane-Viaño, I.; Ong, J.J.; Luzardo-Álvarez, A.; González-Barcia, M.; Basit, A.W.; Otero-Espinar, F.J.; Goyanes, A. 3D printed tacrolimus suppositories for the treatment of ulcerative colitis. Asian J. Pharm. Sci. 2020, 16, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Brunet, M.; van Gelder, T.; Asberg, A.; Haufroid, V.; Hesselink, D.A.; Langman, L.; Lemaitre, F.; Marquet, P.; Seger, C.; Shipkova, M.; et al. Therapeutic Drug Monitoring of Tacrolimus-Personalized Therapy: Second Consensus Report. Ther. Drug Monit. 2019, 41, 261–307. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation * | F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F8 | F9 |
|---|---|---|---|---|---|---|---|---|---|---|
| PVA filament | 7950 | 7800 | 6900 | 6000 | 6900 | 6000 | 7350 | 6900 | 6900 | 6000 |
| Sorbitol | 0 | 0 | 0 | 0 | 0 | 0 | 450 | 900 | 900 | 1800 |
| PEG 10,000 | 0 | 0 | 900 | 1800 | 0 | 0 | 0 | 0 | 0 | 0 |
| PEG 35,000 | 0 | 0 | 0 | 0 | 900 | 1800 | 0 | 0 | 0 | 0 |
| Mg Stearate | 0 | 150 | 150 | 150 | 150 | 150 | 150 | 150 | 150 | 150 |
| Temperature (°C) | >225 | >225 | >220 | × | × | × | 195 | 185 | 185 | 150 |
| Printability | ✓ | ✓✓ | × | × | × | × | ✓✓✓ | ✓✓✓✓ | ✓✓✓✓ | ✓✓✓✓✓ |
| Extrudability | ✓ | ✓ | × | × | × | × | ✓ | ✓ | ✓ | ✓ |
| Stability Specification | ||||||
|---|---|---|---|---|---|---|
| Row | Test Item | Time (Month) | 0 | 1 | 3 | 6 |
| Standard | ||||||
| 1 | Appearance | Yellowish Round Tablet | Complies | Complies | Complies | Complies |
| 2 | Hardness | Above 50 kg | Complies | Complies | Complies | Complies |
| 3 | Friability | Less Than 1% | Complies | Complies | Complies | Complies |
| 4 | Assay | 93.0–105.0% | 98.9 | 90.01 | 98.6 | 98.21 |
| 5 | Total microbial count | Less Than 1000 Cfu/g | Less Than 10 | Less Than 10 | Less Than 10 | Less Than 10 |
| Mold/Yeast count | Less Than 100 Cfu/g | Less Than 10 | Less Than 10 | Less Than 10 | Less Than 10 | |
| E. coli | Negative | Negative | Negative | Negative | Negative | |
| Salmonella species | Negative | Negative | Negative | Negative | Negative | |
| Pseudomonas aeroginosa | Negative | Negative | Negative | Negative | Negative | |
| Staphylococcus aureous | Negative | Negative | Negative | Negative | Negative | |
| Candida albicans | Negative | Negative | Negative | Negative | Negative | |
| Aspergillus niger | Negative | Negative | Negative | Negative | Negative | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdollahi, A.; Ansari, Z.; Akrami, M.; Haririan, I.; Dashti-Khavidaki, S.; Irani, M.; Kamankesh, M.; Ghobadi, E. Additive Manufacturing of an Extended-Release Tablet of Tacrolimus. Materials 2023, 16, 4927. https://doi.org/10.3390/ma16144927
Abdollahi A, Ansari Z, Akrami M, Haririan I, Dashti-Khavidaki S, Irani M, Kamankesh M, Ghobadi E. Additive Manufacturing of an Extended-Release Tablet of Tacrolimus. Materials. 2023; 16(14):4927. https://doi.org/10.3390/ma16144927
Chicago/Turabian StyleAbdollahi, Azin, Zahra Ansari, Mohammad Akrami, Ismaeil Haririan, Simin Dashti-Khavidaki, Mohammad Irani, Mojtaba Kamankesh, and Emad Ghobadi. 2023. "Additive Manufacturing of an Extended-Release Tablet of Tacrolimus" Materials 16, no. 14: 4927. https://doi.org/10.3390/ma16144927
APA StyleAbdollahi, A., Ansari, Z., Akrami, M., Haririan, I., Dashti-Khavidaki, S., Irani, M., Kamankesh, M., & Ghobadi, E. (2023). Additive Manufacturing of an Extended-Release Tablet of Tacrolimus. Materials, 16(14), 4927. https://doi.org/10.3390/ma16144927