
Overview of the Effect of Different Regenerative Materials in Class II Furcation Defects in Periodontal Patients




Abstract
:1. Introduction
- Biocompatibility to allow integration with the host tissues without eliciting inflammatory responses.
- Proper degradation profile to match with the new tissue formation.
- Adequate mechanical and physical properties to allow its placement in vivo.
- Sufficient sustained strength to avoid membrane collapse and perform their barrier function [18].
- Non-absorbable barriers
- Absorbable barriers
- They contain bone-forming cells (osteogenesis).
- They function as a scaffold for bone formation (osteoconduction).
- They contain biological substances in their matrix that induce bone formation (osteoinduction).
- Autogenous: Grafts obtained by the patient, harvested both from intraoral and extraoral sites, consisting of cortical bone or cancellous bone and marrow.
- Allogeneic: Grafts of human origin. Three types of bone allografts are used in periodontics, namely, demineralized freeze-dried bone, non-demineralized freeze-dried bone and frozen iliac cancellous bone.
- Xenogeneic: Graft from a non-human donor, mainly from bovine or porcine origin.
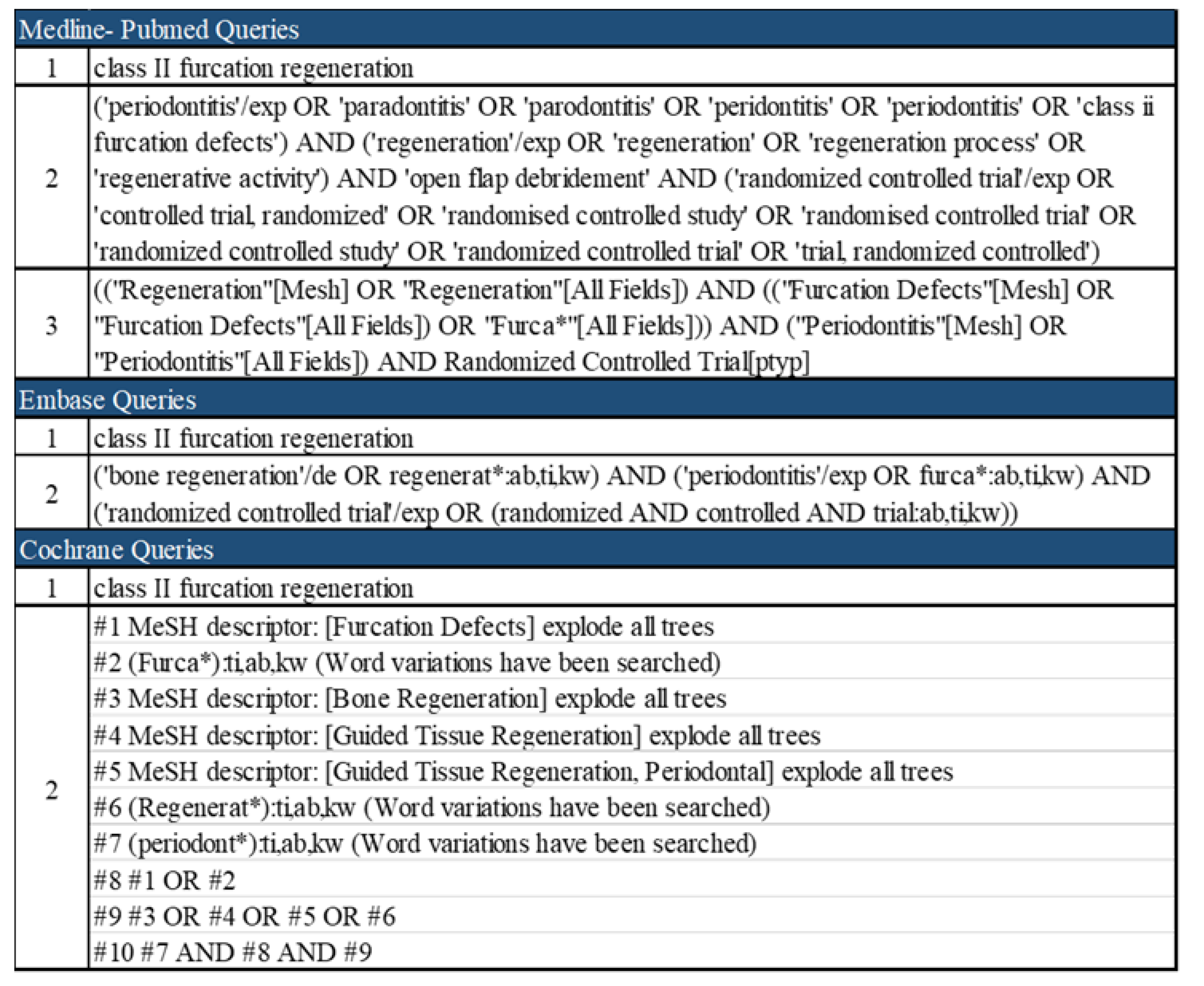
2. Materials and Methods
- −
- Randomized control trials (RCTs) in periodontitis patients with at least one class II furcation involvement were included. No distinction between maxillary and mandibular molars was considered.
- −
- Only RCTs that considered one or more of the above-mentioned treatment methods with open flap debridement (OFD) as control and a follow-up period of at least 6 months were included.
- −
- Studies published in English.
- −
- Systematic reviews and meta-analyses, case series or case reports, narrative revisions and RCTs without OFD as control group.
- −
- The measurements of the considered outcomes were performed solely during the surgical phase and not clinically prior to the surgery.
- −
- Histological analyses, in vitro studies and trials conducted on animals.
3. Results
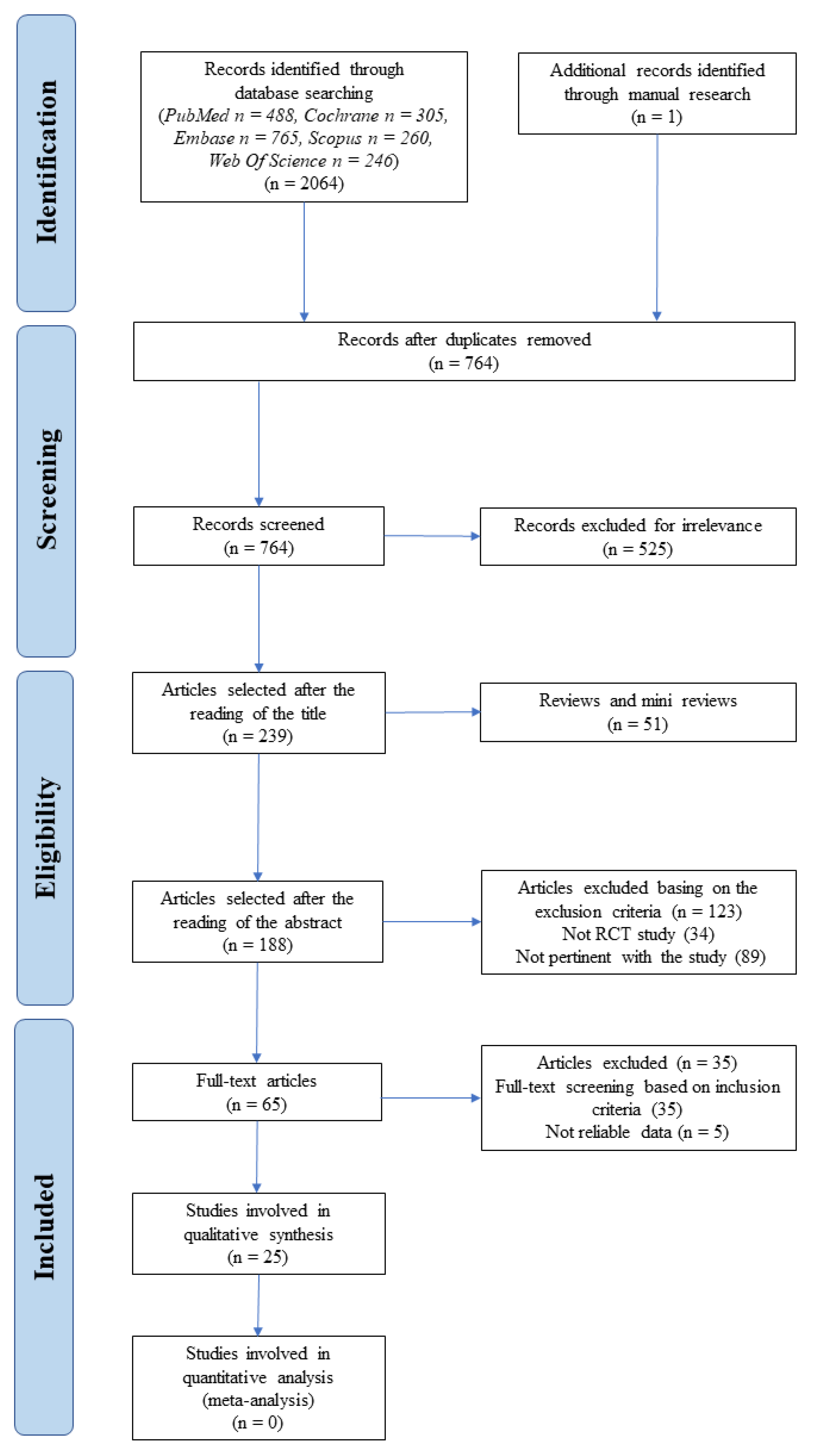
3.1. Study Selection
3.2. Risk of Bias across the Included Studies
3.3. Qualitative Synthesis
3.3.1. Non-Absorbable Membranes
3.3.2. Absorbable Membranes
3.3.3. Blood Derivatives
3.3.4. Miscellaneous Materials
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S162–S170. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Laine, M.L.; Crielaard, W.; Loos, B.G. Genetic susceptibility to periodontitis. Periodontology 2000 2012, 58, 37–68. [Google Scholar] [CrossRef] [PubMed]
- Lopez, R.; Hujoel, P.; Belibasakis, G.N. On putative periodontal pathogens: An epidemiological perspective. Virulence 2015, 6, 249–257. [Google Scholar] [CrossRef] [Green Version]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. (Qassim) 2017, 11, 72–80. [Google Scholar]
- Salvi, G.E.; Mischler, D.C.; Schmidlin, K.; Matuliene, G.; Pjetursson, B.E.; Brägger, U.; Lang, N.P. Risk factors associated with the longevity of multi-rooted teeth. Long-term outcomes after active and supportive periodontal therapy. J. Clin. Periodontol. 2014, 41, 701–707. [Google Scholar] [CrossRef]
- Swan, R.H.; Hurt, W.C. Cervical enamel projections as an etiologic factor in furcation involvement. J. Am. Dent. Assoc. 1976, 93, 342–345. [Google Scholar] [CrossRef]
- Vandersall, D.C. Pearls, grooves, and projections. J. Am. Dent. Assoc. 1979, 99, 794. [Google Scholar] [CrossRef]
- Hou, G.L.; Tsai, C.C. Cervical enamel projection and intermediate bifurcational ridge correlated with molar furcation involvements. J. Periodontol. 1997, 68, 687–693. [Google Scholar] [CrossRef]
- Loos, B.; Claffey, N.; Egelberg, J. Clinical and microbiological effects of root debridement in periodontal furcation pockets. J. Clin. Periodontol. 1988, 15, 453–463. [Google Scholar] [CrossRef]
- Kalkwarf, K.L.; Kaldahl, W.B.; Patil, K.D. Evaluation of furcation region response to periodontal therapy. J. Periodontol. 1988, 59, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Dannewitz, B.; Zeidler, A.; Husing, J.; Saure, D.; Pfefferle, T.; Eickholz, P.; Pretzl, B. Loss of molars in periodontally treated patients: Results 10 years and more after active periodontal therapy. J. Clin. Periodontol. 2016, 43, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Huynh-Ba, G.; Kuonen, P.; Hofer, D.; Schmid, J.; Lang, N.P.; Salvi, G.E. The effect of periodontal therapy on the survival rate and incidence of complications of multirooted teeth with furcation involvement after an observation period of at least 5 years: A systematic review. J. Clin. Periodontol. 2009, 36, 164–176. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Periodontology. Glossary of Periodontal Terms, 3rd ed.; American Academy of Periodontology: Chicago, IL, USA, 1992; p. 50. [Google Scholar]
- Melcher, A.H. On the repair potential of periodontal tissues. J. Periodontol. 1976, 47, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Nyman, S.; Gottlow, J.; Lindhe, J.; Karring, T.; Wennstrom, J. New attachment formation by guided tissue regeneration. J. Periodontal. Res. 1987, 22, 252–254. [Google Scholar] [CrossRef]
- Caton, J.G.; DeFuria, E.L.; Polson, A.M.; Nyman, S. Periodontal regeneration via selective cell repopulation. J. Periodontol. 1987, 58, 546–552. [Google Scholar] [CrossRef]
- Bottino, M.C.; Thomas, V.; Schmidt, G.; Vohra, Y.K.; Chu, T.M.; Kowolik, M.J.; Janowski, G.M. Recent advances in the development of GTR/GBR membranes for periodontal regeneration—A materials perspective. Dent. Mater. 2012, 28, 703–721. [Google Scholar] [CrossRef]
- Nyman, S.; Gottlow, J.; Karring, T.; Lindhe, J. The regenerative potential of the periodontal ligament. An experimental study in the monkey. J. Clin. Periodontol. 1982, 9, 257–265. [Google Scholar] [CrossRef]
- Tatakis, D.N.; Promsudthi, A.; Wikesjo, U.M. Devices for periodontal regeneration. Periodontology 2000 1999, 19, 59–73. [Google Scholar] [CrossRef]
- Lindhe, J.; Lang, N.P.; Berglundh, T.; Giannobile, W.V.; Sanz, M. Clinical Periodontology and Implant Dentistry, 6th ed.; John Wiley and Sons, Inc.: Chichester, UK; Ames, IA, USA, 2015; p. 1. [Google Scholar]
- Brunsvold, M.A.; Mellonig, J.T. Bone grafts and periodontal regeneration. Periodontology 2000 1993, 1, 80–91. [Google Scholar] [CrossRef]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G.; Nemcovsky, C.; Donos, N.; Lyngstadaas, S.P.; Deschner, J.; Dard, M.; et al. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Alessandri, R.; Miron, R.; Salvi, G.E.; Bosshardt, D.D. Enamel Matrix Proteins and Periodontal Wound Healing and Regeneration. Clin. Adv. Periodontics 2011, 1, 101–117. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, R.E.; Carlson, E.R.; Eichstaedt, R.M.; Schimmele, S.R.; Strauss, J.E.; Georgeff, K.R. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 638–646. [Google Scholar] [CrossRef]
- DeLong, J.M.; Russell, R.P.; Mazzocca, A.D. Platelet-rich plasma: The PAW classification system. Arthroscopy 2012, 28, 998–1009. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Ghanaati, S.; Booms, P.; Orlowska, A.; Kubesch, A.; Lorenz, J.; Rutkowski, J.; Landes, C.; Sader, R.; Kirkpatrick, C.; Choukroun, J. Advanced platelet-rich fibrin: A new concept for cell-based tissue engineering by means of inflammatory cells. J. Oral Implantol. 2014, 40, 679–689. [Google Scholar] [CrossRef]
- Kobayashi, E.; Fluckiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Jepsen, S.; Gennai, S.; Hirschfeld, J.; Kalemaj, Z.; Buti, J.; Graziani, F. Regenerative surgical treatment of furcation defects: A systematic review and Bayesian network meta-analysis of randomized clinical trials. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 352–374. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Caton, J.; Greenstein, G.; Zappa, U. Synthetic bioabsorbable barrier for regeneration in human periodontal defects. J. Periodontol. 1994, 65, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Dubrez, B.; Duroux, P.; Cimasoni, G. Bone density of class II furcation lesions treated by guided tissue regeneration. A follow-up study by digital analysis of superimposable radiographs. J. Clin. Periodontol. 1996, 23, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Lekovic, V.; Kenney, E.B.; Carranza, F.A.; Martignoni, M. The use of autogenous periosteal grafts as barriers for the treatment of Class II furcation involvements in lower molars. J. Periodontol. 1991, 62, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; O’Neal, R.B.; Thomas, C.L.; Shyr, Y.; MacNeil, R.L. Evaluation of an absorbable collagen membrane in treating Class II furcation defects. J. Periodontol. 1994, 65, 1029–1036. [Google Scholar] [CrossRef]
- Jaiswal, R.; Deo, V. Evaluation of the effectiveness of enamel matrix derivative, bone grafts, and membrane in the treatment of mandibular Class II furcation defects. Int. J. Periodontics Restor. Dent. 2013, 33, e58–e64. [Google Scholar] [CrossRef] [Green Version]
- Avera, J.B.; Camargo, P.M.; Klokkevold, P.R.; Kenney, E.B.; Lekovic, V. Guided tissue regeneration in Class II furcation involved maxillary molars: A controlled study of 8 split-mouth cases. J. Periodontol. 1998, 69, 1020–1026. [Google Scholar] [CrossRef]
- Metzler, D.G.; Seamons, B.C.; Mellonig, J.T.; Gher, M.E.; Gray, J.L. Clinical evaluation of guided tissue regeneration in the treatment of maxillary class II molar furcation invasions. J. Periodontol. 1991, 62, 353–360. [Google Scholar] [CrossRef]
- Mombelli, A.; Zappa, U.; Brägger, U.; Lang, N.P. Systemic antimicrobial treatment and guided tissue regeneration. Clinical and microbiological effects in furcation defects. J. Clin. Periodontol. 1996, 23, 386–396. [Google Scholar] [CrossRef]
- Pontoriero, R.; Lindhe, J.; Nyman, S.; Karring, T.; Rosenberg, E.; Sanavi, F. Guided tissue regeneration in degree II furcation-involved mandibular molars. A clinical study. J. Clin. Periodontol. 1988, 15, 247–254. [Google Scholar] [CrossRef]
- Pontoriero, R.; Lindhe, J. Guided tissue regeneration in the treatment of degree II furcations in maxillary molars. J. Clin. Periodontol. 1995, 22, 756–763. [Google Scholar] [CrossRef]
- Balusubramanya, K.V.; Ramya, R.; Govindaraj, S.J. Clinical and radiological evaluation of human osseous defects (mandibular grade ii furcation involvement) treated with bioresorbable membrane: Vicryl mesh. J. Contemp. Dent. Pract. 2012, 13, 806–811. [Google Scholar] [PubMed]
- Paul, B.F.; Mellonig, J.T.; Towle, H.J., 3rd; Gray, J.L. Use of a collagen barrier to enhance healing in human periodontal furcation defects. Int. J. Periodontics Restor. Dent 1992, 12, 123–131. [Google Scholar]
- Verma, V.; Saimbi, C.S.; Khan, M.A.; Goel, A. Use of periosteal membrane as a barrier membrane for the treatment of buccal Grade II furcation defects in lower molars: A novel technique. Indian J. Dent. Res. 2011, 22, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Yukna, C.N.; Yukna, R.A. Multi-center evaluation of bioabsorbable collagen membrane for guided tissue regeneration in human Class II furcations. J. Periodontol. 1996, 67, 650–657. [Google Scholar] [CrossRef]
- Agarwal, A.; Manjunath, R.G.S.; Sethi, P.; Shankar, G.S. Platelet-rich fibrin in combination with decalcified freeze-dried bone allograft for the management of mandibular degree II furcation defect: A randomised controlled clinical trial. Singapore Dent. J. 2020, 39, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, P.; Pradeep, A.R.; Agarwal, E.; Rao, N.S.; Naik, S.B.; Priyanka, N.; Kalra, N. Comparative evaluation of autologous platelet-rich fibrin and platelet-rich plasma in the treatment of mandibular degree II furcation defects: A randomized controlled clinical trial. J. Periodontal Res. 2013, 48, 573–581. [Google Scholar] [CrossRef]
- Kanoriya, D.; Pradeep, A.R.; Garg, V.; Singhal, S. Mandibular Degree II Furcation Defects Treatment With Platelet-Rich Fibrin and 1% Alendronate Gel Combination: A Randomized Controlled Clinical Trial. J. Periodontol. 2017, 88, 250–258. [Google Scholar] [CrossRef]
- Pradeep, A.R.; Pai, S.; Garg, G.; Devi, P.; Shetty, S.K. A randomized clinical trial of autologous platelet-rich plasma in the treatment of mandibular degree II furcation defects. J. Clin. Periodontol. 2009, 36, 581–588. [Google Scholar] [CrossRef]
- Sharma, A.; Pradeep, A.R. Autologous platelet-rich fibrin in the treatment of mandibular degree II furcation defects: A randomized clinical trial. J. Periodontol. 2011, 82, 1396–1403. [Google Scholar] [CrossRef]
- Siddiqui, Z.R.; Jhingran, R.; Bains, V.K.; Srivastava, R.; Madan, R.; Rizvi, I. Comparative evaluation of platelet-rich fibrin versus beta-tri-calcium phosphate in the treatment of Grade II mandibular furcation defects using cone-beam computed tomography. Eur. J. Dent. 2016, 10, 496–506. [Google Scholar] [CrossRef] [Green Version]
- Anderegg, C.R.; Alexander, D.C.; Freidman, M. A bioactive glass particulate in the treatment of molar furcation invasions. J. Periodontol. 1999, 70, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Chitsazi, M.T.; Mostofi Zadeh Farahani, R.; Pourabbas, M.; Bahaeddin, N. Efficacy of open flap debridement with and without enamel matrix derivatives in the treatment of mandibular degree II furcation involvement. Clin. Oral Investig. 2007, 11, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Eto, A.L.; Joly, J.C.; Jeffcoat, M.; de Araújo, N.S.; de Araújo, V.C.; Cury, P.R. Use of anorganic bovine-derived hydroxyapatite matrix/cell-binding peptide (P-15) in the treatment of class II furcation defects: A clinical and radiographic study in humans. J. Periodontol. 2007, 78, 2277–2283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houser, B.E.; Mellonig, J.T.; Brunsvold, M.A.; Cochran, D.L.; Meffert, R.M.; Alder, M.E. Clinical evaluation of anorganic bovine bone xenograft with a bioabsorbable collagen barrier in the treatment of molar furcation defects. Int. J. Periodontics Restor. Dent. 2001, 21, 161–169. [Google Scholar]
- Lekovic, V.; Camargo, P.M.; Weinlaender, M.; Vasilic, N.; Aleksic, Z.; Kenney, E.B. Effectiveness of a combination of platelet-rich plasma, bovine porous bone mineral and guided tissue regeneration in the treatment of mandibular grade II molar furcations in humans. J. Clin. Periodontol. 2003, 30, 746–751. [Google Scholar] [CrossRef]
- Mohamed, M.K. Clinical evaluation of combined porous hydroxyiapatite and platelet rich plasma in management of mandibular Class II furcation defects. J. Int. Oral Health 2016, 82, 172–176. [Google Scholar]
- Pradeep, A.R.; Karvekar, S.; Nagpal, K.; Patnaik, K.; Raju, A.; Singh, P. Rosuvastatin 1.2 mg In Situ Gel Combined With 1:1 Mixture of Autologous Platelet-Rich Fibrin and Porous Hydroxyapatite Bone Graft in Surgical Treatment of Mandibular Class II Furcation Defects: A Randomized Clinical Control Trial. J. Periodontol. 2016, 87, 5–13. [Google Scholar] [CrossRef]
- Santana, R.B.; de Mattos, C.M.; Van Dyke, T. Efficacy of combined regenerative treatments in human mandibular class II furcation defects. J. Periodontol. 2009, 80, 1756–1764. [Google Scholar] [CrossRef]
- Serroni, M.; Paolantonio, M.; Romano, L.; Santamaria, P.; Rexhepi, I.; Sinjari, B.; Paolantonio, G.; Secondi, L.; De Ninis, P.; Femminella, B. The added benefit of L-PRF to autogenous bone grafts in the treatment of degree II furcation involvement in mandibular molars. J. Periodontol. 2021. [Google Scholar] [CrossRef]
- Tsao, Y.P.; Neiva, R.; Al-Shammari, K.; Oh, T.J.; Wang, H.L. Effects of a mineralized human cancellous bone allograft in regeneration of mandibular Class II furcation defects. J. Periodontol. 2006, 77, 416–425. [Google Scholar] [CrossRef]
- Graziani, F.; Gennai, S.; Karapetsa, D.; Rosini, S.; Filice, N.; Gabriele, M.; Tonetti, M. Clinical performance of access flap in the treatment of class II furcation defects. A systematic review and meta-analysis of randomized clinical trials. J. Clin. Periodontol. 2015, 42, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Karanxha, L.; Goker, F.; Satpathy, A.; Taschieri, S.; Francetti, L.; Das, A.C.; Kumar, M.; Panda, S.; Fabbro, M.D. Autologous Platelet Concentrates in Treatment of Furcation Defects-A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soares, D.M.; de Melo, J.G.A.; Barboza, C.A.G.; Alves, R.V. The use of enamel matrix derivative in the treatment of class II furcation defects: Systematic review and meta-analysis. Aust. Dent. J. 2020, 65, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Swami, R.K.; Kolte, A.P.; Bodhare, G.H.; Kolte, R.A. Bone replacement grafts with guided tissue regeneration in treatment of grade II furcation defects: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 807–821. [Google Scholar] [CrossRef] [PubMed]
- Tarallo, F.; Mancini, L.; Pitzurra, L.; Bizzarro, S.; Tepedino, M.; Marchetti, E. Use of Platelet-Rich Fibrin in the Treatment of Grade 2 Furcation Defects: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2104. [Google Scholar] [CrossRef]
- Troiano, G.; Laino, L.; Dioguardi, M.; Giannatempo, G.; Lo Muzio, L.; Lo Russo, L. Mandibular Class II Furcation Defect Treatment: Effects of the Addition of Platelet Concentrates to Open Flap: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Periodontol. 2016, 87, 1030–1038. [Google Scholar] [CrossRef]
- Tavelli, L.; Ravidà, A.; Barootchi, S.; Chambrone, L.; Giannobile, W.V. Recombinant Human Platelet-Derived Growth Factor: A Systematic Review of Clinical Findings in Oral Regenerative Procedures. JDR Clin. Trans. Res. 2021, 6, 161–173. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Author (Year) | Random Allocation | Inclusion/Exclusion Criteria Clearly Defined | Blinding of Participants | Blinding of Examiners | Balanced Experimental Groups | Identical Treatment between the Groups | Reporting of Follow-Up | Total |
|---|---|---|---|---|---|---|---|---|
| Non-Resorbable Membranes | ||||||||
| Avera et al. (1998) | Y | Y | N | Unclear | Y | Y | Y | 5 of 7 |
| Metzler et al. (1991) | Y | N | N | N | Y | Y | Y | 4 of 7 |
| Mombelli et al. (1996) | Y | Y | Y | Y | Y | Y | Y | 7 of 7 |
| Pontoriero et al. (1988) | Y | Y | N | Unclear | Y | Y | Y | 5 of 7 |
| Pontoriero et al. (1995) | Y | N | N | N | Y | Y | Y | 4 of 7 |
| Absorbable Membranes | ||||||||
| Balusubramanya et al. (2012) | Y | Y | Unclear | Unclear | Y | Y | Y | 5 of 7 |
| Paul et al. (1992) | Y | N | N | N | Y | Y | Y | 5 of 7 |
| Verma et al. (2011) | Y | Y | Unclear | N | Y | Y | Y | 5 of 7 |
| Yukna et al. (1996) | Y | N | Unclear | Y | Y | Y | Y | 5 of 7 |
| Blood Derivates (PRP, PRF) | ||||||||
| Agarwal et al. (2020) | Y | Y | Unclear | Y | Y | Y | Y | 6 of 7 |
| Bajaj et al. (2013) | Y | Y | Y | Y | Y | Y | Y | 7 of 7 |
| Kanoriya et al. (2017) | Y | Y | Y | Y | Y | Y | Y | 7 of 7 |
| Pradeep et al. (2009) | Y | Y | Y | Y | Y | Y | Y | 7 of 7 |
| Sharma et al. (2011) | Y | Y | Y | Y | Y | Y | Y | 7 of 7 |
| Siddiqui et al. (2016) | Y | Y | Unclear | Unclear | Y | Y | Y | 5 of 7 |
| Miscellaneous Materials | ||||||||
| Anderegg et al. (1999) | Y | Unclear | Unclear | N | Y | Y | Y | 4 of 7 |
| Chitsazi et al. (2007) | Y | Y | Unclear | N | Y | Y | Y | 5 of 7 |
| Eto et al. (2007) | Y | Y | Unclear | Y | Y | Y | Y | 6 of 7 |
| Houser et al. (2001) | Y | Unclear | Unclear | Y | N | Y | Y | 4 of 7 |
| Lekovic et al. (2003) | Y | Y | Unclear | Y | Y | Y | Y | 6 of 7 |
| Mohamed et al. (2016) | N | Unclear | Unclear | N | Y | Y | Y | 3 of 7 |
| Pradeep et al. (2016) | Y | Y | Y | Y | Y | Y | Y | 7 of 7 |
| Santana et al. (2009) | Y | Y | Unclear | Y | Y | Y | Y | 6 of 7 |
| Serroni et al. (2021) | Y | Y | Unclear | Y | Y | Y | Y | 6 of 7 |
| Tsao et al. (2006) | Y | Y | Unclear | Y | Y | Y | Y | 6 of 7 |
| Author (Year) | Study Design | Age | Sex | Diagnosis of Periodontitis | Systemic Conditions | Medication | Smoking | Oral Hygiene |
|---|---|---|---|---|---|---|---|---|
| Non-Absorbable Membranes | ||||||||
| Mombelli et al. (1996) | split mouth | 35–65 | NR | moderate to advanced | NO | no antibiotics in the past 3 months | NR | NR |
| Pontoriero et al. (1988) | split mouth | 22–65 | NR | moderately advanced to advanced | NR | NR | NR | NR |
| Metzler et al. (1991) | split mouth | 29–64 | 13 M 4 F | moderate to advanced adult | NR | NR | NR | plaque score 10% or lower |
| Avera et al. (1998) | split mouth | mean age: 42 ± 6.5 | 3 M 5 F | NR | NO | NR | NR | plaque score 10% or lower |
| Pontoriero et al. (1995) | split mouth | 21–59 | NR | moderately advanced to advanced | NR | NR | NR | 0.4–0.7 plaque score |
| Absorbable Membranes | ||||||||
| Balusubramanya et al. (2012) | split mouth | 18–60 | NR | advanced | no patients requiring antibiotic prophylaxis | NR | NO | acceptable |
| Verma et al. (2011) | split mouth | 28–49 | 7 M 5 F | NR | NO | not prior to 1 month | NR | acceptable |
| Paul et al. (1992) | split mouth | 42–65 | 6 M 1 F | advanced | NO | NR | NR | NR |
| Yukna et al. (1996) | split mouth | 46.8 | 15 M 12 F | NR | NR | NR | NR | NR |
| Blood Derivatives | ||||||||
| Bajaj et al. (2013) | parallel arms | mean age: 39.4 | 22 M 20 F | chronic | NO | no medication affecting periodontal healing | NO | acceptable |
| Kanoriya et al. (2017) | parallel arms | 30–50 | 36 M 36 F | chronic (not aggressive) | NO | no medication affecting periodontal therapy | NO | acceptable |
| Sharma et al. (2011) | split mouth | mean age: 34.2 | 10 M 8 F | NR | NO | no medication affecting periodontal healing | NO | acceptable |
| Pradeep et al. (2009) | split mouth | mean age: 42.8 | 10 F 10 M | NR | NO | no medication affecting wound healing | NO | acceptable |
| Agarwal et al. (2020) | parallel arms | 30–65 mean age: 46 ± 15 | 20 M 26 F | chronic moderate to severe | NO | NO | NO | NR |
| Siddiqui et al. (2016) | split mouth/parallel arms | 30–50 | 24 M 7 F | chronic moderate to severe | NO | no antibiotics or medications affecting the periodontal therapy 6 months prior to the study | NO | Plaque score: 0.1–0.9 |
| Miscellaneous Materials | ||||||||
| Tsao et al. (2006) | parallel arms | mean age: 54.4 ± 9.8 | 15 M 12 F | NR | NO | #no steroids (only for topical use)/not for 1 month #no antibiotics within 3 months prior to enrollment #not chronically treated with medication affecting periodontal status | NR | acceptable |
| Pradeep et al. (2016) | parallel arms | 25–55 | 60 M 50 F | chronic (not aggressive) | NO | #no antibiotics in the preceding 6 months #no drugs affecting periodontal wound healing | NO | acceptable |
| Lekovic et al. (2003) | split mouth | mean age: 38 ± 11 | 12 M 14 F | NR | NO | no medication causing gingival enlargement | 9 smokers 17 non-smokers | acceptable |
| Santana et al. (2009) | parallel arms | 41–63 mean age: 48.3 | 26 M 34 F | advanced chronic (not aggressive) | NO | not for 6 months/no | NO | acceptable |
| Eto et al. (2007) | split mouth | 34–63 mean age: 44.3 | NR | chronic | NO | no medication affecting periodontal healing | NO | NR |
| Houser et al. (2001) | split mouth/parallel arms | mean age: 46 | 13 M 8 F | advanced adult | NR | NR | NR | 20% plaque index prior to the surgical therapy |
| Chitsazi et al. (2007) | parallel arms | 32–48 mean age: 40 | 7 M 3 F | chronic moderate to severe | NO | no antibiotics in the past 6 months | NO | NR |
| Serroni et al. (2021) | parallel arms | 39–65 mean age: 54 ± 14 | 22 M 22 F | stage 3–stage 4 | NO | no medication affecting periodontal healing 6 months prior to the study | NO | Full mouth plaque score < 20% |
| Anderegg et al. (1999) | split mouth | 42–67 Mean age: 55 | 9 M 6 F | moderate to advanced | NO | no medication at least 6 months prior to the study | NR | Plaque index ≤ 10% |
| Mohamed et al. (2016) | split mouth | 38–52 | 14 M | moderate to severe | NO | No medication 6 months prior to the study | NR | NR |
| Study (Year) | Intervention | N | Follow-Up Period (Months) | Outcomes (pre-op and post-op) | |||
|---|---|---|---|---|---|---|---|
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Non-Resorbable Membranes | |||||||
| Mombelli et al. (1996) | E-PTFE | 5 furc | 12.5 | - | 3.6 ± 1.52 NR | - | - |
| E-PTFE + antibiotic | 5 furc | 12.5 | - | 3.8 ± 0.84 NR | - | - | |
| OFD + antibiotic | 5 furc | 12.5 | - | 4.2 ± 1.09 NR | - | - | |
| OFD | 5 furc | 12.5 | - | 3.4 ± 1.14 NR | - | - | |
| Pontoriero et al. (1988) (A) | PTFE | 21 subj/furc (buccal) | 6 | 7.3 ± 1.1 3.2 ± 1.4 | 6 ± 0.9 1.5 ± 1.2 | 4.4 ± 1.2 0.3 ± 0.4 | - |
| OFD | 21 subj/furc (buccal) | 6 | 7.3 ± 1.5 5.8 ± 1.1 | 6 ± 1.6 3.2 ± 0.8 | 4 ± 0.8 2.0 ± 1.1 | - | |
| Pontoriero et al. (1988) (B) | PTFE | 21 subj/furc (lingual) | 6 | 7.5 ± 1.6 4.6 ± 1.7 | 6 ± 1 2.5 ± 1 | 4 ± 0.8 0.7 ± 1.0 | - |
| OFD | 21 subj/furc (lingual) | 6 | 7.2 ± 0.6 6.6 ± 0.7 | 5.4 ± 0.5 3.3 ± 0.5 | 4.4 ± 1.2 2.2 ± 1.2 | - | |
| Metzler et al. (1991) | E-PTFE | 17 subj/furc | 6 | 6.4 ± 1.3 5.4 ± 1.3 | 5.0 ± 1.5 3.3 ± 1.6 | - | - |
| OFD | 17 subj/furc | 6 | 5.7 ± 1.5 5.5 ± 1.7 | 4.6 ± 1.4 3.7 ± 1.5 | - | - | |
| Avera et al. (1998) (A) | PTFE | 8 subj/furc (buccal) | 9 | - | 7 ± 0.66 4.12 ± 0.6 | - | - |
| OFD | 8 subj/furc (buccal) | 9 | - | 6.25 ± 0.59 4.87 ± 0.57 | - | - | |
| Avera et al. (1998) (B) | PTFE | 8 subj/furc (lingual) | 9 | - | 6.63 ± 0.57 3.75 ± 0.59 | - | - |
| OFD | 8 subj/furc (lingual) | 9 | - | 5.75 ± 0.41 4.5 ± 0.45 | - | - | |
| Pontoriero et al. (1995) | E-PTFE + CPF | 28 subj/furc (mesial) | 6 | 7 6.3 | 5.7 4.1 | - | - |
| OFD | 28 subj/furc (mesial) | 6 | 7.2 7.1 | 5.6 4.3 | - | - | |
| Study (Year) | Intervention | N | Follow-Up Period (Months) | Outcome (pre-op and post-op) | |||
|---|---|---|---|---|---|---|---|
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Absorbable Membranes | |||||||
| Balusubramanya et al. (2012) | v. m. + CPF | 11 furc | 6 | 4.09 ± 0.70 1.91 ± 0.70 | - | - | 8.27 ± 1.19 6.73 ± 0.90 |
| OFD | 11 furc | 6 | 3.82 ± 0.60 2.73 ± 1.01 | - | - | 7.73 ± 1.35 6.36 ± 1.12 | |
| Verma et al. (2011) | aut. periost. gr. | 12 subj/furc | 6 | 5.33 ± 0.49 3.17 ± 0.39 | - | - | - |
| OFD | 12 subj/furc | 6 | 5.50 ± 0.80 4.67 ± 0.78 | - | - | - | |
| Paul et al. (1992) | c. m. | 7 subj/14 furc | 6 | 6.86 ± 1.77 | 5.00 ± 0.93 NR | - | - |
| OFD | 7 subj/14 furc | 6 | 5.79 ± 1.26 | 4.29 ± 0.59 NR | - | - | |
| Yukna et al. (1996) | c. m. | 27 furc | 6–12 | - | 5.8 ± 1.2 4.1 ± 1.3 | - | - |
| OFD | 27 furc | 6–12 | - | 5.5 ± 1.6 4.2 ± 1.6 | - | - | |
| Study (Year) | Intervention | N | Follow-Up Period (Months) | Outcome (pre-op and post-op) | |||
|---|---|---|---|---|---|---|---|
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Blood Derivatives | |||||||
| Bajaj et al. (2013) | PRF | 12 (24 furc) | 9 | 7.42 ± 0.78 4.54 ± 0.51 | 7.29 ± 0.95 3.0 ± 0.51 | 8.17 ± 0.82 5.42 ± 0.72 | - |
| PRP | 13 (25 furc) | 9 | 7.08 ± 0.72 4.38 ± 0.71 | 7.17 ± 1.01 3.25 ± 0.68 | 8.08 ± 0.65 5.58 ± 0.72 | - | |
| OFD | 12 (23 furc) | 9 | 7.32 ± 0.80 5.92 ± 0.70 | 6.87 ± 0.90 5.29 ± 0.99 | 7.96 ± 0.86 6.87 ± 0.85 | - | |
| Kanoriya et al. (2017) | PRF | 24 subj/furc | 9 | 7.56 ± 0.94 4.17 ± 0.83 | 7.73 ± 1.35 4.04 ± 0.87 | 7.13 ± 0.75 4.26 ± 0.81 | - |
| PRF + 1% ALN | 25 subj/furc | 9 | 7.52 ± 0.91 3.4 ± 0.57 | 7.52 ± 1.22 3.12 ± 0.88 | 7.16 ± 1.02 3.52 ± 0.65 | - | |
| OFD | 23 subj/furc | 9 | 7.41 ± 0.92 5.08 ± 0.88 | 7.66 ± 1.27 5.25 ± 1.15 | 7.08 ± 0.82 5.04 ± 0.80 | - | |
| Sharma et al. (2011) | PRF | 18 subj/furc | 9 | 7.39 ± 1.145 5.06 ± 1.434 | 6.39 ± 1.145 2.33 ± 1.029 | 8.83 ± 1.618 6.17 ± 1.654 | - |
| OFD | 18 subj/furc | 9 | 7.33 ± 1.029 6.06 ± 1.162 | 6.33 ± 1.029 3.44 ± 1.042 | 8.94 ± 1.474 7.06 ± 1.349 | - | |
| Pradeep et al. (2009) | PRP | 20 subj/furc | 6 | 8.40 ± 1.71 6.40 ± 1.71 | 6.00 ± 0.94 3.70 ± 0.95 | 10.60 ± 2.07 8.10 ± 2.13 | - |
| OFD | 20 subj/furc | 6 | 7.00 ± 1.05 6.90 ± 1.66 | 5.10 ± 1.20 4.30 ± 1.64 | 8.70 ± 1.64 7.90 ± 1.85 | - | |
| Agarwal et al. (2020) | PRF | 20 subj/furc | 9 | 7.15 ± 0.67 3.60 ± 0.99 | 6.35 ± 0.93 2.55 ± 0.51 | - | 5.30 ± 0.66 3.50 ± 0.69 |
| PRF + al. gr. | 20 subj/furc | 9 | 7.15 ± 0.67 3.25 ± 0.44 | 6.30 ± 0.73 2.30 ± 0.47 | - | 5.20 ± 0.77 3.40 ± 0.59 | |
| OFD | 20 subj/furc | 9 | 6.90 ± 0.64 5.55 ± 0.51 | 6.10 ± 0.85 4.60 ± 0.60 | - | 5.20 ± 0.62 3.85 ± 0.77 | |
| Siddiqui et al. (2016) | PRF | 15 furc | 6 | 5.47 ± 1.30 3.07 ± 1.03 | 3.73 ± 1.22 1.47 ± 0.64 | 4.60 ± 0.91 2.20 ± 0.86 | - |
| β-TCP | 15 furc | 6 | 5.53 ± 1.25 3 ± 0.85 | 4 ± 1.25 1.53 ± 0.52 | 4.53 ± 0.74 2.27 ± 0.59 | - | |
| OFD | 15 furc | 6 | 5.47 ± 1.06 4.53 ± 1.13 | 4.07 ± 1.10 3.04 ± 0.77 | 4.47 ± 0.83 3.73 ± 0.80 | - | |
| Study (Year) | Intervention | N | Follow-Up Period (Months) | Outcome (pre-op and post-op) | |||
|---|---|---|---|---|---|---|---|
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Miscellaneous Materials | |||||||
| Tsao et al. (2006) | al. gr. | 9 subj/furc | 6 | 5.1 ± 2.8 5.0 ± 1.9 | 4.3 ± 1.8 3.4 ± 1.4 | - | 3.9 ± 1.1 2.7 ± 1.4 |
| al. gr. + c. m. | 9 subj/furc | 6 | 5.2 ± 2.0 5.6 ± 2.4 | 4.6 ± 1.1 3.9 ± 1.5 | - | 4.2 ± 1.2 3.1 ± 1.2 | |
| OFD | 9 subj/furc | 6 | 5.4 ± 1.3 6.3 ± 1.8 | 4.7 ± 0.9 4.5 ± 0.9 | - | 4.7 ± 1.7 3.8 ± 1.6 | |
| Pradeep et al. (2016) | PRF + syn. gr. | 35 subj/furc | 9 | 7.57 ± 0.50 4.25 ± 0.44 | 7.65 ± 1.05 3.97 ± 0.16 | 7.48 ± 0.61 4.51 ± 0.50 | - |
| RSV + PRF + syn. gr. | 35 subj/furc | 9 | 7.51 ± 0.50 3.34 ± 0.48 | 7.65 ± 1.05 3.02 ± 0.16 | 7.42 ± 0.60 3.37 ± 0.49 | - | |
| OFD | 35 subj/furc | 9 | 7.54 ± 0.56 5.71 ± 0.45 | 7.34 ± 0.76 5.22 ± 0.91 | 7.45 ± 0.50 5.82 ± 0.38 | - | |
| Lekovic et al. (2003) | PRP + xen. gr. + c. m. | 26 subj/furc | 9 | - | 6.86 ± 0.31 2.79 ± 0.32 | - | - |
| OFD | 26 subj/furc | 9 | - | 6.78 ± 0.28 4.297 ± 0.36 | - | - | |
| Santana et al. (2009) | comp. gr + PTFE + CPF | 30 subj/furc | 12 | 7.06 ± 0.7 4.01 ± 1.0 | 6.36 ± 1 2.8 ± 1.6 | 4.85 ± 0.9 2.4 ± 1.3 | - |
| OFD | 30 subj/furc | 12 | 6.65 ± 0.8 6 ± 0.6 | 5.95 ± 1.3 5.3 ± 1.0 | 6.10 ± 1.4 5.56 ± 0.8 | - | |
| Eto et al. (2007) | syn. gr. + P15+ CPF | 12 subj/furc | 6–7 | 12.8 ± 2.7 11.1 ± 2.1 * | 3.2 ± 1.5 2.4 ± 0.7 | 8.5 ± 2.6 6.1 ± 2.3 * | - |
| OFD | 12 subj/furc | 6–7 | 13.7 ± 2.6 11.6 ± 3.3 * | 4.3 ± 2.7 2.7 ± 2.9 | 8.4 ± 3.2 6.9 ± 1.9 | - | |
| Houser et al. (2001) | xen. gr. + c. m. | 16 subj/18 furc | 6 | 6.4 4.6 | 5.9 3.9 | - | 5.2 3.0 |
| OFD | 11 subj/13 furc | 6 | 6.3 5.7 | 5.7 5.4 | - | 5.5 5.7 | |
| Chisatzi et al. (2007) | EMD | 10 subj/10 furc | 6 | 10.8 9.35 | 4.75 2.80 | 4.70 2.80 | - |
| OFD | 10 subj/10 furc | 6 | 10.9 10.00 | 4.65 3.10 | 4.60 4.00 | - | |
| Serroni et al. (2021) | L-PRF + aut. b. gr. | 18 subj/furc | 6 | 6.56 ± 2.455 4.50 ± 2.595 | 4.61 ± 1.379 2.33 ± 1.029 | 5.50 ± 1.043 3.22 ± 1.003 | - |
| aut. b. gr. | 18 subj/furc | 6 | 6.83 ± 2.093 4.89 ± 2.324 | 5.17 ± 0.618 3 ± 0.343 | 5.11 ± 0.9 3.67 ± 0.97 | - | |
| OFD | 18 subj/furc | 6 | 8.33 ± 2.951 7.39 ± 2.570 | 5.61 ± 1.614 4.39 ± 1.335 | 6.06 ± 1.731 5 ± 1.283 | - | |
| Anderegg et al. (1999) | b. g. | 15 subj/furc | 6 | 6.67 ±0.29 3.40 ± 0.21 | - | - | - |
| OFD | 15 subj/furc | 6 | 6.47 ± 0.24 4.07 ± 0.28 | - | - | - | |
| Mohamed et al. (2016) | syn. gr. + PRP | 11 subj/furc | 6 | 5.7 ± 1.2 4.2 ± 0.9 | - | - | - |
| OFD | 11 subj/furc | 6 | 5.9 ± 1.1 4.6 ± 1.3 | - | - | - | |
| (A) | |||||||
| Study (Year) | Intervention | N | Follow-up Period (Months) | Outcome (pre-op and post-op) | |||
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Non-Resorbable Membranes | |||||||
| Mombelli et al. (1996) | E-PTFE | 5 furc | 12.5 | −0.4 ± 2.07 | 0.2 ± 1.3 | - | 0 ± 1 (2 furc open) |
| E-PTFE + antibiotic | 5 furc | 12.5 | 0.2 ± 1.48 | 0.8 ± 1.3 | - | 1.2 ± 1.09 | |
| OFD + antibiotic | 5 furc | 12.5 | 0 ± 1.22 | 1 ± 0.71 | - | 0.4 ± 1.52 | |
| OFD | 5 furc | 12.5 | −0.8 ± 0.84 | 0.4 ± 0.55 | - | −0.5 ± 0.58 (1 furc open) | |
| Pontoriero et al. (1988) (A) | PTFE | 21 subj/furc (buccal) | 6 | 4.1 *1 | 4.5 * | 4.1 ± 1.3 * | - |
| OFD | 21 subj/furc (buccal) | 6 | 1.5 * | 2.8 * | 1.9 ± 1.3 | - | |
| Pontoriero et al. (1988) (B) | PTFE | 21 subj/furc (buccal) | 6 | 2.9 *1 | 3.5 * | 3.3 ± 1 * | - |
| OFD | 21 subj/furc (buccal) | 6 | 0.6 | 2.1 * | 2.2 ± 1.1 * | - | |
| Metzler et al. (1991) | E-PTFE | 17 subj/furc | 6 | 1 ± 0.9 | 1.7 ± 0.8 | - | - |
| OFD | 17 subj/furc | 6 | 0.2 ± 0.6 | 0.9 ± 0.8 | - | - | |
| Avera et al. (1998) (A) | PTFE | 8 subj/furc (buccal) | 9 | 2 ± 0.631 | 2.88 ± 0.481 | - | - |
| OFD | 8 subj/furc (buccal) | 9 | 0.5 ± 0.42 | 1.38 ± 0.65 | - | - | |
| Avera et al. (1998) (B) | PTFE | 8 subj/furc (lingual) | 9 | 1.5 ± 0.461 | 2.88 ± 0.551 | - | - |
| OFD | 8 subj/furc (lingual) | 9 | 0.13 ± 0.48 | 1.25 ± 0.53 | - | - | |
| Pontoriero et al. (1995) | E-PTFE + CPF | 28 subj/furc (mesial) | 6 | 0.7 * | 1.6 * | - | - |
| OFD | 28 subj/furc (mesial) | 6 | 0.1 | 1.3 * | - | - | |
| (B) | |||||||
| Study (year) | Intervention | N | Follow-up period (months) | Outcome (pre-op and post-op) | |||
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Absorbable Membranes | |||||||
| Balusubramanya et al. (2012) | v. m. + CPF | 11 furc | 6 | 2.18 ± 0.60 *1 | - | - | 1.54 ± 1.04 * |
| OFD | 11 furc | 6 | 1.09 ± 0.94 * | - | - | 1.37 ± 1.12 * | |
| Verma et al. (2011) | aut. periost. gr. | 12 subj/furc | 6 | 2.17 ± 0.72 *1 | - | - | - |
| OFD | 12 subj/furc | 6 | 0.83 ± 0.72 * | - | - | - | |
| Paul et al. (1992) | c. m. | 7 subj/14 furc | 6 | 1.64 ± 0.84 | 1.50 ± 0.76 *1 | - | - |
| OFD | 7 subj/14 furc | 6 | 1.00 ± 1.61 | 0.86 ± 0.77 | - | - | |
| Yukna et al. (1996) | c. m. | 27 furc | 6–12 | 0.8 ± 1.4 | 1.7 ± 1.3 * | - | - |
| OFD | 27 furc | 6–12 | 0.4 ± 1.8 | 1.3 ± 1.4 * | - | - | |
| (C) | |||||||
| Study (year) | Intervention | N | Follow-up period (months) | Outcome (pre-op and post-op) | |||
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Blood Derivatives | |||||||
| Bajaj et al. (2013) | PRF | 12 (24 furc) | 9 | 2.87 ± 0.85 *1 | 4.29 ± 1.04 *1 | 2.75 ± 0.94 *1 | - |
| PRP | 13 (25 furc) | 9 | 2.71 ± 1.04 *1 | 3.92 ± 0.93 *1 | 2.5 ± 0.83 *1 | - | |
| OFD | 12 (23 furc) | 9 | 1.37 ± 0.58 * | 1.58 ± 1.02 * | 1.08 ± 0.50 * | - | |
| Kanoriya et al. (2017) | PRF | 24 subj/furc | 9 | 3.39 ± 0.49 *1,2 | 3.69 ± 0.76 *1,2 | 2.86 ± 0.062 *1,2 | - |
| PRF + 1% ALN | 25 subj/furc | 9 | 4.12 ± 0.6 *1 | 4.4 ± 0.57 *1 | 3.64 ± 0.90 *1 | - | |
| OFD | 23 subj/furc | 9 | 2.33 ± 0.48 * | 2.41 ± 0.77 * | 2.04 ± 0.35 * | - | |
| Sharma et al. (2011) | PRF | 18 subj/furc | 9 | 2.333 ± 0.485 *1 | 4.056 ± 0.416 *1 | 2.667 ± 0.594 *1 | - |
| OFD | 18 subj/furc | 9 | 1.278 ± 0.461 * | 2.889 ± 0.676 * | 1.889 ± 0.758 * | - | |
| Pradeep et al. (2009) | PRP | 20 subj/furc | 6 | 2.50 ± 1.64 *1 | 2.3 ± 1.41 *1 | 2.50 ± 1.17 *1 | - |
| OFD | 20 subj/furc | 6 | 0.10 ± 1.10 | 0.80 ± 1.31 | 0.80 ± 0.63 * | - | |
| Agarwal et al. (2020) | PRF | 15 furc | 6 | 3.55 ± 1.05 *1 | 3.80 ± 0.77 *1 | - | 1.80 ± 0.83 * |
| PRF+ al. gr. | 15 furc | 6 | 3.90 ± 0.72 *1 | 4 ± 0.79 *1 | - | 1.80 ± 0.41 * | |
| OFD | 15 furc | 6 | 1.35 ± 0.49 * | 1.50 ± 0.76 * | - | 1.35 ± 0.67 * | |
| Siddiqui et al. (2016) | PRF | 15 furc | 6 | 2.40 ± 0.91 *1 | 2.27 ± 1.10 * | 2.40 ± 1.06 *1 | - |
| β-TCP | 15 furc | 6 | 2.53 ± 0.83 *1 | 2.47 ± 1.51 * | 2.27 ± 0.46 *1 | - | |
| OFD | 15 furc | 6 | 0.93 ± 0.46 * | 1.03 ± 0.67 * | 0.73 ± 0.46 * | - | |
| (D) | |||||||
| Study (year) | Intervention | N | Follow-up period (months) | Outcome (pre-op and post-op) | |||
| VCAL (mm) | VPD (mm) | HCAL (mm) | HPD (mm) | ||||
| Miscellaneous Materials | |||||||
| Tsao et al. (2006) | al. gr. | 9 subj/furc | 6 | 0.1 ± 1 | 0.9 ± 0.9 * | - | 1.2 ± 1.9 |
| al. gr. + c. m. | 9 subj/furc | 6 | −0.3 ± 1.2 | 0.7 ± 1 | - | 1.1 ± 0.5 * | |
| OFD | 9 subj/furc | 6 | −0.9 ± 1.6 | 0.1 ± 1.1 | - | 0.9 ± 1.9 | |
| Pradeep et al. (2016) | PRF + syn. gr. | 35 subj/furc | 9 | 3.31 ± 0.52 *1‚2 | 3.68 ± 1.07 *1‚2 | 2.97 ± 0.56 *1‚2 | - |
| RSV + PRF + syn. gr. | 35 subj/furc | 9 | 4.17 ± 0.70 *1 | 4.62 ± 1.03 *1 | 4.05 ± 0.76 *1 | - | |
| OFD | 35 subj/furc | 9 | 1.82 ± 0.78 * | 2.11 ± 1.25 * | 1.62 ± 0.64 * | - | |
| Lekovic et al. (2003) | PRP + xen. gr. + c. m. | 26 subj/furc | 9 | 3.29 ± 0.42 *1 | 4.07 ± 0.33 *1 | - | - |
| OFD | 26 subj/furc | 9 | 1.68 ± 0.31 * | 2.49 ± 0.38 * | - | - | |
| Santana et al. (2009) | comp. gr + PTFE + CPF | 30 subj/furc | 12 | 3.05 ± 0.6 *1 | 3.56 ± 0.6 *1 | 3.45 ± 1.3 *1 | - |
| OFD | 30 subj/furc | 12 | 0.65 ± 0.6 * | 0.6 ± 1 * | 0.55 ± 0.7 * | - | |
| Eto et al. (2007) | syn. gr. + P15+ CPF | 12 subj/furc | 6–7 | - | - | - | - |
| OFD | 12 subj/furc | 6–7 | - | - | - | - | |
| Houser et al. (2001) | xen. gr. + c. m. | 16 subj/18 furc | 6 | 1.8 ± 1.8 * | 2 ± 1.7 *1 | 2.2 ± 2.2 *1 | - |
| OFD | 11 subj/13 furc | 6 | 0.6 ± 2.06 | 0.3 ± 1.37 | −0.2 ± 1.6 | - | |
| Chisatzi et al. (2007) | EMD | 10 subj/10 furc | 6 | 1.45 * | 1.95 * | 1.9 *1 | - |
| OFD | 10 subj/10 furc | 6 | 0.9 * | 0.9 * | 0.6 *1 | - | |
| Serroni et al. (2021) | L-PRF + aut. b. gr. | 18 subj/furc | 6 | 2.139 ± 0.278 *1‚2 | 2.515 ± 0.714 *1 | 2.299 ± 0.18 *1‚2 | - |
| aut. b. gr. | 18 subj/furc | 6 | 1.994 ± 0.276 *1 | 2.150 ± 0.169 *1 | 1.613 ± 0.183 *1 | - | |
| OFD | 18 subj/furc | 6 | 0.811 ± 0.284 * | 1.002 ± 0.714 * | 0.866 ± 0.184 * | - | |
| Anderegg et al. (1999) | b. g. | 15 subj/furc | 6 | 3.27 ± 0.27 * | - | - | - |
| OFD | 15 subj/furc | 6 | 2.40 ± 0.24 * | - | - | - | |
| Mohamed et al. (2016) | syn. gr. + PRP | 11 subj/furc | 6 | - | - | - | 2.3 |
| OFD | 11 subj/furc | 6 | - | - | - | 1.7 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgiou, G.O.; Tarallo, F.; Marchetti, E.; Bizzarro, S. Overview of the Effect of Different Regenerative Materials in Class II Furcation Defects in Periodontal Patients. Materials 2022, 15, 3194. https://doi.org/10.3390/ma15093194
Georgiou GO, Tarallo F, Marchetti E, Bizzarro S. Overview of the Effect of Different Regenerative Materials in Class II Furcation Defects in Periodontal Patients. Materials. 2022; 15(9):3194. https://doi.org/10.3390/ma15093194
Chicago/Turabian StyleGeorgiou, Gerasimos Odysseas, Francesco Tarallo, Enrico Marchetti, and Sergio Bizzarro. 2022. "Overview of the Effect of Different Regenerative Materials in Class II Furcation Defects in Periodontal Patients" Materials 15, no. 9: 3194. https://doi.org/10.3390/ma15093194
APA StyleGeorgiou, G. O., Tarallo, F., Marchetti, E., & Bizzarro, S. (2022). Overview of the Effect of Different Regenerative Materials in Class II Furcation Defects in Periodontal Patients. Materials, 15(9), 3194. https://doi.org/10.3390/ma15093194