
Retrospective Long-Term Clinical Outcome of Feldspathic Ceramic Veneers




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Statistical Analysis
3. Results
3.1. Comparison between the Prep and No-Prep Technique
3.2. Comparison between the Five Groups of Maximum Veneer Thickness
3.3. Comparison between the Baseline Scores and the Scores after 7 Years
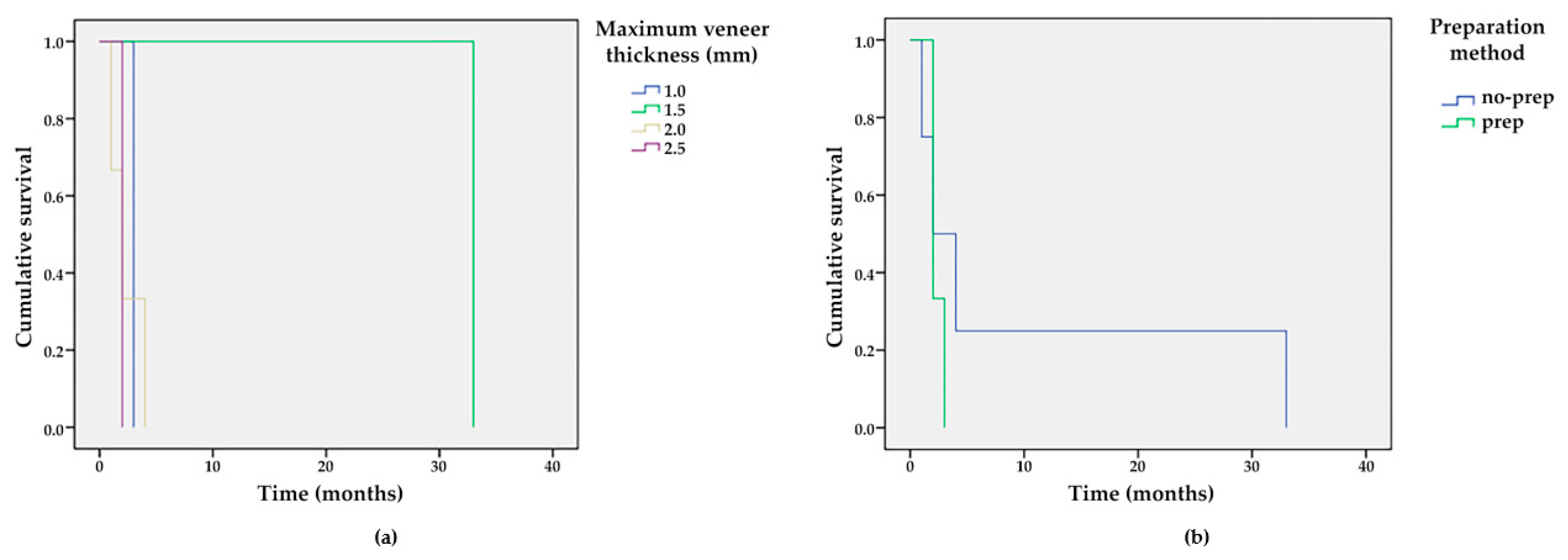
3.4. Survival Time Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aslam, A.; Khan, D.A.; Hassan, S.H.; Ahmed, B. Ceramic Fracture in Metal-Ceramic Restorations: The Aetiology. Dent. Update 2017, 44, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, M.J.; Aquilino, S.A.; Diaz-Arnold, A.M.; Haselton, D.R.; Stanford, C.M.; Vargas, M.A. Relative translucency of six all-ceramic systems. Part I: Core materials. J. Prosthet. Dent. 2002, 88, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Edelhoff, D.; Sorensen, J.A. Tooth structure removal associated with various preparation designs for anterior teeth. J. Prosthet. Dent. 2002, 87, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.H.D.; Lima, E.; Miranda, R.B.P.; Favero, S.S.; Lohbauer, U.; Cesar, P.F. Dental ceramics: A review of new materials and processing methods. Braz. Oral Res. 2017, 31, e58. [Google Scholar] [CrossRef] [PubMed]
- Bosch, G.; Ender, A.; Mehl, A. Non- and minimally invasive full-mouth rehabilitation of patients with loss of vertical dimension of occlusion using CAD/CAM: An innovative concept demonstrated with a case report. Int. J. Comput. Dent. 2015, 18, 273–286. [Google Scholar] [PubMed]
- Savi, A.; Turillazzi, O.; Crescini, A.; Manfredi, M. Esthetic treatment of a diffuse amelogenesis imperfecta using pressed lithium disilicate and feldspathic ceramic restorations: 5-year follow up. J. Esthet. Restor. Dent. 2014, 26, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Tyas, M.J.; Anusavice, K.J.; Frencken, J.E.; Mount, G.J. Minimal intervention dentistry—A review. FDI Commission Project 1-97. Int. Dent. J. 2000, 50, 1–12. [Google Scholar] [CrossRef]
- Vailati, F.; Gruetter, L.; Belser, U.C. Adhesively restored anterior maxillary dentitions affected by severe erosion: Up to 6-year results of a prospective clinical study. Eur. J. Esthet. Dent. 2013, 8, 506–530. [Google Scholar]
- McLaren, E.A.; Whiteman, Y.Y. Ceramics: Rationale for material selection. Compend. Contin. Educ. Dent. 2010, 31, 666–668. [Google Scholar] [PubMed]
- McLaren, E.A.; LeSage, B. Feldspathic veneers: What are their indications? Compend. Contin. Educ. Dent. 2011, 32, 44–49. [Google Scholar]
- Layton, D.M.; Clarke, M.; Walton, T.R. A systematic review and meta-analysis of the survival of feldspathic porcelain veneers over 5 and 10 years. Int. J. Prosthodont. 2012, 25, 590–603. [Google Scholar] [PubMed]
- Morimoto, S.; Albanesi, R.B.; Sesma, N.; Agra, C.M.; Braga, M.M. Main Clinical Outcomes of Feldspathic Porcelain and Glass-Ceramic Laminate Veneers: A Systematic Review and Meta-Analysis of Survival and Complication Rates. Int. J. Prosthodont. 2016, 29, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Layton, D.M.; Walton, T.R. The up to 21-year clinical outcome and survival of feldspathic porcelain veneers: Accounting for clustering. Int. J. Prosthodont. 2007, 25, 604–612. [Google Scholar]
- Peumans, M.; De Munck, J.; Fieuws, S.; Lambrechts, P.; Vanherle, G.; Van Meerbeek, B. A prospective ten-year clinical trial of porcelain veneers. J. Adhes. Dent. 2004, 6, 65–76. [Google Scholar]
- Pini, N.P.; Aguiar, F.H.; Lima, D.A.; Lovadino, J.R.; Terada, R.S.; Pascotto, R.C. Advances in dental veneers: Materials, applications, and techniques. Clin. Cosmet. Investig. Dent. 2012, 10, 9–16. [Google Scholar]
- Strassler, H.E. Minimally invasive porcelain veneers: Indications for a conservative esthetic dentistry treatment modality. Gen. Dent. 2007, 55, 686–694, quiz 695–696, 712. [Google Scholar]
- Smales, R.J.; Etemadi, S. Long-term survival of porcelain laminate veneers using two preparation designs: A retrospective study. Int. J. Prosthodont. 2004, 17, 323–326. [Google Scholar] [CrossRef]
- Wildgoose, D.G.; Winstanley, R.B.; van Noort, R. The laboratory construction and teaching of ceramic veneers: A survey. J. Dent. 1997, 25, 119–123. [Google Scholar] [CrossRef]
- Venturini, A.B.; Prochnow, C.; May, L.G.; Bottino, M.C.; Felipe Valandro, L. Influence of hydrofluoric acid concentration on the flexural strength of a feldspathic ceramic. J. Mech. Behav. Biomed. Mater. 2015, 48, 241–248. [Google Scholar] [CrossRef]
- Giordano, R.A., 2nd; Pelletier, L.; Campbell, S.; Pober, R. Flexural strength of an infused ceramic, glass ceramic, and feldspathic porcelain. J. Prosthet. Dent. 1995, 73, 411–418. [Google Scholar] [CrossRef]
- Gresnigt, M.; Ozcan, M. Esthetic rehabilitation of anterior teeth with porcelain laminates and sectional veneers. J. Can. Dent. Assoc. 2011, 77, b143. [Google Scholar] [PubMed]
- Toreskog, S. The minimally invasive and aesthetic bonded porcelain technique. Int. Dent. J. 2002, 52, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Touati, B. Innovative dental ceramics: Expanding the material alternatives. Pract. Proced. Aesthet. Dent. 2005, 17, 357–358. [Google Scholar] [PubMed]
- Federizzi, L.; Gomes, É.A.; Báratro, S.S.; Baratto-Filho, F.; Bacchi, A.; Spazzin, A.O. Use of Feldspathic Porcelain Veneers to Improve Smile Harmony: A 3-Year Follow-up Report. Braz. Dent. J. 2016, 27, 767–774. [Google Scholar] [CrossRef] [Green Version]
- Giordano, R. Materials for chairside CAD/CAM-produced restorations. J. Am. Dent. Assoc. 2006, 137, 14S–21S. [Google Scholar] [CrossRef] [PubMed]
- Javaheri, D. Considerations for planning esthetic treatment with veneers involving no or minimal preparation. J. Am. Dent. Assoc. 2007, 138, 331–337. [Google Scholar] [CrossRef] [Green Version]
- Radz, G.M. Minimum thickness anterior porcelain restorations. Dent. Clin. N. Am. 2011, 55, 353–370, ix. [Google Scholar] [CrossRef]
- Magne, P.; Belser, U.C. Novel porcelain laminate preparation approach driven by a diagnostic mock-up. J. Esthet. Restor. Dent. 2004, 16, 7–16, discussion 17–18. [Google Scholar] [CrossRef]
- Mozayek, R.S.; Alkhalil, M.A.; Allaf, M.; Dayoub, S. Evaluation of the fracture strength of porcelain sectional veneers made from different sintered feldspathic porcelains: An in vitro study. Dent. Med. Probl. 2019, 56, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Farias-Neto, A.; Gomes, E.M.; Sánchez-Ayala, A.; Sánchez-Ayala, A.; Vilanova, L.S. Esthetic Rehabilitation of the Smile with No-Prep Porcelain Laminates and Partial Veneers. Case Rep. Dent. 2015, 2015, 452765. [Google Scholar] [CrossRef] [Green Version]
- Guess Gierthmuehlen, P.C.; Steger, E. CAD/CAM Solutions for Minimally Invasive All-Ceramic Rehabilitation of Extended Erosive Lesions. Compend. Contin. Educ. Dent. 2016, 37, 340–345. [Google Scholar] [PubMed]
- da Cunha, L.F.; Gonzaga, C.C.; Saab, R.; Mushashe, A.M.; Correr, G.M. Rehabilitation of the dominance of maxillary central incisors with refractory porcelain veneers requiring minimal tooth preparation. Quintessence Int. 2015, 46, 837–841. [Google Scholar] [PubMed]
- Agustín-Panadero, R.; Solá-Ruíz, M.F.; Chust, C.; Ferreiroa, A. Fixed dental prostheses with vertical tooth preparations without finish lines: A report of two patients. J. Prosthet. Dent. 2016, 115, 520–526. [Google Scholar] [CrossRef]
- Imburgia, M.; Canale, A.; Cortellini, D.; Maneschi, M.; Martucci, C.; Valenti, M. Minimally invasive vertical preparation design for ceramic veneers. Int. J. Esthet. Dent. 2016, 11, 460–471. [Google Scholar] [PubMed]
- García-Gil, I.; Perez de la Calle, C.; Lopez-Suarez, C.; Pontevedra, P.; Suarez, M.J. Comparative analysis of trueness between conventional and digital impression in dental-supported fixed dental prosthesis with vertical preparation. J. Clin. Exp. Dent. 2020, 12, e896–e901. [Google Scholar] [CrossRef] [PubMed]
- Vailati, F.; Belser, U.C. Full-mouth adhesive rehabilitation of a severely eroded dentition: The three-step technique. Part 1. Eur. J. Esthet. Dent. 2008, 3, 30–44. [Google Scholar] [PubMed]
- Vailati, F.; Belser, U.C. Full-mouth adhesive rehabilitation of a severely eroded dentition: The three-step technique. Part 2. Eur. J. Esthet. Dent. 2008, 3, 128–146. [Google Scholar]
- Vailati, F.; Belser, U.C. Full-mouth adhesive rehabilitation of a severely eroded dentition: The three-step technique. Part 3. Eur. J. Esthet. Dent. 2008, 3, 236–257. [Google Scholar] [PubMed]
- Grütter, L.; Vailati, F. Full-mouth adhesive rehabilitation in case of severe dental erosion, a minimally invasive approach following the 3-step technique. Eur. J. Esthet. Dent. 2013, 8, 358–375. [Google Scholar]
- D’Arcangelo, C.; Vadini, M.; D’Amario, M.; Chiavaroli, Z.; De Angelis, F. Protocol for a new concept of no-prep ultrathin ceramic veneers. J. Esthet. Restor. Dent. 2018, 30, 173–179. [Google Scholar] [CrossRef]
- Signore, A.; Kaitsas, V.; Tonoli, A.; Angiero, F.; Silvestrini-Biavati, A.; Benedicenti, S. Sectional porcelain veneers for a maxillary midline diastema closure: A case report. Quintessence Int. 2013, 44, 201–206. [Google Scholar] [PubMed]
- Vadini, M.; D’Amario, M.; De Angelis, F.; Falco, A.; D’Arcangelo, C. No-Prep Rehabilitation of Fractured Maxillary Incisors with Partial Veneers. J. Esthet. Restor. Dent. 2016, 28, 351–358. [Google Scholar] [CrossRef]
- Piwowarczyk, A.; Blum, J.; Abendroth, H. Non-prep restoration of an ankylosed incisor: A case report. Quintessence Int. 2015, 46, 281–285. [Google Scholar] [PubMed]
- Furuse, A.Y.; Soares, J.V.; Cunali, R.S.; Gonzaga, C.C. Minimum intervention in restorative dentistry with V-shaped facial and palatal ceramic veneers: A clinical report. J. Prosthet. Dent. 2016, 115, 527–530. [Google Scholar] [CrossRef]
- Ostermann, F.; Meyer, G.; Kern, M. Survey of clinically used adhesive ceramic bonding methods—Follow up after 12 years. Dent. Mater. 2021, 37, e195–e200. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Gresnigt, M.M.M.; Cune, M.S.; Schuitemaker, J.; van der Made, S.A.M.; Meisberger, E.W.; Magne, P.; Özcan, M. Performance of ceramic laminate veneers with immediate dentine sealing: An 11 year prospective clinical trial. Dent. Mater. 2019, 35, 1042–1052. [Google Scholar] [CrossRef]
- Hickel, R.; Peschke, A.; Tyas, M.; Mjör, I.; Bayne, S.; Peters, M.; Hiller, K.A.; Randall, R.; Vanherle, G.; Heintze, S.D. FDI World Dental Federation: Clinical criteria for the evaluation of direct and indirect restorations-update and clinical examples. Clin. Oral Investig. 2010, 14, 349–366. [Google Scholar] [CrossRef]
- Cvar, J.F.; Ryge, G. Reprint of criteria for the clinical evaluation of dental restorative materials. 1971. Clin. Oral Investig. 2005, 9, 215–232. [Google Scholar]
- Kasem, A.T.; Sakrana, A.A.; Ellayeh, M.; Özcan, M. Evaluation of zirconia and zirconia-reinforced glass ceramic systems fabricated for minimal invasive preparations using a novel standardization method. J. Esthet. Restor. Dent. 2020, 32, 560–568. [Google Scholar] [CrossRef]
- Abduo, J. Safety of increasing vertical dimension of occlusion: A systematic review. Quintessence Int. 2012, 43, 369–380. [Google Scholar] [PubMed]
- Silverman, M.M. Accurate measurement of vertical dimension by phonetics and the speaking centric space. Part I. Dent. Dig. 1951, 57, 261–265. [Google Scholar] [PubMed]
- Otto, T.; De Nisco, S. Computer-aided direct ceramic restorations: A 10-year prospective clinical study of Cerec CAD/CAM inlays and onlays. Int. J. Prosthodont. 2002, 15, 122–128. [Google Scholar] [PubMed]
- Sjögren, G.; Molin, M.; van Dijken, J.W. A 10-year prospective evaluation of CAD/CAM-manufactured (Cerec) ceramic inlays cemented with a chemically cured or dual-cured resin composite. Int. J. Prosthodont. 2004, 17, 241–246. [Google Scholar]
- Zimmer, S.; Göhlich, O.; Rüttermann, S.; Lang, H.; Raab, W.H.; Barthel, C.R. Long-term survival of Cerec restorations: A 10-year study. Oper. Dent. 2008, 33, 484–487. [Google Scholar] [CrossRef]
- Bindl, A.; Mörmann, W.H. Survival rate of mono-ceramic and ceramic-core CAD/CAM-generated anterior crowns over 2-5 years. Eur. J. Oral Sci. 2004, 112, 197–204. [Google Scholar] [CrossRef]
- Luciano, M.; Francesca, Z.; Michela, S.; Tommaso, M.; Massimo, A. Lithium disilicate posterior overlays: Clinical and biomechanical features. Clin. Oral Investig. 2020, 24, 841–848. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.; Gadow, R.; Mitic, V. Proceedings of the IV Advanced Ceramics and Applications Conference; Springer: Belgrade, Serbia, 2017. [Google Scholar]
- Kürklü, D.; Azer, S.S.; Yilmaz, B.; Johnston, W.M. Porcelain thickness and cement shade effects on the color and translucency of porcelain veneering materials. J. Dent. 2013, 41, 1043–1050. [Google Scholar] [CrossRef]
- Igiel, C.; Weyhrauch, M.; Mayer, B.; Scheller, H.; Lehmann, K.M. Effects of ceramic layer thickness, cement color, and abutment tooth color on color reproduction of feldspathic veneers. Int. J. Esthet. Dent. 2018, 13, 110–119. [Google Scholar]
- Sari, T.; Ural, C.; Yüzbasioglu, E.; Duran, I.; Cengiz, S.; Kavut, I. Color match of a feldspathic ceramic CAD-CAM material for ultrathin laminate veneers as a function of substrate shade, restoration color, and thickness. J. Prosthet. Dent. 2018, 119, 455–460. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, S.W.; Lim, H.P.; Park, C.; Yun, K.D. Biocompatibility Evaluation of Feldspathic Porcelain with Nano-Sized Silver Ion Particles. J. Nanosci. Nanotechnol. 2018, 18, 1237–1240. [Google Scholar] [CrossRef] [PubMed]
- Sinescu, C.; Negrutiu, M.L.; Todea, C.; Balabuc, C.; Filip, L.; Rominu, R.; Bradu, A.; Hughes, M.; Podoleanu, A.G. Quality assessment of dental treatments using en-face optical coherence tomography. J. Biomed. Opt. 2008, 13, 54–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrini, F.; Sannino, G.; Chiola, C.; Capparé, P.; Gastaldi, G.; Gherlone, E.F. Influence of Intra-Oral Scanner (I.O.S.) on The Marginal Accuracy of CAD/CAM Single Crowns. Int. J. Environ. Res. Public Health 2019, 16, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Esthetic properties | ||
| C1 = Staining: (a) surface and (b) margin | C2 = Color match and translucency | C3 = Esthetic anatomical form |
| Functional properties | ||
| C4 = Fracture of restorative material and retention | C5 = Marginal adaptation | C6 = Occlusal contour and wear |
| Biological properties | ||
| C7 = Postoperative sensitivity and tooth vitality | C8 = Recurrent caries | C9 = Tooth integrity |
| C10 = Periodontal response (always compared to a reference tooth) | C11 = Adjacent mucosa | |
| Score | ||
| 1 = Clinically excellent/very good | 2 = Clinically good | 3 = Clinically sufficient/satisfactory |
| 4 = Clinically unsatisfactory (but reparable) | 5 = Clinically poor (replacement necessary) | |
| Maximum Thickness (mm) | 0.5/1 | 0.5/1.5 | 0.5/2 | 0.5/2.5 | 1/1.5 | 1/2 | 1/2.5 | 1.5/2 | 1.5/2.5 | 2/2.5 |
|---|---|---|---|---|---|---|---|---|---|---|
| p-Value | ||||||||||
| C1_T7 | <0.001 * | 0.001 * | 0.001 * | 0.007 * | 0.532 | 0.302 | 0.903 | 0.119 | 0.601 | 0.765 |
| C3_T7 | 0.052 | 0.025 * | 0.025 * | 0.001 * | 0.679 | <0.001 * | 0.108 | <0.001 * | 0.151 | 0.849 |
| C4_T7 | 0.012 * | 0.005 * | 0.005 * | <0.001 * | 0.382 | 0.012 * | 0.029 * | 0.054 | 0.080 | 0.605 |
| C6_T7 | <0.001 * | 0.001 * | 0.001 * | 0.017 * | 0.676 | 0.080 | 0.765 | 0.048 * | 0.917 | 0.238 |
| C7_T7 | 1.000 | 0.010 * | 1.000 | 1.000 | 0.016 * | 1.000 | 1.000 | 0.145 | 0.643 | 1.000 |
| C8_T7 | 0.007 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.089 | 0.664 | 0.345 | 0.285 |
| C9_T7 | 1.000 | 0.071 | 0.011 * | <0.001 * | 0.094 | 0.018 * | 0.270 | 0.467 | 0.410 | 0.605 |
| C10_T7 | 0.007 * | <0.001 * | <0.001 * | <0.001 * | 0.017 * | <0.001 * | 0.089 | 0.021 * | 0.482 | 0.531 |
| Overall Score | Score for N Method | Score for P Method | |
|---|---|---|---|
| p-Value | |||
| C1_T7—C1_T1 | <0.001 * | <0.001 * | <0.001 * |
| C2_T7—C2_T1 | 1.000 | 1.000 | 1.000 |
| C3_T7—C3_T1 | <0.001 * | <0.001 * | <0.001 * |
| C4_T7—C4_T1 | <0.001 * | <0.001 * | <0.001 * |
| C5_T7—C5_T1 | 1.000 | 1.000 | 1.000 |
| C6_T7—C6_T1 | <0.001 * | <0.001 * | <0.001 * |
| C7_T7—C7_T1 | 0.046 * | 1.000 | 0.046 * |
| C8_T7—C8_T1 | <0.001 * | <0.001 * | <0.001 * |
| C9_T7—C9_T1 | 0.014 * | 0.157 | 0.046 * |
| C10_T7—C10_T1 | <0.001 * | <0.001 * | 0.014 * |
| C11_T7—C11_T1 | 1.000 | 1.000 | 1.000 |
| Mean | Median | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | Estimate | Std. Error | 95% Confidence Interval | Estimate | Std. Error | 95% Confidence Interval | ||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
| Preparation method | ||||||||
| N | 10.000 | 5.036 | 0.130 | 19.870 | 2.000 | 1.061 | 0.000 | 4.079 |
| P | 2.333 | 0.211 | 1.920 | 2.747 | 2.000 | - | - | - |
| Overall | 6.714 | 2.986 | 0.862 | 12.567 | 2.000 | 0.309 | 1.395 | 2.605 |
| Maximum thickness (mm) | ||||||||
| 1.0 | 3.000 | 0.000 | 3.000 | 3.000 | 3.000 | - | - | - |
| 1.5 | 33.000 | 0.000 | 33.000 | 33.000 | 33.000 | - | - | - |
| 2.0 | 2.333 | 0.558 | 1.240 | 3.427 | 2.000 | 0.577 | 0.868 | 3.132 |
| 2.5 | 2.000 | 0.000 | 2.000 | 2.000 | 2.000 | - | - | - |
| Overall | 6.714 | 2.986 | 0.862 | 12.567 | 2.000 | 0.309 | 1.395 | 2.605 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihali, S.G.; Lolos, D.; Popa, G.; Tudor, A.; Bratu, D.C. Retrospective Long-Term Clinical Outcome of Feldspathic Ceramic Veneers. Materials 2022, 15, 2150. https://doi.org/10.3390/ma15062150
Mihali SG, Lolos D, Popa G, Tudor A, Bratu DC. Retrospective Long-Term Clinical Outcome of Feldspathic Ceramic Veneers. Materials. 2022; 15(6):2150. https://doi.org/10.3390/ma15062150
Chicago/Turabian StyleMihali, Sorin Gheorghe, Dan Lolos, George Popa, Anca Tudor, and Dana Cristina Bratu. 2022. "Retrospective Long-Term Clinical Outcome of Feldspathic Ceramic Veneers" Materials 15, no. 6: 2150. https://doi.org/10.3390/ma15062150
APA StyleMihali, S. G., Lolos, D., Popa, G., Tudor, A., & Bratu, D. C. (2022). Retrospective Long-Term Clinical Outcome of Feldspathic Ceramic Veneers. Materials, 15(6), 2150. https://doi.org/10.3390/ma15062150