
Clinical and Microbiological Evaluation of a Chlorhexidine-Modified Glass Ionomer Cement (GIC-CHX) Restoration Placed Using the Atraumatic Restorative Treatment (ART) Technique

 ,
,  ,
,  ,
,  ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
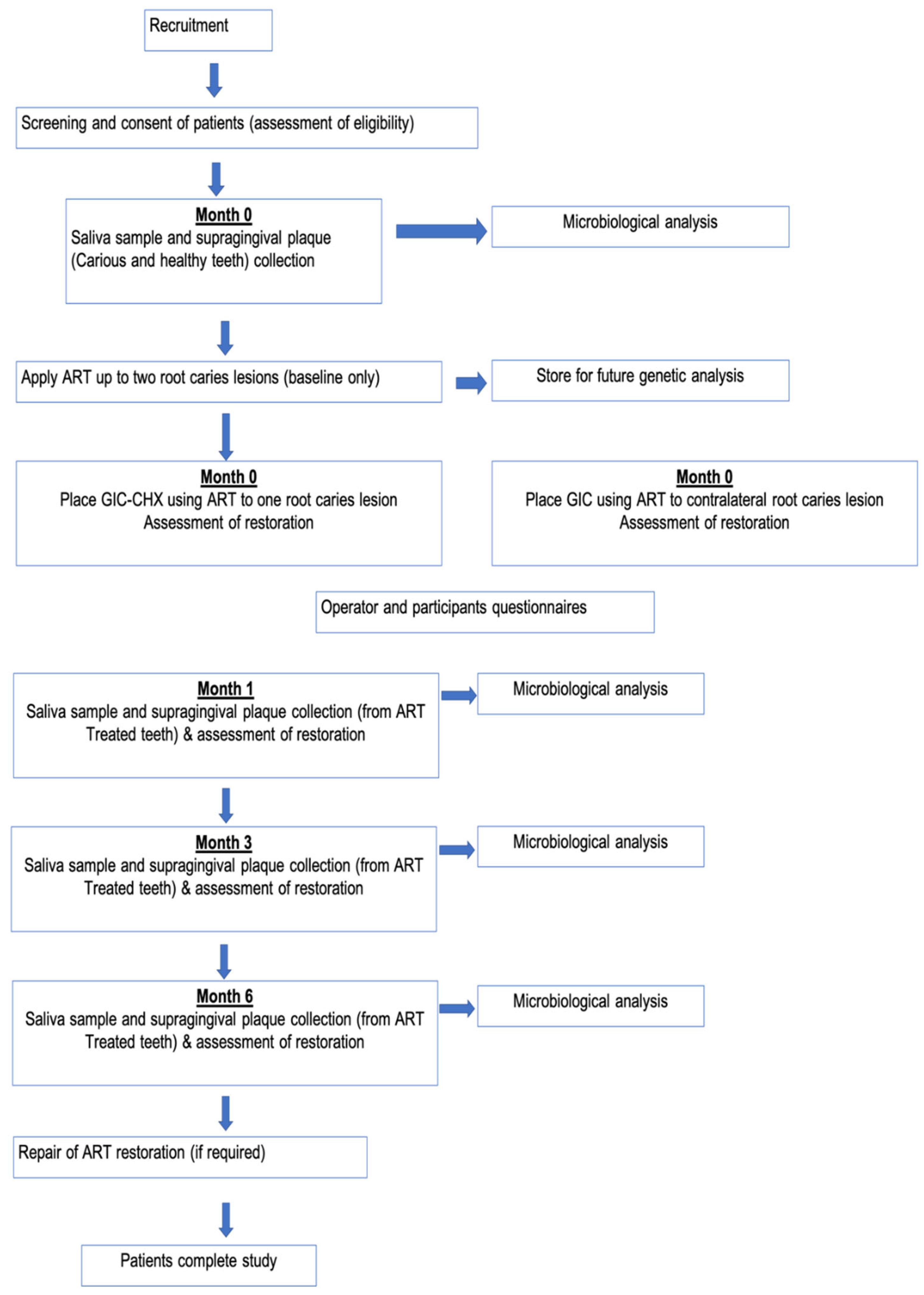
2.1. Participant Recruitment
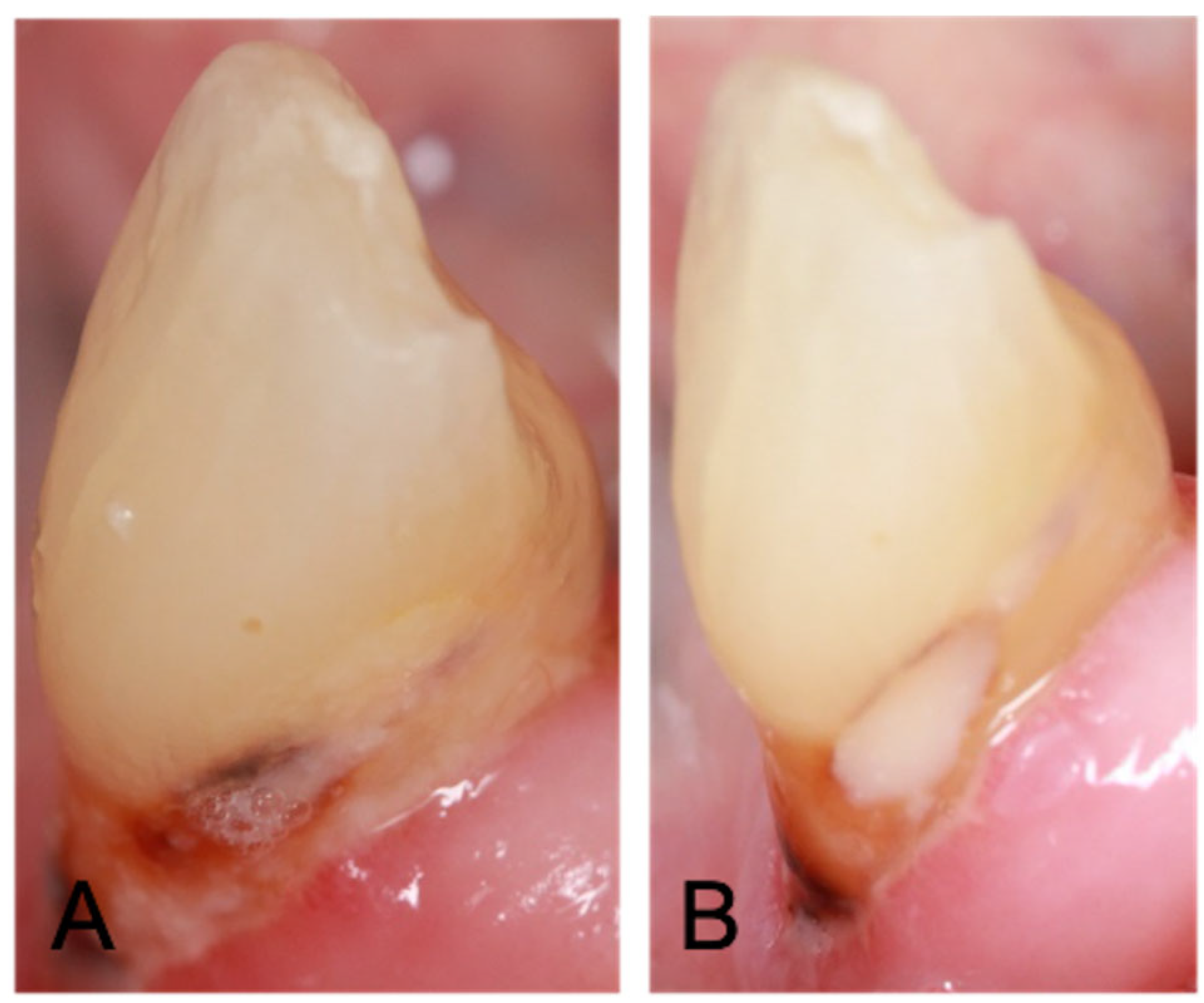
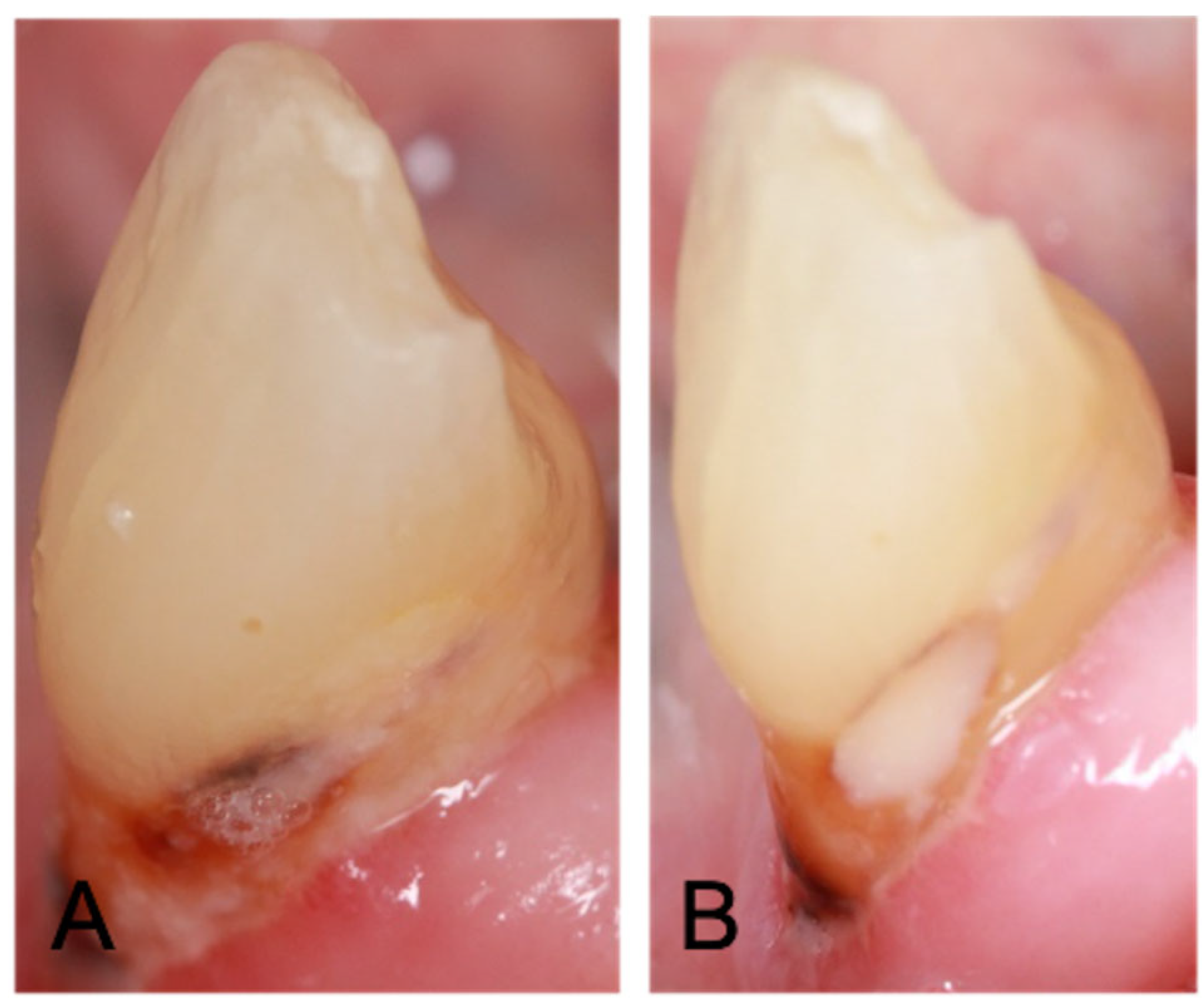
2.2. Preparation for, and Application of, GIC/GIC-CHX Restorations Using ART
2.3. Microbiological Analysis
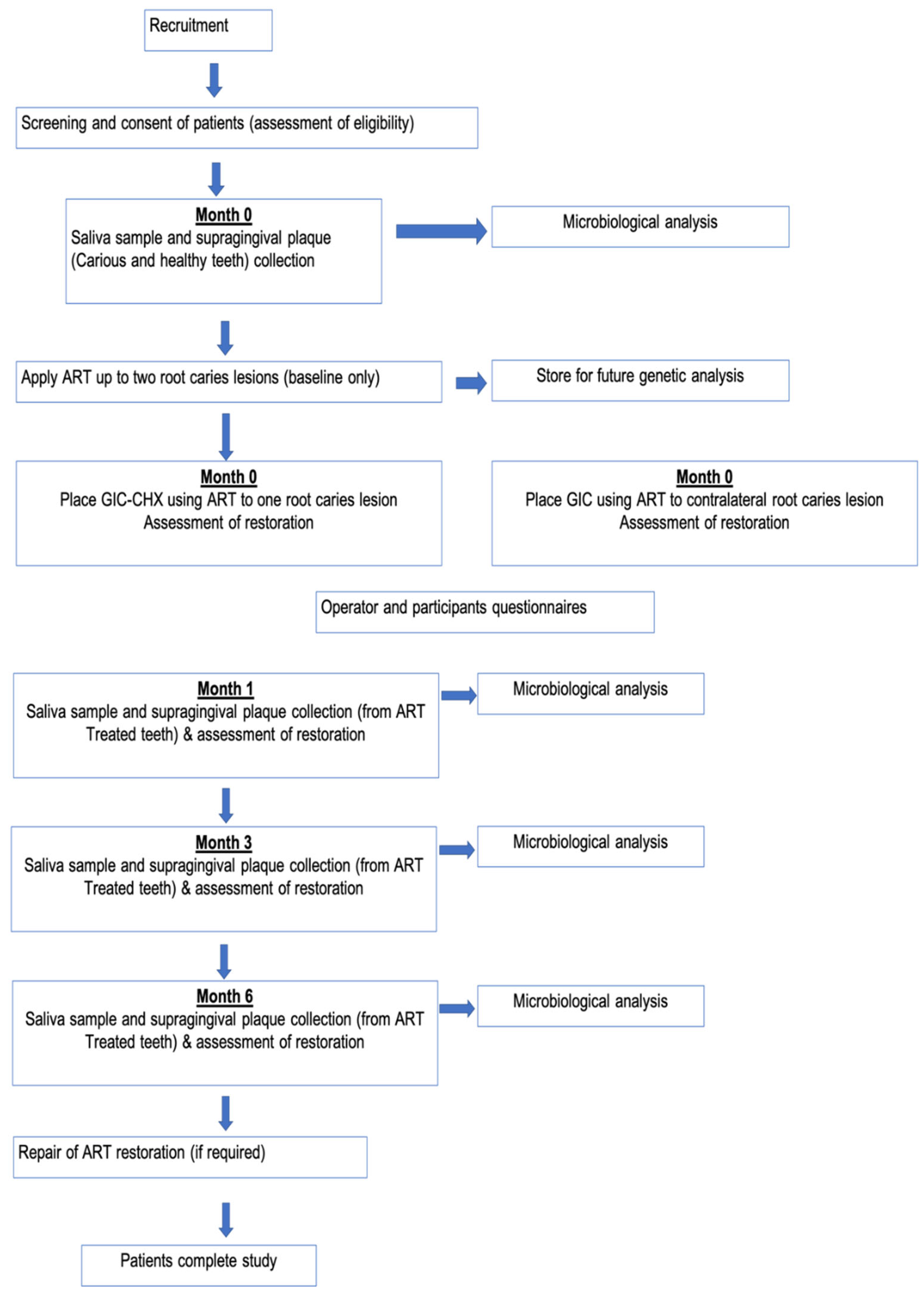
Sample Collection
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Participants
3.2. Clinical Performance and Patient-Rated Acceptability of ART
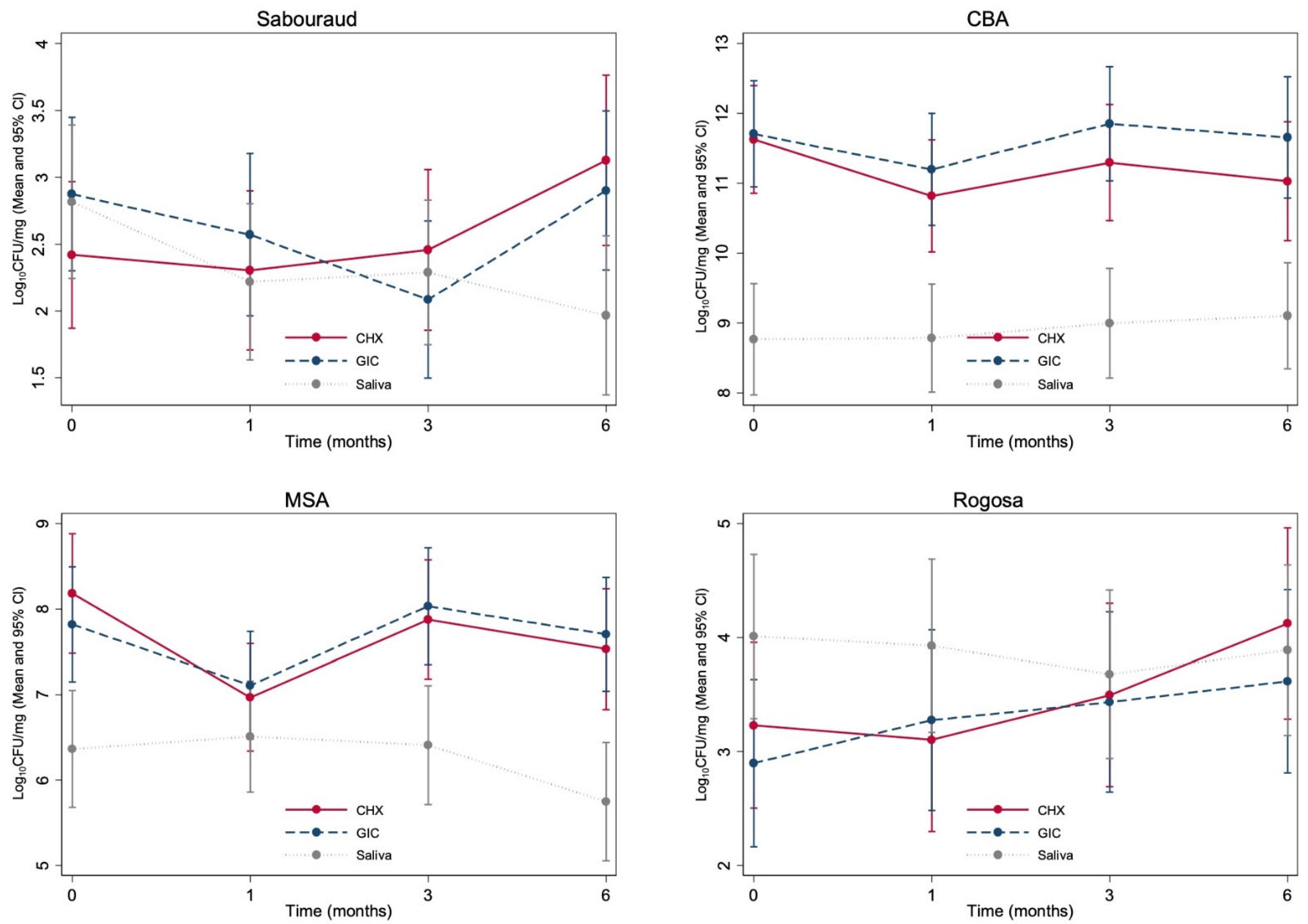
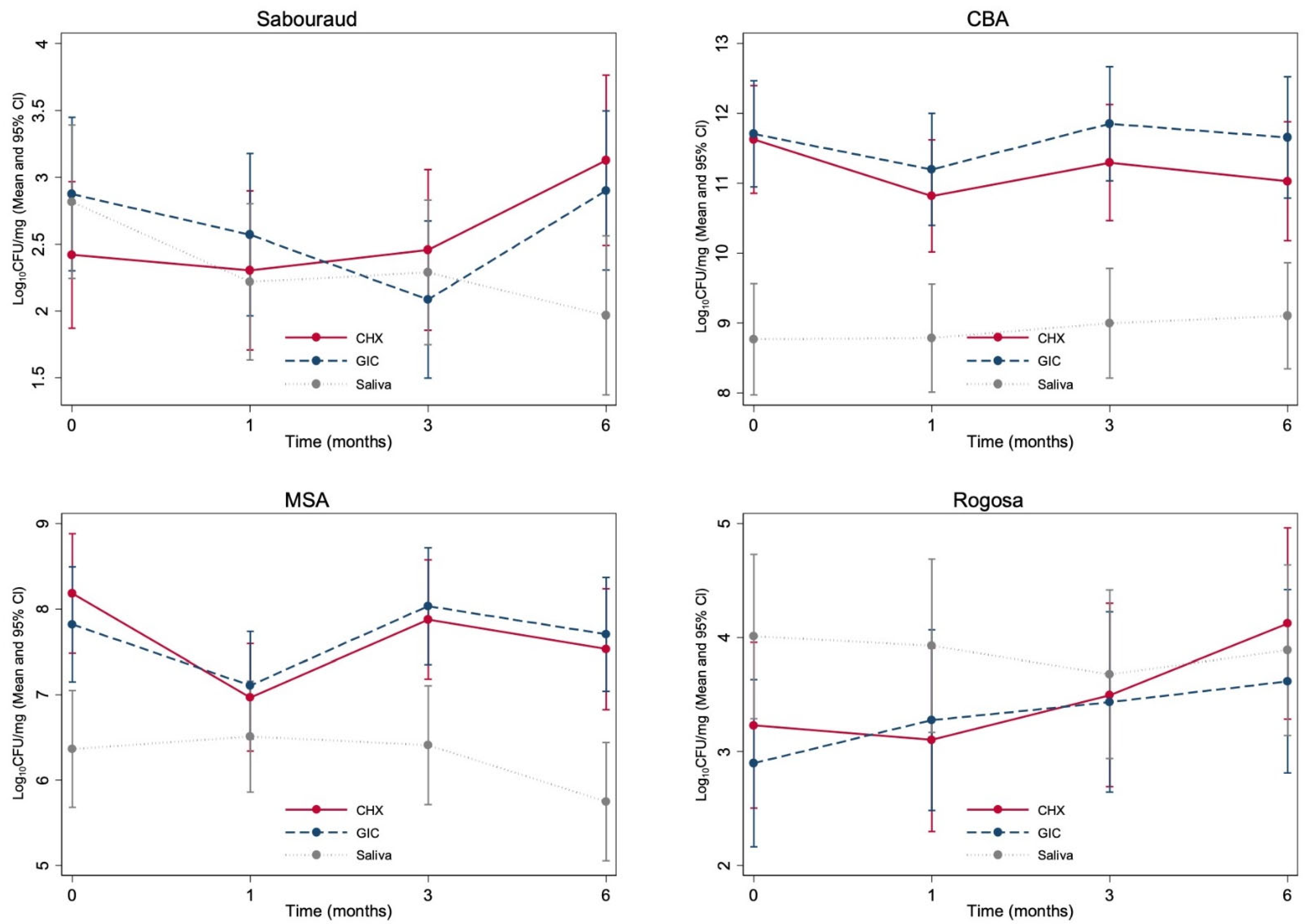
3.3. Microbiological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fontana, M.; Zero, D.T. Assessing patients’ caries risk. J. Am. Dent. Assoc. 2006, 137, 1231–1239. [Google Scholar] [CrossRef] [Green Version]
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [Green Version]
- Hellyer, P.H.; Beighton, D.; Heath, M.R.; Lynch, E.J. Root caries in older people attending a general dental practice in East Sussex. Br. Dent. J. 1990, 169, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Papas, A.S.; Joshi, A.; Belanger, A.J.; Kent, J.R.L.; Palmer, A.C.; DePaola, P.F. Dietary models for root caries. Am. J. Clin. Nutr. 1995, 61, 417S–422S. [Google Scholar] [CrossRef]
- AlQranei, M.S.; Balhaddad, A.A.; Melo, M.A.S. The burden of root caries. Gerodontology 2021, 38, 136–153. [Google Scholar] [CrossRef]
- Saunders, R.H.; Handelman, S.L. Effects of hyposalivatory medications on saliva flow rates and dental caries in adults aged 65 and older. Spéc. Care Dent. 1992, 12, 116–121. [Google Scholar] [CrossRef]
- Hu, J.Y.; Chen, X.C.; Li, Y.Q.; Smales, R.J.; Yip, K.H. Radiation-induced root surface caries restored with glassionomer cement placed in conventional and ART cavity preparations: Results at two years. Aust. Dent. J. 2005, 50, 186–190. [Google Scholar] [CrossRef] [Green Version]
- Brailsford, S.R.; Fiske, J.; Gilbert, S.; Clark, D.; Beighton, D. The effects of the combination of chlorhexidine/thymol- and fluoride-containing varnishes on the severity of root caries lesions in frail institutionalised elderly people. J. Dent. 2002, 30, 319–324. [Google Scholar] [CrossRef]
- Frencken, J.E. The Atraumatic Restorative Treatment (ART) approach can improve oral health for the elderly; myth or reality? Gerodontology 2014, 31, 81–82. [Google Scholar] [CrossRef]
- Nyvad, B.; Fejerskov, O. Active root surface caries converted into inactive caries as a response to oral hygiene. Eur. J. Oral Sci. 1986, 94, 281–284. [Google Scholar] [CrossRef]
- Smales, R.J.; Yip, H.-K. The atraumatic restorative treatment (ART) approach for the management of dental caries. Quintessence Int. 2002, 33, 427–432. [Google Scholar]
- Innes, N.; Stewart, M.; Souster, G.; Evans, D. The Hall Technique; retrospective case-note follow-up of 5-year RCT. Br. Dent. J. 2015, 219, 395–400. [Google Scholar] [CrossRef]
- Frencken, J.E.; Hof, M.A.V.; Taifour, D.; Al-Zaher, I. Effectiveness of ART and traditional amalgam approach in restoring single-surface cavities in posterior teeth of permanent dentitions in school children after 6.3 years. Community Dent. Oral Epidemiol. 2007, 35, 207–214. [Google Scholar] [CrossRef]
- Mickenautsch, S.; Yengopal, V.; Banerjee, A. Atraumatic restorative treatment versus amalgam restoration longevity: A systematic review. Clin. Oral Investig. 2010, 14, 233–240. [Google Scholar] [CrossRef]
- da Mata, C.; Allen, P.F.; Cronin, M.; O’Mahony, D.; McKenna, G.; Woods, N. Cost-effectiveness of ART restorations in elderly adults: A randomized clinical trial. Commun. Dent. Oral Epidemiol. 2014, 42, 79–87. [Google Scholar] [CrossRef]
- Frencken, J.E.; Leal, S.C.; Navarro, M.F. Twenty-five-year atraumatic restorative treatment (ART) approach: A comprehensive overview. Clin. Oral Investig. 2012, 16, 1337–1346. [Google Scholar] [CrossRef] [Green Version]
- Jedrychowski, J.R.; Caputo, A.A.; Kerper, S. Antibacterial and mechanical properties of restorative materials combined with chlorhexidines. J. Oral Rehabil. 1983, 10, 373–381. [Google Scholar] [CrossRef]
- Millett, D.T.; Doubleday, B.; Alatsaris, M.; Love, J.; Wood, D.; Luther, F.; Devine, D. Chlorhexidine-modified glass ionomer forbandcementation? An in vitro study. J Orthodont. 2005, 32, 36–42. [Google Scholar] [CrossRef]
- Takahashi, Y.; Imazato, S.; Kaneshiro, A.V.; Ebisu, S.; Frencken, J.E.; Tay, F.R. Antibacterial effects and physical properties of glass-ionomer cements containing chlorhexidine for the ART approach. Dent. Mater. 2006, 22, 647–652. [Google Scholar] [CrossRef]
- Türkün, L.S.; Türkün, M.; Ertug˘rul, F.; Ates¸, M.; Brugger, S. Long-Term Antibacterial Effects and Physical Properties of a Chlorhexidine-Containing Glass Ionomer Cement. J. Esthet. Restor. Dent. 2008, 20, 29–44. [Google Scholar] [CrossRef]
- Souza, M.; Cecchin, D.; Farina, A.P.; Leite, C.E.; Cruz, F.F.; Pereira, C.D.C.; Ferraz, C.; Figueiredo, J.A.P. Evaluation of Chlorhexidine Substantivity on Human Dentin: A Chemical Analysis. J. Endod. 2012, 38, 1249–1252. [Google Scholar] [CrossRef]
- Frencken, J.E.; Pilot, T.; Songpaisan, Y.; Phantumvanit, P. Atraumatic Restorative Treatment (ART): Rationale, Technique, and Development. J. Public Heal. Dent. 1996, 56, 135–140. [Google Scholar] [CrossRef]
- Ryge, G. Clinical criteria. Int. Dent. J. 1980, 30, 347–358. [Google Scholar] [PubMed]
- Honkala, S. Atraumatic dental treatment among Finnish elderly persons. J. Oral Rehabil. 2002, 29, 435–440. [Google Scholar] [CrossRef]
- Lo, E.; Luo, Y.; Tan, H.; Dyson, J.; Corbet, E. ART and conventional root restorations in elders after 12 months. J. Dent. Res. 2006, 85, 929–932. [Google Scholar] [CrossRef]
- Olson, H.; Ratnayake, J.; Veerasamy, A.; Quaranta, A.; Meldrum, A. Working characteristics for practising dental hygienists in two countries in different hemispheres. Int. J. Dent. Hyg. 2021, 20, 209–218. [Google Scholar] [CrossRef]
- Loch, C.; Ratnayake, J.; Veerasamy, A.; Cathro, P.; Lee, R.; Brunton, P. Direct Restorations, Endodontics, and Bleaching: Materials and Techniques Used by General Dentists of New Zealand. Int. J. Dent. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Mickenautsch, S.; Frencken, J.E.; Hof, M.A.V. Atraumatic Restorative Treatment and Dental Anxiety in Outpatients Attending Public Oral Health Clinics in South Africa. J. Public Health Dent. 2007, 67, 179–184. [Google Scholar] [CrossRef]
- Frencken, J.E.; Holmgren, C.J. How effective is ART in the management of dental caries? Community Dent. Oral Epidemiol. 1999, 27, 423–430. [Google Scholar] [CrossRef]
- Lang, N.P.; Catalanotto, F.A.; Knöpfli, R.U.; Antczak, A.A.A. Quality-specific taste impairment following the application of chlorhexidine digluconate mouthrinses. J. Clin. Periodontol. 1988, 15, 43–48. [Google Scholar] [CrossRef]
- Crisp, S.; Lewis, B.; Wilson, A. Characterization of glass-ionomer cements: 2. Effect of the powder: Liquid ratio on the physical properties. J. Dent. 1976, 4, 287–290. [Google Scholar] [CrossRef]
- Pereira, P.; Inokoshi, S.; Tagami, J. In vitro secondary caries inhibition around fluoride releasing materials. J. Dent. 1998, 26, 505–510. [Google Scholar] [CrossRef]
- de Castilho, A.R.F.; Duque, C.; de Cássia Negrini, T.; Sacono, N.T.; de Paula, A.B.; de Souza Costa, C.A.; Spolidóriod, D.M.P.; Puppin-Rontaniae, R.M. In vitro and in vivo investigation of the biological and mechanical behaviour of resin-modified glass-ionomer cement containing chlorhexidine. J. Dent. 2013, 41, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Marti, L.M.; Da Mata, M.; Ferraz-Santos, B.; Azevedo, E.R.; Giro, E.M.A.; Zuanon, A.C.C. Addition of Chlorhexidine Gluconate to a Glass Ionomer Cement: A Study on Mechanical, Physical and Antibacterial Properties. Braz. Dent. J. 2014, 25, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Palmer, G.; Jones, F.; Billington, R.; Pearson, G. Chlorhexidine release from an experimental glass ionomer cement. Biomaterials 2004, 25, 5423–5431. [Google Scholar] [CrossRef]
- Hoszek, A.; Ericson, D. In Vitro Fluoride Release and the Antibacterial Effect of Glass Ionomers Containing Chlorhexidine Gluconate. Oper. Dent. 2008, 33, 696–701. [Google Scholar] [CrossRef] [Green Version]
- Lear, C.; Flanagan, J.; Moorrees, C. The frequency of deglutition in man. Arch. Oral Biol. 1965, 10, 83. [Google Scholar] [CrossRef]
- Du, X.; Huang, X.; Huang, C.; Frencken, J.; Yang, T. Inhibition of early biofilm formation by glass-ionomer incorporated with chlorhexidine in vivo: A pilot study. Aust. Dent. J. 2012, 57, 58–64. [Google Scholar] [CrossRef]
- Palenik, C.; Behnen, M.; Setcos, J.; Miller, C. Inhibition of microbial adherence and growth by various glass ionomers in vitro. Dent. Mater. 1992, 8, 16–20. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Age | ||
| <30 | 2 | 8 |
| 50–59 | 6 | 23 |
| 60–69 | 10 | 38 |
| >70 | 8 | 31 |
| Gender | ||
| Male | 16 | 62 |
| Female | 10 | 38 |
| Ethnicity | ||
| New Zealand European | 18 | 69 |
| Māori | 3 | 12 |
| Asian | 1 | 4 |
| Other | 4 | 15 |
| Smoking status | ||
| Former smoker | 11 | 42 |
| Never smoked | 11 | 42 |
| Current smoker | 4 | 15 |
| Frequency of toothbrushing | ||
| Irregular | 2 | 8 |
| Regular: once a day | 11 | 42 |
| Regular: twice a day | 13 | 50 |
| n | % | |
|---|---|---|
| How comfortable was the ART? | ||
| Very comfortable | 14 | 54 |
| Comfortable | 10 | 38 |
| Neutral | 0 | 0 |
| Uncomfortable | 2 | 8 |
| Very Uncomfortable | 0 | 0 |
| How much pain did you feel during the ART? | ||
| None | 16 | 62 |
| A little pain | 10 | 38 |
| A lot of pain | 0 | 0 |
| How anxious did you feel during the ART? | ||
| Not at all anxious | 24 | 92 |
| A little anxious | 2 | 8 |
| Very anxious | 0 | 0 |
| How anxious did you feel during your clinical visit? | ||
| Not at all anxious | 21 | 81 |
| A little anxious | 5 | 19 |
| Very anxious | 0 | 0 |
| How much time did you feel that the ART procedure took? | ||
| Less than expected | 2 | 8 |
| As expected | 11 | 42 |
| More than expected | 13 | 50 |
| How confident were you that the dentist was able to apply the treatment? | ||
| Very confident | 19 | 73 |
| Confident | 7 | 27 |
| Neutral | 0 | 0 |
| Unconfident | 0 | 0 |
| Very unconfident | 0 | 0 |
| How satisfied are you with the appearance of the ART treatment of your tooth? | ||
| Very satisfied | 10 | 38 |
| Satisfied | 15 | 58 |
| Neutral | 1 | 4 |
| Dissatisdfied | 0 | 0 |
| n | % | |
|---|---|---|
| How smooth does your treated tooth feel compared to your other teeth? | ||
| Very smooth | 7 | 28 |
| Quite smooth | 9 | 36 |
| Neutral | 7 | 28 |
| A little rough | 2 | 8 |
| Very rough | 0 | 0 |
| How much pain did you have in your tooth/teeth following ART treatment? | ||
| None | 23 | 92 |
| A little pain | 2 | 8 |
| A lot of pain | 0 | 0 |
| How anxious did you feel throughout your clinical visit? | ||
| Not at all anxious | 25 | 100 |
| A little anxious | 0 | 0 |
| Very anxious | 0 | 0 |
| How satisfied are you with the appearance of the ART treatment on your tooth/teeth? | ||
| Very satisfied | 11 | 44 |
| Satisfied | 10 | 40 |
| Neutral | 4 | 16 |
| Unsatisfied | 0 | 0 |
| Very unsatisfied | 0 | 0 |
| Have you experienced any taste change since receiving treatment? | ||
| None | 24 | 96 |
| A little change | 1 | 4 |
| A lot of change | 0 | 0 |
| n | % | |
|---|---|---|
| How easy was the ART procedure? | ||
| Very easy | 9 | 35 |
| Quite easy | 12 | 46 |
| Neutral | 4 | 15 |
| Quite difficult | 1 | 4 |
| Very difficult | 0 | 0 |
| How long did the procedure take? | ||
| Less than expected | 5 | 19 |
| As expected | 14 | 54 |
| More than expected | 7 | 27 |
| How satisfied are you with the appearance of the restoration following the ART treatment? | ||
| Very satisfied | 7 | 27 |
| Satisfied | 14 | 54 |
| Neutral | 4 | 15 |
| Unsatisfied | 1 | 4 |
| Very unsatisfied | 0 | 0 |
| Time taken for GIC-CHX to set | ||
| Quicker than GIC | 8 | 31 |
| Same as GIC | 14 | 54 |
| Longer than GIC | 4 | 15 |
| How satisfied are you with the appearance of the patient’s tooth? | p-value | ||||
|---|---|---|---|---|---|
| GIC | GIC-CHX | 0.995 * | |||
| n | % | n | % | ||
| Very satisfied | 4 | 16 | 4 | 16 | |
| Satisfied | 13 | 52 | 13 | 52 | |
| Neutral | 5 | 20 | 7 | 28 | |
| Unsatisfied | 1 | 4 | 0 | 0 | |
| Very unsatisfied | 2 | 8 | 1 | 4 | |
| How satisfied are you with the condition of the patient’s tooth? | p-value | ||||
| GIC | GIC-CHX | 0.899 * | |||
| n | % | n | % | ||
| Very satisfied | 3 | 12 | 3 | 12 | |
| Satisfied | 16 | 64 | 16 | 64 | |
| Neutral | 4 | 16 | 3 | 12 | |
| Unsatisfied | 0 | 0 | 2 | 8 | |
| Very unsatisfied | 2 | 8 | 1 | 1 | |
| 1st Operator | 2nd Operator | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | p-Value | 6 Months | p-Value | 6 Months | p-Value | ||||||||||
| GIC | GIC-CHX | GIC | GIC CHX | GIC | GIC CHX | ||||||||||
| Anatomic form | n | % | n | % | n | % | n | % | n | % | n | % | |||
| The restoration is continuous with the existing anatomic form | 24 | 96 | 25 | 100 | 1 * | 16 | 64 | 17 | 68 | 1 * | 19 | 76 | 22 | 88 | 0.453 |
| Slightly under/over contoured | 1 | 4 | 0 | 0 | 9 | 36 | 8 | 32 | 6 | 24 | 3 | 12 | |||
| Secondary caries | |||||||||||||||
| No visible evidence | 25 | 100 | 25 | 100 | 1 * | 23 | 92 | 25 | 100 | 0.5 * | 25 | 100 | 25 | 100 | 1 |
| Visible evidence | 0 | 0 | 0 | 0 | 2 | 8 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| Marginal adaptation | |||||||||||||||
| Continuous with existing anatomic form | 23 | 92 | 23 | 92 | 1 ** | 6 | 24 | 12 | 48 | 0.036 ** | 7 | 28 | 14 | 56 | 0.098 |
| Explorer catches but no crevice visible | 2 | 8 | 2 | 8 | 9 | 36 | 11 | 44 | 13 | 52 | 9 | 36 | |||
| Obvious crevice at margin, dentine or lute exposed | 0 | 0 | 0 | 10 | 40 | 2 | 8 | 5 | 20 | 2 | 8 | ||||
| Surface roughness | |||||||||||||||
| Smooth | 21 | 84 | 20 | 80 | 1 ** | 4 | 16 | 15 | 60 | 0.002 ** | 14 | 56 | 15 | 60 | 1 |
| Slightly rough | 4 | 16 | 5 | 20 | 19 | 76 | 10 | 40 | 11 | 44 | 10 | 40 | |||
| Rough | 0 | 0 | 0 | 0 | 2 | 8 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| Colour match | |||||||||||||||
| Very good/good almost invisible | 20 | 80 | 10 | 40 | 0.002 ** | 16 | 64 | 21 | 84 | 0.227 ** | 25 | 100 | 21 | 86 | 0.125 |
| Slightly mismatch | 5 | 20 | 14 | 56 | 9 | 36 | 4 | 16 | 0 | 0 | 4 | 14 | |||
| Gross mismatch outside of normal range | 0 | 0 | 1 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| Gingival health | |||||||||||||||
| Healthy gingivae | 13 | 52 | 5 | 20 | 0.112 *** | 7 | 28 | 16 | 64 | 0.006 *** | 0 | 0 | 0 | 0 | 0.022 |
| Mild inflammation | 6 | 24 | 12 | 48 | 13 | 52 | 9 | 36 | 8 | 32 | 15 | 60 | |||
| Moderate inflammation | 5 | 20 | 8 | 32 | 5 | 20 | 0 | 0 | 15 | 60 | 10 | 40 | |||
| Severe inflammation | 1 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 8 | 0 | 0 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratnayake, J.; Veerasamy, A.; Ahmed, H.; Coburn, D.; Loch, C.; Gray, A.R.; Lyons, K.M.; Heng, N.C.K.; Cannon, R.D.; Leung, M.; et al. Clinical and Microbiological Evaluation of a Chlorhexidine-Modified Glass Ionomer Cement (GIC-CHX) Restoration Placed Using the Atraumatic Restorative Treatment (ART) Technique. Materials 2022, 15, 5044. https://doi.org/10.3390/ma15145044
Ratnayake J, Veerasamy A, Ahmed H, Coburn D, Loch C, Gray AR, Lyons KM, Heng NCK, Cannon RD, Leung M, et al. Clinical and Microbiological Evaluation of a Chlorhexidine-Modified Glass Ionomer Cement (GIC-CHX) Restoration Placed Using the Atraumatic Restorative Treatment (ART) Technique. Materials. 2022; 15(14):5044. https://doi.org/10.3390/ma15145044
Chicago/Turabian StyleRatnayake, Jithendra, Arthi Veerasamy, Hassan Ahmed, David Coburn, Carolina Loch, Andrew R. Gray, Karl M. Lyons, Nicholas C. K. Heng, Richard D. Cannon, Marcus Leung, and et al. 2022. "Clinical and Microbiological Evaluation of a Chlorhexidine-Modified Glass Ionomer Cement (GIC-CHX) Restoration Placed Using the Atraumatic Restorative Treatment (ART) Technique" Materials 15, no. 14: 5044. https://doi.org/10.3390/ma15145044
APA StyleRatnayake, J., Veerasamy, A., Ahmed, H., Coburn, D., Loch, C., Gray, A. R., Lyons, K. M., Heng, N. C. K., Cannon, R. D., Leung, M., & Brunton, P. A. (2022). Clinical and Microbiological Evaluation of a Chlorhexidine-Modified Glass Ionomer Cement (GIC-CHX) Restoration Placed Using the Atraumatic Restorative Treatment (ART) Technique. Materials, 15(14), 5044. https://doi.org/10.3390/ma15145044