
Assessment of Conventionally and Digitally Fabricated Complete Dentures: A Comprehensive Review

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Literature Review
2.1. Data Collection
2.2. History of CAD/CAM
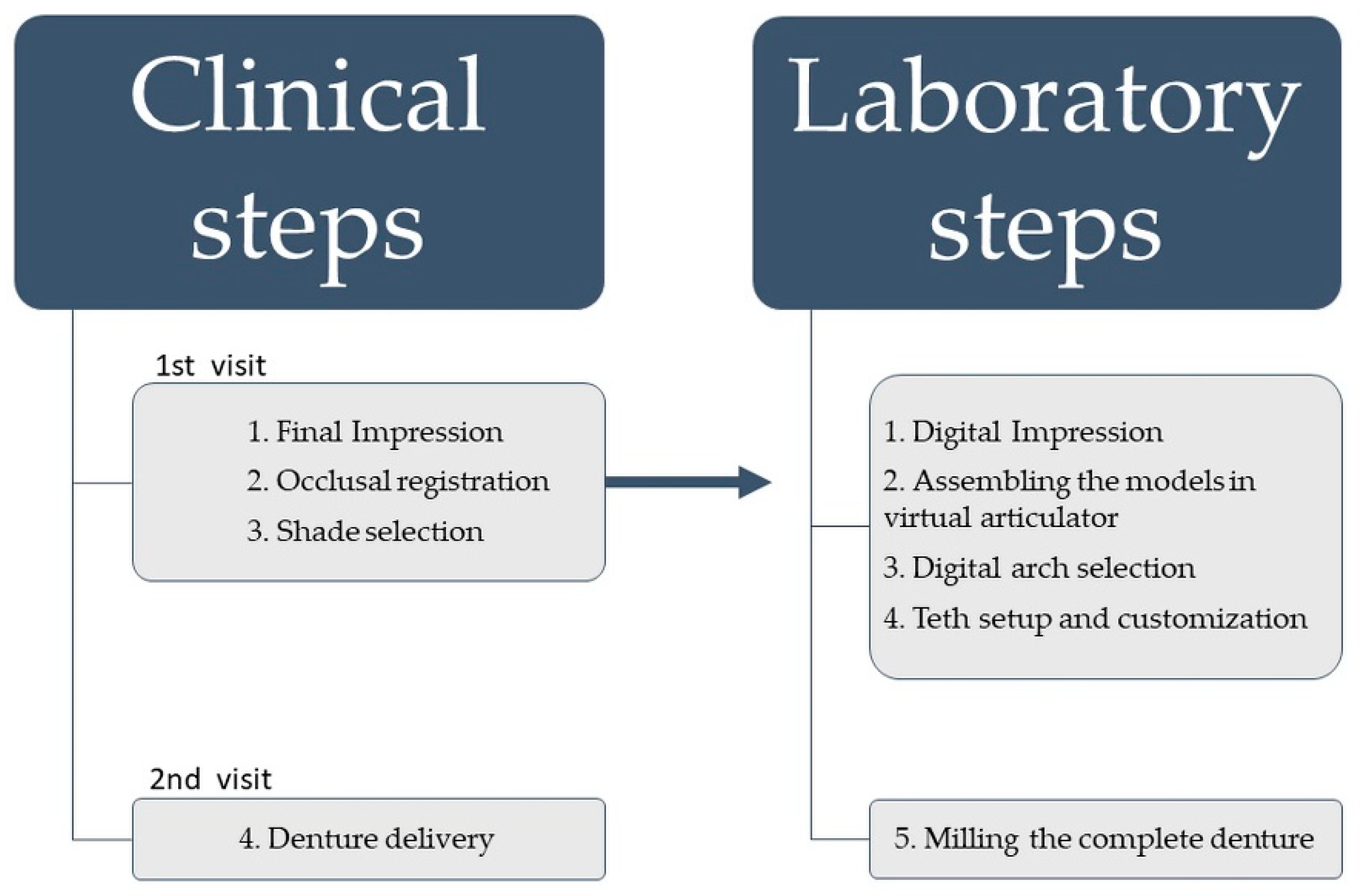
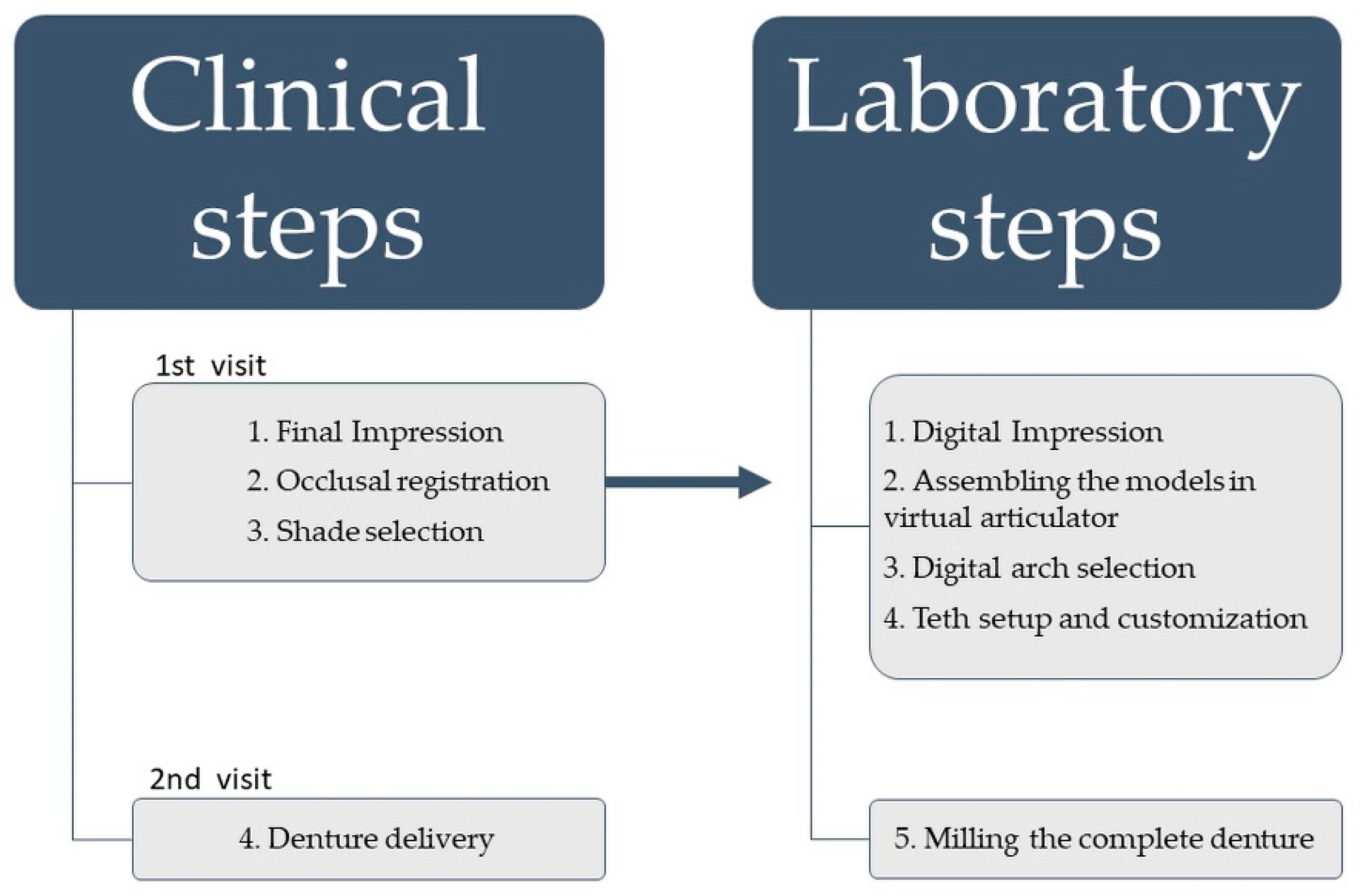
2.3. Manufacturing of Computer-Engineered Complete Dentures
2.4. Fabrication of Conventional Complete Dentures
3. Results
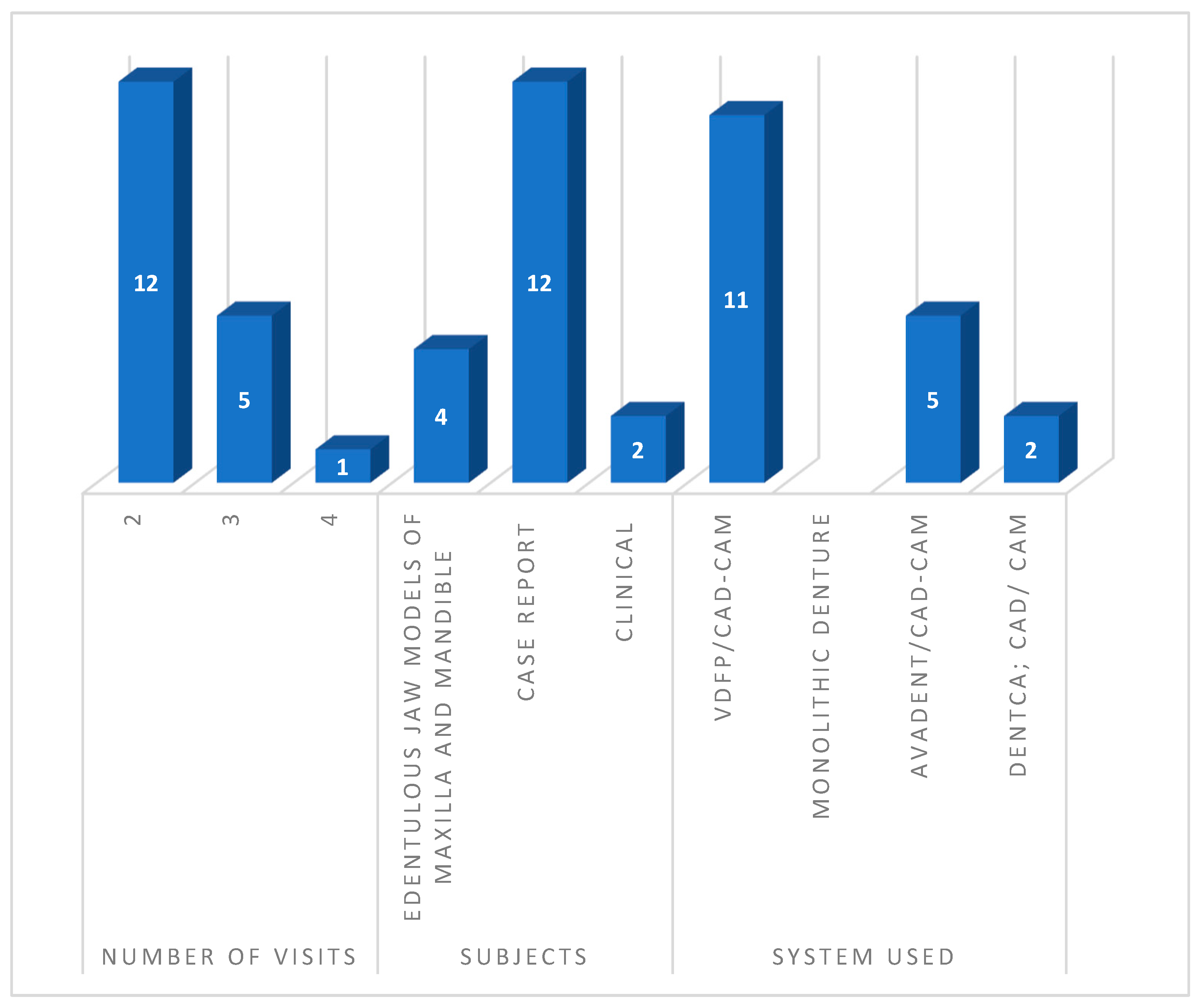
3.1. Study Selection and Collections

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) /Year/ Study Type | Country/Number of Visits | Subjects | Technique | Findings |
|---|---|---|---|---|
| Mai et al., 2020/Cast Model study [13] | Republic of Korea/ 2 Visits | Edentulous Jaw Models of Maxilla and Mandible | VDFP */CAD-CAM * | Base and dental parts of new dentures were designed efficiently and predictably. Digital protocol facilitates the design process, border seal, and tooth arrangement. |
| Srinivasan, 2019 /Case report [37] | Switzerland/ 3 Visits | Male/65 years/Maxillary and Mandibular CD * | VDFP */Anatomic Measuring Device (AMD *) AvaDent/CAD-CAM * | Production of clinically acceptable CECDs reduced the number of clinical visits without the use of complex equipment. |
| Male/71 years/Maxillary and Mandibular Resin RPD | ||||
| Lee et al., 2019/ Case report [15] | Korea/ 2 Visits | Male/53 years/Maxillary and Mandibular CD * | VDFP */CAD-CAM * | Addition of conventional impression and maxillomandibular relationship with laboratory steps using CAD-CAM * technology. Minimized the clinical time. |
| Goodacre et al., 2018/Case report [38] | USA/ 2 Visits | Male/78 years/Maxillary CD * and Mandibular Overdenture by Dental Implants | VDFP */Anatomic Measuring Device (AMD *) AvaDent/CAD-CAM * | Intraoral scanning captured true mucostatic impression, achieving good retention and stability of the CECD prostheses. Digitally recording tooth location and base morphology of the present dentures reduced the number of clinical steps and eliminated the need to transport conventional impressions to the laboratory. |
| Contrepois et al., 2018/Case report [16] | France/ 2 Visits | Female/78 years/Maxillary and Mandibular CD * | VDFP */CAD-CAM * | Designing the shape of the teeth for each patient results in better denture customization as well as the appropriate level of tooth staining and an appropriate denture base. Full CECD fabrication ensured a good aesthetic result. |
| Janeva et al., 2017/Case report [17] | Macedonia/ 3 Visits | Male/63 years/Maxillary and Mandibular CD * | VDFP */Anatomic Measuring Device (AMD *) AvaDent/CAD-CAM * | Combined advantages of CAD/CAM * and traditional clinical recording methods. CAD/CAM * technology eliminated many laboratory steps and simplified the process. |
| Ohkubo et al., 2017/Case report [18] | Japan/ 2 Visits | Female/82 years/Maxillary and Mandibular CD * | VDFP */DENTCA Piezography Technique CAD-CAM * | Concept of neutral zone and denture space were verified, and denture teeth and flange forms were appropriately designed. |
| AlHelal et al., 2017/ Case report [39] | Saudi Arabia/ 2 Visits | Male/20-Maxillary CD * | VDFP */CAD-CAM * Monolithic Denture | CECDs minimized the number of appointments, enhanced fitting, and retention, and allowed automated archiving. |
| Yilmaz et al., 2017/ Cast Model study [12] | Turkey/ 2 Visits | Edentulous Jaw Models of Maxilla and Mandible | VDFP */CAD-CAM * | CECDs do not optimally assess maxillomandibular relationships, maxillary incisal edge placement, and lip support. Creating a mandibular occlusal plane was not possible and resulted in higher costs. |
| Bajunaid SO /2016/Case report [10] | Saudi Arabia/ 2 Visits | Female/67 years/Maxillary CD * and Mandibular Complete Overdenture | VDFP */CAD-CAM * | Excellent denture base contact, which reduced the number of required dental appointments. Unsatisfactory aesthetic outcomes can be corrected with more experience. Authors recommended the use of this technique in dental school for all levels of study. |
| de Mendonça et al., 2016/Case report [19] | Brazil/ 3 Visits | Female/63 years/Maxillary CD * and Mandibular Complete Overdenture | VDFP */Prototype then 3D CAD-CAM * | CECDs eliminate acrylic base shrinkage and decreased porosity compared to conventionally processed dentures. CECDs decreased the retention of Candida albicans. Posteriorly, teeth modified and merged into milled sockets with a milled base. |
| Kim et al., 2016/Case report [20] | Republic Korea/3 Visits | Male/75 years/Maxillary and Mandibular CD * | VDFP */Dentca; CAD/CAM * | Dentures were delivered during 2nd visit with a reduction in the number of clinical and laboratory steps. Clinically acceptable CECDs with smooth surfaces. |
| Female/61 years/Maxillary and Mandibular CD * | ||||
| Joda et al., 2016/Case report [25] | Switzerland/ 4 Visits | Male/75 years/Maxillary and Mandibular CD * Patient with dental implants | VDFP */Digital Denture Provisional (DDP) CAD-CAM * | Virtually designed and monolithic milled structure. Patient benefits from time and cost savings. Digitalization technique is ideal for planning and provisional steps. |
| Bilgin et al., 2015/Cast Model study [21] | Turkey/ 3 Visits | Edentulous Jaw Models of Maxilla and Mandible | One-set aligned Artificial tooth System CAD- CAM * and Rapid Prototyping (RP) | CAD/CAM * and RP reduce chair time. Achieved self-designed aesthetics, occlusion, and increased durability. Good for single CD * opposed natural dentition fabricated using RP or CAD/CAM *. |
| Bidra et al., 2016/Clinical Study [22] | Canada/ 2 Visits | 10 Maxillary CD * or Implant-Retained Overdentures | VDFP */CAD-CAM * Monolithic Denture | All dentures in a good state after a 12-months follow-up. Retention loss and excessive tooth wear were observed in five cases. Higher patient satisfaction (79%) regarding their CECDs. |
| Canada/ 2 Visits | 10 Mandibular Complete or Implant-Retained Overdentures | |||
| Infante et al., 2014/Case report [23] | USA/ 2 Visits | Male/62 years/Maxillary and Mandibular CD * | VDFP */Anatomic Measuring Device (AMD *) AvaDent/CAD-CAM * | Used AMD * clinical records during a one-step appointment. AMD * device allowed the collection of all of the necessary clinical information Virtual denture was milled without the use of stone models and processing. |
| Kattadiyil et al., 2013/Case report [40] | USA/ 2 Visits | Female/56 years/Maxillary and Mandibular CD * | VDFP */Anatomic Measuring Device (AMD *) AvaDent/CAD-CAM * | Final impressions for both arches, border molding, jaw relationship, and tooth arrangements were made in the first appointment. Less clinical time was required. Polymerization shrinkage was eliminated. |
| USA/ 2 Visits | Male/54 year/Maxillary and Mandibular CD * | VDFP */Dentca CAD/CAM * | ||
| Kanazawa et al., 2011/Cast Model study [24] | Japan/ 2 Visits | Edentulous Jaw Models of Maxilla and Mandible | VDFP */CAD-CAM * Monolithic Denture | Dental 3D CBCT * used to process the 3D STL morphological file for the artificial teeth. CD * manufacturing using CAD/CAM * caused large deviations between manufactured teeth and sockets on the prostheses base. |
3.2. Study Characteristics and Quality of the Reports
3.3. Synthesis of Results
4. Discussion
4.1. Retention and Fitting
4.2. Denture Surface Quality
4.3. Clinical Time
4.4. Patient Satisfaction
4.5. Manufacturing Time
4.6. Materials Selection
4.7. Complementary Aspects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferro, K.J.; Morgano, S.M.; Driscoll, C.F.; Freilich, M.A.; Guckes, A.D.; Knoernschild, K.L.; McGarry, T.J.; Twain, M. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [Google Scholar] [CrossRef] [Green Version]
- Grant, G.T.; Campbell, S.D.; Masri, R.M.; Andersen, M.R. American College of Prosthodontists Digital Dentistry Glossary Development Task, F. Glossary of Digital Dental Terms: American College of Prosthodontists. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2016, 25 (Suppl. 2), S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Bahman, A.; Ianuzzo, F. Computer-aided engineering simulations. In Wide Bandgap Power Semiconductor Packaging; Woodhead Publishing: Sawston, UK, 2018; pp. 199–223. [Google Scholar]
- Kattadiyil, M.T.; AlHelal, A. An update on computer-engineered complete dentures: A systematic review on clinical outcomes. J. Prosthet. Dent. 2017, 117, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Heikal, M.M.A.; Nabi, N.A.; Elkerdawy, M.W. A Study Comparing Patient Satisfaction and Retention of CAD/CAM Milled Complete Dentures and 3D Printed CAD/CAM Complete Dentures versus Conventional Complete Dentures: A Randomized Clinical Trial. Braz. Dent. Sci. 2022, 25, e2785. [Google Scholar] [CrossRef]
- Han, W.; Li, Y.; Zhang, Y.; Lv, Y.; Zhang, Y.; Hu, P.; Liu, H.; Ma, Z.; Shen, Y. Design and fabrication of complete dentures using CAD/CAM technology. Medicine 2017, 96, e5435. [Google Scholar] [CrossRef]
- Masri, G.; Mortada, R.; Ounsi, H.; Alharbi, N.; Boulos, P.; Salameh, Z. Adaptation of Complete Denture Base Fabricated by Conventional, Milling, and 3-D Printing Techniques: An In Vitro Study. J. Contemp. Dent. Pract. 2020, 21, 367–371. [Google Scholar]
- Gherlone, E.F.; Ferrini, F.; Crespi, R.; Gastaldi, G.; Capparé, P. Digital Impressions for Fabrication of Definitive “All-on-Four” Restorations. Implant. Dent. 2015, 24, 125–129. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Garbacea, A.; Naylor, W.P.; Daher, T.; Marchack, C.B.; Lowry, J. CAD/CAM fabricated complete dentures: Concepts and clinical methods of obtaining required morphological data. J. Prosthet. Dent. 2012, 107, 34–46. [Google Scholar] [CrossRef]
- Bajunaid, S.O. A first experience with digital complete overdentures. Saudi Dent. J. 2016, 28, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Baba, N.Z.; Goodacre, B.J.; Goodacre, C.J.; Muller, F.; Wagner, S. CAD/CAM Complete Denture Systems and Physical Properties: A Review of the Literature. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2021, 30, 113–124. [Google Scholar] [CrossRef]
- Yilmaz, B.; Azak, A.N.; Alp, G.; Ekşi, H. Use of CAD-CAM technology for the fabrication of complete dentures: An alternative technique. J. Prosthet. Dent. 2017, 118, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.N.; Lee, D.H. A Digital Technique to Replicate Edentulous Arches with Functional Borders and Accurate Maxillomandibular Relationship for Digital Complete Denture. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2020, 29, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Çakmak, G.; Donmez, M.B.; Atalay, S.; Yilmaz, H.; Kokat, A.M.; Yilmaz, B. Accuracy of single implant scans with a combined healing abutment-scan body system and different intraoral scanners: An in vitro study. J. Dent. 2021, 113, 103773. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Kwon, K.-R.; Pae, A.; Noh, K.; Paek, J.; Hong, S.-J. Rehabilitation of fully edentulous patient using Ceramill full denture system (FDS). J. Korean Acad. Prosthodont. 2019, 57, 232–237. [Google Scholar] [CrossRef] [Green Version]
- Contrepois, M.; Sireix, C.; Soenen, A.; Pia, J.P.; Lasserre, J.F. Complete denture fabrication with CAD/CAM technology: A case report. Int. J. Esthet. Dent. 2018, 13, 66–85. [Google Scholar]
- Janeva, N.; Kovacevska, G.; Janev, E. Complete Dentures Fabricated with CAD/CAM Technology and a Traditional Clinical Recording Method. Open Access Maced. J. Med. Sci. 2017, 5, 785–789. [Google Scholar] [CrossRef] [Green Version]
- Ohkubo, C.; Shimpo, H.; Tokue, A.; Park, E.J.; Kim, T.H. Complete denture fabrication using piezography and CAD-CAM: A clinical report. J. Prosthet. Dent. 2018, 119, 334–338. [Google Scholar] [CrossRef]
- de Mendonca, A.F.; Furtado de Mendonca, M.; White, G.S.; Sara, G.; Littlefair, D. Total CAD/CAM Supported Method for Manufacturing Removable Complete Dentures. Case Rep. Dent. 2016, 2016, 1259581. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.-J.; Kim, K.-H.; Yeo, D.-H. Fabrication of computer-aided design/computer-aided manufacturing complete denture and conventional complete denture: Case report. J. Dent. Rehabil. Appl. Sci. 2016, 32, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Bilgin, M.S.; Erdem, A.; Aglarci, O.S.; Dilber, E. Fabricating Complete Dentures with CAD/CAM and RP Technologies. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2015, 24, 576–579. [Google Scholar] [CrossRef]
- Bidra, A.S.; Farrell, K.; Burnham, D.; Dhingra, A.; Taylor, T.D.; Kuo, C.L. Prospective cohort pilot study of 2-visit CAD/CAM monolithic complete dentures and implant-retained overdentures: Clinical and patient-centered outcomes. J. Prosthet. Dent. 2016, 115, 578–586.e571. [Google Scholar] [CrossRef] [PubMed]
- Infante, L.; Yilmaz, B.; McGlumphy, E.; Finger, I. Fabricating complete dentures with CAD/CAM technology. J. Prosthet. Dent. 2014, 111, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, M.; Inokoshi, M.; Minakuchi, S.; Ohbayashi, N. Trial of a CAD/CAM system for fabricating complete dentures. Dent. Mater. J. 2011, 30, 93–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joda, T.; Müller, P.; Zimmerling, F.; Schimmel, M. CAD/CAM produced complete dentures with the “Digital Denture Professional System”. Swiss Dent. J. Sso 2016, 126, 899–909. [Google Scholar]
- Maeda, Y.; Minoura, M.; Tsutsumi, S.; Okada, M.; Nokubi, T. A CAD/CAM system for removable denture. Part I: Fabrication of complete dentures. Int. J. Prosthodont. 1994, 7, 17–21. [Google Scholar]
- Kawahata, N.; Ono, H.; Nishi, Y.; Hamano, T.; Nagaoka, E. Trial of duplication procedure for complete dentures by CAD/CAM. J. Oral Rehabil. 1997, 24, 540–548. [Google Scholar] [CrossRef]
- Busch, M.; Kordass, B. Concept and development of a computerized positioning of prosthetic teeth for complete dentures. Int. J. Comput. Dent. 2006, 9, 113–120. [Google Scholar]
- Kattadiyil, M.T.; Goodacre, C.J.; Baba, N.Z. CAD/CAM complete dentures: A review of two commercial fabrication systems. J. Calif. Dent. Assoc. 2013, 41, 407–416. [Google Scholar]
- McLaughlin, J.B.; Ramos, V., Jr.; Dickinson, D.P. Comparison of Fit of Dentures Fabricated by Traditional Techniques Versus CAD/CAM Technology. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2019, 28, 428–435. [Google Scholar] [CrossRef]
- Baba, N.Z.; AlRumaih, H.S.; Goodacre, B.J.; Goodacre, C.J. Current techniques in CAD/CAM denture fabrication. Gen. Dent. 2016, 64, 23–28. [Google Scholar]
- Steinmassl, O.; Dumfahrt, H.; Grunert, I.; Steinmassl, P.A. CAD/CAM produces dentures with improved fit. Clin. Oral Investig. 2018, 22, 2829–2835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirayama, H. Digital removable complete denture (DRCD). In Digital Restorative Dentistry; Springer: Berlin/Heidelberg, Germany, 2019; pp. 115–136. [Google Scholar]
- Edition, P.T. Parameters of Care for the Specialty of Prosthodontics. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2005, 14, 1–103. [Google Scholar]
- Bonnet, G.; Batisse, C.; Bessadet, M.; Nicolas, E.; Veyrune, J.L. A new digital denture procedure: A first practitioners appraisal. BMC Oral Health 2017, 17, 155. [Google Scholar] [CrossRef] [Green Version]
- Al Moaleem, M.M.; Al-layl, O.; Alhomood, M.; Ageeli, W.; Qsadi, A.; Mohammed, T.; Baraqt, E.; Zubayni, B.; Alalmaie, N.; Huraysi, A. Computer Engineering Complete Dentures Workflow: Systematic Techniques Review. J. Pharm. Res. Int. 2021, 33, 207–220. [Google Scholar] [CrossRef]
- Srinivasan, M.; Schimmel, M.; Naharro, M.; O’Neill, C.; McKenna, G.; Muller, F. CAD/CAM milled removable complete dentures: Time and cost estimation study. J. Dent. 2019, 80, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z.; Kattadiyil, M.T. Comparison of denture tooth movement between CAD-CAM and conventional fabrication techniques. J. Prosthet. Dent. 2018, 119, 108–115. [Google Scholar] [CrossRef] [PubMed]
- AlHelal, A.; AlRumaih, H.S.; Kattadiyil, M.T.; Baba, N.Z.; Goodacre, C.J. Comparison of retention between maxillary milled and conventional denture bases: A clinical study. J. Prosthet. Dent. 2017, 117, 233–238. [Google Scholar] [CrossRef]
- Kattadiyil, M.T.; Jekki, R.; Goodacre, C.J.; Baba, N.Z. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J. Prosthet. Dent. 2015, 114, 818–825. [Google Scholar] [CrossRef]
- Janeva, N.M.; Kovacevska, G.; Elencevski, S.; Panchevska, S.; Mijoska, A.; Lazarevska, B. Advantages of CAD/CAM versus Conventional Complete Dentures—A Review. Open Access Maced. J. Med. Sci. 2018, 6, 1498–1502. [Google Scholar] [CrossRef] [Green Version]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Thalji, G.; Jia-mahasap, W. CAD/CAM removable dental prostheses: A review of digital impression techniques for edentulous arches and advancements on design and manufacturing systems. Curr. Oral Health Rep. 2017, 4, 151–157. [Google Scholar] [CrossRef]
- Andreescu, C.F.; Ghergic, D.L.; Botoaca, O.; Hancu, V.; Banateanu, A.M.; Patroi, D.N. Evaluation of different materials used for fabrication of complete digital denture. Mater. Plast. 2018, 55, 124. [Google Scholar] [CrossRef]
- Paolone, G.; Moratti, E.; Goracci, C.; Gherlone, E.; Vichi, A. Effect of Finishing Systems on Surface Roughness and Gloss of Full-Body Bulk-Fill Resin Composites. Materials 2020, 13, 5657. [Google Scholar] [CrossRef] [PubMed]
- Al Moaleem, M.M.; Porwal, A.; Alahmari, N.; Shariff, M. Oral Biofilm on Dental Materials Among Khat Chewers. Curr. Pharm. Biotechnol. 2020, 21, 964–972. [Google Scholar] [CrossRef]
- Ramage, G.; Coco, B.; Sherry, L.; Bagg, J.; Lappin, D.F. In vitro Candida albicans biofilm induced proteinase activity and SAP8 expression correlates with in vivo denture stomatitis severity. Mycopathologia 2012, 174, 11–19. [Google Scholar] [CrossRef]
- Al-Fouzan, A.F.; Al-Mejrad, L.A.; Albarrag, A.M. Adherence of Candida to complete denture surfaces in vitro: A comparison of conventional and CAD/CAM complete dentures. J. Adv. Prosthodont. 2017, 9, 402–408. [Google Scholar] [CrossRef] [Green Version]
- Taebunpakul, P.; Jirawechwongsakul, P. Palatal Inflammation and the Presence of Candida in Denture-Wearing Patients. J. Int. Soc. Prev. Community Dent. 2021, 11, 272–280. [Google Scholar] [CrossRef]
- Murat, S.; Alp, G.; Alatali, C.; Uzun, M. In Vitro Evaluation of Adhesion of Candida albicans on CAD/CAM PMMA-Based Polymers. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2019, 28, e873–e879. [Google Scholar] [CrossRef]
- Saponaro, P.C.; Yilmaz, B.; Johnston, W.; Heshmati, R.H.; McGlumphy, E.A. Evaluation of patient experience and satisfaction with CAD-CAM-fabricated complete dentures: A retrospective survey study. J. Prosthet. Dent. 2016, 116, 524–528. [Google Scholar] [CrossRef]
- Saponaro, P.C.; Yilmaz, B.; Heshmati, R.H.; McGlumphy, E.A. Clinical performance of CAD-CAM-fabricated complete dentures: A cross-sectional study. J. Prosthet. Dent. 2016, 116, 431–435. [Google Scholar] [CrossRef]
- Kivovics, P.; Jahn, M.; Borbely, J.; Marton, K. Frequency and location of traumatic ulcerations following placement of complete dentures. Int. J. Prosthodont. 2007, 20, 397–401. [Google Scholar] [PubMed]
- Inokoshi, M.; Kanazawa, M.; Minakuchi, S. Evaluation of a complete denture trial method applying rapid prototyping. Dent. Mater. J. 2012, 31, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwindling, F.S.; Stober, T. A comparison of two digital techniques for the fabrication of complete removable dental prostheses: A pilot clinical study. J. Prosthet. Dent. 2016, 116, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Wulfman, C.; Bonnet, G.; Carayon, D.; Lance, C.; Fages, M.; Vivard, F.; Daas, M.; Rignon-Bret, C.; Naveau, A.; Millet, C. Digital removable complete denture: A narrative review. Fr. J. Dent. Med. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Baba, N.Z. Materials and processes for CAD/CAM complete denture fabrication. Curr. Oral Health Rep. 2016, 3, 203–208. [Google Scholar] [CrossRef]
- Urechescu, H.; Pricop, M.; Pricop, C.; Mateas, M.; Natanael, S.; Galatanu, S.V.J.M.P. Thermoplastic materials used for fabrication of maxillary obturator prostheses. Mat. Plast. 2017, 54, 477. [Google Scholar] [CrossRef]
- Bechir, A.; Pacurar, M.; Bechir, E.S.; Comaneanu, M.R.; Cires, M.C.; Maris, M.; Barbu, H.J.M.P. Aesthetic importance of resin based dental materials used for orthodontic appliances. Mater Plast. 2014, 51, 57–61. [Google Scholar]
- Baba, N.Z.; Charles, J.G.; Kattadiyil, M.T. CAD/CAM removable prosthodontics. In Clinical Applications of Digital Technology; Masri, R.D.C., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015. [Google Scholar]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Muller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2019, 121, 637–643. [Google Scholar] [CrossRef]
- Bacali, C.; Mesaroș, A.Ș.; Năstase, V.; Constantiniuc, M. Particularities of CAD-CAM commercial systems with applicability in the orofacial sphere; digital complete denture. Health Sports Rehabil. Med. 2019, 20, 22–25. [Google Scholar] [CrossRef]
- Alhallak, K.R.; Nankali, A. 3D Printing Technologies for Removable Dentures Manufacturing: A Review of Potentials and Challenges. Eur. J. Prosthodont. Restor. Dent. 2021, 30, 14–19. [Google Scholar] [CrossRef]
- Peroz, S.; Peroz, I.; Beuer, F.; Sterzenbach, G.; von Stein-Lausnitz, M. Digital versus conventional complete dentures: A randomized, controlled, blinded study. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef] [PubMed]
- Paes Junior, T.J.D.A.; Tribst, J.P.M.; Dal Piva, A.M.D.O.; de Figueiredo, V.M.G.; Borges, A.L.S.; Inagati, C.M. Influence of Fibromucosa Height and Loading on the Stress Distribution of a Total Prosthesis: A Finite Element Analysis. Braz. Dent. Sci. 2021, 24, 2. [Google Scholar] [CrossRef]
- Todescan, F.F.; Hayashi, M.M.; Giugni, L.R.; Bottino, M.A.; Tribst, J.P.M. From Denture to the Final Implant-Supported Prosthesis Using a Full-Digital Protocol: A Dental Technique. Oral 2021, 1, 332–339. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Addes, M.K.; Al Qahtani, N.M.; Al Ahmari, N.M.; Alfarsi, M.A. Clinical analysis of CAD-CAM milled and printed complete dentures using computerized occlusal force analyser. Technol. Health Care 2022, 29, 1–15. [Google Scholar] [CrossRef]
- Ciancaglini, R.; Gherlone, E.F.; Redaelli, S.; Radaelli, G. The distribution of occlusal contacts in the intercuspal position and temporomandibular disorder. J. Oral Rehabil. 2002, 29, 1082–1090. [Google Scholar] [CrossRef]
- Gherlone, E.; Polizzi, E.; Tetè, G.; Capparè, P. Dentistry and COVID-19 pandemic: Operative indications post-lockdown. New Microbiol. 2021, 44, 1–11. [Google Scholar] [PubMed]
- Calderini, A.; Pantaleo, G.; Rossi, A.; Gazzolo, D.; Polizzi, E. Adjunctive effect of chlorhexidine antiseptics in mechanical periodontal treatment: First results of a preliminary case series. Int. J. Dent. Hyg. 2013, 11, 180–185. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mubaraki, M.Q.; Moaleem, M.M.A.; Alzahrani, A.H.; Shariff, M.; Alqahtani, S.M.; Porwal, A.; Al-Sanabani, F.A.; Bhandi, S.; Tribst, J.P.M.; Heboyan, A.; et al. Assessment of Conventionally and Digitally Fabricated Complete Dentures: A Comprehensive Review. Materials 2022, 15, 3868. https://doi.org/10.3390/ma15113868
Mubaraki MQ, Moaleem MMA, Alzahrani AH, Shariff M, Alqahtani SM, Porwal A, Al-Sanabani FA, Bhandi S, Tribst JPM, Heboyan A, et al. Assessment of Conventionally and Digitally Fabricated Complete Dentures: A Comprehensive Review. Materials. 2022; 15(11):3868. https://doi.org/10.3390/ma15113868
Chicago/Turabian StyleMubaraki, Manal Q., Mohammed M. Al Moaleem, Abdulrahman H. Alzahrani, Mansoor Shariff, Saeed M. Alqahtani, Amit Porwal, Fuad A. Al-Sanabani, Shilpa Bhandi, João Paulo Mendes Tribst, Artak Heboyan, and et al. 2022. "Assessment of Conventionally and Digitally Fabricated Complete Dentures: A Comprehensive Review" Materials 15, no. 11: 3868. https://doi.org/10.3390/ma15113868
APA StyleMubaraki, M. Q., Moaleem, M. M. A., Alzahrani, A. H., Shariff, M., Alqahtani, S. M., Porwal, A., Al-Sanabani, F. A., Bhandi, S., Tribst, J. P. M., Heboyan, A., & Patil, S. (2022). Assessment of Conventionally and Digitally Fabricated Complete Dentures: A Comprehensive Review. Materials, 15(11), 3868. https://doi.org/10.3390/ma15113868