
Essential Oils for Bone Repair and Regeneration—Mechanisms and Applications

 ,
, 

Abstract
:1. Introduction
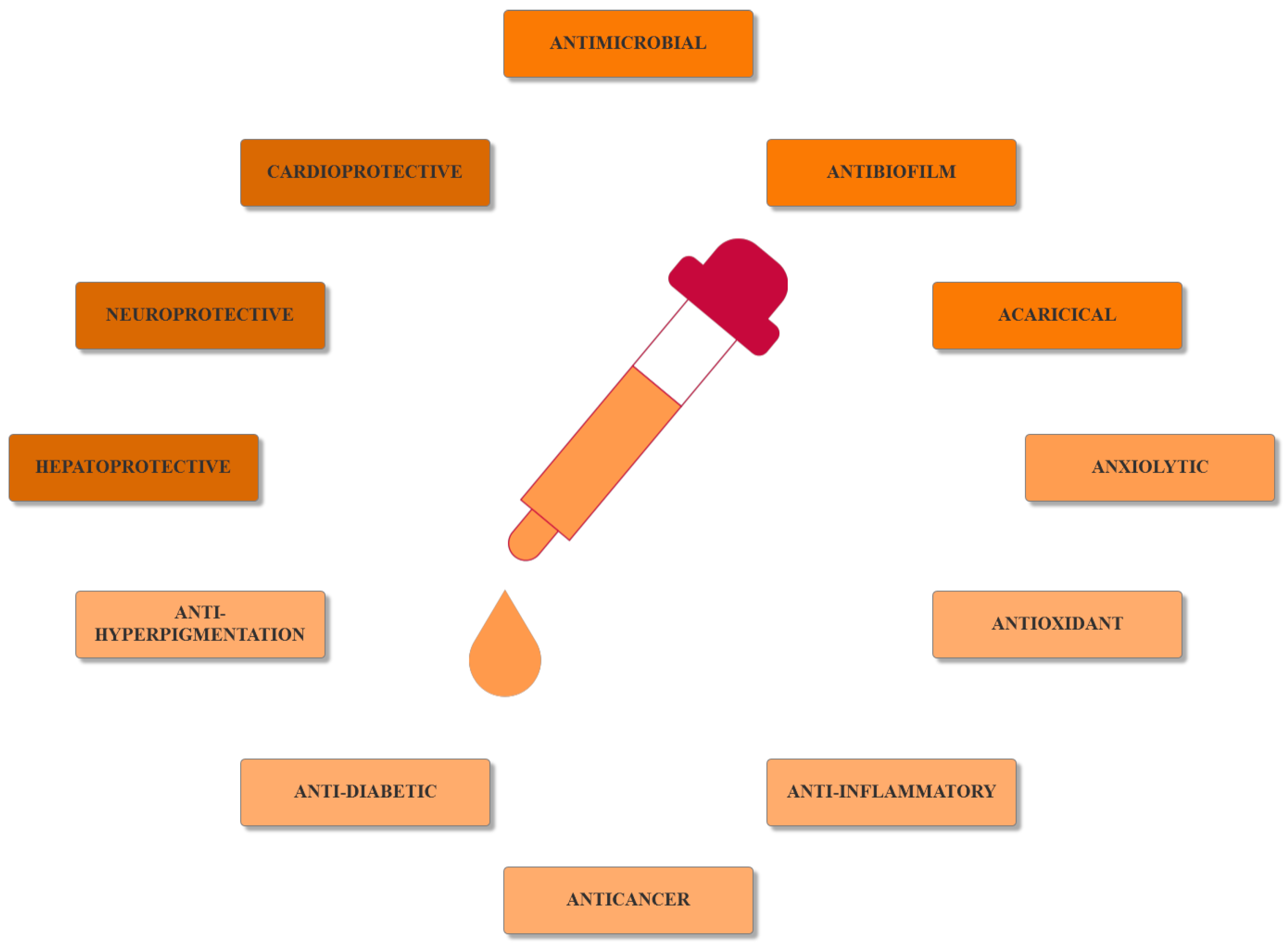
2. Bioactivities and Mechanisms of Action of Essential Oils
3. Essential Oils for Bone Repair and Regeneration
4. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martins, J.P.; Ferreira, M.P.A.; Ezazi, N.Z.; Hirvonen, J.T.; Santos, H.A.; Thrivikraman, G.; França, C.M.; Athirasala, A.; Tahayeri, A. Chapter 4—3D printing: Prospects and challenges. In Nanotechnologies in Preventive and Regenerative Medicine; Uskoković, V., Uskoković, D.P., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 299–379. [Google Scholar]
- Lacroix, D. 3—Biomechanical aspects of bone repair. In Bone Repair Biomaterials, 2nd ed.; Pawelec, K.M., Planell, J.A., Eds.; Woodhead Publishing: Sawston, UK, 2019; pp. 53–64. [Google Scholar]
- Leonardo, C.; Giorgio, L.I.; Sara, R.; Sabrina, G.; Andrea, V.; Annapaola, P.; Alessandro, S.; Barbara, D.; Paolo, M.; Adriano, P.; et al. Nanostructured surface bioactive composite scaffold for filling of bone defects. Biointerface Res. Appl. Chem. 2020, 10, 5038–5047. [Google Scholar]
- Zamfirescu, A.I.; Banciu, A.; Banciu, D.; Jinga, S.I.; Busuioc, C. Composite Fibrous Scaffolds Designed for Bone Regeneration. Rev. Romana De Mater. Rom. J. Mater. 2020, 50, 161–165. [Google Scholar]
- Yang, Y.; Chawla, A.; Zhang, J.; Esa, A.; Jang, H.L.; Khademhosseini, A. Chapter 29—Applications of Nanotechnology for Regenerative Medicine; Healing Tissues at the Nanoscale. In Principles of Regenerative Medicine, 3rd ed.; Atala, A., Lanza, R., Mikos, A.G., Nerem, R., Eds.; Academic Press: Boston, MA, USA, 2019; pp. 485–504. [Google Scholar]
- Zarif, M.-E. A review of chitosan-, alginate-, and gelatin-based biocomposites for bone tissue engineering. Biomater. Tissue Eng. Bull. 2018, 5, 97–109. [Google Scholar]
- Sharma, A.; Sharma, P.K.; Malviya, R. Stimuli-responsive supramolecules for bone tissue engineering. Biointerface Res. Appl. Chem. 2020, 10, 5122–5127. [Google Scholar]
- Zang, J.; Lu, L.; Yaszemski, M.J. Chapter 3—Bone Disorders. In Materials for Bone Disorders; Bose, S., Bandyopadhyay, A., Eds.; Academic Press: Cambridge, MA, USA, 2017; pp. 83–118. [Google Scholar]
- Jayash, S.N.; Al-Namnam, N.M.; Shaghayegh, G. Osteoprotegerin (OPG) pathways in bone diseases and its application in therapeutic perspectives. Biointerface Res. Appl. Chem. 2020, 10, 5193–5200. [Google Scholar]
- Man, G.S.; Mologhianu, G. Osteoarthritis pathogenesis—A complex process that involves the entire joint. J. Med. Life 2014, 7, 37–41. [Google Scholar]
- Blanchard, R.; Thomas, C.D.L.; Hardiman, R.; Clement, J.G.; Cooper, D.C.; Pivonka, P. Structural and Material Changes of Human Cortical Bone With Age: Lessons from the Melbourne Femur Research Collection. In Encyclopedia of Biomedical Engineering; Narayan, R., Ed.; Elsevier: Oxford, UK, 2019; pp. 246–264. [Google Scholar]
- Gimigliano, F. 34—Osteoporosis. In Braddom’s Rehabilitation Care: A Clinical Handbook; Cifu, D.X., Lew, H.L., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 238–243.e235. [Google Scholar]
- Slovik, D.M. Chapter 141—Osteoporosis. In Essentials of Physical Medicine and Rehabilitation, 4th ed.; Frontera, W.R., Silver, J.K., Rizzo, T.D., Eds.; Content Repository Only: Philadelphia, PA, USA, 2020; pp. 799–805. [Google Scholar]
- Chandrasekaran, V.; Brennan-Olsen, S.L.; Stuart, A.L.; Pasco, J.A.; Berk, M.; Hodge, J.M.; Williams, L.J. Bipolar disorder and bone health: A systematic review. J. Affect. Disord. 2019, 249, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.S.; Waterson, B. Principles of management of long bone fractures and fracture healing. Surgery 2020, 38, 91–99. [Google Scholar] [CrossRef]
- Singh, V. Medicinal plants and bone healing. Natl. J. Maxillofac. Surg. 2017, 8, 4–11. [Google Scholar] [CrossRef]
- Goharian, A. Chapter 3—Osseointegration Concepts of Trauma Fracture Fixation and Joint Replacement. In Osseointegration of Orthopaedic Implants; Goharian, A., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 55–76. [Google Scholar]
- Loi, F.; Córdova, L.A.; Pajarinen, J.; Lin, T.-H.; Yao, Z.; Goodman, S.B. Inflammation, fracture and bone repair. Bone 2016, 86, 119–130. [Google Scholar] [CrossRef] [Green Version]
- Bose, S.; Banerjee, D.; Bandyopadhyay, A. Chapter 1—Introduction to Biomaterials and Devices for Bone Disorders. In Materials for Bone Disorders; Bose, S., Bandyopadhyay, A., Eds.; Academic Press: Cambridge, MA, USA, 2017; pp. 1–27. [Google Scholar]
- Cavanna, M.; Peschiera, V.; Staletti, L.; Berlusconi, M. Allograft for the treatment of massive bone loss in open and infected IIIA fracture of the distal femur: A case report. Injury 2018. [Google Scholar] [CrossRef]
- Caldwell, S. 12—Bone Grafting Complications. In Misch’s Avoiding Complications in Oral Implantology; Resnik, R.R., Misch, C.E., Eds.; Mosby: St. Louis, MO, USA, 2018; pp. 440–498. [Google Scholar]
- Bartl, R.; Bartl, C. Bone Disorders; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Carson, M.A.; Clarke, S.A. Bioactive Compounds from Marine Organisms: Potential for Bone Growth and Healing. Mar. Drugs 2018, 16, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelghany, A.M.; Meikhail, M.S.; Hegazy, E.; Badr, S.I.; Agag, D.A. Synthesis of borate modified bioactive glass scaffold using PVP burning-out method for bone tissue replacement. Biointerface Res. Appl. Chem. 2019, 9, 4044–4049. [Google Scholar]
- Checa, S. Chapter 13—Multiscale Agent-Based Computer Models in Skeletal Tissue Regeneration. In Numerical Methods and Advanced Simulation in Biomechanics and Biological Processes; Cerrolaza, M., Shefelbine, S.J., Garzón-Alvarado, D., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 239–244. [Google Scholar]
- Miranda, L.L.; Guimarães-Lopes, V.d.P.; Altoé, L.S.; Sarandy, M.M.; Melo, F.C.S.A.; Novaes, R.D.; Gonçalves, R.V. Plant Extracts in the Bone Repair Process: A Systematic Review. Mediat. Inflamm. 2019, 2019, 1296153. [Google Scholar] [CrossRef] [PubMed]
- Freires, I.A.; Santaella, G.M.; de Cássia Orlandi Sardi, J.; Rosalen, P.L. The alveolar bone protective effects of natural products: A systematic review. Arch. Oral Biol. 2018, 87, 196–203. [Google Scholar] [CrossRef]
- Alaribe, F.N.; Razwinani, M.; Maepa, M.; Motaung, K.S.C. The Potential Effect of Medicinal Plants for Cartilage Regeneration. In Cartilage Tissue Engineering and Regeneration Techniques; IntechOpen: London, UK, 2019. [Google Scholar]
- Manciu, F.S.; Guerrero, J.; Rivera, D.; Chang, S.Y.; Bennet, K.E. Combined Theoretical and Experimental Study of Nordihydroguaiaretic Acid—From Traditional Medicine to Modern Spectroscopic Research. Biointerface Res. Appl. Chem. 2020, 10, 6728–6743. [Google Scholar]
- Suvarna, V.; Sarkar, M.; Chaubey, P.; Khan, T.; Sherje, A.; Patel, K.; Dravyakar, B. Bone Health and Natural Products—An Insight. Front. Pharm. 2018, 9, 981. [Google Scholar] [CrossRef]
- Benelli, G.; Pavela, R. Repellence of essential oils and selected compounds against ticks—A systematic review. Acta Trop. 2018, 179, 47–54. [Google Scholar] [CrossRef]
- Baptista-Silva, S.; Borges, S.; Ramos, O.L.; Pintado, M.; Sarmento, B. The progress of essential oils as potential therapeutic agents: A review. J. Essent. Oil Res. 2020, 1–17. [Google Scholar] [CrossRef]
- Naeem, A.; Abbas, T.; Ali, T.; Hasnain, A. Essential oils: Brief background and uses. Ann. Short Rep. 2018, 1, 1006. [Google Scholar]
- Podgoreanu, P.; Negrea, S.M.; Buia, R.; Delcaru, C.; Trusca, S.B.; Lazar, V.; Chifiriuc, M.C. Alternative strategies for fighting multidrug resistant bacterial infections. Biointerface Res. Appl. Chem. 2019, 9, 3834–3841. [Google Scholar]
- Putnam, S.E.; Scutt, A.M.; Bicknell, K.; Priestley, C.M.; Williamson, E.M. Natural products as alternative treatments for metabolic bone disorders and for maintenance of bone health. Phytother. Res. Ptr. 2007, 21, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, O.; Linero, I. Regenerative Medicine: A New Paradigm in Bone Regeneration. Adv. Tech. Bone Regen. 2016, 12, 253–274. [Google Scholar]
- Heghes, S.C.; Vostinaru, O.; Rus, L.M.; Mogosan, C.; Iuga, C.A.; Filip, L. Antispasmodic Effect of Essential Oils and Their Constituents: A Review. Molecules 2019, 24, 1675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- León-Méndez, G.; Pájaro-Castro, N.; Pájaro-Castro, E.; Torrenegra-Alarcon, M.; Herrera-Barros, A. Essential oils as a source of bioactive molecules. Rev. Colomb. De Cienc. Químico Farm. 2019, 48, 80–93. [Google Scholar]
- Ribeiro-Santos, R.; Andrade, M.; Sanches-Silva, A.; de Melo, N.R. Essential Oils for Food Application: Natural Substances with Established Biological Activities. Food Bioprocess. Technol. 2018, 11, 43–71. [Google Scholar] [CrossRef]
- Dhifi, W.; Bellili, S.; Jazi, S.; Bahloul, N.; Mnif, W. Essential Oils’ Chemical Characterization and Investigation of Some Biological Activities: A Critical Review. Medicines 2016, 3, 25. [Google Scholar] [CrossRef] [Green Version]
- Morsy, N.F.S. Chemical structure, quality indices and bioactivity of essential oil constituents. Act. Ingred. Aromat. Med. Plants; Intech 2017, 11, 175–206. [Google Scholar]
- Eslahi, H.; Fahimi, N.; Sardarian, A.R. Chemical Composition of Essential Oils. In Essential Oils in Food Processing; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2017; pp. 119–171. [Google Scholar]
- Aldred, E.M.; Buck, C.; Vall, K. Chapter 22—Terpenes. In Pharmacology; Aldred, E.M., Buck, C., Vall, K., Eds.; Churchill Livingstone: Edinburgh, Scotland, UK, 2009; pp. 167–174. [Google Scholar]
- Wińska, K.; Mączka, W.; Łyczko, J.; Grabarczyk, M.; Czubaszek, A.; Szumny, A. Essential Oils as Antimicrobial Agents—Myth or Real Alternative? Molecules 2019, 24, 2130. [Google Scholar] [CrossRef] [Green Version]
- Mihai, A.D.; Chircov, C.; Grumezescu, A.M.; Holban, A.M. Magnetite Nanoparticles and Essential Oils Systems for Advanced Antibacterial Therapies. Int. J. Mol. Sci. 2020, 21, 7355. [Google Scholar] [CrossRef]
- Khan, Z.; Upadhyaya, H. Chapter 15—Impact of Nanoparticles on Abiotic Stress Responses in Plants: An Overview. In Nanomaterials in Plants, Algae and Microorganisms; Tripathi, D.K., Ahmad, P., Sharma, S., Chauhan, D.K., Dubey, N.K., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 305–322. [Google Scholar]
- Zia-ur-Rehman, M.; Qayyum, M.F.; Akmal, F.; Maqsood, M.A.; Rizwan, M.; Waqar, M.; Azhar, M. Chapter 7—Recent Progress of Nanotoxicology in Plants. In Nanomaterials in Plants, Algae, and Microorganisms; Tripathi, D.K., Ahmad, P., Sharma, S., Chauhan, D.K., Dubey, N.K., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 143–174. [Google Scholar]
- Teleanu, R.I.; Chircov, C.; Grumezescu, A.M.; Volceanov, A.; Teleanu, D.M. Antioxidant Therapies for Neuroprotection—A Review. J. Clin. Med. 2019, 8, 1659. [Google Scholar] [CrossRef] [Green Version]
- Brainina, K.Z.; Varzakova, D.P.; Kazakov, Y.E.; Vidrevich, M.B. Noninvasive electrochemical antioxidant activity estimation: Saliva analysis. Biointerface Res. Appl. Chem. 2018, 8, 3381–3387. [Google Scholar]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef]
- Sies, H. Chapter 13—Oxidative Stress: Eustress and Distress in Redox Homeostasis. In Stress: Physiology, Biochemistry, and Pathology; Fink, G., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 153–163. [Google Scholar]
- Tan, B.L.; Norhaizan, M.E.; Liew, W.-P.-P.; Sulaiman Rahman, H. Antioxidant and Oxidative Stress: A Mutual Interplay in Age-Related Diseases. Front. Pharmacol. 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Zhang, Y.; Zhang, X.; Lu, W.; Liu, X.; Hu, M.; Wang, D. Aucubin exerts anti-osteoporotic effects by promoting osteoblast differentiation. Aging 2020, 12, 2226–2245. [Google Scholar] [CrossRef] [PubMed]
- Domazetovic, V.; Marcucci, G.; Iantomasi, T.; Brandi, M.L.; Vincenzini, M.T. Oxidative stress in bone remodeling: Role of antioxidants. Clin. Cases Min. Bone Metab. 2017, 14, 209–216. [Google Scholar] [CrossRef]
- Lee, S.; Le, N.H.; Kang, D. Melatonin alleviates oxidative stress-inhibited osteogenesis of human bone marrow-derived mesenchymal stem cells through AMPK activation. Int. J. Med. Sci. 2018, 15, 1083–1091. [Google Scholar] [CrossRef] [Green Version]
- Azizieh, F.Y.; Shehab, D.; Jarallah, K.A.; Gupta, R.; Raghupathy, R. Circulatory Levels of RANKL, OPG, and Oxidative Stress Markers in Postmenopausal Women With Normal or Low Bone Mineral Density. Biomark Insights 2019, 14. [Google Scholar] [CrossRef]
- Qin, D.; Zhang, H.; Zhang, H.; Sun, T.; Zhao, H.; Lee, W.H. Anti-osteoporosis effects of osteoking via reducing reactive oxygen species. J. Ethnopharmacol. 2019, 244, 112045. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.K.; Mohamad, N.V.; Ibrahim, N.; Chin, K.Y.; Shuid, A.N.; Ima-Nirwana, S. The Molecular Mechanism of Vitamin E as a Bone-Protecting Agent: A Review on Current Evidence. Int. J. Mol. Sci. 2019, 20, 1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Xu, Z.; Duan, C.; Liu, W.; Sun, J.; Han, B. Role of TCF/LEF Transcription Factors in Bone Development and Osteogenesis. Int. J. Med. Sci. 2018, 15, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Kovács, B.; Vajda, E.; Nagy, E.E. Regulatory Effects and Interactions of the Wnt and OPG-RANKL-RANK Signaling at the Bone-Cartilage Interface in Osteoarthritis. Int. J. Mol. Sci. 2019, 20, 4653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, T.; Hayashi, M.; Sasaki, F.; Nakashima, T. RANKL biology: Bone metabolism, the immune system, and beyond. Inflamm. Regen. 2020, 40, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochette, L.; Meloux, A.; Rigal, E.; Zeller, M.; Cottin, Y.; Vergely, C. The Role of Osteoprotegerin and Its Ligands in Vascular Function. Int. J. Mol. Sci. 2019, 20, 705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, H.; He, X.; Zhang, Y.; Wu, R.; Chen, J.; Lin, Y.; Shen, B. MicroRNA Alterations for Diagnosis, Prognosis, and Treatment of Osteoporosis: A Comprehensive Review and Computational Functional Survey. Front. Genet 2020, 11, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Infante, M.; Fabi, A.; Cognetti, F.; Gorini, S.; Caprio, M.; Fabbri, A. RANKL/RANK/OPG system beyond bone remodeling: Involvement in breast cancer and clinical perspectives. J. Exp. Clin. Cancer Res. 2019, 38, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobeiha, M.; Moghadasian, M.H.; Amin, N.; Jafarnejad, S. RANKL/RANK/OPG Pathway: A Mechanism Involved in Exercise-Induced Bone Remodeling. Biomed. Res. Int. 2020, 2020, 6910312. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.-R.; Wang, Y.; Sun, Y.-C. Imbalance of osteoprotegerin/receptor activator of nuclear factor-κB ligand and oxidative stress in patients with obstructive sleep apnea-hypopnea syndrome. Chin. Med. J. 2019, 132, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Palomer, E.; Buechler, J.; Salinas, P.C. Wnt Signaling Deregulation in the Aging and Alzheimer’s Brain. Front. Cell Neurosci. 2019, 13, 227. [Google Scholar] [CrossRef]
- Ljungberg, J.K.; Kling, J.C.; Tran, T.T.; Blumenthal, A. Functions of the WNT Signaling Network in Shaping Host Responses to Infection. Front. Immunol. 2019, 10, 2521. [Google Scholar] [CrossRef] [PubMed]
- Shaw, H.V.; Koval, A.; Katanaev, V.J.S.M.W. Targeting the Wnt signalling pathway in cancer: Prospects and perils. Swiss Med. Wkly. 2019, 149, w20129. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Fernandez, C.; Gonzalez, P.; Rodriguez, F. New insights into Wnt signaling alterations in amyotrophic lateral sclerosis: A potential therapeutic target? Neural. Regen. Res. 2020, 15, 1580–1589. [Google Scholar] [CrossRef]
- Wan, M. LRPs in Bone Homeostasis and Disease. In Encyclopedia of Bone Biology; Zaidi, M., Ed.; Academic Press: Oxford, UK, 2020; pp. 461–469. [Google Scholar]
- Mo, Y.; Wang, Y.; Zhang, L.; Yang, L.; Zhou, M.; Li, X.; Li, Y.; Li, G.; Zeng, Z.; Xiong, W.; et al. The role of Wnt signaling pathway in tumor metabolic reprogramming. J.Cancer 2019, 10, 3789–3797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kan, C.; Ding, N.; Kan, L. Heterotopic Ossification and Calcification. In Encyclopedia of Endocrine Diseases, 2nd ed.; Huhtaniemi, I., Martini, L., Eds.; Academic Press: Oxford, UK, 2019; pp. 356–364. [Google Scholar]
- Staehlke, S.; Haack, F.; Waldner, A.-C.; Koczan, D.; Moerke, C.; Mueller, P.; Uhrmacher, A.M.; Nebe, J.B. ROS Dependent Wnt/β-Catenin Pathway and Its Regulation on Defined Micro-Pillars—A Combined In Vitro and In Silico Study. Cells 2020, 9, 1784. [Google Scholar] [CrossRef]
- Wang, Y.; Fan, X.; Xing, L.; Tian, F. Wnt signaling: A promising target for osteoarthritis therapy. Cell Commun. Signal. 2019, 17, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Tannous, E.; Zheng, J.J. Oxidative stress upregulates Wnt signaling in human retinal microvascular endothelial cells through activation of disheveled. J. Cell Biochem. 2019, 120, 14044–14054. [Google Scholar] [CrossRef] [PubMed]
- Shams Moattar, F.; Sariri, R.; Giahi, M.; Yaghmaee, P. Essential Oil Composition and Antioxidant Activity of Calamintha officinalis Moench. J. Appl. Biotechnol. Rep. 2018, 5, 55–58. [Google Scholar] [CrossRef]
- Farias, P.K.S.; Silva, J.C.R.L.; Souza, C.N.d.; Fonseca, F.S.A.d.; Brandi, I.V.; Martins, E.R.; Azevedo, A.M.; Almeida, A.C.d. Antioxidant activity of essential oils from condiment plants and their effect on lactic cultures and pathogenic bacteria. Ciência Rural 2019, 49. [Google Scholar] [CrossRef] [Green Version]
- Sridevi, P.; Budde, S.; Adapa, D. Anti-oxidants and their role in disease management. Int. J. Med. Res. Health Sci. 2018, 7, 175–190. [Google Scholar]
- Olmedo, R.; Ribotta, P.; Grosso, N.R. Antioxidant Activity of Essential Oils Extracted from Aloysia triphylla and Minthostachys mollis that Improve the Oxidative Stability of Sunflower Oil under Accelerated Storage Conditions. Eur. J. Lipid Sci. Technol. 2018, 120, 1700374. [Google Scholar] [CrossRef] [Green Version]
- Torres-Martínez, R.; García-Rodríguez, Y.M.; Ríos-Chávez, P.; Saavedra-Molina, A.; López-Meza, J.E.; Ochoa-Zarzosa, A.; Garciglia, R.S. Antioxidant Activity of the Essential Oil and its Major Terpenes of Satureja macrostema (Moc. and Sessé ex Benth.) Briq. Pharm. Mag. 2018, 13, S875–S880. [Google Scholar]
- Hashemi, S.M.B.; Khorram, S.B.; Sohrabi, M. Antioxidant Activity of Essential Oils in Foods. In Essential Oils in Food Processing; Wiley-Blackwell: Hoboken, NJ, USA, 2017; pp. 247–265. [Google Scholar]
- Ansari, M.Y.; Ahmad, N.; Haqqi, T.M. Oxidative stress and inflammation in osteoarthritis pathogenesis: Role of polyphenols. Biomed. Pharmacother. 2020, 129, 110452. [Google Scholar] [CrossRef] [PubMed]
- Pisoschi, A.M.; Pop, A.; Iordache, F.; Stanca, L.; Predoi, G.; Serban, A.I. Oxidative stress mitigation by antioxidants—An overview on their chemistry and influences on health status. Eur. J. Med. Chem. 2021, 209, 112891. [Google Scholar] [CrossRef] [PubMed]
- Abd El Raheim, M.; Soliman, G.A.; Al-Saikhan, F.I.; Gabr, G.A.; Majid, A.; Ganaie, M.N.; Al Enazi, S.Z.; Radwan, A.M. The Potential Anti-inflammatory activity of essential oils of Pituranthos triradiatus and Anthemis deserti in rats. Bull. Environ. Pharm. Life Sci. 2015, 4, 28–31. [Google Scholar]
- Kar, S.; Gupta, P.; Gupta, J. Essential Oils: Biological Activity Beyond Aromatherapy. Nat. Prod. Sci. 2018, 24, 139–147. [Google Scholar] [CrossRef] [Green Version]
- da Silveira e Sá, R.d.C.; Andrade, L.N.; de Sousa, D.P. Sesquiterpenes from Essential Oils and Anti-Inflammatory Activity. Nat. Prod. Commun. 2015, 10, 1767–1774. [Google Scholar] [CrossRef] [Green Version]
- Xiao, D.; Zhang, J.; Zhang, C.; Barbieri, D.; Yuan, H.; Moroni, L.; Feng, G. The role of calcium phosphate surface structure in osteogenesis and the mechanisms involved. Acta Biomater. 2020, 106, 22–33. [Google Scholar] [CrossRef]
- Florea, D.A.; Chircov, C.; Grumezescu, A.M. Hydroxyapatite Particles—Directing the Cellular Activity in Bone Regeneration Processes: An Up-To-Date Review. Appl. Sci. 2020, 10, 3483. [Google Scholar] [CrossRef]
- Shih, Y.V.; Varghese, S. Tissue engineered bone mimetics to study bone disorders ex vivo: Role of bioinspired materials. Biomaterials 2019, 198, 107–121. [Google Scholar] [CrossRef]
- Setiawati, R.; Rahardjo, P. Bone Development and Growth. In Osteogenesis and Bone Regeneration; IntechOpen: London, UK, 2018. [Google Scholar]
- Luo, Z.; Shang, X.; Zhang, H.; Wang, G.; Massey, P.A.; Barton, S.R.; Kevil, C.G.; Dong, Y. Notch Signaling in Osteogenesis, Osteoclastogenesis, and Angiogenesis. Am. J. Pathol. 2019, 189, 1495–1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iaquinta, M.R.; Mazzoni, E.; Bononi, I.; Rotondo, J.C.; Mazziotta, C.; Montesi, M.; Sprio, S.; Tampieri, A.; Tognon, M.; Martini, F. Adult Stem Cells for Bone Regeneration and Repair. Front. Cell Dev. Biol. 2019, 7, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, M. Bone tissue regeneration: Biology, strategies and interface studies. Prog. Biomater. 2019, 8, 223–237. [Google Scholar] [CrossRef] [Green Version]
- Majidinia, M.; Sadeghpour, A.; Yousefi, B. The roles of signaling pathways in bone repair and regeneration. J. Cell. Physiol. 2018, 233, 2937–2948. [Google Scholar] [CrossRef]
- Damlar, İ.; Arpağ, O.F.; Tatli, U.; Altan, A. Effects of Hypericum perforatum on the healing of xenografts: A histomorphometric study in rabbits. Br. J. Oral. Maxillofac. Surg. 2017, 55, 383–387. [Google Scholar] [CrossRef]
- Kania, N.; Widowati, W.; Dewi, F.R.P.; Christianto, A.; Setiawan, B.; Budhiparama, N.; Noor, Z. Cinnamomum burmanini Blume increases bone turnover marker and induces tibia’s granule formation in ovariectomized rats. J. Ayurveda Integr. Med. 2018, 9, 20–26. [Google Scholar] [CrossRef]
- Elbahnasawy, A.S.; Valeeva, E.R.; El-Sayed, E.M.; Rakhimov, I.I. The Impact of Thyme and Rosemary on Prevention of Osteoporosis in Rats. J. Nutr. Metab. 2019, 2019, 1431384. [Google Scholar] [CrossRef] [Green Version]
- Sapkota, M.; Li, L.; Kim, S.-W.; Soh, Y. Thymol inhibits RANKL-induced osteoclastogenesis in RAW264.7 and BMM cells and LPS-induced bone loss in mice. Food Chem. Toxicol. 2018, 120, 418–429. [Google Scholar] [CrossRef]
- Belkhodja, H.; Meddah, B.; Meddah TirTouil, A.; Slimani, K.; Tou, A. Radiographic and Histopathologic Analysis on Osteoarthritis Rat Model Treated with Essential Oils of Rosmarinus officinalis and Populus alba. Pharm. Sci. 2017, 23, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Funk, J.L.; Frye, J.B.; Oyarzo, J.N.; Chen, J.; Zhang, H.; Timmermann, B.N. Anti-inflammatory effects of the essential oils of ginger (Zingiber officinale Roscoe) in experimental rheumatoid arthritis. Pharma Nutr. 2016, 4, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Bi, J.-P.; Li, P.; Xu, X.-X.; Wang, T.; Li, F. Anti-rheumatoid arthritic effect of volatile components in notopterygium incisum in rats via anti-inflammatory and anti-angiogenic activities. Chin. J. Nat. Med. 2018, 16, 926–935. [Google Scholar] [CrossRef]
- Xu, C.; Sheng, S.; Dou, H.; Chen, J.; Zhou, K.; Lin, Y.; Yang, H. α-Bisabolol suppresses the inflammatory response and ECM catabolism in advanced glycation end products-treated chondrocytes and attenuates murine osteoarthritis. Int. Immunopharmacol. 2020, 84, 106530. [Google Scholar] [CrossRef] [PubMed]
- Gomes, B.S.; Neto, B.P.S.; Lopes, E.M.; Cunha, F.V.M.; Araújo, A.R.; Wanderley, C.W.S.; Wong, D.V.T.; Júnior, R.C.P.L.; Ribeiro, R.A.; Sousa, D.P.; et al. Anti-inflammatory effect of the monoterpene myrtenol is dependent on the direct modulation of neutrophil migration and oxidative stress. Chem. Biol. Interact. 2017, 273, 73–81. [Google Scholar] [CrossRef]
- Efe Arslan, D.; Kutlutürkan, S.; Korkmaz, M. The Effect of Aromatherapy Massage on Knee Pain and Functional Status in Participants with Osteoarthritis. Pain Manag. Nurs. 2019, 20, 62–69. [Google Scholar] [CrossRef]
- Nasiri, A.; Mahmodi, M.A.; Nobakht, Z. Effect of aromatherapy massage with lavender essential oil on pain in patients with osteoarthritis of the knee: A randomized controlled clinical trial. Complementary Ther. Clin. Pract. 2016, 25, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.Y.; Mani, M.P.; Jaganathan, S.K. Engineering electrospun multicomponent polyurethane scaffolding platform comprising grapeseed oil and honey/propolis for bone tissue regeneration. PLoS ONE 2018, 13, e0205699. [Google Scholar] [CrossRef] [Green Version]
- Mani, M.P.; Jaganathan, S.K.; Supriyanto, E. Enriched Mechanical Strength and Bone Mineralisation of Electrospun Biomimetic Scaffold Laden with Ylang Ylang Oil and Zinc Nitrate for Bone Tissue Engineering. Polymers 2019, 11, 1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaganathan, S.K.; Prasath Mani, M.; Ayyar, M.; Rathanasamy, R. Biomimetic electrospun polyurethane matrix composites with tailor made properties for bone tissue engineering scaffolds. Polym. Test. 2019, 78, 105955. [Google Scholar] [CrossRef]
- Zhang, Z.; Zheng, Y.; Zhang, L.; Mani, M.P.; Jaganathan, S.K. In vitro blood compatibility and bone mineralization aspects of polymeric scaffold laden with essential oil and metallic particles for bone tissue engineering. Int. J. Polym. Anal. Charact. 2019, 24, 504–516. [Google Scholar] [CrossRef]
- Banerjee, S.; Bagchi, B.; Pal, K.; Bhandary, S.; Kool, A.; Hoque, N.A.; Biswas, P.; Thakur, P.; Das, K.; Karmakar, P.; et al. Essential oil impregnated luminescent hydroxyapatite: Antibacterial and cytotoxicity studies. Mater. Sci. Eng. C 2020, 111190. [Google Scholar] [CrossRef]
- Florea, A.D.; Dănilă, E.; Constantinescu, R.R.; Kaya, M.A.; Kaya, A.D.; Coară, G.; Albu, L.; Chelaru, C. Composite scaffolds for bone regeneration made of collagen/hydroxyapatite/eucalyptus essential oil. In Proceedings of the 7th International Conference on Advanced Materials and Systems, Bucharest, Romania, 18–20 October 2018. [Google Scholar]
- Polo, L.; Díaz de Greñu, B.; Della Bella, E.; Pagani, S.; Torricelli, P.; Vivancos, J.L.; Ruiz-Rico, M.; Barat, J.M.; Aznar, E.; Martínez-Máñez, R.; et al. Antimicrobial activity of commercial calcium phosphate based materials functionalized with vanillin. Acta Biomater. 2018, 81, 293–303. [Google Scholar] [CrossRef]
- Chen, X.; Fan, H.; Deng, X.; Wu, L.; Yi, T.; Gu, L.; Zhou, C.; Fan, Y.; Zhang, X. Scaffold Structural Microenvironmental Cues to Guide Tissue Regeneration in Bone Tissue Applications. Nanomaterials 2018, 8, 960. [Google Scholar] [CrossRef] [Green Version]
- Cazzola, M.; Ferraris, S.; Allizond, V.; Bertea, C.M.; Novara, C.; Cochis, A.; Geobaldo, F.; Bistolfi, A.; Cuffini, A.M.; Rimondini, L.; et al. Grafting of the peppermint essential oil to a chemically treated Ti6Al4V alloy to counteract the bacterial adhesion. Surf. Coat. Technol. 2019, 378, 125011. [Google Scholar] [CrossRef]
- Constantino, J.A.; Delgado-Rastrollo, M.; Pacha-Olivenza, M.A.; Pérez-Giraldo, C.; Quiles, M.; González-Martín, M.L.; Gallardo-Moreno, A.M. In vivo bactericidal efficacy of farnesol on Ti6Al4V implants. Rev. Española de Cirugía Ortopédica y Traumatol. 2016, 60, 260–266. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | Isoprene Units | Carbon Atoms | Examples and Chemical Structures | |||||
|---|---|---|---|---|---|---|---|---|
| Hemiterpenes | 1 | 5 |  | |||||
| isoprene | ||||||||
| Monoterpenes | 2 | 10 |  |  |  |  | ||
| limonene | myrcene | γ-terpinene | p-cymene | |||||
 |  |  | ||||||
| α-pinene | β-pinene | sabinene | ||||||
| Sesquiterpenes | 3 | 15 |  |  |  | |||
| α-farnesene | δ-cadinene | zingiberene | ||||||
 |  |  |  | |||||
| R-humulone | S-humulone | guaiazulene | elamazulene | |||||
| Diterpenes | 4 | 20 |  |  |  | |||
| phytane | cembrene A | taxadiene | ||||||
 |  |  | ||||||
| sclarene | labdane | abietane | ||||||
| Sesterterpenes | 5 | 25 |  |  |  | |||
| astellatene | boleracene | caprutriene | ||||||
 |  |  | ||||||
| retigeranin B | brarapadiene A | brarapadiene B | ||||||
| Triterpenes | 6 | 30 |  |  |  | |||
| squalene | malabaricane | lanostane | ||||||
 |  |  | ||||||
| hopane | oleanane | ursolic acid | ||||||
| Tetraterpenes | 8 | 40 |  |  | ||||
| phytoene | β-carotene | |||||||
 |  | |||||||
| lycopene | lutein | |||||||
 | ||||||||
| cryptoxanthin | ||||||||
| Protein Class | Members |
|---|---|
| Secreted cysteine-rich glycoproteins | Wnt1, Wnt2, Wnt2b, Wnt3, Wnt3a, Wnt4, Wnt5a, Wnt5b, Wnt6, Wnt7a, Wnt7b, Wnt8a, Wnt8b, Wnt9a, Wnt9b, Wnt10a, Wnt10b, Wnt11, and Wnt16 |
| Seven-pass transmembrane Frizzled receptors | Fz1, Fz-2, Fz-3, Fz-4, Fz-5, Fz-6, Fz-7, Fz-8, Fz-9, and Fz-10 |
| Transmembrane tyrosine kinases | Ryk, ROR, and PTK7 |
| Muscle skeletal tyrosine kinase | MuSK |
| Low-density lipid receptor-related proteins co-receptors | LRP5 and LRP6 |
| Collagens | Proteoglycans/Glycosaminoglycans | Matrix Proteins |
|---|---|---|
| Collagen type I Collagen type III | Decorin Lumican Biglycan Epiphycan Keratocan | Osteocalcin Osteopontin Osteonectin Sialoprotein |
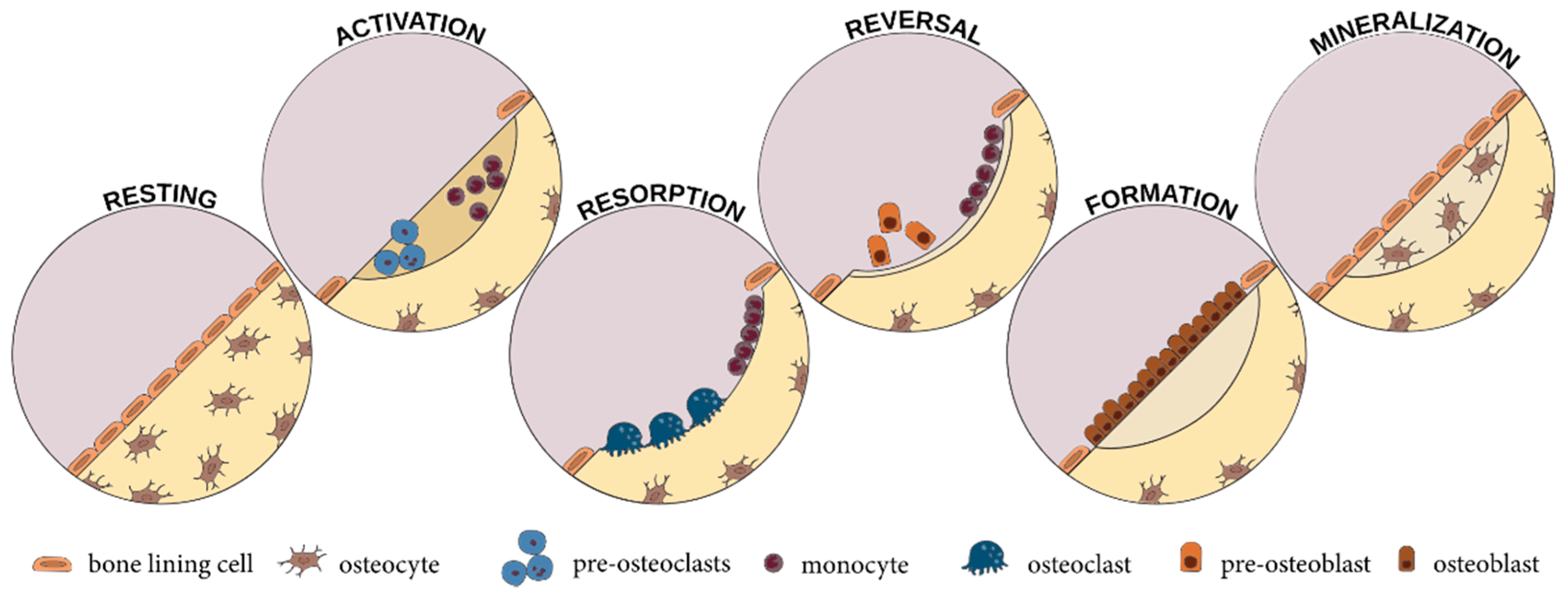
| Bone Repair Phase | Key Events | Signaling Molecules |
|---|---|---|
| Inflammation | Production of pro-inflammatory cytokines, chemokines, and growth factors Recruitment of polymorphonuclear neutrophils, macrophages, and platelets Activation of the blood coagulation cascade Formation of hematoma Angiogenesis | Tumor necrosis factor-α Interleukin-1, -6, -11, -18 Platelet-derived growth factor Transforming growth factor-b1 Tumor-derived growth factor-β Insulin-like growth factor Fibroblast growth factor-2 |
| Bone production | Differentiation of progenitor cells into chondrocytes Formation of fibrocartilage Fibrocartilage calcification Woven bone deposition | Bone morphogenetic protein Tumor-derived growth factor-β2 and -β3 |
| Bone remodeling | Differentiation of osteoprogenitor cells into osteoblasts and osteoclasts Resorption of woven bone Deposition of lamellar bone | Interleukin-1, -6, -11, and -12 Tumor necrosis factor-α Interferon-γ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chircov, C.; Miclea, I.I.; Grumezescu, V.; Grumezescu, A.M. Essential Oils for Bone Repair and Regeneration—Mechanisms and Applications. Materials 2021, 14, 1867. https://doi.org/10.3390/ma14081867
Chircov C, Miclea II, Grumezescu V, Grumezescu AM. Essential Oils for Bone Repair and Regeneration—Mechanisms and Applications. Materials. 2021; 14(8):1867. https://doi.org/10.3390/ma14081867
Chicago/Turabian StyleChircov, Cristina, Ion Iulian Miclea, Valentina Grumezescu, and Alexandru Mihai Grumezescu. 2021. "Essential Oils for Bone Repair and Regeneration—Mechanisms and Applications" Materials 14, no. 8: 1867. https://doi.org/10.3390/ma14081867
APA StyleChircov, C., Miclea, I. I., Grumezescu, V., & Grumezescu, A. M. (2021). Essential Oils for Bone Repair and Regeneration—Mechanisms and Applications. Materials, 14(8), 1867. https://doi.org/10.3390/ma14081867